Embed Size (px)
Citation preview

180 Parasitology Today, vol. 4, no. 6, 1988
The Epidemiology of Toxocara canis
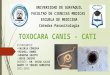
v v Embryonated eggs ingested by another animal - such as a rodent - produce larvae that may migrate in the host tis- sues and will resume development when the prey is eaten by a carnivore. In the case of Toxocara canis - a common asca- rid parasite of the dog- the close associ- ation between dogs and man makes the likelihood of transmission to humans quite high. By contrast, the cat ascarid T. cati is not thought to be a frequent cause of human infection, perhaps because of
Fig. I. Toxocara canis. (A) Egg. (/3) Larva.
;illespie rrable association with lany of which can also
canis (Fig. I), is of ram larvae becoming about 20-30 patients
areas with dog faeces sources of Toxocara indicators vary widely
defaecation habits of
:mbryonate in the soil _~ctive stage in about
ingestion, the eggs hatch in the duodenum and L2 larvae migrate through liver and lungs to the trachea where, as L3 larvae, they can be coughed up and swallowed and so reach the stomach and small intestine. Altoge- ther there are four larval moults with adults developing in the small intestine about 3-6 weeks after ingestion of eggs ~. The adult worms pass eggs continuously - up to 20 000 per day - for about 6 months.
This sequence of events only occurs in pups up to about 5 weeks old. In older dogs, parasite development halts at the second larval stage, and these larvae undergo somatic migration to the tissues where they persist for long periods. In infected bitches however, these larvae can become reactivated during preg- nancy - usually after the sixth week of gestation - when they migrate trans- placentally to infect the foetus 2. Trans- mammary infection can also occur by viable larvae in the milk although this is less common 3. Perinatal transmission proves to be highly efficient, so that almost all pups are infected by the time of whelping". Toxocara-free dogs are uncommon; infections can be eliminated by anthelmintic treatment with piper- azine and thiabendazole (see below), but unless maintained in a Toxocara-free environment, treated dogs will be quickly reinfected.
The age-related resistance to the development of T. canis in dogs was once thought to result from developing humoral immunity, although experi- ments with ascarid-free puppies have since shown that this is not the case s . Resistance in older dogs can be over- come by the use of corticosteroids in doses sufficient to suppress lymphocyte responses to lectin mitogens 6, but the reactivation of L2 larvae in pregnant bitches is conventionally ascribed to
hormonal changes during pregnancy, because transplacental migration of the larvae does not occur until late in preg- nancy (around the 40th day of gestation).
T. conis also fails to develop beyond the second larval stage in non-canid hosts. If such infected hosts fall prey to a dog the ingested larvae in the prey tis- sues can initiate a non-patent infection in the adult dog 7. Thus dogs can acquire T. canis infection in one of five ways:
( I ) Infection in utero from trans- placental passage of L2 larvae. (2) Ingestion of viable larvae in mater- nal milk. (3) Ingestion of embryonated eggs from contaminated soil by mature dogs, leading to non-patent infection. (4) Ingestion of puppy faeces leading to a patent infection in lactating bitches. (5) Ingestion of infective (L2) larvae in the tissues of an infected prey.
Transplacental transmission of T. canis in dogs means that the overall incidence of canine infection is not strongly influ- enced by climate 8, although the nema- tode eggs are susceptible to cold and larval development ceases at tempera- tures below 10°C. In general, canine toxocariasis can be found from the trop- ics to the subarctic, but is not recorded from dogs and wild canids at latitudes above 60°N. The apparent prevalence of canine infection as measured by faecal egg counts and postmortem examina- tion of dogs is greatly influenced by the age of dogs studied, and by deworming policies. The frequency of positive faecal specimens in young dogs ( < I year old) ranges from 66% in rural Germany9 to 33% in London m, and only 7% in Israel j ~. In dogs over I year old, preva- lence ranges from 6%-22% 9,10. In show dogs - although one might suppose that care was optimal - 20% of dogs under I year old gave positive faecal specimens, while for dogs of all age groups, 6% were excreting T. canis eggs12.
Owners of infected puppies and lac- tating bitches are clearly at risk of Tox- ocara infection, but a more significant public health risk comes from embryo- nated Toxocara eggs in the soil. Faecal contamination is a particular problem in densely populated urban areas where dog owners walk their pets in public parks and other pedestrian areas. In London parks, 35% of soil samples dur- ing the early 1970s were found to have
~) 1988, Elsevier Publications, Cambridge 0169-4758/88~02.00

Parasitology Today, vol. 4, no. 6, 1988
eggs of T. canis ~3, and a survey 14 years later showed that 323 of 503 soil samples from five east London parks were positive t4.
