Embed Size (px)
Citation preview

The future of barium imagingRAD Magazine, 39, 461, 28-29
Dr A LeslieSpecialist registrar clinical radiology
Dr A McCullochConsultant radiologist
Dr I A ZealleyConsultant radiologist
NHS Tayside, Tayside University Hospitals NHS Trust
IntroductionBarium sulphate has been used as a gastro-intestinal (GI) contrast agent for over 100 years.Since the first report of single contrast bariumradiography in 1910, barium techniques haveevolved in parallel with technical developmentssuch as fluoroscopic image intensification.1 Doublecontrast techniques were first described in the1920s1 but did not become mainstream until the1960s and 1970s when double contrast techniqueswere refined. This development facilitated highquality examination of bowel segments inacces-sible to compression.2-4 Rectal tube insufflation forbarium enema was followed by nasogastric tubeinsufflation for upper GI barium studies, eventu-ally superceded by gastric insufflation using car-bon dioxide producing oral preparations.1
Barium techniques to examine the GI tract extend all theway from the mouth to the anal canal. They are well-established and widely practised. However, barium imagingfaces stiff competition from other technical innovations thathave occurred over its long history. It has become evidentthat the indications for which barium imaging remains theinvestigation of choice have diminished considerably.
Evidence of better diagnostic performance has seenseveral barium applications supplanted by emerging radio-graphic techniques. This to the dismay of “traditionalist”radiologists who appreciate and enjoy the skill required toproduce high quality barium examinations, and becausebarium images often have an aesthetic quality independentof their subject matter or clinical utility. When endoscopywas limited to diagnosis only, the battle lines were fairlydrawn but the pendulum started to swing irrevocably withthe development of endoscopic techniques to biopsy and treatlesions.
This article describes the current and predicted futurerole of barium imaging from top to bottom (pun intended)and discusses the alternative, competing investigations ineach anatomical area.
Mouth and oropharynxThe modified barium swallow (MBS) using videofluoroscopyis a dynamic evaluation of the oral, pharyngeal and upperoesophageal phases of swallowing. It is performed both toevaluate suspected disorders of swallowing and to assess theimpact of therapeutic interventions. The commonest indica-tion is dysphagia following stroke and current guidelines forthis indication robustly support the MBS as the optimalinvestigation.5 However, MBS does require that the patient
is fit for transfer to the fluoroscopy suite and that they areable to sit upright. Fibreoptic endoscopic evaluation of swal-lowing (FEES) is an alternative to the MBS which hasadvantages in some settings,5 principally that it is portableand therefore suitable for unfit patients. A further recentinnovation is evaluation of swallowing using ‘real time’ MRfluoroscopy.6
Oesophagus, stomach and duodenumBefore the advent of flexible endoscopy the investigation ofsuspected upper GI disease relied heavily on barium studies.The introduction of flexible endoscopy in the late 1960s, withfurther development of therapeutic applications from thelate 1970s onwards, has led to a progressive decline in therole of barium imaging. More recently, the development ofpowerful acid-suppressing drugs and reliable eradicationtherapy for gastric Helicobacter pylori infection has signifi-cantly reduced the need for investigation.7
Robust evidence-based guidelines for the management ofdyspepsia recommend onward referral to secondary care forpatients with recurrent symptoms or ‘alarm features’(anaemia, weight loss). The investigation of choice isendoscopy, with barium studies being reserved only for thoseintolerant of endoscopy.7
High quality double contrast barium studies can indicaterisk for Barrett’s oesophagus in patients with gastro-oesophageal reflux8 but follow-up surveillance for malignanttransformation is with structured endoscopic biopsyprotocols.9,10
Barium studies were traditionally employed for theassessment of anastomotic integrity after upper GI surgery.Modern practice prefers water-soluble contrast agents forfluoroscopic studies, and often CT instead. However, bariumimaging remains the investigation of choice for selected com-plications following laparoscopic fundoplication or gastricbanding surgery.11-13
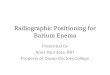
Another resilient indication for barium studies is in theinvestigation of suspected pharyngeal pouch (figure 1), notleast because there is good evidence that barium findingscorrelate well with clinical outcome after surgical treat-ment.14
