Embed Size (px)
Citation preview

The Effects of Extra-Articular Suture Tension on ContactMechanics of the Lateral Compartment of Cadaveric StiflesTreated with the TightRope CCLs or Lateral Suture Technique
Catherine A. Tonks,1 DVM, Antonio Pozzi,1 DMV, MS, Diplomate ACVS, Hang-Yin Ling,2 PhD, andDaniel D. Lewis1, DVM, Diplomate ACVS1Comparative Orthopaedics Biomechanics Laboratory, Department of Small Animal Clinical Sciences, College of Veterinary Medicine, University of
Florida, Gainesville, FL and 2Department of Orthopedics and Rehabilitation, College of Medicine, University of Florida, Gainesville, FL
Corresponding Author
Antonio Pozzi, Department of Small Animal
Clinical Sciences, College of Veterinary
Medicine, University of Florida, Gainesville,
FL 32610
E-mail: [email protected]
Submitted April 2009
Accepted January 2010
DOI:10.1111/j.1532-950X.2010.00664.x
Objective: To determine the effect of suture tension on contact pressures in thelateral compartment of the stifle for the TightRope CCLs (TR) and circumfabel-lar–tibial suture (LS) techniques.Study Design: Ex vivo biomechanical study.Sample Population: Pelvic limbs (n=12) from dogs weighing 21–24 kg.Methods: A pressure sensor was used to record peak contact pressure (PCP)and mean contact pressure (MCP) and contact area (CA) in limbs mounted in amaterials testing machine. Stifles were stabilized using either a TR or LS techniqueand the prosthesis was tensioned increasingly from 25 to 70N. PCP, MCP, andCA were collected at each applied tension before and after applying an axial loadof 150N.Results: In the unloaded condition, LS stabilization resulted in a significantincrease (P=.034) in PCP at Z40N tensions, whereas TR stabilization resultedin a significant increase (P=.047) in PCP at 70N tension. There was a significantincrease in CA at tensions Z60N in the LS group. No effect on MCP was noted.No significant differences in contact pressures were observed in the loaded condi-tion. There were no significant differences in normalized PCP and CA betweenstabilization groups at any of the tension increment.Conclusions: The application of high tension to the extra-articular prosthesis alterslateral compartment contact pressures in the unloaded stifle in this ex vivo model.Clinical Relevance: Over tightening of an extra-articular prosthesis may increaselateral compartment pressure at the time of surgery. The clinical implications ofthis finding are unknown, as weight bearing may negate any detrimental effect ofhigh prosthesis tension.
Extra-articular stabilization techniques have been success-fully used for treatment of cranial cruciate ligament (CCL)insufficiency in dogs since described by Childers in 1966.1
These techniques rely on use of a synthetic or biologicprosthesis that temporarily stabilizes the CCL-deficient sti-fle until sufficient periarticular fibrosis develops to providemore permanent stability.2 Although a number of extra-articular stabilization techniques have been described,1–6
the most widely used technique7 is a modification of theprocedure described by DeAngelis and Lau,3 commonlyreferred to as the circumfabellar–tibial suture or lateral su-ture (LS) technique. The LS technique is performed byplacing a prosthetic suture around the lateral fabella and
through a hole drilled in the tibial tuberosity. The pros-thetic suture is secured in a loop using a knot or crimpclamp.8 Most owners report satisfactory results after LSstabilization, but most dogs do not regain normal functionof the affected stifle.3,9,10 Furthermore, studies have shownthat LS stabilization, as with any other stabilizationtechnique of CCL-deficient stifles, fails to mitigate theradiographic progression of osteoarthrosis.11,12
Despite widespread use of LS stabilization in dogs,13
only a few studies have evaluated the biomechanical effectsof this procedure. Chailleux et al14 evaluated the ex vivo3-dimensional kinematics of CCL-deficient stifles afterperforming a modified retinacular imbrication technique,a technique similar to LS. Their results showed a 301decrease in stifle flexion and increased external rotationraising concerns of increased lateral compartmental pres-sures.14 It would be important to define contact mechanics
Presented in part at the Veterinary Orthopedic Society Confer-
ence, Steamboat Springs, Colorado, March 2009.
