Embed Size (px)
Citation preview

Gout:Its not all crystal clear
Robert L. Wortmann, M.D.Robert L. Wortmann, M.D.Department of Internal MedicineDepartment of Internal Medicine
The University of Oklahoma College of Medicine, TulsaThe University of Oklahoma College of Medicine, Tulsa
But it should be!!!!!!!!
Name another disease thatName another disease that
-the cause and pathophysiology are -the cause and pathophysiology are so so well undeerstoodwell undeerstood
-the diagnosis can be made with -the diagnosis can be made with such certaintysuch certainty
-available therapies can be so -available therapies can be so effectiveeffective

Objectives
Review the clinical features of goutReview the clinical features of gout Review the rationale for therapies of gouty Review the rationale for therapies of gouty
arthritis and the underlying hyperuricemiaarthritis and the underlying hyperuricemia Answer questionsAnswer questions
Clinical Features of Gout
1.1. HyperuricemiaHyperuricemia
2.2. Acute Monoarticular ArthritisAcute Monoarticular Arthritis
3.3. Tophi and Chronic ArthritisTophi and Chronic Arthritis
4.4. NephrolithiasisNephrolithiasis

Clinical Course of Classic Gout

Stage I
Asymptomatic HyperuricemiaAsymptomatic Hyperuricemia Serum Urate > 7.0 mg/dlSerum Urate > 7.0 mg/dl

Prevalence of Hyperuricemia
Adult MalesAdult Males
U.S.U.S.
FranceFrance
5%5%
17%17%
Hospitalized MalesHospitalized Males
Los Angeles VALos Angeles VA
Milwaukee VAMilwaukee VA
13%13%
21%21%

Factors Considered in Therapy of Asymptomatic Hyperuricemia
1.1. Renal DiseaseRenal Disease
2.2. FraminghamFramingham
3.3. SMA-12 AutoanalyzerSMA-12 Autoanalyzer
4.4. Antihyperuricemic MedicationsAntihyperuricemic Medications

Is Hyperuricemia a risk factor for coronary artery disease? Hyperuricemia is a common feature of the Hyperuricemia is a common feature of the
Metabolic SyndromeMetabolic Syndrome Epidemiologic studies are mixed and Epidemiologic studies are mixed and
confusingconfusing Richard Johnson’s rat model of Richard Johnson’s rat model of
hyperuricemiahyperuricemia

Management of Asymptomatic Hyperuricemia Determine the causeDetermine the cause Address contributing factorsAddress contributing factors
HypertensionHypertension ObesityObesity AlcoholismAlcoholism HyperlipidemiaHyperlipidemia
At this time, specific urate-lowering drugs are not At this time, specific urate-lowering drugs are not indicatedindicated

Stage II
Acute Gouty ArthritisAcute Gouty Arthritis Intercritical GoutIntercritical Gout

Clinical Course of Classic Gout

Overall Gout Prevalence Among All Enrollees 1990-1999
J Rheumatol Aug 2004

Annual Gout Prevalence Among All Enrollees by Age Group 1990-1999
J Rheumatol Aug 2004








Therapy for Acute Gouty Arthritis ColchicineColchicine
OralOral IVIV
Nonsteroidal Anti-inflammatory AgentsNonsteroidal Anti-inflammatory Agents CorticosteroidsCorticosteroids
Intra-articularIntra-articular IM (IM (ACTHACTH)) POPO

Drug Actions In Acute Gout
Colchicine inhibitsColchicine inhibits E-selectin mediated PMN adhesionE-selectin mediated PMN adhesion PMN L-selectin expressionPMN L-selectin expression Il-1 expressionIl-1 expression Il-8 productionIl-8 production PMN motilityPMN motility ChemotaxisChemotaxis
Drug Actions In Acute Gout
NSAIDsNSAIDsInhibits PGEInhibits PGE22
CorticosteroidsCorticosteroidsInhibit PGEInhibit PGE22 and LTB and LTB44
Stabilize lysosomal membranesStabilize lysosomal membranes ACTHACTH
Agonist of the leukocyte melatonin Agonist of the leukocyte melatonin receptor-3receptor-3
The The secretsecret is is not whatnot what is is used, but used, but how quicklyhow quickly therapy is initiated after therapy is initiated after the attack begins!the attack begins!