Oesophageal motility disorders often require a multi-modality approach, with some disorders being associatedwith characteristic barium findings.15 Oesophageal mano-metry is the definitive investigation for oesophageal dys-motility but barium studies and/or endoscopy are also rec-ommended as the initial ‘screening’ investigations.16
Small bowelThe most common indication for small bowel investigation isknown or suspected Crohn’s disease (CD). The initial diag-nosis of Crohn’s disease relies on a combination of clinical,laboratory, endoscopic, histological and imaging informa-tion.17 The European Crohn’s and Colitis Organisation(ECCO) consensus on CD states that “…ileocolonoscopy andbiopsies from the terminal ileum as well as each colonic seg-ment to look for microscopic evidence of Crohn’s disease arefirst line procedures to establish the diagnosis. Irrespectiveof the findings at ileocolonoscopy, further investigation isrecommended to examine the location and extent of anyCrohn’s disease in the upper gastrointestinal tract or smallbowel.”18
Although there is no irrefutable evidence, it is generallyaccepted that barium studies (follow through or enteroclysis)are more sensitive for detecting subtle, early mucosal dis-ease than the current competitor investigations such as MRor CT enterography/enteroclysis. Thus, for suspected CDwhere ileocolonoscopy is unrewarding, barium studies retain

a role for the detection of early disease.However, in patients with an established diagnosis there
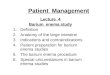
is no need to detect subtle mucosal disease. These patientsmay be effectively followed up with MR or CT entero-graphy/enteroclysis that have the advantages of detectingand depicting the peri-enteric complications that characteriseCD (fistula, abscess).18 There are also indications that MRand CT findings may provide additional information aboutthe stage of inflammation (acute vs chronic) which may helpto guide appropriate therapy (figure 2).
A further pertinent point is that patients with CD aretypically young and require repeated investigation.Accumulated ionising radiation burden is an important fac-tor, with one in seven CD patients accumulating over 75mSvfrom diagnostic tests.19 MR enterography for follow-up ofestablished CD avoids this risk.
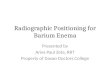
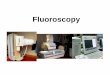
Large bowelThe double contrast barium enema (DCBE) (figure 3) is atime-honoured investigation and is widely available.However, for most indications colonoscopy is the investiga-tion of choice for suspected colorectal pathology. Morerecently CT colonography (CTC) (figure 4) has emerged asa further alternative to DCBE.
Colorectal cancer (symptomatic)Current guidelines recommend colonoscopy as the most sen-sitive technique to diagnose colorectal cancer (also enablingbiopsy and polypectomy).20 CTC is recommended as a sensi-tive alternative to colonoscopy.20 These guidelines examineda meta-analysis which concluded that CTC was “…the mostaccurate and best tolerated radiological imaging method ofdiagnosing colorectal cancer…”. This view is supported bythe results of the recently published SIGGAR multicentrerandomised trial comparing DCBE and CTC in symptomaticpatients.21 The study demonstrated that CTC detects 31%more cancers or large polyps (≥10mm) than DCBE. For sus-pected colorectal cancer CTC has effectively supplantedDCBE as the radiological investigation of choice.
Colorectal cancer (screening)There is no compelling evidence to support colonoscopy, CTCor DCBE as a primary modality for general populationscreening for colorectal cancer.20 The current UK BowelScreening Programme utilises guaiac faecal occult blood(FOB) testing as the primary modality. Individuals who testpositive for FOB are invited to attend for colonoscopy. Onlya very small proportion of patients undergo radiologicalimaging, typically as an adjuvant investigation following anincomplete colonoscopy.
Individuals at increased risk of developing colorectal can-cer because of familial genetic mutations, long-standingulcerative colitis or prior history of high risk adenomatouspolyps are offered colonoscopic surveillance in accordancewith guidelines developed by the BSG/ACPGBI22 and SIGN.20
Ulcerative colitisThe diagnosis of ulcerative colitis (UC) is typically based onclinical suspicion augmented by appropriate macroscopicfindings at endoscopy, typical histology on biopsy and exclu-sion of infectious agents on stool samples.17 Barium imag-ing is no longer indicated in either the acute or thenon-acute setting.
