Embed Size (px)
Citation preview

BASIC SCIENCE
The genetics of breast cancerAlexandra J Murray
D Mark Davies
AbstractBreast cancer is the commonest cancer affecting women. A family history
of breast cancer increases a woman’s lifetime risk of developing the
disease. Most of the genetic risk is due to low-risk and moderate-risk
susceptibility alleles rather than high-penetrance genes such as BRCA1
and BRCA2. Pathogenic variants in these two tumour suppressor genes
only account for about 2% of all breast cancers. Female carriers of the
BRCA gene pathogenic variants have a high lifetime risk of developing
breast and ovarian cancer and male carriers have an increased risk of
prostate and breast cancer.
Patients with a significant family history of breast cancer should be
referred to their local cancer genetics service for a formal cancer genetics
risk assessment, discussion of risk management options such as surveil-
lance and risk-reducing surgery and consideration of genetic testing. If
a BRCA pathogenic variant is identified in a family, predictive testing
can be offered to unaffected family members to clarify risks and help
with risk management decisions.
Patients with cancer are increasingly likely to have tailored treatment,
based on genetic information. Targeted therapies exploiting vulnerabil-
ities associated with deficient BRCA function are being developed.
Keywords Autosomal dominant; breast cancer; cancer genetics; genetic
testing; germline mutation; magnetic resonance imaging; mammography;
ovarian cancer; pathogenic variants; risk assessment; screening; somatic
mutation; tumour suppressor gene
Background
Breast cancer is the commonest cancer affecting women. A
woman in the developed world has a lifetime risk of developing
breast cancer of approximately 9e11%. In 2009, over 48,000
women in the UK were diagnosed with breast cancer. Each year,
about 350 men are also diagnosed with breast cancer.
The risk of developing breast cancer for women in the general
population increases with age. Other factors known to increase
the risk include the use of hormone replacement therapy (HRT),
especially combined oestrogen and progesterone preparations,
hormonal contraceptives, obesity and alcohol. High parity,
young age at first childbirth, breastfeeding, late menarche and
early menopause all decrease the risk.
Alexandra J Murray FRCP is a Consultant Clinical Geneticist at the
University Hospital of Wales, Cardiff and Singleton Hospital, Swansea,
UK. Conflicts of interest: none declared.
D Mark Davies MRCP PhD is a Clinical Lecturer in Cancer Genetics and
Medical Oncology at the University Hospital of Wales, Cardiff, UK.
Conflicts of interest: none declared.
SURGERY 31:1 1
The clustering of breast cancer in families is almost entirely
due to genetic variation rather than shared lifestyle or environ-
ment. The risk of developing breast cancer is twice as high in
women who have an affected first-degree relative (FDR) than
women in the general population. The majority of the genetic
risk is due to low-risk or moderate-risk susceptibility alleles, each
of which confers only a very small increased risk in isolation but
which in combination may have quite a significant effect.1
Currently these low-penetrance genes cannot be used clinically
in the management of individual patients but they may, in time,
be helpful in the context of population screening programmes for
disease prevention. Pathogenic variants in high-penetrance genes
such as BRCA1 and BRCA2 (Table 1) confer a high risk of breast
cancer, but these variants are rare and only account for a small
percentage of breast cancers.
BRCA1 and BRCA2
Pathogenic variants in the BRCA1 and BRCA2 genes account for
the majority of families with an apparently dominant-looking
predisposition to breast cancer. However, they are only respon-
sible for about 2% of all breast cancers.
The BRCA1 and BRCA2 genes are tumour suppressor genes
and their proteins are involved in fundamental cell processes,
including repair of DNA double-strand breaks and checkpoint
control of the cell cycle.
The role of tumour suppressor genes in cancer development
can be explained by the ‘two-hit hypothesis’ proposed by Alfred
Knudson. In the case of BRCA1 or BRCA2, a breast cancer
develops if both copies of the relevant gene in a single cell are
damaged. Although the DNA in our tissues acquires somatic
mutations over time, in most cases it is still likely to take many
years for both copies of a BRCA gene to become mutated in any
one cell. However, if a person inherits a germline pathogenic
variant in a BRCA gene from one parent, any cell subsequently
only requires a single somatic mutation to inactivate the second
copy of the gene. This explains why hereditary cancers often
develop at an earlier age than sporadic ones.
Variation in the sequence of the BRCA genes is common.
Some variation has no effect on protein function and therefore no
increase in cancer risk. Some variants interfere with protein
function and lead to an increased risk of cancer. Such a change is
often loosely referred to as a ‘mutation’. However, some biolo-
gists define a mutation as simply a change in DNA sequence,
while others consider a mutation to be a sequence change
occurring below a certain frequency in a population or
a sequence change associated with disease. To prevent this
confusion the term variant is preferred and variants are classified
as pathogenic, non-pathogenic or of unknown significance,
depending on their associated cancer risk.