Survival of ascarid eggs is inhibited by hot dry sandy soils ~s but can be up to 2 years in clay soils in a temperate cli- mate 16'~7. Survival is also favoured by a warm moist climate, with up to 41% of soil samples in St Lucia found to be positive 18. Eggs are also susceptible to the cold, and larvae die at temperatures below -15°C. Despite this, 32.5% of soil samples in Montreal public parks were shown to be positive, as were 17.9% of samples from chi!ldren's play areas - even though air temperatures in Montreal may fall to -26°C during the winter ~9. It seems that snow cover may provide insulation against the extreme air temperatures.
Human Toxocariasis
Humans are infected, like other para- tenic hosts, by ingestion of ernbryonated T. canis eggs. Second stage larvae migrate through the tissues to cause the syn- drome of visceral larval migrans (VLM) 2°. Children playing in areas con- taminated with dog faeces are most at risk, because of their likelihood of ingesting soil particles. Other helminth eggs can also be transmitted in this way, so that in some areas, infection with Toxocara is often associated with infec- tion with Trichuris and Ascar/s. T. canis is the main cause of VLM, although the syndrome can also be caused by other ascarids such as Baylisascaris procyonis 2 ~ and, to a much lesser extent, Lagochil- ascaris minor and T. carl.
Migration of T. canis larvae in infected humans can continue for more than a year 22, and clinical symptoms seem to relate to the number of migrating larvae. Often symptoms do not develop or may go unrecognized, or clinical illness may occur associated with fever, eosinophilia, hepatosplenomegaly and bronchospasm (death attributed to toxocariasis has been reported in the past). Ocular dis- ease (OLM) occurs when migrating lar- vae become trapped in the eye - the consequent eosinophilic inflammatory response results in damage to the reti- na 23. In extreme cases, OLM may pre- sent with loss of vision or se.vere ocular inflammation. In young chi;Idren how- ever, visual impairment may often go unnoticed until detected later during a routine medical examination. Even in older children and adults, if lesions are distant from the macula and there is only mild inflammation, then visual defects may go unnoticed.
181
(
i m i ,in!,o n Op :c ::,i ®
Fig. 2. IJfe cycle of Toxocara ranis. Pregnant and lactating bitches and their puppies are central to the transmission ofT. ranis. Dormant second stage larvae are reactivated in the pregnant bitch, and infect the puppies mainly by the transplacentol route(I); larvae can also be passed to the puppies in the milk(2); and the lactating bitch will acquire adult worms from eating infective eggs in her puppies' faeces(3). In the lactating bitch and her puppies, the L2 larvae migrate from the intestine through liver and lungs to the trachea. Here, as L3 larvae, they are coughed up and swallowed to develop to L4 larvae and adults in the small intestine. These adults mature and pass eggs out with the faeces for several months(4). The eggs embryonate after about 2-3 weeks in the soil(5), from where they may be ingested by another dog or non-canid host such as man or a rodent(6). In non-canid hosts, and in older dogs, the eggs hatch in the duodenum and the L2 larvae migrate into the tissues but do not develop further. Dogs can also acquire infection by eating infected prey animals such as rodents(7). In humans, particularly in young children, migrating T. ranis larvae provoke inflammatory tissue reactions leading to the clinical syndrome of visceral larva migrans (VLM). Ocular damage (OLM) can occur when migrating larvae become trapped in the eye.
The incomplete life cycle of T. canis in humans means that diagnosis is difficult. Because adult worms do not develop and eggs are not shed, faecal examina- tion is not helpful. In OLM, the retinal lesion may resemble a retinal neoplasm, subsiding to a clear-cut area of retinal degeneration, although in younger chil- dren we find that ocular inflammation and uveitis are common signs. In cases of VLM, symptoms such as fever, hepatoo splenomegaly, hypereosinophilia and bronchospasm, are suggestive, and a high proportion of young patients show elevated IgG and IgM levels and raised levels of isohaemagglutinins to blood group A and B antigens. Definitive diag- nosis can be provided by histological examination of biopsy material. In tis- sues, the larvae of T. canis are always rhabditoid, measuring 290-350 Ilm, and found within a granulomatous lesion of closely packed eosinophils and histio- cytes. However, it is rarely clinically justi- fied to obtain such biopsy material, and even when it is available diagnosis is very time-consuming because many sections usually require examination to find the sparse parasites. Previous serological tests based on egg antigens or adult
worm extracts tended to be unreliable (often cross-reacting with other hel- minths such as Ascaris), but an effective ELISA test to detect antibody directed against the excretory-secretory anti- gens of Toxocara larvae is now widely used 24. An antigen-detecting ELISA test is also being developed.