Veterinary Surgery 39 (2010) 343–349 c� Copyright 2010 by The American College of Veterinary Surgeons 343

in stifle joints after LS stabilization to understand and re-fine surgical treatment of CCL insufficiency in dogs.
The TightRope CCLs extra-articular stabilization tech-nique was developed to provide bone-to-bone fixation of theprostheses using a stiff prosthetic material.6 Femoral and tib-ial bone tunnels are used to place a fiber tape prosthesis acrossthe lateral aspect of the stifle. The suture is anchored to thefemur and tibia using toggle buttons placed at the medial or-ifices of the bone tunnels.6 Tension placed on anterior cruciateligament grafts in people is widely accepted to be an impor-tant biomechanical factor influencing procedure success.15
Excessive tension can cause premature failure of the prosthe-sis, whereas insufficient tension may not provide adequatejoint stability. Appropriate suture tension should neutralizecranial tibial thrust while allowing a normal range of motion,and restore normal kinematics and contact mechanics tothe CCL-deficient stifle.16 Although the amount of tensionapplied to anterior cruciate ligament grafts has been evaluatedin humans,15 guidelines for extra-articular prosthetic suturetension in dogs are imprecise and unsubstantiated.3,4,6
Our objectives were to: (1) determine the effect of in-creasing suture tension on contact pressures within the lateralcompartment of the unloaded and axially loaded stifle stabi-lized with either TR and LS techniques; or (2) to compare the2 techniques for their effects on contact pressures. Wehypothesized that increasing suture tension would cause aprogressive increase in lateral compartmental pressure inCCL-deficient stifles treated by both TR and LS techniques.Conversely, we hypothesized that tension o 40N would re-establish normal lateral compartment contact pressures. Ourspecific aims were: (1) to measure the peak contact pressure(PCP), mean contact pressure (MCP), and contact area (CA)in the lateral compartment after progressive tensioning of TRand LS prostheses; and (2) to compare the effect of axial loadon lateral compartment pressure after progressive increasesin prosthesis tension.
MATERIALS AND METHODS
Twelve pelvic limbs were collected from 6mixed breed dogs(body weight, 21–24 kg) euthanatized for reasons unrelatedto the study. Limbs were determined free of macroscopicstifle pathology during specimen preparation.
Specimen Preparation
Limbs were wrapped in saline (0.9% NaCl) solutionsoaked towels and frozen at � 201C, then thawed over-night at �4.51C before use. After thawing, soft tissues wereremoved taking care to preserve the stifle joint capsule. Thefemur, tibia, and fibula were transected 10 cm from thestifle. The long axis of the tibia was positioned verticallyand potted in epoxy resin (Bondo, Bondo Corporation,Atlanta, GA). Specimens were wrapped in saline solutionsoaked towels and frozen at � 201C.
Potted specimens were thawed overnight at �4.51C.The specimens were kept moist during the experiment byspraying with isotonic saline solution. After craniomedial
and craniolateral arthrotomies, the coronary ligament ofthe lateral meniscus was transected to aid in submeniscalsensor placement. The tendons of origin of the long digitalextensor and popliteal muscles were excised to facilitate ac-cess to the lateral compartment of the stifle. The medial andlateral collateral ligaments of the stifle were carefully iso-lated and a 3.5-mm-diameter bone tunnel was drilledthrough the femoral condyle, centered at the origins of theligaments. Femoral osteotomies were performed to outlinea 40mm2 block of bone that circumscribed the entire originof each collateral ligament. The bone block was freed fromthe underlying condyle using an osteotome allowing bothcollateral ligaments to be reflected.
Holes were drilled in the potting material securing thetibia to enable attachment of the epoxy base to an uncon-strained multidirectional motion platform allowing 31 oftibial motion including cranial/caudal, medial/lateral, androtational freedom. A craniocaudal hole was drilled paral-lel to the joint line 1 cm distal to the femoral diaphysealosteotomy and a 6.3-mm-diameter threaded rod wasplaced to allow attachment of the femoral jig.
Surgical Technique
Stifles were divided into TR (n=6) and LS (6) groups.