Stage III
Chronic Gouty ArthritisChronic Gouty Arthritis Tophi on physical examTophi on physical exam Chronic degenerative arthritisChronic degenerative arthritis

Clinical Course of Classic Gout










Antihyperuricemic Therapy
1.1. Treat acute attack until resolvedTreat acute attack until resolved
2.2. Colchicine or NSAID for prophylaxisColchicine or NSAID for prophylaxis
3.3. Xanthine oxidase inhibitor or uricosuricXanthine oxidase inhibitor or uricosuric
4.4. Address other problemsAddress other problems HypertensionHypertension ObesityObesity AlcoholismAlcoholism

Goal of Antihyperuricemic Therapy Serum Urate Serum Urate 5.0 mg/dl! 5.0 mg/dl! Lowering serum urate to > Lowering serum urate to >
7.0 mg/dl does not reverse 7.0 mg/dl does not reverse the problem. It only slows the problem. It only slows the rate of progression.the rate of progression.

TOPHITOPHI MEAN SERUM URATEMEAN SERUM URATE
ReducedReduced 6.2 mg/dl6.2 mg/dl
IncreasedIncreased 8.2 mg/dl8.2 mg/dl
McCarthy, Wortmann. Arthritis Rheum 1991; 34:1489.

Candidates for Uricosuric Agents Compliant patientsCompliant patients Under 60 years oldUnder 60 years old Good renal function*Good renal function* No ASANo ASA
Can use 81 mg but sould be taken 6 hours after Can use 81 mg but sould be taken 6 hours after the uricosuricthe uricosuric
No history of kidney stonesNo history of kidney stones Underexcrete uric acidUnderexcrete uric acid

Candidates for Allopurinol Everyone except thoseEveryone except those
Sensitive to itSensitive to it Taking azathioprineTaking azathioprine
Allopurinol hasAllopurinol has Once-a-day dosageOnce-a-day dosage Few drug-drug interactionsFew drug-drug interactions Effective in renal failure*Effective in renal failure* Can be used in overproducers and Can be used in overproducers and
underproducersunderproducers

Although there have been no new urate-lowering therapies available to treat gout since 1964, there will be soon.

Urate-lowering Agents in Clinical Trials
ProductProduct PhasePhase MechanismMechanism
FebuxostatFebuxostat IIIIII NP-SIXONP-SIXO
PuricasePuricase IIII PEG urate oxidasePEG urate oxidase
Uricase PEG20Uricase PEG20 II PEG urate oxidasePEG urate oxidase
oxypurinoloxypurinol IIII XOIXOI
Y-700Y-700 I-III-II XOIXOI
KT-433KT-433 IIII UricosuricUricosuric
Febuxostat
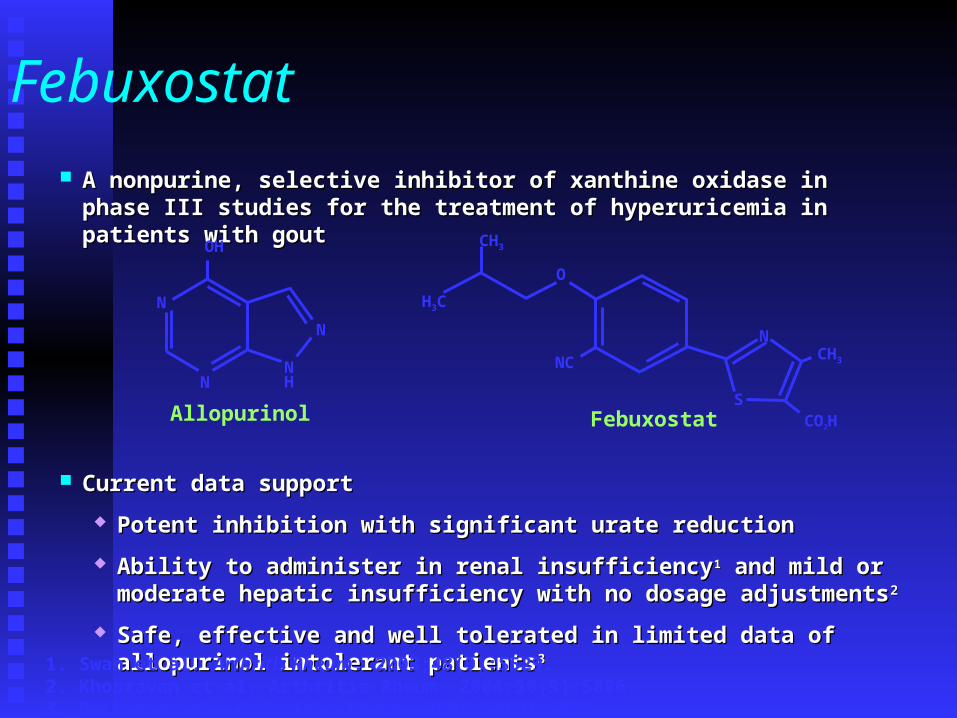
A nonpurine, selective inhibitor of xanthine oxidase in phase III studies for the A nonpurine, selective inhibitor of xanthine oxidase in phase III studies for the treatment of hyperuricemia in patients with gouttreatment of hyperuricemia in patients with gout
Current data supportCurrent data support
Potent inhibition with significant urate reductionPotent inhibition with significant urate reduction
Ability to administer in renal insufficiencyAbility to administer in renal insufficiency11 and mild or moderate hepatic and mild or moderate hepatic insufficiency with no dosage adjustmentsinsufficiency with no dosage adjustments22
Safe, effective and well tolerated in limited data of allopurinol intolerant Safe, effective and well tolerated in limited data of allopurinol intolerant patientspatients33
N
N
NH
N
OH
Allopurinol
1. Swan et al. Arthritis Rheum. 2003;48(9):S529.2. Khosravan et al. Arthritis Rheum. 2004;50(9):S806.3. Becker et al. Arthritis Rheum. 2004;50(9):S803.
Febuxostat
O
NC
N
CO2HS
CH3
CH3
H3C

