Embed Size (px)
Citation preview

DISEASES OF THE AORTA 0733-8651199 $8.00 + .OO
THE GENETIC BASIS OF AORTIC DISEASE
Marfan Syndrome and Beyond
Petros Tsipouras, MD, and David I. Silverman, MD
In 1896, Antoine Marfan described doli- chostenomelia, probably the most characteris- tic clinical sign of the condition bearing his
Ironically, the patient originally de- scribed by Marfan was probably not affected by the disorder we now call Marfan syndrome. The protean cardiovascular manifestations of Marfan syndrome, including aortic dilatation and dissecting aneurysm, were first described in 1943:~~~ The natural history, clinical hetero- geneity, and differential diagnosis of the dis- order have been extensively studied. Treat- ment of Marfan syndrome has evolved from managing catastrophic cardiovascular events to the prevention of these events by pharma- cologic treatment with P-adrenergic receptor antagonists and preemptive surgical interven- tion for valvular and aortic disease. Variabil- ity of clinical expression is the hallmark of Marfan syndrome and is observed both within and between families.& Between 1990 and 1992, the chromosomal localization, de- termination of immunohistochemical and bio- chemical phenotype, isolation and cloning of
Supported in part by the National Institutes of Health General Clinical Research Center Grant MOlRR06192, NIH HD-22610.
the FBNZ gene, and identification of FBNZ gene mutations of Marfan syndrome were achieved and described in several publica- t ion~.~ , 22, 27, 34, 59 To date, well over 100 muta- tions have been identified in individuals af- fected with Marfan syndrome and other Marfan-related phenotypes, such as MASS (mitral valve prolapse, aortic dilatation, and - skin and Skeletal manifestations), isolated ec- topia lentis, annuloaortic ectasia, and neona- tal Marfan syndrome.1° Together, these phe- notypes define a spectrum of clinically overlapping conditions, called fibrillinopathies, that are causally linked to mutations in the FBNl gene. To date, however, no definite phenotype-genotype correlation has emerged between the topology of the defect within the protein molecule and the clinical syn- drome.'O
MOLECULAR BASIS OF MARFAN SYNDROME
With the linking of the FBNZ gene to Mar- fan syndrome, the molecular basis of the dis- ease was finally defined.9, 27, 59 The FBNl gene,
From the Departments of Pediatrics (PT) and Medicine (DIS), John Dempsey Hospital, University of Connecticut Health Center, Farmington, Connecticut
CARDIOLOGY CLINICS OF NORTH AMERICA
VOLUME 17 NUMBER 4 NOVEMBER 1999 683

684 TSIPOURAS & SILVERMAN
which is localized on chromosome 15,27 en- codes the fibrillin-1 protein, a major structural component of elastin-associated mi~rofibrils.~~ Immunofluorescence studies using antifibril- lin monoclonal and polyclonal antibodies have demonstrated abnormalities of elastin- associated microfibrils in cultured skin fibro- blasts and skin obtained from affected indi- viduals.22 The role and function of microfibrils are discussed later.
Elastin-Associated Microfibrils
The term microfibrils was originally used to identify morphologically similar matrix struc- tures displaying a diameter of less than 20 nm and lacking the characteristic 67-nm banding periodicity of interstitial collagen fibers.30 Currently, microfibrils are divided into two classes according to their average diameter. The larger of the two classes has an average diameter of 10 nm and is commonly referred to as the elas tin-associated mi~rof ibr i l .~~ Immu- nohistochemical studies have identified mi- crofibrils in the suspensory ligament of the lens, pleura, perichondrium, periosteum, me- ninges, aorta, cartilage, tendon, muscle, and many other 1 5 z 3 1 The complete macro- molecular composition of the microfibril is as yet unclear because its elucidation is made difficult by the highly insoluble nature of the matrix aggregate. The main protein compo- nent of the microfibril, however, seems to be fibrillin-1. The microfibrils form a meshwork in the various tissues into which elastin is, in many instances, embedded." 50 In the wall of the proximal aorta, the presence of the elastin- associated microfibrillar network gives the or- gan its elasticity and facilitates its function as an auxiliary pump.
Fibrillin-1 is an acidic glycoprotein with an estimated molecular mass of 350 kD.I5, 31 A closely related protein, fibrillin-2, has also been identified and characterized. Fibrillin-1 has an unusually high cysteine content (14%), one third of which has the potential to form disulfide bonding.38 In vitro studies suggest that fibrillin-1 is synthesized as the precursor profibrillin and converted to the mature form following secretion into the extracellular ma- trix. Study of the biosynthesis of fibrillin has
shown that molecules are rapidly incorpo- rated into a high-molecular-weight aggregate, supporting the notion that fibrillin-1 does not exist as an extracellular m0nomer.4~ The struc- ture of the fibrillin-1 protein is complex and redundant. Much of the molecule is com- posed of a series of epidermal growth factor- like sequences, 46 of which are tandemly re- peated and irregularly interspersed among eight cysteine transforming growth factor+ binding, protein-like domains.
FBNl Gene and Mutations
The FBNZ gene is approximately 110 kb in length, and the coding information is distrib- uted in 65 ex on^.^^ More than 100 FBNl gene mutations have been identified in individuals affected with Marfan syndrome.'O Almost all of the mutations are specific to a particular individual or family, and they are distributed throughout the gene, with no obvious correla- tion between location and phenotypic sever- ity, apart from an apparent clustering of mu- tations causing neonatal Marfan syndrome in the middle of the Most mutations are missense point mutations, but small, in- frame deletions or insertions, premature ter- mination codons, and larger mutations have also been detected. Protein studies using cul- tured skin fibroblasts have shown that the FBNZ mutations cause abnormalities in the synthesis and extracellular matrix deposition of fibrillin. Although the effects of FBNZ gene mutations in fibrillin homeostasis form a con- tinuum, a categorization of the biochemical findings has recently emerged.' Substantially decreased amounts of deposited fibrillin in the extracellular matrix are associated with more severe cardiac complications and aortic surgery at an earlier age.' In contrast, higher levels of deposited fibrillin have been de- tected in patients with phenotypically milder Marfan syndrome or Marfan-related disor- ders, including ectopia lentis, MASS, or annuloaortic ectasia.'