TR Stifles.6 After exposing the lateral fabella and the lat-
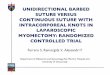
eral joint capsule a femoral tunnel was drilled originatingon the caudal aspect of the lateral femoral condyle (Fig 1),immediately distal to the lateral fabella–femoral condylejunction, and exiting on the medial aspect of the femurproximal to the medial trochlear ridge. The proximal as-pect of the muscular groove of the long digital extensormuscle on the tibia was exposed and a tibial tunnel wasdrilled with its origin in the cranial aspect of the grooveabout 2mm distal to the joint (Fig 1). The tunnel wasdrilled at a 301 proximo-distal angle exiting on the medialaspect of the proximal tibia.
LS Stifles.8 Stifles were prepared by drilling a 2.8mm holein the cranioproximal tibial tuberosity 8mm caudal to thetibial tuberosity (Fig 1).
The prosthesis was not placed in either group at this stageand specimens were wrapped in saline solution soaked towelsand frozen at � 201C. At the time of testing, the potted spec-imens were thawed overnight at�4.51C. Surgical preparationof the specimens was completed by placing the TR and LSprosthesis in the previously drilled holes. Fiber tape was usedfor both the TR and LS prostheses.
TR Stifles. The TR needle, attached via a pull-through su-ture to a toggle through which the fiber tape was threaded,was pulled through the femoral tunnel from medial-to-lat-eral. Tension was applied laterally on the TR needle andmedially on the fiber tape to slide the toggle in the bonetunnel. The TR needle and the TR toggle button were thenadvanced in the tibial tunnel from lateral-to-medial. Whenthe button emerged from the tibial tunnel, the button wasmanually flipped and seated firmly against the medial cortex
344 Veterinary Surgery 39 (2010) 343–349 c� Copyright 2010 by The American College of Veterinary Surgeons
Tonks et alContact Pressures after Extra-Articular Stabilization

of the tibia. The TR pull-through suture was cut and theneedle removed. The fiber tape was pulled tight on the lateralaspect of the stifle and secured against the medial cortex ofthe femur using a 2nd toggle and a tensioner device.
LS Stifles. Fiber tape was passed around the lateral fabellain a caudoproximal-to-craniodistal fashion, then passedthrough the previously drilled hole in the base of the tibialtuberosity. The fiber tape was passed under the patellar ten-don, tied and tensioned from the lateral aspect of the stifle.
Sensors and Sensor Placement
Before specimen testing, custom designed, plastic laminatedpressure sensors (Tekscan Inc., South Boston, MA) wereplaced beneath the lateral meniscus. Sensors had an area of30.9� 12.0mm and a thickness of 0.08mm. Exposure of thelateral compartment of the stifle was facilitated by reflectingboth collateral ligaments and applying a varus and internalrotational force to the femur. The sensor was gently manip-ulated into the space subjacent to the lateral meniscus in acaudal-to-cranial direction. Sensor positioning was accom-plished without damaging the sensor by grasping the tip
of the nonsensing portion and lubricating the sensor andmeniscus with water-based lubricant. The osteotomized bonesegments attached to the origins of the medial and lateralcollateral ligaments were replaced and secured to the femurwith lateromedial placement of a screw, washer, and nutafter the sensor was positioned.
Lateral compartmental PCP, MCP, and CA were re-corded using the pressure sensing software. Each sensorcontained 6 rows and 15 columns of sensing elementsproviding 90 sensels. The sensors had a pressure sensitivityof 0.01MPa and a pressure range of 0.5–30.0MPa. Thelower threshold was decreased after each calibration. A newsensor was used to evaluate each stifle. Each new sensor wasconditioned and calibrated according to the manufacturer’sguidelines immediately before testing of each specimen.17
Biomechanical Testing
A femoral jig (Fig 2) was used to mount the limb in thematerials testing machine (858 Mini Bionix II, MTS Sys-tems Corp., Eden Prairie, MN). The femur was fixed to the
Figure 1 Illustration of the lateral aspect of the stifle depicting the loca-
tions of the insertion points of the extra-articular prosthesis. The black dots
represent the femoral and tibial tunnels for the Tightrope technique. The
white dots represent the fabella of the lateral head of the gastrocnemius
muscle and tibial tunnel for the lateral circumfabellar–tibial suture technique.