The BRCA1 gene is a large gene of 24 exons, located on the
long arm of chromosome 17. Pathogenic variants can be found in
any part of the gene and most result in truncation or total loss of
the BRCA1 protein. There is a wide spectrum of pathogenic
variants but there are a few common, ‘founder’ pathogenic
variants in certain populations such as Ashkenazi Jews. The
commonest of these, 185delAG, is responsible for about one in
five cases of early onset breast cancer in Ashkenazi Jewish
women. The BRCA2 gene has 27 exons and is found on the long
� 2013 Elsevier Ltd. All rights reserved.
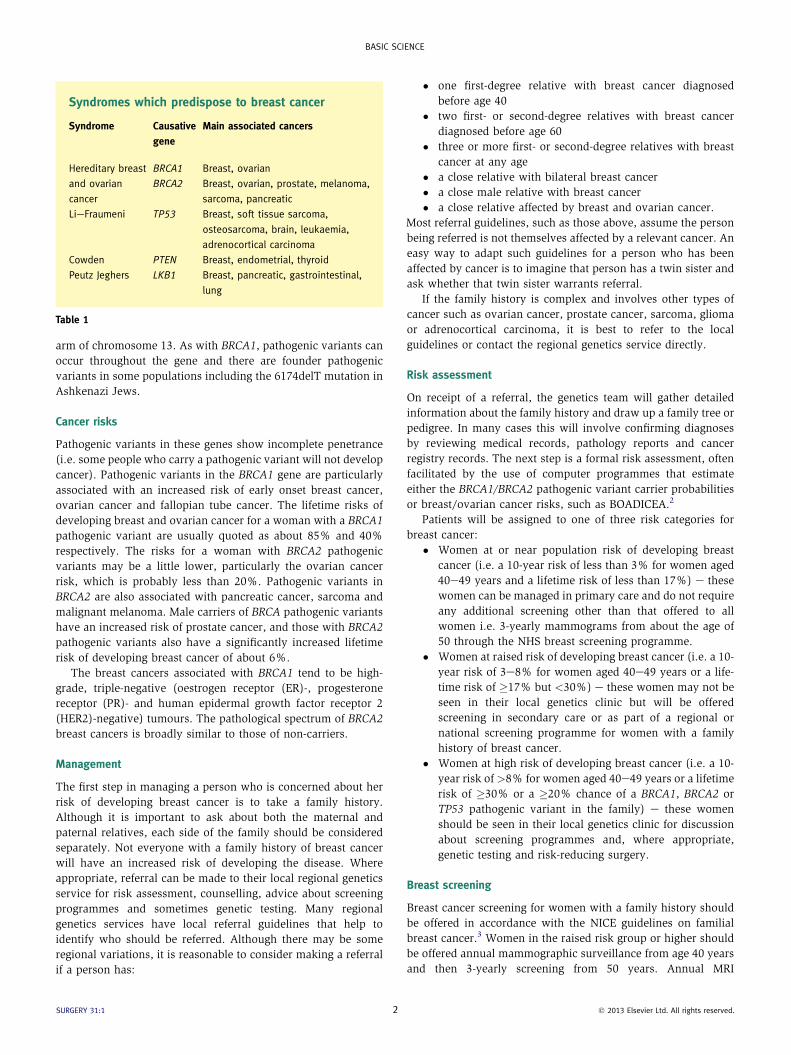
Syndromes which predispose to breast cancer
Syndrome Causative
gene
Main associated cancers
Hereditary breast
and ovarian
cancer
BRCA1 Breast, ovarian
BRCA2 Breast, ovarian, prostate, melanoma,
sarcoma, pancreatic
LieFraumeni TP53 Breast, soft tissue sarcoma,
osteosarcoma, brain, leukaemia,
adrenocortical carcinoma
Cowden PTEN Breast, endometrial, thyroid
Peutz Jeghers LKB1 Breast, pancreatic, gastrointestinal,
lung
Table 1
BASIC SCIENCE
arm of chromosome 13. As with BRCA1, pathogenic variants can
occur throughout the gene and there are founder pathogenic
variants in some populations including the 6174delT mutation in
Ashkenazi Jews.
Cancer risks
Pathogenic variants in these genes show incomplete penetrance
(i.e. some people who carry a pathogenic variant will not develop
cancer). Pathogenic variants in the BRCA1 gene are particularly
associated with an increased risk of early onset breast cancer,
ovarian cancer and fallopian tube cancer. The lifetime risks of
developing breast and ovarian cancer for a woman with a BRCA1
pathogenic variant are usually quoted as about 85% and 40%
respectively. The risks for a woman with BRCA2 pathogenic
variants may be a little lower, particularly the ovarian cancer
risk, which is probably less than 20%. Pathogenic variants in
BRCA2 are also associated with pancreatic cancer, sarcoma and
malignant melanoma. Male carriers of BRCA pathogenic variants
have an increased risk of prostate cancer, and those with BRCA2
pathogenic variants also have a significantly increased lifetime
risk of developing breast cancer of about 6%.