These difficulties in diagnosis have made it almost impossible to obtain an accurate estimate of the incidence and prevalence of human infection. In the UK, more than 300 new cases oftoxoca- riasis are diagnosed each year, and over half of these have evidence of ocular involvement 2s. In one US study, T. canis accounted for 37% of retinal diagnoses for paediatric patients 26, but worldwide there are few reliable indicators for the prevalence of the disease. Surveys of adult blood donors in the UK indicate that 2.8% have significant levels of anti- Taxacara antibody 24, while reports from Australia 27 and Holland 28 indicate rates of around 7%. However, most of these positive results from adults would repre- sent antibody from past infections because the peak age of infection is about 2-4 years old and the infection tends to resolve in later life.

182 Parasitology Today, voL 4, no. 6, 1988
The burden of clinical illness falls mainly on children, with highest preva- lence in those under 10. Surveys from this age group are few, but indicate a much higher seroprevalence than in adults. The most recent survey of UK children showed 15.2% seropositive 29, while among children in the USA the overall seroprevalence is around 7%, rising to 23% in the southern states 3°. There is a higher prevalence in black children, but this probably reflects lower socioeconomic indicators rather than increased genetic susceptibility. A history of pica (eating earth) is often associated with seropositivity for Toxocclrc123'30.
A close association with dogs, either professionally or as pet owners, as expected, is strongly correlated with Toxocara infection. A case control study of OLM found that patients were sig- nificantly more likely than control sub- jects to have acquired a puppy during the previous year 3t. Veterinarians, kennel workers, and their assistants are also at higher risk; in one study, 15.7% of dog breeders were shown to be seroposi- tive, and the proport ion of positive reac- tions was related to the closeness of contact with whelping bitches, to the number of puppies born per year in the kennels, and to the length of time en- gaged in dog breeding 32. A similar study among hydatid disease control officers in New Zealand showed that 25.6% were seropositive, compared with 3.3% of a control population 33. Even contact with dogs in the course of recreation seems to increase the risk of infection; VLM has recently been recognized as a common problem in the Midi-Pyrenees Depart- ment of France - here seropositivity is associated with hunting and the posses- sion of two or more hunting dogs 34.
"Let's take the little one - looks much more comfortable"
Trea tment and Control
The natural history of VLM is towards resolution, and so treatment is only insti- tuted in patients with more severe symptoms. Anthelmintic treatment has not been proven effective by controlled trials, but clinical usage points to patient improvement after therapy. Diethyl car- bamazine up to 6 mg/kg day- i for 3 weeks has been used by some workers, and others use thiabendazole at 50 mg/kg day- i in divided doses for 7 days, with the possible addition of systemic steroids to reduce inflammation. We have been using this regimen with suc- cess for ocular cases where treatment is more difficult because inflammation from dying worms may provoke increased retinal damage. Local steroid injection or systemic steroids can be very effective in reducing the inflammation and improving visual acuity. Vitrectomy may be of benefit for the relief of trac- tional retinal detachment, and photo- coagulation of suitably placed lesions may also be beneficial.
In dogs, adult worms can be elimin- ated using a range of anthelmintics such as piperazine, thiabendazole, fenbenda- zole and mebendazole. Because adult worms in puppies and lactating bitches are central to the parasite's life cycle, an effective control measure is to treat lac- tating bitches and puppies until 3 months old in order to eliminate the successive waves of prenatal transmission, trans- mammary transfer of larvae, and ingestion of infective puppy faeces.
Control of T. canis infections in hum- ans and dogs is feasible using currently available drugs, but prevention of serious human infection will require much greater attention to the prevention of contact between children and infective dog faeces. What can be achieved in this respect is illustrated by the example of Iceland where the parasite has been completely eradicated. Iceland banned the possession of dogs (but not cats) some 40 years ago as a means to control hydatid disease - a serological survey in 1982 then failed to demonstrate a single case of Toxocara infection 3s. Such draco- nian control measures are unlikely to be instigated in other countries, but this does present the challenge that more could be done to prevent young children coming into contact with the faeces of infected dogs. Owners should be encouraged to deworm their dogs regu- larly, and to prevent promiscuous defae- cation. Children's play areas in public parks should be made 'dogproofl as this can decrease the level of soil contamina-
tion in one of the most 'at risk' areas 14. Such measures may not remove the risk oftoxocariasis completely, but might sig- nificantly lessen the chance of infection and consequent blindness in young children.