Figure 2 Illustration of the testing apparatus including femoral jig, pot-
ted stifle, and Tekscan sensor positioned subjacent to lateral meniscus.
Veterinary Surgery 39 (2010) 343–349 c� Copyright 2010 by The American College of Veterinary Surgeons 345
Tonks et al Contact Pressures after Extra-Articular Stabilization

MTS actuator using a 6.3 mm diameter threaded rodplaced through the previously drilled hole in the diaphysis.The cranial-to-caudal orientation of the pin allowed ad-duction or abduction of the femur. The potted end of thetibia was fixed to a platform with 3 degrees of freedom(cranial–caudal translation, medial–lateral translation, andtibial rotation). Once the stifle was positioned at 1351 offlexion, (verified with a goniometer) flexion–extension androtation of the femur were constrained. Only flexion–extension was constrained, allowing tibial translation inthe cranial–caudal and medial–lateral planes and tibialrotation.
All stifles were tested in an unloaded and loaded condi-tion. Contact pressure data were collected after each incre-mental increase in fiber tape prosthesis (FiberTape, ArthrexVet Systems, Bonita Springs, FL) tension. Tensioning of thefiber tape prosthesis was performed using a calibrated tensi-oner device (Tensioner device, Arthrex Vet Systems) in bothTR and LS stabilization groups. During tensioning, the jointangle was held at 1351. The tension increments used were asmarked on the tensioning device (25, 30, 40, 50, 60, 70N).After applying tension, the tensioning device was locked tomaintain suture tension while collecting contact pressuredata. In the unloaded condition, no load was applied to thestifle during testing. In the loaded condition, axial compres-sion was applied to the stifle at a rate of 0.1mm/s to a max-imum load of 150N. Themagnitude and rate of loading werebased on a previous pilot test that was performed to evaluatethe highest loads that the sensors could tolerate for the entireexperiment without being damaged.
The same sequence of testing was used for each limb.First, specimens were tested in both unloaded and loadedconditions with an intact CCL and without tension on thepreplaced prosthesis. The CCL was then transected and thetest performed in the unloaded and loaded conditions.Prosthesis tension was increased to the next prescribedincrement and retested.
Data Analysis
Statistical analysis was performed using 1-way repeated mea-sures ANOVA to evaluate differences in PCP, MCP, and CAbetween the treated stifles and intact controls. The stifle withan intact CCL and the preplaced TR or LS suture withouttension was used as the control for all statistical comparisons.Each tension condition was compared with the control forunloaded and loaded conditions. Statistical analysis was per-formed using repeatedmeasures ANOVA to directly comparenormalized PCP and CA values between the TR and LS tech-niques in the unloaded condition. The PCP and CA valueswere normalized by dividing each value by its control. Whenstatistically significant differences were detected, a pairwisemultiple comparisons procedure (Bonferroni) was performed.For all statistical analyses performed (SPSS Inc., Chicago,IL), Po .05 (Table 1) was considered statistically significant.
RESULTS
Transection of the CCL caused gross tibial subluxationand internal rotation in the loaded condition when no ten-sion was applied to the prosthesis. Reduction of the tibialsubluxation was observed in all specimens in both groupsafter tensioning the prosthesis. A contact pressure map ofthe CCL-deficient stifles without tension applied to theprosthesis could not be generated because of the severity ofthe subluxation.