DIAGNOSIS
Marfan syndrome is a systemic disorder of connective tissue, the diagnosis of which is

THE GENETIC BASIS OF AORTIC DISEASE 685
based on well-defined diagnostic criteria. The disease has been reported in all races and in multiple ethnic groups. The prevalence of the Marfan syndrome has been estimated to be approximately 4 to 6 per 100,000 US popula- tion, which may be an ~nderestimate.~~ Given that a positive family history for the Marfan syndrome can be found in no more than 70% of affected individuals, the rate of new muta- tions is believed to be high. Correct clinical diagnosis depends on the recognition of phe- notypic manifestations correlated with family and genetic history (see box).
Diagnostic Requirements for Marfan Syndrome
A. lndexcase 1. If family or genetic history is not
contributory Major criteria in at least two
different organ systems Involvement of a third organ
system 2. If the mutation known to cause
Marfan syndrome in others is detected
One major criterion in an organ
Involvement of a second organ
Presence of a major criterion in the
Major criterion in an organ system Involvement of a second organ system
system
system
family history
B. Relative of index case
A list of major and minor criteria has been defined for each one of the following systems: skeletal, cardiovascular, ocular, pulmonary, skin and integument, dura, and family and genetic history (Table 1).
an arm span-to-height ratio of more than 1.05.6, 6o Arachnodactyly, determined by the wrist and thumb signs, is another historically identified physical sign. The wrist sign of Walker and Murdoch is present when the thumb and little finger, clasped around the wrist, overlap appreciably. Steinberg's thumb sign is present when the thumb apposed across the palm extends so that the bony tip of the distal phalanx extends clearly beyond the ulnar margin of the hand.49, 6o The thumb or wrist signs are positive in approximately 75% of individuals affected with the Marfan syndrome and in 1% to 2% of normal people.6 Anterior chest wall deformities in the form of pectus carinatum (pigeon breast), pectus excavatum, scoliosis of more than 204 spon- dylolisthesis, reduced extension of the elbows (< 170"), pes planus, and protrusio acetabuli (diagnosed by radiography of the pelvis) are some common, specific skeletal signs of Mar- fan syndrome.6
Ocular Manifestations
Sixty percent of individuals with Marfan syndrome have ectopia lentis.6 The disloca- tion of the lens can be unilateral or bilateral and can occur in any direction, although su- perior displacement is the usual finding. Al- though ectopia lentis is a highly specific man- ifestation, it also appears as an isolated finding segregating in families without other extraocular manifestations of Marfan syn- d r ~ m e . ~ ~ Abnormally flat cornea, increased axial length of the globe, and hypoplastic iris are additional primary clinical manifestations of Marfan syndrome,6, 45 but myopia, amblyo- pia, glaucoma, cataracts, and retinal detach- ment are also common findings6, 45
Cardiovascular Manifestations Skeletal Manifestations
Dolichostenomelia is one of the constant findings on physical examination in patients with Marfan syndrome. Dolichostenomelia is manifested as either a reduction of the upper- to-lower segment ratio (< 0.85 in Caucasians and < 0.78 in people of African descent) or
Structural cardiovascular abnormalities oc- cur in more than 80% of individuals affected with Marfan syndrome.6, 45 The most common manifestations include dilatation of the as- cending aorta involving at least the sinuses of Valsalva, aortic regurgitation, ascending aortic dissection, and mitral valve prolapse

686 TSIPOURAS & SILVERMAN
Table 1. CLINICAL MANIFESTATIONS
Diagnostic Criteria
System Major Minor
Skeletal system pectus carinatum pectus excavatum requiring surgery reduced upper-to-lower segment ratio or
arm span-teheight ratio greater than 1.05
wrist and thumb signs scoliosis of > 20" or spondylolisthesis reduced extension at the elbows (< 170") medial displacement of the medial
malleolus causing pes planus protrusio acetabulae of any degree
(ascertained on radiographs)
pectus excavatum of moderate severity joint hypermobility highly arched palate with crowding of
teeth facial appearance (dolichocephaly,
malar hypoplasia, down-slanting palpebral fissures, retrognathia)
enophthalmos
For skeletal system to be considered involved, at least 2 of the components comprising the major criterion or 1 component
Ocular system ectopia lentis abnormally flat cornea
comprising the major criterion plus 2 of the minor criteria must be present.
increased axial length of globe hypoplastic iris or hypoplastic ciliary
muscle
For ocular system to be involved, at least 2 of the minor criteria must be present.
Cardiovascular system dilatation of the ascending aorta with or mitral valve prolapse with or without
dilatation of the main pulmonary
calcification of mitral annulus dilatation or dissection of the
without aortic regurgitation and involving at least the sinuses of Valsalva artery
mitral valve regurgitation
dissection of the ascending aorta
descending thoracic or abdominal aorta
For the cardiovascular system to be involved, a major criterion or only one of the minor criteria must be present.
Pulmonary system none spontaneous pneumothorax, or apical blebs (ascertained by chest
radiography)
For the pulmonary system to be involved, one of the minor criteria must be present.
Skin and integument none striae atrophicae (stretch marks) not associated with marked weight changes, pregnancy, or repetitive stress, or
recurrent or incisional herniae
For the skin and intexument to be involved, one of the minor criteria must be present.
Dura lumbosacral dural ectasia by CT or MR none image
For the durn to be involved, the major criterion must be present.
Family/ Genetic History having parent, child, or sibling who none meets these diagnostic criteria independently
presence of mutation in FBN1, known to cause Marfan syndrome; or
presence of haplotype around FBNl inherited by descendent known to be associated with unequivocally diagnosed Marfan syndrome in the family
For the familylgenetic history to be contributory, one of the major criteria must be present.

THE GENETIC BASIS OF AORTIC DISEASE 687
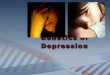
Figure 1. Large (7 cm) aneurysm of the ascending thoracic aorta in an asymptomatic 24-year-old man. The patient underwent successful aortic valve and root replacment.
with or without mitral valve regurgitation. The utility of echocardiography for detecting the cardiovascular manifestations of Marfan syndrome has made it a requisite component of both initial diagnostic evaluation and long- term follow-up. Alternative imaging tech- niques, including MR imaging, CT scanning, and transesophageal echocardiography (TEE), allow for the noninvasive or semi-invasive identification of abnormalities of the more distal aorta and its branches.
The prevalence of different cardiac manifes- tations and complications of Marfan syn- drome varies with age. Among children with the syndrome, mitral valve prolapse and se- vere mitral regurgitation are the most com- mon cardiac manifestations. In adults, aortic root dilatation, aortic regurgitation, and aortic dissection predominate. Neonatal Marfan syndrome, which most often occurs as a de nozm mutation, usually includes severe (and frequently fatal) mitral and aortic valve involvement.