The breast cancers associated with BRCA1 tend to be high-
grade, triple-negative (oestrogen receptor (ER)-, progesterone
receptor (PR)- and human epidermal growth factor receptor 2
(HER2)-negative) tumours. The pathological spectrum of BRCA2
breast cancers is broadly similar to those of non-carriers.
Management
The first step in managing a person who is concerned about her
risk of developing breast cancer is to take a family history.
Although it is important to ask about both the maternal and
paternal relatives, each side of the family should be considered
separately. Not everyone with a family history of breast cancer
will have an increased risk of developing the disease. Where
appropriate, referral can be made to their local regional genetics
service for risk assessment, counselling, advice about screening
programmes and sometimes genetic testing. Many regional
genetics services have local referral guidelines that help to
identify who should be referred. Although there may be some
regional variations, it is reasonable to consider making a referral
if a person has:
SURGERY 31:1 2
� one first-degree relative with breast cancer diagnosed
before age 40
� two first- or second-degree relatives with breast cancer
diagnosed before age 60
� three or more first- or second-degree relatives with breast
cancer at any age
� a close relative with bilateral breast cancer
� a close male relative with breast cancer
� a close relative affected by breast and ovarian cancer.
Most referral guidelines, such as those above, assume the person
being referred is not themselves affected by a relevant cancer. An
easy way to adapt such guidelines for a person who has been
affected by cancer is to imagine that person has a twin sister and
ask whether that twin sister warrants referral.
If the family history is complex and involves other types of
cancer such as ovarian cancer, prostate cancer, sarcoma, glioma
or adrenocortical carcinoma, it is best to refer to the local
guidelines or contact the regional genetics service directly.
Risk assessment
On receipt of a referral, the genetics team will gather detailed
information about the family history and draw up a family tree or
pedigree. In many cases this will involve confirming diagnoses
by reviewing medical records, pathology reports and cancer
registry records. The next step is a formal risk assessment, often
facilitated by the use of computer programmes that estimate
either the BRCA1/BRCA2 pathogenic variant carrier probabilities
or breast/ovarian cancer risks, such as BOADICEA.2
Patients will be assigned to one of three risk categories for
breast cancer:
� Women at or near population risk of developing breast
cancer (i.e. a 10-year risk of less than 3% for women aged
40e49 years and a lifetime risk of less than 17%) e these
women can be managed in primary care and do not require
any additional screening other than that offered to all
women i.e. 3-yearly mammograms from about the age of
50 through the NHS breast screening programme.
� Women at raised risk of developing breast cancer (i.e. a 10-
year risk of 3e8% for women aged 40e49 years or a life-
time risk of �17% but <30%) e these women may not be
seen in their local genetics clinic but will be offered
screening in secondary care or as part of a regional or
national screening programme for women with a family
history of breast cancer.
� Women at high risk of developing breast cancer (i.e. a 10-
year risk of >8% for women aged 40e49 years or a lifetime
risk of �30% or a �20% chance of a BRCA1, BRCA2 or
TP53 pathogenic variant in the family) e these women
should be seen in their local genetics clinic for discussion
about screening programmes and, where appropriate,
genetic testing and risk-reducing surgery.
Breast screening
Breast cancer screening for women with a family history should
be offered in accordance with the NICE guidelines on familial
breast cancer.3 Women in the raised risk group or higher should
be offered annual mammographic surveillance from age 40 years
and then 3-yearly screening from 50 years. Annual MRI
� 2013 Elsevier Ltd. All rights reserved.

BASIC SCIENCE
surveillance should be offered to women aged 30e49 years who
are known to have a BRCA1 or BRCA2 pathogenic variant and
women aged 20 years or older who are TP53 pathogenic variant
carriers (i.e. LieFraumeni syndrome). MRI surveillance is also
indicated in certain other high-risk situations which are detailed
in the NICE guidance.
Genetic testing
When the family history is suggestive of a BRCA pathogenic
variant, genetic testing can be undertaken. Ideally, this is per-
formed on DNA extracted from a blood sample of a family
member affected by a BRCA related cancer. The clues in the
family history that are suggestive of a pathogenic variant include:
� multiple individuals on one side of the family with breast
or ovarian cancer
� a young average age of diagnosis
� male breast cancer
� associated cancers (e.g. prostrate cancer, sarcoma,
pancreatic cancer)
� individuals with more than one primary cancer, including
bilateral breast cancer
� Ashkenazi Jewish ancestry.