There were incremental increases in pressures for all 3contact variables as increasing tension was applied to bothTR and LS fiber tape prostheses. Prosthesis tension onlyhad significant effect on contact pressures in the unloadedcondition for both stabilization groups (Table 1). In CCL-deficient stifles stabilized with TR technique, there was asignificant increase in PCP (P=.047) compared with in-tact controls when 70N of tension was applied to the pros-thesis (Table 1). In LS stabilization group (Table 1), therewas a significant increase in PCP (P=.034) when tensionwas Z40N. Prosthesis tension did not have a significanteffect on MCP in either stabilization group (Table 2). CAincreased (P=.26) in the LS stabilization group when
Table 1 Mean (�SE) Peak Contact Pressures for Intact (Control) and
Cranial Cruciate Ligament-Deficient Stifles Stabilized with TightRope
CCLs (TR) or Lateral Suture (LS) Technique, Tested at 25–70 N of Ten-
sion in the Unloaded and Loaded Condition
Tension (N)
TR Stabilization Group LS Stabilization Group
Unloaded Loaded Unloaded Loaded
0 (control) 0.20� 0.08 1.44� 0.19 0.19� 0.08 1.76�0.27
25 0.13� 0.08 1.73� 0.49 0.11� 0.05 2.24�0.39
30 0.22� 0.08 1.75� 0.48 0.29� 0.02 2.32�0.33
40 0.41� 0.08 1.66� 0.39 0.48� 0.09
(P40-0o .05)
2.25�0.32
50 0.58� 0.17 1.76� 0.41 0.74� 0.09
(P50-0o .05)
2.09�0.48
60 0.76� 0.15 2.04� 0.66 0.88� 0.09
(P60-0o .05)
2.24�0.53
70 0.89� 0.08
(P70-0o .05)
2.15� 0.70 1.05� 0.1
(P70-0o .05)
2.39�0.48
P-values for post hoc pairwise comparisons shown in bold type are given
where significant differences were detected by ANOVA.
Table 2 Mean (�SE) Mean Contact Pressure for Intact (Control) and
Cranial Cruciate Ligament-Deficient Stifles Stabilized with TightRope
CCLs (TR) or Lateral Suture (LS) Technique, Tested at 25–70 N of
Tension in the Unloaded and Loaded Condition
Tension (N)
TR Stabilization Group LS Stabilization Group
Unloaded Loaded Unloaded Loaded
0 (control) 0.16� 0.05 0.66� 0.08 0.16� 0.06 0.69�0.07
25 0.09� 0.06 0.71� 1.8 0.11� 0.05 0.79�0.09
30 0.14� 0.04 0.67� 0.16 0.21� 0.01 0.77�0.05
40 0.29� 0.03 0.73� 0.16 0.27� 0.02 0.77�0.05
50 0.36� 0.03 0.76� 0.16 0.35� 0.03 0.76�0.08
60 0.41� 0.05 0.74� 0.14 0.42� 0.03 0.85�0.17
70 0.48� 0.05 0.87� 0.17 0.47� 0.04 0.94�0.14
No significant differences were detected between group means.
346 Veterinary Surgery 39 (2010) 343–349 c� Copyright 2010 by The American College of Veterinary Surgeons
Tonks et alContact Pressures after Extra-Articular Stabilization

tension was 460N, but no difference were found for theTR stabilization group (Table 3).
In the loaded condition, no significant differences werefound among control and treated stifles for PCP (Tables1–3), MCP, or CA, regardless of stabilization techniqueused. Pressures consistently increased when load wasapplied.
Normalization of PCP and CA data for the stabilizedstifles allowed for a direct comparison of the 2 surgical tech-niques for variables that were found to be significantly differ-ent in the unloaded condition (Tables 4). No significantdifference was found between the TR- and LS-stabilized sti-fles at any prosthesis tension. Normalization of MCP wasnot performed because tension did not have a significanteffect on MCP in either the loaded or unloaded condition.
DISCUSSION
Our results confirmed that over tightening an extra-articu-lar prosthesis when performing either TR or LS stabiliza-tion technique increased lateral compartment pressures inour unloaded ex vivo model, but lateral compartment pres-sure normalized when an axial load was applied to the
joint. These findings should be interpreted cautiously be-cause the muscle forces and cyclic loading of the extra-articular stabilization were not replicated in this model.Nevertheless, the significant increase in contact pressure athigher suture tensions tested in the unloaded stifles wouldsuggest excessive tightening of an extra-capsular prosthesismight result in elevated contact pressures during the earlyconvalescent period after surgery, when dogs typicallyplace limited weight on the affected hind limb. Early weightbearing after extra-articular stabilization of the CCL-deficient stifle may be important to resolve abnormalitiesin contact mechanics and kinematics,14 which were evidentin this study and a previous ex vivo investigation.
One of our objectives was to evaluate whether prosthesistension had similar effects on lateral compartment pressuresin unloaded and loaded stifles. While there were significantdifferences in PCP and CA after tensioning of the prosthesisin the unloaded condition, loading of the specimens elimi-nated any significant alteration of lateral contact pressures.A larger sample size may have provided the additional powerrequired to determine whether significant differences existedin the loaded condition.