References I Sprent, J.F.A. (1958) Parasitology 48, 185-198 2 Douglas, J.R. and Baker, N.FL (t959)J. Parasitol.
45,43 3 Sprent, J.F.A. ( 1961 )J. Parasitol. 47, 284 4 Griesmer, R.A. and Gibson, J.P. (1963)J. Am.
Vet./vled. Assoc. 143,965 5 Greve, JH. (1971)Am.J. Vet. Res. 32, 1185-
1192 6 Lloyd, S., Kristensen, S. and Soulsby, E.J.L.
( 1981 ) Z. Parasitenkd 66, 57-6 I 7 Scothern, M.W., Kusel, J.R and Groves, H.F.
( 1965)J. Am. Vet. Med. Assoc. 146, 45 8 Ng, B.K.Y. and Kelly, J.D. (1985) Int.J. Zoon. 2,
76 9 Hinz, E. and Baltz, I. (1985) Int.J. Zoon. 12, 21 I
I 00ldham, J.N. ( 1965)./. Helminthol. 50, 95 I I Gross, E.M., Zeitan, R. and Torok, V. ( 1984)J.
Helminthol. 58, 139 12 Jacobs, D.E. and Pegg, E.J. ( 1976)J. Helminthol.
50,265 13 Borg, O.A. and Woodruff, A.W. (1973) Brit.
Meal.J. 4,470 14 Snow, K.R., Ball, S.J. and Bewick, J.A. (1987) Vet.
Rec. 120, 66 15 Dunsmore, J.D., Thompson, R.C.A. and Bates,
I.A. (1984) Vet. Parasitol. 16, 303-31 I 16 ]acobs, D.E., Pegg, E.J. and Stevenson, P. (1977)
]. Small Anim. Pract. 18, 79-92 17 Beaver, P.C. ( t 975) Health Lab. Sci. 12, I 16-
125 18 Thompson, D.E. et al. (1986) Bull. WHO 64,
283 19 Ghadirian, E. et al. (1976) Can. J. Publ. Hlth 67,
495 20 Glickman, L.T. and Schantz, P.M. (I 98 I) Epide-
miol. Rev. 3,230-250 21 Kazacos, K.S. (1986) Parasitology Today 2, 253-
255 22 Smith, M.D.H. and Beaver, P,C. (1953) Paediat-
rics 12,491-497 23 Molk, R. ( 1983)Am. Ophthalmol. 15, 216 24 Savigny, D.H. de, Voller, A. and Woodruff,
A.W. ( 1979)J. Gin. Patho132, 284-288 25 Ree, G.H., Voller, A. and Woodruff, A.W.
(I 978)Brit. Med.J. 288,628 26 Pollard, Z,F. et al. (1979) Ophthalmology 83,
743-749 27 Nicholas, W.C., Stewart, A.C. and Walker, J.C.
(1986) Trans. R. Soc. Trop. Med. Hyg. 80, 217- 221
28 Van Knapen, F. et al. (1983) _7. Parasitenkd 63, 113-118
29 Josephs, D.S., Bhinder, P, and Thompson, A.R. ( 1981 ) Publ. Hlth London 95,273-275
30 Worley, G. et al. ( 1984)J. Infect. Dis. 149, 59 I 31 Schantz, P.M. et al. (1980) Am.J. Publ. Hlth 70,
1269-1272 32 Woodruff, A.W., Savigny, D.H. de and Jacobs,
D.E. (1978) Brit. Med.J. 2, 1747-1748 33 Clemett, R.S. et al. (1985) New Zealand Med. J.
98,737-739 34 Glickman, L.A. et al. (1987) Am. J. Publ. Hlth.
125, 1819 35 Woodruff, A.W., Savigny, D,H. de and Hendy-
Ibbs, P,M. (1982) Brit. Med.J. 4, 309
Stephen Gillespie is lecturer in Clinical Tropical Medicine at the Hospital for Tropical Diseases, London N W l, UK.



![Seroprevalence of Toxocara canis infection and associated ...Toxocara cati, whose definitive hosts are dogs and cats, respectively [2]. The global prevalence of Toxocara in-fection](https://img.dokumen.tips/doc/110x75/612367411c89fe286420a222/seroprevalence-of-toxocara-canis-infection-and-associated-toxocara-cati-whose.jpg)