Febuxostat Phase III Clinical Trial
Study design: randomized, double-blind, 52 Study design: randomized, double-blind, 52 week, multicenter trial. week, multicenter trial.
Objective: to assess safety and efficacy (vs. Objective: to assess safety and efficacy (vs. allopurinol) of daily febuxostat allopurinol) of daily febuxostat administration in lowering sUA levels in administration in lowering sUA levels in subjects with gout and hyperuricemia (sUA subjects with gout and hyperuricemia (sUA 8.0 mg/dL).8.0 mg/dL).
Enrollment: N=760 subjectsEnrollment: N=760 subjects
Becker et al. ACR/ARHP Program Book Supplement. 2004;L18.

Febuxostat Phase III Clinical Trial Results
Compared to allopurinol, significantly more patients on either dose of febuxostat were able to achieve mean serum
urate concentrations less than 6.0 mg/dL
FebuxostatFebuxostat80 mg 80 mg
FebuxostatFebuxostat120 mg 120 mg
AllopurinolAllopurinol300 mg 300 mg
Last 3 sUA <6.0 Last 3 sUA <6.0 mg/dL mg/dL
53% (136/255)*53% (136/255)* 62% (154/250)*62% (154/250)* 21% (53/251)21% (53/251)
Wk 52 sUA Wk 52 sUA <6.0 mg/dL<6.0 mg/dL
81% (129/159)*81% (129/159)* 82% (119/145)*82% (119/145)* 39% (70/178)39% (70/178)
*p<0.05 for each febuxostat group vs. allopurinol group
Proportion of Subjects with sUA <6.0 mg/dL (ITT Subjects)
Becker et al. ACR/ARHP Program Book Supplement. 2004;L18.

Why do people still suffer from gout?
Despite the fact that we understand its cause Despite the fact that we understand its cause and underlying pathophysiologyand underlying pathophysiology
Despite the fact that we can diagnosis it Despite the fact that we can diagnosis it with absolute certaintywith absolute certainty
Despite the fact that we have such rational Despite the fact that we have such rational and effective therapiesand effective therapies
Treatment Failures
Poor prescriptionPoor prescription Poor compliancePoor compliance
Inadequacy of Allopurinol at a dose 300 mg/day
Ann Rheum Disease 1998Ann Rheum Disease 1998 47%47%
J Rheumatol 2001J Rheumatol 2001 66%66%
N Engl J Med in pressN Engl J Med in press 61-79%61-79%

“Gout is Like Matches”
NSAID – puts out the fireNSAID – puts out the fire Colchicine prophylaxis – keeps matches Colchicine prophylaxis – keeps matches
dampdamp Xanthine oxidase inhibitors and uricosurics Xanthine oxidase inhibitors and uricosurics
– removes the matches– removes the matches