Although joint alignment was not measured after eachtreatment, we suspect that when prosthesis tension was theonly force applied to the stifle, tensioning the lateral posi-tion prosthesis widens the joint space in the medial com-partment and compresses the joint surfaces of the lateralcompartment. Our supposition is supported by Chailleuxet al14 using a modified retinacular imbrication techniquein an ex vivo model simulating the non-weight-bearing phaseof the gait. That study established that extra-articular stabili-zation induced significant excessive external rotation of thetibia. It is likely that any extra-articular reconstruction tech-nique causes malalignment of the femorotibial joint whichmay be mitigated during loading the stifle; however, an invivo kinematic analysis would be needed to confirm that stiflealignment would return to normal with weight bearing.
Extra-articular reconstruction techniques have beenused to augment intra-articular procedures in human pa-tients with anterior cruciate ligament failure.18–20 The loca-tion of fixation points of the extra-articular graft purportedlyinfluences lateral compartment pressures. Ideally a prosthe-ses mimicking the CCL should be secured at isometric loca-tions, so that the distance between points of attachmentremains constant as the stifle moves through a range of mo-tion.21 Isometry of suture placement would prevent laxity oroverconstraint of the joint at different flexion angle. How-ever, an extra-capsular prosthesis can never be truly isomet-ric because the stifle does not function as a pure hinge joint.Tightening an extra-articular prosthesis in an effort to stabi-lize the joint eliminates the normal motion of the femur andtibia.14,22 In addition, alterations in the instant center of ro-tation may change the direction of surface velocity, causingcompression of the joint surfaces at their point of contact.22
Our results substantiate that excessive tensioning of theextra-articular prosthesis is detrimental to lateral compart-ment contact pressures. Nonisometric placement of prosthe-ses, such as in the LS or TR techniques, could result in
Table 3 Mean (�SE) Contact Area for Intact (Control) and Cranial
Cruciate Ligament-Deficient Stifles Stabilized with TightRope CCLs
(TR) or Lateral Suture (LS) Technique, Tested at 25–70 N of Tension in
the Unloaded and Loaded Condition
Tension (N)
TR Stabilization Group LS Stabilization Group
Unloaded Loaded Unloaded Loaded
0 (control) 14.83�6.84 90�11.29 7.17�2.68 1.76�0.27
25 4.5�3.07 83.33�15.72 3.67�1.8 2.24�0.39
30 12.33�5.22 83.67�16.63 19.67�4.01 2.32�0.33
40 24.33�8.07 79.17�16.05 36�7.76 2.25�0.32
50 30.62�11.43 77.67�13.68 53.5�8.6 2.09�0.48
60 43.83�9.86 82.83�14.05 60.67�8.44
(P60-0o .05)
2.24�0.53
70 52.67�11.73 2.15�0.70 68.17�9.01
(P70-0o .05)
2.39�0.48
P-values for post hoc pairwise comparisons shown in bold type are given
where significant differences were detected by ANOVA.
Table 4 Mean (�SE) Normalized Peak Contact Pressures (PCP) and
Contact Areas (CA) in Cranial Cruciate Ligament-Deficient Stifles Stabi-
lized with the TightRope CCLs (TR) or Lateral Suture (LS) Technique at
25–70 N of Tension in the Unloaded Condition
Tension (N)
PCP (MPa) CA (mm2)
TR LS TR LS
25 0.1� 0.07 0.06� 0.03 0.06� 0.05 0.35�0.02
30 0.18� 0.06 0.19� 0.04 0.15� 0.06 0.24�0.06
40 0.31� 0.07 0.32� 0.89 0.32� 0.12 0.40�0.07
50 0.43� 0.06 0.47� 0.09 0.39� 0.16 0.59�0.07
60 0.56� 0.07 0.56� 0.09 0.54� 0.14 0.68�0.08
70 0.66� 0.08 0.66� 0.09 0.62� 0.16 0.76�0.09
No significant differences were detected between group means.