In most laboratories both genes will be sequenced to identify
point mutations or small deletions, and MLPA (Multiplex
Ligation-dependent Probe Amplification) will be performed to
look for deletions or duplications of one or more whole exons.
If a pathogenic variant is identified in either gene, unaffected, at-
risk familymembers canbe offered predictive testing to clarify their
risks. Predictive testing should only be undertaken in regional
genetics centreswith appropriate pre-test andpost-test counselling.
Risk-reducing surgery in unaffected BRCA pathogenic variant
carriers
Some women at high risk of breast or ovarian cancer want to be
more proactive in managing their risk and request risk-reducing
surgery as an alternative to regular surveillance. The two options
available to these women are mastectomy and bilateral salpingo-
oophorectomy (BSO).4 Risk-reducing mastectomy in BRCA path-
ogenic variant carriers reduces the risk of breast cancer by around
95%. Ideally, women considering risk-reducing mastectomy
should be seen and assessed by a multidisciplinary team who can
assist in the decision making process. They need appropriate
counselling and sufficient time to weigh up the advantages,
namely a reduced risk of breast cancer and the alleviation of
anxiety, and the disadvantages, which include the risk of surgical
complications and possible psychological problems.
BSO in BRCA pathogenic variant carriers reduces the risk of
ovarian cancer by approximately 90% and will reduce a wom-
an’s risk of developing breast cancer by up to 50%, depending on
her age at the time of the procedure. The effects of the surgically
induced menopause can be alleviated by the use of hormone
replacement therapy (HRT). The decision to use HRT will depend
on a woman’s personal circumstances. Although HRT is known
to be associated with an increased risk of breast cancer, it
SURGERY 31:1 3
appears that the use of HRT does not reverse the reduction in
breast cancer risk in these women. The effectiveness of screening
for ovarian cancer remains unproven.
Medical management of affected BRCA pathogenic variant
carriers
The BRCA status of women affected by cancer is increasingly
impacting on how they are treated.5 Female pathogenic variant
carriers who have had breast cancer, have a significantly higher
risk of developing a second breast cancer in the contralateral
breast (approximately 25% compared to 10% in non-carriers).
This raises the question whether a risk-reducing contralateral
mastectomy should be performed, possibly as part of the initial
surgical procedure. There is no evidence that BRCA pathogenic
variant carriers are more radiosensitive than the general pop-
ulation, in terms of response or toxicity. There is pre-clinical
evidence that BRCA associated tumours may be more sensitive
to certain chemotherapy drugs and this is currently being tested
in large scale clinical trials.
Advances in the understanding of the biological function of
BRCA 1/2 encoded proteins have led to the development of tar-
geted therapies, which are currently in clinical trials.6 The
BRCA1 and BRCA2 proteins are involved in DNA repair. The
poly(ADP-ribose) polymerase (PARP) proteins also have impor-
tant roles in DNA repair. Inhibiting PARP in the presence BRCA
deficiency leads to cell death but PARP inhibition in cells with
normal BRCA function is well tolerated. The concept that the
mutation or inhibition of two pathways can lead to cell death,
when mutation or inhibition of either alone would not, is termed
synthetic lethality. PARP inhibitors have been tested in clinical
trials in patients with BRCA-related cancers and have shown very
encouraging results in phase 1 and II trials. However, the results
of larger phase III studies have been mixed and considerable
work remains to define the role of PARP inhibitors. A
REFERENCES
1 Gage M, Wattendorf D, Henry LR. Translational advances regarding
hereditary breast cancer syndromes. J Surg Oncol 2012; 105: 444e51.
2 Antoniou AC, Cunningham AP, Peto J, et al. The BOADICEA model of
genetic susceptibility to breast and ovarian cancers: updates and
extensions. Br J Cancer 2008; 98: 1457e66.
3 National Institute for Health and Clinical Excellence. Familial breast
cancer: the classification and care of women at risk of familial breast
cancer in primary, secondary and tertiary care. NICE Clinical Guideline
41: London, UK; 2006. http://guidance.nice.org.uk/cg41/guidance/pdf/
English.
4 Nathanson KL, Domchek SM. Therapeutic approaches for women
predisposed to breast cancer. Annul Rev Med 2011; 62: 295e306.
5 Trainer AH, Lewis CR, Tucker K, Meiser B, Friedlander M, Ward RL. The
role of BRCA mutation testing in determining breast cancer therapy.
Nat Rev Clin Oncol 2010; 7: 708e17.
6 Kummar S, Chen A, Parchment RE, et al. Advances in using PARP
inhibitors to treat cancer. BMC Med 2012; 10: 25.
� 2013 Elsevier Ltd. All rights reserved.





