Aortic Root Enlargement
Dilatation of the aortic root is diagnosed when the maximum diameter at the sinuses of Valsalva, as measured by echocardiogra- phy CT scan, or MR imaging, exceeds estab- lished limits for age and body surface area
(Fig. 1). Enlargement of the aortic root in pa- tients with Marfan syndrome is most com- mon and most marked at the level of the sinuses of Valsalva. More than 50% of chil- dren (excluding those with neonatal Marfan syndrome) and approximately 80% of af- fected adults demonstrate aortic root dilata- tion. Despite the age-related increase in the prevalence of aortic enlargement in longitudi- nal studies, few individuals affected with Marfan syndrome maintain normal aortic root diameters after age 60 years.
Although aortic enlargement is restricted to the sinuses of Valsalva in some affected individuals, dilatation more commonly ex- tends into the ascending aorta and distal seg- ments. Patients affected with the Marfan syn- drome whose dilatation is limited to the sinuses of Valsalva experience a more benign, short-term clinical course compared with those with generalized aortic enlargement.49, 57
Enlargement of distal aortic segments (i.e., the arch, descending thoracic, and abdominal aorta) and of medium-sized arteries, such as the iliac or carotid artery, may occur alone or in combination but seldom occurs in the absence of aortic root involvement. Dissecting aneurysm in the presence of modest aortic dilatation (< 5 cm in diameter) breeds true in families.57 As such, a family history of dissec- tion, despite minimal aortic dilatation, consti-

688 TSIPOURAS & SILVERMAN
tutes a significant risk factor in the assess- ment and ongoing management of affected relatives with Marfan
Dissection of the Aorta
Patients with aortic dissection classically present with severe midline pain in the front or back of the chest or abdomen, but rela- tively small dissections within the ascending aorta may occur in the absence of a clinically recognized pain syndrome and are subse- quently detected during elective surgical re- pair. Aortic dissection should be documented by TEE, CT, or MR imaging. Most aortic dis- sections in patients with Marfan syndrome arise in the proximal aorta and extend through a variable portion of the aorta and its branches, but dissection can also begin in more distal aortic segments.
Aortic Regurgitation
Among patients with Marfan syndrome, aortic regurgitation is relatively uncommon in childhood but increases in prevalence with age. Aortic regurgitation occurs rarely in pa- tients with Marfan syndrome who have nor- mal-sized aortic roots but becomes increas- ingly common as the aortic root size increases. As with aortic dilatation in patients with other disorders, the points of attachment of the aortic cusp to the aortic wall are pro- gressively displaced away from the center of the aorta (at the sinotubular junction), and ultimately the leaflets fail to coapt adequately. As with patients without Marfan syndrome but with aortic dilatation, color and continu- ous wave Doppler flow imaging are the tech- niques of choice for diagnosis and quantifica- tion of severity of aortic regurgitation.
Mitral Valve Prolapse
Mitral valve prolapse (MVP) occurs in 50% to 60% of individuals affected with the Mar- fan syndrome,6 but primary MVP is 400 times more common in the general population than in patients with Marfan syndrome-related MVP. The diagnosis of MVP should be estab- lished following stringent criteria, including late systolic prolapse of more than 3 mm on
M-mode echocardiography.8 Computed two- dimensional echocardiography has identified a unique pattern of MVP in individuals af- fected with Marfan syndrome in which all visible chordae attached to the posterior mi- tral leaflet arise directly from the posterior left ventricular wall and not from the postero- medial papillary muscle.40
Manifestations from Other Systems
Spontaneous pneumothorax occurs in ap- proximately 5% of individuals affected with Marfan syndrome.18 Apical blebs detected by chest radiography are commonly found in affected individuals. Pectus excavatum or scoliosis can cause a marked restrictive venti- latory defect that may improve following pec- tus repair. Striae atrophicae, preferentially lo- calized on the shoulders, flank, or thighs, and recurrent or incisional herniae are common skin manifestations. Lumbosacral dural ecta- sia evaluated by MR imaging or CT scanning can be diagnosed in probably more than 40% of individuals affected with Marfan syn- drome.44 Dural ectasia is associated with en- largement of the neural canal, thinning of the cortex of the pedicles and laminae of the vertebrae, and widening of the neural forami- naeM and is usually manifested as persistent lower back pain.
NEONATAL MARFAN SYNDROME
Although infants and young children were among the first patients in whom Marfan syn- drome was documented, recognition of the disorder in early life is often difficult. Some infants, however, present with striking and severe clinical manifestations and exhibit a characteristic aged facial appearance caused by deep-set eyes, down-slanted palpebral fis- sures, highly arched palate, striking arachno- dactyly of fingers and toes, pectus deformi- ties, scoliosis, flexion contractures, pes planus, multivalvular involvement, aortic root dilatation, and ectopia l e n t i ~ . ~ ~ This strik- ing phenotypic presentation is also described as infantile or neonatal Marfan syndrome. Flexion contractures and scoliosis are clinical

THE GENETIC BASIS OF AORTIC DISEASE 689
manifestations in congenital contractural ar- achnodactyly (Beals syndrome), a phenotypi- cally similar disorder that, unlike Marfan syn- drome, does not involve the cardiovascular or ocular systems.37 The cardiovascular mani- festations of neonatal Marfan syndrome often are refractory to medical or surgical treatment and lead to congestive heart failure with early mortality.35
DIFFERENTIAL DIAGNOSIS
Several disorders phenotypically overlap with the Marfan syndrome, but are distinct entities. These include:
Homocystinuria-Several inborn errors of metabolism result in elevated plasma levels of methionine and homocysteine. Deficiency of the enzyme cystathionine p- synthase produces this disorder. Doli- chostenomelia, osteoporosis, mental re- tardation, seizures, psychosis, ectopia lentis, and premature atherosclerosis are several of the manifestations associated with homocys t in~r ia .~~ The life expec- tancy of patients with this disorder is se- verely reduced. Accurate diagnosis is es- sential because some individuals may benefit from vitamin B, supplementation therapy. Congenital contractural arachnodacty- ly-Also known as Beak syndrome, this condition has a benign course?O, 37 It is characterized by dolichostenomelia, ar- achnodactyly, scoliosis, flexion con- tractures that improve with age, and ab- normalities of the external ear.37 Familial thoracic aortic aneurysm-Also described as annuloaortic ectasia and fa- milial aortic dissection, is considered by some to be a single entity, but clinical experience suggests that dissection of the ascending aorta occurs in some families without marked prior di1atati0n.l~. 53 To make the diagnosis of familial annuloaor- tic ectasia, aortic involvement must be present in at least two related individuals. Other systems are not involved. Annul- oaortic ectasia is inherited as an autoso- ma1 dominant trait. The natural history of