Veterinary Surgery 39 (2010) 343–349 c� Copyright 2010 by The American College of Veterinary Surgeons 347
Tonks et al Contact Pressures after Extra-Articular Stabilization

excessive or ineffective prosthesis tension at different jointangles. Further in vivo studies are necessary to determine theclinical impact of these biomechanical abnormalities.
Several factors that affect in vivo prosthesis tensionwere not investigated in this study. The influence of thesefactors on the long-term prosthesis tension is unknown,but warrant consideration when interpreting our results.Ligament prostheses are high load-bearing structures thatare subjected to both quasi-static and impact loading. Highloads caused by excessive postoperative activity, or severejoint instability may predispose to early creep elongation ofthe prosthesis. An over-tightened prosthesis cyclicallyloaded outside the range of its tolerance may loosen withweight bearing and have no impact on lateral contact pres-sures. In our study only instantaneous contact pressuremeasurements were taken because ex vivo cycling testwould not accurately mimic the biological cycling the pros-thesis undergoes. Many variables such as variations inweight bearing, degree of periarticular fibrosis, stifle con-formation, presence of meniscal pathology and meniscaltreatment, body weight, and activity level would influencethe cycling of an extra-articular prosthesis. In our study weelected to test the prosthesis in the worse scenario of hightension, as if no creep elongation would occur during theconvalescent period.
Although high prosthesis tension increased contactpressures in the unloaded stifle, the lack of kinematic datadid not allow us to define tension values necessary toprevent tibial subluxation. Further studies are required todetermine the optimal tension required to achieve normalkinematics in loaded stifles stabilized with either the TR orLS technique.
A cadaver model is limited by the absence of the mus-cular forces present in vivo. The unloaded condition wastested to approximate the non-weight-bearing phase of thegait cycle; however, the model did not replicate the muscleforces acting about the stifle. Muscles are important con-tributors to the joint reaction force and compartmentalpressures during all phases of the gait cycle.23 Therefore,muscular forces acting across the joint may minimize theeffect of high prosthesis tension in the non-weight-bearing stifle in the absence of ground reaction force.Muscular forces are also known to play a significant rolein knee stability in human patients after anterior cruciateligament reconstruction.23 Future studies involving in vivomodels as well as kinematic analysis should improve ourunderstanding of the effects of extra-articular prosthesestension.
A specific limitation of this model is related to the softtissue dissection required for intra-articular placement ofthe sensor. Most of the joint capsule and the coronal at-tachment of the lateral meniscus to the tibial plateau wasincised to allow for insertion of the sensor subjacent to themeniscus. This exposure allowed covering the entire con-tact area of the lateral compartment with the sensor. Be-cause the menisco-tibial and menisco-femoral ligamentswere preserved, we suspect that loss of the peripheral coro-nal ligament should not have markedly affected our results.
Another factor that may have affected our results is the cy-clic freezing and thawing of our specimens. A previousstudy concluded that 4 freeze–thaw cycles modified themechanical properties of the meniscus.24 In our study,specimens underwent 3 freeze–thaw cycles and the impactof this processing is unknown.
We concluded that over tightening of an extra-articu-lar prosthesis, regardless of technique, can increase lateralcompartment contact pressures when the stifle is unloaded.Optimal tension for TR and LS could not be defined in ourstudy because of the many mechanical and biologic factorsthat may influence the effects and properties of the tension-ed suture. However, tensions 4 40N for the LS techniqueand 4 70N for the TR technique altered the contact pres-sures in the unloaded stifle, suggesting that tensioningan extra-articular prosthesis should be done cautiously.This finding is supported by a previous study that foundthat dogs that had satisfactory limb function after LSstabilization had more cranial drawer motion and a greaterrange of motion than dogs that did poorly.25 In this study,the effect of tension was eliminated by axial load, suggest-ing that early weight bearing may mitigate abnormalities incontact pressures caused by excessive tension of an extra-articular prosthesis.
REFERENCES
1. Childers HE: New methods for cruciate ligament repair II.
Repair by suture technique. Mod Vet Pract 1966;47:59–60
2. Brinker WO, Piermattei DL, Flo GL: Diagnosis and
Treatment of Orthopedic Conditions of the Hindlimb, in
Brinker WO, Piermattei DL, Flo GL (eds): Handbook of
Small Animal Orthopedics and Fracture Treatment (ed 2).