Rectum and anal canalEvacuation proctography for the assessment of defaecationhas been performed in specialised centres for over 50 years.The technique is associated with a high ionising radiationdose as it involves lateral fluoroscopy through the pelvis.In recent years, dynamic MR defaecography has emergedas an alternative to conventional barium technique. The MR
approach has the advantage that it not only demonstratesthe morphology of the bowel lumen but also the positionand movement of the important soft tissue structures aroundthe bowel during defaecation. A further advantage is that allof this additional information comes with no radiation bur-den. It seems likely that as the relevant equipment andexpertise become more widespread, MR defaecography willsupplant barium techniques.
Gastrointestinal haemorrhageAlthough historically barium studies were recommendedinvestigations in the management of acute GI bleeding,23
their role was being challenged almost immediately.24 CTangiography, endoscopy/colonoscopy and catheter angio-graphy have completely superseded barium imaging in thediagnosis of acute GI bleeding, with the latter having anadditional therapeutic role. Current guidance for bothvariceal and non-variceal acute upper GI bleeding is earlyendoscopy and endotherapy.25 Similarly, for patients withmassive lower GI bleeding, the initial investigation of choiceis colonoscopy.25
ConclusionAfter a long run in the spotlight it is clear that recent yearshave seen a substantial contraction of indications for whichbarium imaging is the investigation of choice. The likelyabandonment of the DCBE in favour of CTC will be theAlamo for colonic barium imaging. However, barium imagingremains the preferred modality for a limited range of indi-cations including the MBS for functional assessment of swal-lowing, assessment of pharyngeal pouch, and small bowelbarium studies for the detection of early, subtle Crohn’s dis-ease. In addition, there will always be a proportion ofpatients intolerant of endoscopy or colonoscopy, or for whomMRI is contraindicated. The heyday of barium imaging hasundoubtedly passed, a consequence of relentless innovationin diagnostic imaging, but some applications remain andthey remind us all of the pivotal role barium once playedin diagnostic radiology practice for so many years.
References1, Eisenberg R, Margulis A. Brief history of gastrointestinal radiology.
Radiographics 1991;11:121-132.2, Welin S. Results of the Malmö technique of colon examination. JAMA
1967;199(6):369-71.3, Laufer I. The double-contrast enema: Myths and misconceptions.
Gastrointest Radiol 1976;1(1):19-31.4, Laufer I. Double-contrast enema: Technical aspects. In: Double-contrast
gastrointestinal radiology with endoscopic correlation. Philadelphia, Pa:Saunders, 1979;495-515.
5, Scottish Intercollegiate Guidelines Network, Healthcare ImprovementScotland. Guideline 119; Management of Patients with Stroke:Identification and Management of Dysphagia.
6, Barkhausen J, Goyen M, von Winterfeld F, Lauenstein T, Arweiler-HarbeckD, Debatin J F. Visualization of swallowing using real-time TrueFISPMR fluoroscopy. Eur Radiol 2002;12(1):129-33. Epub 2001 Oct 13.
7, Scottish Intercollegiate Guidelines Network, Healthcare ImprovementScotland. Guideline 68; Dyspepsia.
8, Gilchrist A M, Levine M S, Carr R F, Saul S H, Katzka D A, Herlinger H,Laufer I. Barrett’s esophagus: Diagnosis by double-contrast esophagogra-phy. Am J Roentgenol 1988;150(1):97-102.
9, Watson A, Heading R C, Shepherd N A. Guidelines for the diagnosis andmanagement of Barrett’s columnar-lined oesophagus. London: The BritishSociety of Gastroenterology. Available from: http://www.bsg.org.uk/pdf_word_docs/Barretts_Oes.
10, Scottish Intercollegiate Guidelines Network, Healthcare ImprovementScotland. Guideline 87; Management of oesophageal and gastric cancer.