the aortic disease in patients with annu- loaortic ectasia parallels that observed in the Marfan syndrome, although some ob- servers believe that aortic disease in pa- tients with annuloaortic ectasia follows a milder course. In the authors' clinical practice, patients with annuloaortic ecta- sia are managed in a manner similar to that for those with Marfan syndrome, in- cluding regular surveillance of aortic root size by echocardiography, avoidance of contact sports and isometric exercise, and prophylactic medical treatment with p- adrenergic receptor antagonists. MASS phenotype-Many individuals re- ferred with the diagnosis of Marfan syn- drome do not meet the diagnostic criteria of Marfan syndrome but nonetheless present with clinical signs suggestive of a systemic disorder of connective tissue. Many such individuals are affected with a phenotypically similar condition, MASS.16 In addition to MVP, these individuals of- ten present with mild aortic dilatation (usually < 2 standard deviations more than the expected diameter); myopia; striae atrophicae; pectus excavatum; joint hypermobility; highly arched palate with crowding of teeth; and a facial appear- ance characterized by dolichocephaly, malar hypoplasia, enophthalmos, retro- gnathia, and down-slanting palpebral fissures.I6 The MASS phenotype clinically overlaps with that of Marfan syndrome but should not be considered either as a prodromal state leading to Marfan syn- drome, or alternatively, as a forme fruste of it. The MASS phenotype is inherited as an autosomal dominant trait, and muta- tions in the FBNZ gene have been identi- fied in several affected individuals.l0 Dif- ferentiating Marfan syndrome from MASS, however, has important implica- tions in terms of both natural history and management. Although the cardiovascu- lar manifestations in patients with MASS are not as accurately delineated as in those with Marfan syndrome, significant aortic dilatation, regurgitation, or dis- secting aortic aneurysm have not been reported to date. The authors perform regular echocardiographic assessment of

690 TSIPOURAS & SILVERMAN
aortic root size for patients diagnosed with MASS but refrain from initiation of prophylactic therapy with P-adrenergic receptor antagonists as a matter of course. The management of the remaining patho- logic manifestations associated with MASS is symptomatic. Familial MVP syndrome-This syn- drome clinically overlaps with MASS. This diagnosis has been used to describe individuals whose primary manifestation is MVP, but other skeletal abnormalities are also found, including mild scoliosis and pectus ex~avatum.~ The phenotypic distinction between MASS and MVP syn- drome is tenuous, and these two condi- tions may represent two ends of a pheno- typic spectrum. Families showing an autosomal dominant mode of inheritance have been de~cribed.~ The symptomatic management of patients with MVP is out- lined in another section of this article. Familial ectopia lentis-Several families have been described in whom ectopia lentis is inherited as an autosomal domi- nant trait and is the predominant (al- though not exclusive) clinical feature.59 Although no cardiovascular involvement exists, skeletal features consistent with those of patients with Marfan syndrome might be found in some affected individ- uals." Marfan-like connective tissue disor- der-This condition, described in a large French pedigree, consists of dilatation of the ascending aorta, aortic dissection, MVP, and skeletal features consistent with those of patients with Marfan syn- d r ~ m e . ~ Clinically, this phenotype resem- bles MASS with the exception of aortic dissection. Genetic linkage studies, how- ever, have excluded mutations in the FBNl gene and set this phenotype apart from the Marfan syndrome and the MASS phenotype. Stickler syndrome-Patients with this multisystem genetic disorder present with high myopia, vitreoretinal degenera- tion, retinal detachment, deafness, ar- thropathy, mild spondyloepiphyseal dys- plasia, joint hypermobility, midfacial hypoplasia, micrognathia, highly arched
palate, and MVP.58 Minimum diagnostic criteria include involvement of the eye, craniofacies, and at least one other sys- tem. Many individuals affected with Stickler syndrome have a habitus reminis- cent of the Marfan syndrome.
LABORATORY DIAGNOSIS
The delineation of the molecular basis of Marfan syndrome and other fibrillinopathies has not led to the development of a single laboratory test that can be used as a compan- ion to diagnosis by physical examination. Ge- netic linkage analysis, FBNZ gene mutation analysis, fibrillin biochemical studies, and fi- brillin immunofluorescence studies are per- formed in few specialized laboratories and provide variable levels of sensitivity and specificity. The previous types of laboratory analysis can be used in a clinically relevant manner but are not routine diagnostic tests.
Genetic Linkage Analysis
Genetic linkage analysis is based on follow- ing the segregation of intragenic FBNl mark- ers within a family and correlates with the inheritance of the disorder. Such analysis is not technically challenging and can be per- formed with a short turnaround 59 but affected relatives must be available for the analysis to be performed. Genetic linkage analysis has been used in the prenatal diagno- sis of Marfan syndrome to predict whether a fetus is affected.25
FBNl Gene Mutation Analysis
Although FBNl gene mutation analysis can be performed from either a blood specimen or skin biopsy, such analysis is made cumber- some by the large size of the gene, its complex structure, and the absence of a predominant mutation in the population. Despite these technical limitations, mutation analysis is the only test that can establish the causative link between the gene and the disorder. The vari- able levels of sensitivity provided by different

THE GENETIC BASIS OF AORTIC DISEASE 691
mutation screening methods can be resolved by sequencing the entire coding sequence of the gene,26 but FBNl gene mutation detection is not specific for Marfan syndrome because such mutations can be found in patients with Marfan-related disorders.'O Therefore, muta- tion analysis is clinically meaningful only within the context of diagnosis by physical examination, as mentioned elsewhere in this article. Identification of an FBNl gene muta- tion can also be used for prenatal diagnostic purposes.
Fibrillin Biochemical Studies
Fibrillin biochemical studies can determine whether synthesis or deposition of fibrillin occurs,within the extracellular matrix but are sometimes difficult to interpret and require cultured skin fibroblasts obtained by skin bi- opsy.' Because the fetal cell types obtained through chorionic villus biopsy or amniocen- tesis do not synthesize fibrillin, biochemical studies performed on these cell types cannot be used for prenatal diagnostic purposes.
Fibrillin lmmunofluorescence Studies
Fibrillin immunofluorescence studies quali- tatively assess the extracellular matrix deposi- tion of fibrillin in cultured skin fibroblasts using fluorescently tagged antifibrillin anti- bodies2* Because the sensitivity of this test varies with the experimental conditions, its value as a diagnostic test remains limited.
NATURAL HISTORY
The clinical course of Marfan syndrome is characterized by progression. Other than doli- chostenomelia and arachnodactyly, manifes- tations from other organ systems are usually not present at birth, making the diagnosis during the neonatal period difficult in the absence of a positive family history. Skeletal manifestations become apparent during childhood, and pectus deformities and scolio- sis worsen during puberty. The characteristic skeletal build, in association with the relative
muscular hypoplasia, gives the appearance of an asthenic habitus in affected individuals early in life. Neither ectopia lentis nor lens subluxation is present at birth, but both are commonly diagnosed during the first year of life. Lumbosacral dural ectasia, manifested as progressive dilatation of the dura with conse- quent erosion of vertebral bone, is another manifestation detected in adulthood that fur- ther underscores the progressive nature of Marfan syndrome.
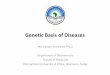
Aortic root size normalized for age and body surface area is larger than normal or at the upper range of normal in early childhood, and the magnitude of dilatation increases markedly during puberty. Before the avail- ability of advanced surgical techniques for aortic repair and replacement, aortic disease was the major cause of cardiovascular mor- bidity and reduced life e~pectancy.~~ From a group of patients followed up at Johns Hop- kins University, Murdoch et a136 initially esti- mated life expectancy in affected individuals at 32 k 16 years and reported that most deaths were secondary to cardiovascular causes. Subsequent advances in medical and surgical treatment of the disease have pro- duced a profound improvement in this rather sobering death rate. In a cohort of more than 400 patients gathered from four centers for the treatment of Marfan syndrome, the au- thors reported an increase in the life expec- tancy of nearly 10 years, to 41 & 18 years (Fig. 2).56 This substantial improvement may be attributed to a dramatic increase in suc- cessful elective and emergent aortic surgery (discussed in detail elsewhere in this issue) and to the use of f3-adrenergic receptor antag- onists for the prevention of the progression of aortic root dilatation. The survival advantage gained by surgery seems to have increased significantly for patients undergoing opera- tion after 1980.56 In contrast to patients with ischemic heart disease, women afflicted with the syndrome enjoy a greater survival advan- tage compared with men.56
MANAGEMENT
The clinical management of individuals with Marfan syndrome requires a coordinated

692 TSIPOURAS & SILVERMAN
194
- m > .- 2 a tn
0.60
0.50 1 0.40 1,/ 0.10
i 1 I
i. -- I I
01 I I I I I I 1 I
0 10 20 30 40 50 60 70 80
AGE
Figure 2. Compari$on of the cumulative probability of survival of men with Marfan syndrome in 1972 (squares) and 1993 (circles). The numbers listed beneath the 1994 survival curve represent the number of patients alive at each decade.
effort from practitioners in a variety of spe- cialties and can be best accomplished in a multidisciplinary clinic. Such a structure is equally useful for diagnostic confirmation or exclusion.
Initial diagnostic evaluation requires the combined elements of history, family history (including construction of a pedigree); physi- cal examination; and anthropometric mea- surements (i.e., height, weight, arm span, up- per segment-to-lower segment ratio, and hand length); comprehensive ophthalmologic evaluation, including slit lamp examination; echocardiography with attention to quantita- tive aortic root assessment; determination of homocysteine levels in the plasma and urine; and, occasionally, other diagnostic tests, such as CT scanning or MR imaging. With the exception of serial echocardiographic assess- ment of the aortic root size and integrity, no defined set of diagnostic tests nor any specific interval for those tests exists. In newly diag- nosed patients, the authors obtain three serial echocardiograms at 6-month intervals to es- tablish the baseline rate of the progression of the aortic root size. For other manifestations, the authors recommend appropriate diagnos- tic workup as necessary. Because Marfan syn- drome is a chronic but progressive condition, affected individuals must be educated and
thoroughly counseled about their condition and should be encouraged to become active participants in disease management. Thus, a major component of the multidisciplinary ap- proach is providing genetic counseling for affected individuals and their families and continuous counseling and support to pa- tients and their immediate families.
Cardiovascular System
A direct relationship exists between aortic root dimension and complications of Marfan syndrome. Aortic regurgitation is virtually nonexistent in individuals whose aortic root is 3.6 cm or less but uniformly occurs in per- sons with aortic root dimensions of 6 cm or more. In 1972, McFarland et a133 first sug- gested that propranolol, a p-adrenergic recep- tor antagonist, should be included in the medical treatment of patients with dissecting aortic aneurysms. In 1983, Pyeritz41 reported for the first time the use of P-adrenergic re- ceptor antagonists to retard the rate of aortic root dilatation in patients with Marfan syn- drome. Since then, their use has become ubiq- uitous. In 1994, Shores et a155 published a landmark study that tested the hypothesis that the long-term administration of oral P-

THE GENETIC BASIS OF AORTIC DISEASE 693
adrenergic receptor antagonists would reduce the rate of aortic dilatation in patients with Marfan syndrome. The trial was an unblinded prospective study of 70 adolescent and adult patients with Marfan syndrome; 32 patients received propranolol, and 38 patients were followed up as controls. Mean follow-up was 9.3 years in the control group and 10.7 years in the treatment group. The rate of increase in aortic ratio (measured aortic diameter di- vided by expected diameter predicted for age, gender, and body surface area-adjusted no- mograms) in patients receiving propranolol was 0.023 per year compared with 0.084 per year in untreated patients. The number of clinical end points (five in the treatment group and nine in the control group) and the estimated survival time were improved in patients receiving propranolol compared with the control group. These initial data were con- firmed by Salim et a151 in a cohort of 113 patients affected with Marfan syndrome and receiving P-adrenergic receptor antagonists or placebo.51 In untreated patients, the rate of aortic dilatation was 2.1 k 1.6 mm/y com- pared with 0.7 k 1.8 mm/y and 1.1 * 1.1 mm/y in two cohorts of patients treated with either atenolol or propranolol. Data from other studies are consistent with these results.51
Retardation of aortic dilatation in these pa- tients seems to be mediated by improvement in aortic root compliance.61 Defined most sim- ply as the rate of change in aortic dimension with increasing aortic pressure, aortic root compliance can be measured noninvasively by echocardiography and MR imaging. Aortic wall stiffness, pulse wave velocity, and aortic distensibility, all of which describe compli- ance, have been reported to be increased in patients with Marfan syndrome compared with control^.'^, 21, 52 Furthermore, P-blockade seems to improve aortic compliance in pa- tients with Marfan syndrome compared with
Taken together, these data make a compelling case for administration of P- adrenergic receptor antagonists to patients with Marfan syndrome whenever possible. Given the small number of patients studied thus far, no firm recommendations can be made with regard to dose or type of P-adren- ergic receptor antagonist^,'^, 48 but common sense suggests that dose titration to a heart
rate less than 60 would provide optimal ther- apy.