11, Baker M E, Einstein D M et al. Gastroesophageal reflux disease:Integrating the barium esophagram before and after antireflux surgery.Radiology 2007;243:329-39.
12, Swenson D W, Levine M S, Rubesin S E, Williams N N, Dumon K. Utilityof routine barium studies after adjustments of laparoscopically insertedgastric bands. Am J Roentgenol 2010;194(1):129-35.
13, Mehanna M J, Birjawi G, Moukaddam H A, Khoury G, Hussein M, Al-Kutoubi A. Complications of adjustable gastric banding, a radiologicalpictorial review. Am J Roentgenol 2006;186(2):522-34.
14, Tsikoudas A, Eason D, Kara N, Brunton J N, Mountain R E. Correlationof radiologic findings and clinical outcome in pharyngeal pouch stapling.

Ann Otol Rhinol Laryngol 2006;115(10):721-6.15, Levine M S, Rubesin S E. Diseases of the esophagus; diagnosis with esoph-
agography. Radiology 2005;237(2):414-27.16, Bodger N, Trudgill K. Guidelines for oesophageal manometry and pH
monitoring. November 2006 BSG Guidelines in Gastroenterology.17, Mowat C, Cole A et al. Guidelines for the management of inflammatory
bowel disease in adults. IBD Section of the British Society ofGastroenterology. Gut 2011;60(5):571-607.
18, Van Assche G, Dignass A et al. The second European evidence-basedconsensus on the diagnosis and management of Crohn’s disease: Definitionsand diagnosis. J Crohns Colitis 2010;4(1):7-27.
19, Desmond A N, O’Regan K et al. Crohn’s disease: factors associated withexposure to high levels of diagnostic radiation. Gut 2008;57(11):1524-9.
20, Scottish Intercollegiate Guidelines Network, Healthcare ImprovementScotland. Guideline 126; Diagnosis and management of colorectal cancer.
21, Halligan S, Wooldrage K et al. SIGGAR investigators. Computed tomo-graphic colonography versus barium enema for diagnosis of colorectal can-cer or large polyps in symptomatic patients (SIGGAR): a multicentrerandomised trial. Lancet 2013;381(9873):1185-93.
22, Cairns S R, Scholefield J H et al. British Society of Gastroenterology;Association of Coloproctology for Great Britain and Ireland. Guidelinesfor colorectal cancer screening and surveillance in moderate and high riskgroups (update from 2002). Gut 2010;59(5):666-89.
23, Allan R N, Dykes P W, Toye D K. Diagnostic accuracy of early radiology inacute gastrointestinal haemorrhage. Br Med J 1972;4(5835):281-4.
24, Cotton P B. Early radiology in acute gastrointestinal haemorrhage. BrMed J 1972;4(5840):608.
25, Scottish Intercollegiate Guidelines Network, Healthcare ImprovementScotland. Guideline 105; Management of acute upper and lower gastroin-testinal bleeding.
A
B
C
Figure 1Barium swallowexaminationdemonstrating alarge pharyngealpouch.
Figures 2A, 2Band 2C(A) Barium follow-through examina-tion showingpersistent shortsegment terminalileal narrowingand spatial separa-tion of small bowelloops in a patientwith confirmedCrohn’s disease. (B and C) MRsmall bowel exami-nation of the samepatient as in (A)performed eightmonths later showing terminalileal active diseasemanifest as layered bowel wallthickening.

Figure 3Barium enema examination showing an annularcarcinoma of proximal sigmoid colon.
Figure 4CT colonography examination showing a polypoidallesion of the sigmoid colon.














![Bowel Elimination Si.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/.../kdm_slide_bowel_elimination.pdfPrimary organ of bowel elimination ... Small bowel series Barium enema. ... Sigmoid](https://img.dokumen.tips/doc/110x75/5adf17e77f8b9ac0428bbfc8/bowel-elimination-sippt-read-only-ocwusuacidocwusuacidkdmslidebowel.jpg)