Successful acceptance of P-adrenergic re- ceptor antagonist therapy may be limited by adverse effects, including bradycardia, hypo- tension, fatigue, dizziness, weakness, and im- potence. Contraindications to P-adrenergic re- ceptor antagonists include asthma; severe peripheral vascular disease; and, occasionally, diabetes. As with other long-term prophylac- tic therapies, the use of these agents can be challenging, especially in asymptomatic pa- tients requiring long-term treatment. Shores et a155 reported that one third of patients treated with P-adrenergic receptor antago- nists developed at least one side effect. Cal- cium channel inhibitors, including verapamil and diltiazem, may represent a therapeutic alternative to patients who cannot or will not take P-adrenergic receptor antagonists. To date, however, no prospective data have been published comparing the rate of aortic dilata- tion in patients affected with Marfan syn- drome given a calcium channel antagonist. A multicenter, international trial entitled ADAMS (Aortic Dilatation and Marfan Syndrome), headed by the University of Con- necticut Health Center, has been initiated for this purpose.
Moderate exercise may be encouraged in all patients affected with Marfan syndrome who can otherwise tolerate it. Restriction of physical activity is recommended for patients with more severe forms of the disease. The authors reported that patients with Marfan syndrome who have a positive family history of severe cardiovascular manifestations, in- cluding sudden cardiac death, aortic dissec- tion, or cardiothoracic surgery, demonstrate greater aortic dilatation and a longer dilated segment compared with patients with a nega- tive family history.57 In addition, a positive family history of severe cardiovascular dis- ease is associated with a decreased life span. Accordingly, the authors recommend in- creased vigilance for such patients, with fre- quent echocardiographic surveillance and a low threshold for surgical intervention. In these patients, strenuous exercise should be discouraged, and isometric exercise and con- tact sports must be prohibited.
Control of hypertension, when it occurs, preferably with P-adrenergic receptor antago-

694 TSIPOURAS & SILVERMAN
nists, is essential. Increasing aortic or mitral regurgitation may be retarded through the use of angiotensin-converting enzyme inhibi- t o r ~ . ~ ~ The presence of symptomatic valvular regurgitation, or evidence of deteriorating left ventricular systolic function in asymptomatic patients, is an indication to strongly consider valve repair or replacement.%
The diagnosis of aortic dissection may be confirmed by either CT, MR imaging, or TEE. Although all three tests provide excellent sen- sitivity and specificity, the speed and portabil- ity of TEE make it an excellent choice. Aortic dissection is classified as proximal or distal according to the revised DeBakey criteria? As with non-Marfan syndrome patients, the decision for medical or surgical treatment is based on the point of origin. As a rule, dissec- tions that begin above the ligamentum arte- riosum require operation, whereas many dis- sections distal to this landmark may be amenable to medical management.41 Acute medical management of dissection in these patients is not altered by the presence of Mar- fan syndrome and requires an aggressive de- crease of the rate-pressure product, through the combined use of either parenteral p-ad- renergic receptor antagonists and sodium ni- troprusside or alternative therapeutic agents, including labetalol or trimethaphan.z8
Ocular System
Because ectopia lentis develops postnatally, it cannot be detected at birth but has been diagnosed as early as 2 months of age. A thorough ophthalmologic examination is re- quired for diagnosis. Refractory errors caused by myopia or ectopia lentis must be corrected with glasses to prevent the development of amblyopia, which may otherwise occur as the result of unequal refraction. Later in life, cata- racts, glaucoma, and retinal detachment are the most common complications. Annual or semiannual ophthalmologic evaluations are recommended.
Skeletal System
Scoliosis occasionally causes orthopedic problems in patients with Marfan syndrome.
The onset of scoliosis in infancy is common in patients with neonatal Marfan syndrome but most commonly appears in puberty. When present, progression may be rapid. Ad- olescents with scoliosis should be evaluated twice a year; progression must be docu- mented radiographically. Bracing is war- ranted when spinal curvature exceeds 20". Surgical correction, in the form of segmental fixation, fusion with a Harrington rod, and bone grafting for stabilization, has yielded good results.
Surgical correction of pectus deformities is usually warranted only for improved cos- mesis. Because significant recurrence of the sternal abnormality has been observed fol- lowing repair early in life, delaying surgery until skeletal maturity has occurred is recom- mended. Pes planus and its associated de- formities frequently cause symptoms, and hammertoes may require surgical interven- tion. Protrusio acetabuli is common in af- fected adults, but orthopedic intervention is usually not necessary.
Management of Pregnant Patients with Marfan Syndrome
In pregnant women affected with the Mar- fan syndrome, the risk for cardiovascular complications seems to be related to the pres- ence or absence of pre-existent cardiovascular disease.lZ In a series of 105 pregnancies car- ried to term (of a total of 25 women) only one severe and two mild cardiovascular complica- tions were reported. One woman with severe mitral regurgitation developed endocarditis shortly before delivery and died after deliv- e r ~ . ~ ~ Only one woman within this group, however, had a prior history of severe cardio- vascular manifestations. Other complications of pregnancy were similar to rates reported in women without Marfan syndrome, as was the rate of cesarean section. The spontaneous abortion rate was increased in women affected with Marfan syndrome. A smaller series of women affected with Marfan syndrome, but also without severe cardio- vascular manifestations, showed similar re- s u l t ~ . ~ ~ In contrast, P y e r i t ~ ~ ~ reported a fear- some complication rate in a series of 32 women, most of whom had significant pre-

THE GENETIC BASIS OF AORTIC DISEASE 695
existent cardiovascular disease. The preg- nancy-related mortality rate in this cohort was 50%, and four survivors required emer- gency aortic dissection repair. In the presence of severe cardiovascular disease, therefore, pregnancy should be strongly discouraged. Intense surveillance, including monthly echo- cardiograms beginning in the fifth month of pregnancy (or earlier if aortic dilatation i s present), is strongly recommended for women at high risk, and delivery via cesarean section should be planned electively. Antibi- otic prophylaxis for endocarditis should be provided when indicated. Overall, pregnancy earlier rather than later in life should be en- couraged.
SUMMARY
The Marfan syndrome and related disor- ders are systemic disorders of connective tis- sue. Proximal aorta is usually dilated. The molecular basis of Marfan syndrome has been elucidated, thus allowing prenatal diagnosis. Life expectancy has markedly improved due to the widespread use of P-adrenergic recep- tor inhibitors and improved surgical manage- ment of the aortic disease.
References
1. Aoyama T, Francke U, Gasner C, et al: Fibrillin abnor- malities and prognosis in Marfan syndrome and re- lated disorders. Am J Med Genet 58:169-176, 1995
2. Baer RW, Taussig HB, Oppenheimer EH: Congenital aneurysmal dilation of the aorta associated with ar- achnodactyly. Bull Hopkins Hosp 72309-331, 1943
3. Boileau C, Jondeau G, Babron MC, et al: Autosomal dominant Marfan-like connective tissue disorder with aortic dilatation and skeletal anomalies not linked to the fibrillin gene. Am J Hum Genet 53:46- 54, 1993
4. Cleary EG, Gibson MA: Elastin-associated microfi- brils and microfibrillar proteins. Int Rev Connect Tis- sue Res 10:297-309, 1983
5. Crawford ES: The diagnosis and management of aor- tic dissection. JAMA 264:2537-2541, 1990
6. DePaepe A, Devereux RB, Dietz HC, et al: Revised diagnostic criteria for the Marfan syndrome. Am J Med Genet 62417426, 1996
7. Deverew RB, Kramer-Fox R, Brown WT, et al: Rela- tion between clinical features of the “mitral prolapse syndrome” and echocardiographically documented mitral valve prolapse. J Am Coll Cardiol 8763-772, 1986
8. Devereux RB, Kramer-Fox R, Kligfield P: Mitral valve
prolapse: Causes, clinical manifestations, and man- agement. Ann Intern Med 111:305-317, 1989
9. Dietz HC, Cutting GR, Pyeritz RE, et al: Marfan syndrome caused by a recurrent de novo missense mutation in the fibrillin gene. Nature 352:337-339, 1991
10. Dietz HC, Pyeritz RE: Mutations in the human gene for fibrillin 1 (FBN1) in the Marfan syndrome and related disorders. Hum Mol Genet 41799-1809, 1995
11. Edwards MJ, Challinor CJ, Colley PW, et al: Clinical and linkage study of a large family with simple ec- topia lentis linked to FBNl. Am J Med Genet 53:65- 71, 1994
12. Elkayam U, Ostrzega E, Shotan A, et al: Cardiovascu- lar problems in pregnant women with the Marfan syndrome. Ann Intern Med 123:117-122, 1995
13. Emanuel R, Ng R, Marchomichelakis J, et al: Formes frustes of Marfan’s syndrome presenting with severe aortic regurgitation: Clinicogenetic studies of 18 fam- ilies. Br Heart J 39390-197, 1977
14. Etter LE, Glover LP: Arachnodactyly complicated by dislocated lens and death from rupture of dissecting aneurysm of the aorta. JAMA 123:88, 1943
15. Gibson MA, Kumaratilake JS, Cleary EGH The pro- tein components of the 12 nanometer microfibrils of elastic and non-elastic tissues. J Biol Chem 264:4590- 4598, 1989
16. Glesby MJ, Pyeritz RE: Association of mitral valve prolapse and systemic abnormalities of connective tissue. JAMA 262523-528, 1989
17. Groenink M, de Roos A, Mulder BJ, et al: Changes in aortic distensibility and pulse wave velocity assessed with magnetic resonance imaging following beta- blocker therapy in the Marfan syndrome. Am J Cardiol 82203-208, 1998
18. Hall JR, Pyeritz RE, Dudgeon DL, et al: Pneumotho- rax in the Marfan syndrome: Prevalence and therapy. Ann Thorac Surg 37500-504, 1984
19. Haouzi A, Berglund H, Pelikan PC, et al: Heteroge- neous aortic response to acute beta-adrenergic block- ade in Marfan syndrome. Am Heart J 133:6&63, 1997
20. Hecht F, Beals RK: “New” syndrome of congenital contractural arachnodactyly originally described by Marfan in 1896. Pediatrics 49:574-579, 1972
21. Hirata K, Triposkiadis F, Sparks E, et al: The Marfan syndrome: Abnormal aortic elastic properties. J Am Coll Cardiol 18:57-63, 1991
22. Hollister DW, Godfrey M, Sakai LY, et al: Marfan syndrome: Immunohistochemical abnormalities of elastin-associated microfibrillar fibre system. N Engl J Med 323352-159,1990
23. Jeremy RW, Huang H, Hwa J, et al: Relation between age, arterial distensibility, and aortic dilatation in the Marfan syndrome. Am J Cardiol 74:369-373, 1994
24. Kainulainen K, Karttunen L, Puhakka L, et al: Muta- tions in the fibrillin gene responsible for dominant ectopia lentis and neonatal Marfan syndrome. Nat Genet 6:64.-69, 1994
25. Kilpatrick MW, Harton GL, Phylactou LA, et al: Pre- implantation genetic diagnosis in Marfan syndrome. Fetal Diagn Ther 11:402406, 1996
26. Kilpatrick MW, Lembessis P, Rose E, et al: A novel G to A substitution at nucleotide 1734 of the FBNl gene, predicting a C534Y mutation responsible for Marfan syndrome. Hum Hered 49:176-177, 1999
27. Lee B, Godfrey M, Vitale E, et al: Linkage of Marfan syndrome and a phenotypically related disorder to two different fibrillin genes. Nature 352330-334,1991
28. Lindsay J: Aortic dissection. In Hurst JW (ed): Cur-

696 TSIPOURAS & SILVERMAN
rent Therapy in Cardiovascular Disease. St Louis,
29. Lipscomb KJ, Smith JC, Clarke B, et al: Outcome of pregnancy in women with Marfan’s syndrome. Br J Obstet Gynaecol 104:201-206, 1997
30. Low FN: Microfibrils: Fine filamentous components of the tissue space. Anat Rec 142:131-137, 1962
31. Maddox BK, Sakai LY, Keene DR, et al: Connective tissue microfibrils. J Biol Chem 264:21381-21385, 1989
32. Marfan AB: Un cas de deformation congenitale des quatres membres plus prononcee aux extremites characterisee par l’alongement des 0s avec un certain degre d’amincissement. Bull Mem SOC Med Hop Paris 13220-226, 1896
33. McFarland J, Willerson JT, Dinsmore RE, et al: The medical treatment of dissecting aortic aneurysms. N Engl J Med 286:115-119, 1972
34. Milewicz DM, Pyeritz RE, Crawford ES, et al: Marfan syndrome: Defective synthesis, secretion, and extra- cellular matrix formation of fibrillin by cultured der- mal fibroblasts. J Clin Invest 89:79-86, 1992
35. Morse RP, Rockenmacher S, Pyeritz RE, et al: Diagno- sis and management of Marfan syndrome in infants. Pediatrics 86:888-895, 1990
36. Murdoch JL, Walker BA, Halpern BL, et al: Life ex- pectancy and causes of death in the Marfan syn- drome. N Engl J Med 286304-808, 1972
37. Park ES, Putnam EA, Chitayat D, et al: Clustering of FBN2 mutations in patients with congenital con- tractural arachnodactyly indicates an important role of the domains encoded by exons 24 through 34 during human development. Am J Med Genet 78:350-355, 1998
38. Pereira L, DAlesio M, Ramirez F, et al: Genomic organization of the sequence coding for fibrillin, the defective gene product in Marfan syndrome. Hum Mol Genet 2:961-968, 1993
39. Pereira L, Levran 0, Ramirez F, et al: A molecular approach to the stratification of cardiovascular risk in families with Marfan’s syndrome. N Engl J Med 331:148-153, 1994
40. Pini R, Roman MJ, Kramer-Fox R, et al: Mitral valve dimensions and motion in Marfan patients with and without mitral valve prolapse: Comparison to pri- mary mitral valve prolapse and normal subjects. Cir- culation 80:915-924, 1989
41. Lindsay Jr. J: Aortic dissection. In Hurst JW (ed): Current Therapy in Cardiovascular Disease. St. Louis, Mosby-Year Book, 1994, pp 331-334
42. Pyeritz RE: Homocystinuria. In Beighton P (ed): McKusick‘s Heritable Disorders of Connective Tis- sue. ed 5, St. Louis, Mosby, 1993, pp 137-178
43. Pyeritz RE: Maternal and fetal complications of preg- nancy in the Marfan syndrome. Am J Med 713784- 790, 1981
44. Pyeritz RE, Fishman EK, Bernhardt BA, et al: Dural ectasia is a common feature of the Marfan syndrome. Am J Hum Genet 43:726-732, 1988
Mosby, 1994, pp 335-342 45. Pyeritz RE, McKusick VA: The Marfan syndrome:
Diagnosis and management. N Engl J Med 300:772- 779, 1979
46. Raizner AE, Siegal C O Mitral regurgitation. In Hurst JW (ed): Current Therapy in Cardiovascular Disease. St Louis, Mosby, 1994, pp 220-224
47. Ramirez F: Fibrillin mutations in Marfan syndrome and related phenotypes. Curr Opin Genet Dev 6:309- 315, 1996
48. Reed CM, Fox ME, Alpert B: Aortic biomechanical properties in pediatric patients with the Marfan syn- drome, and the effects of atenolol. Am J Cardiol 71:60&608, 1993
49. Roman MJ, Rosen SE, Kramer-Fox R, et al: Prognostic significance of the pattern of aortic root dilation in the Marfan syndrome. J Am Coll Cardiol 221470- 1476, 1993
50. Sakai LY, Keene DR, Engvall E: Fibrillin, a new 350 kDa glycoprotein is a component of extracellular mi- crofibrils. J Cell Biol 103:2499-2509, 1986
51. Salim MA, Alpert BS, Ward JC, et al: Effect of beta- adrenergic blockade on aortic root rate of dilation in the Marfan syndrome. Am J Cardiol74:629433, 1994
52. Savolainen A, Keto P, Hekali P, et al: Aortic distensi- bility in children with the Marfan syndrome. Am J Cardiol 70:691-693, 1992
53. Savunen T Cardiovascular abnormalities in relatives of patients operated for annulo-aortic ectasia: A clini- cal and echocardiographic study on 40 families. Eur J Cardiothorac Surg 1:3-10, 1987
54. Schon H R Medical treatment of chronic valvular re- gurgitation. J Heart Valve Dis 2S170-174, 1995
55. Shores J, Berger KR, Murphy EA, et al: Progression of aortic dilation and the benefit of long term beta- adrenergic blockade in Marfan syndrome. N Engl J Med 330:1335-1341, 1994
56. Silverman DI, Burton KJ, Gray J, et al: Life expec- tancy in the Marfan syndrome. Am J Cardiol 75:157- 160, 1995
57. Silverman DI, Gray J, Roman MJ, et al: Family history of severe cardiovascular disease in Marfan syndrome is associated with increased aortic diameter and de- creased survival. J Am Coll Cardiol 26:1062-1067, 1995
58. Stickler GB, Belau PG, Farrel FJ, et al: Hereditary progressive arthro-ophthalmopathy. Mayo Clin Proc 40:433-455, 1965
59. Tsipouras P, Del Mastro R, Sarfarazi M, et al: Linkage of Marfan syndrome, ectopia lentis, and congenital contractural arachnodactyly to the fibrillin genes on chromosomes 15 and 5. N Engl J Med 326:905-909, 1992
60. Tsipouras P, Devereux RB: Marfan syndrome: Genetic basis and clinical manifestations. Seminars in Derma-
61. Yin FCP, Brin KP, Ting CT, et al: Arterial hemody- namic indexes in Marfan syndrome. Circulation 79:854-862, 1989
tology 121219-228, 1993
Address reprint requests to
Petros Tsipouras, MD University of Connecticut Health Center
263 Farmington Avenue Farmington, CT 06030
e-mail: [email protected]