Philadelphia, PA, Saunders, W. B., 1990, pp 341–470
3. DeAngelis M, Lau RE: A lateral retinacular imbrication
technique for surgical correction of anterior cruciate
ligament rupture in the dog. J Am Vet Med Assoc
1970;157:79–84
4. Flo GL: Modification of the lateral retinacular imbrication
technique for stabilizating cruciate ligament injuries. J Am
Anim Hosp Assoc 1975;11:570–573
5. Guenego L, Zahra A, Madelenat A, et al: Cranial cruciate
ligament rupture in large and giant dogs. A retrospective
evaluation of a modified lateral extracapsular stabilization.
Vet Comp Orthop Traumatol 2007;20:43–50
6. Cook JL, Luther JK, Beetem J, et al: Clinical comparison of a
novel extracapsular stabilization procedure and tibial plateau
leveling osteotomy for treatment of CCL deficiency in dogs.
Vet Surg 2010;39:315–323
7. Leighton RL: Preferred method of repair of cranial cruciate
ligament rupture in dogs: a survey of ACVS diplomats
specializing in canine orthopedics. Vet Surg 1999;28:194A
(abstract)
8. Schulz KS: Cranial cruciate ligament rupture, in Fossum TW
(ed): Small Animal Surgery (ed 3). St. Louis, MO, Mosby,
2007, pp 1254–1276
348 Veterinary Surgery 39 (2010) 343–349 c� Copyright 2010 by The American College of Veterinary Surgeons
Tonks et alContact Pressures after Extra-Articular Stabilization

9. Moore KW, Read RA: Cranial cruciate ligament rupture inthe dog—a retrospective study comparing surgicaltechniques. Aust Vet J 1995;72:281–285
10. Conzemius MG, Evans RB, Besancon MF, et al: Effect ofsurgical technique on limb function after surgery for ruptureof the cranial cruciate ligament in dogs. J Am Vet Med Assoc2005;226:232–236
11. Lazar TP, Berry CR, deHaan JJ, et al: Long-termradiographic comparison of tibial plateau leveling osteotomyversus extracapsular stabilization for cranial cruciateligament rupture in the dog. Vet Surg 2005;34:133–141
12. Stork CK, Gibson NR, Owen MR, et al: Radiographicfeatures of a lateral extracapsular wire suture in the caninecranial cruciate deficient stifle. J Small Anim Pract2001;42:487–490
13. Korvick DL, Johnson AL, Schaeffer DJ: Surgeons’preferences in treating cranial cruciate ligament ruptures indogs. J Am Vet Med Assoc 1994;205:1318–1324
14. Chailleux N, Lussier B, De Guise J, et al: In vitro3-dimensional kinematic evaluation of 2 corrective operationsfor cranial cruciate ligament-deficient stifle. Can J Vet Res2007;71:175–180
15. Arneja S, McConkey MO, Mulpuri K, et al: Graft tensioningin anterior cruciate ligament reconstruction: a systematicreview of randomized controlled trials. Arthroscopy2009;25:200–207
16. de Rooster H, de Bruin T, van Bree H: Morphologic andfunctional features of the canine cranial cruciate ligaments.Vet Surg 2006;35:769–780
17. Wirz D, Becker R, Li SF, et al: Validation of the Tekscansystem for static and dynamic pressure measurement of thehuman femorotibial joint. Biomed Tech 2002;47:195–201
18. Wilson WJ, Scranton PE Jr: Combined reconstruction of theanterior cruciate ligament in competitive athletes. J BoneJoint Surg Am 1990;72:742–748
19. Anderson AF, Snyder RB, Lipscomb AB Sr.: Anteriorcruciate ligament reconstruction using the semitendinosusand gracilis tendons augmented by the losee iliotibial bandtenodesis. A long-term study. Am J Sports Med1994;22:620–626
20. Boszotta H, Helperstorfer W, Jusner A, et al:Physiopathology of the knee joint after distal iliotibialband transfer. Arch Orthop Trauma Surg 1992;111:213–219
21. Markolf KL, Hame S, Hunter DM, et al: Effects offemoral tunnel placement on knee laxity and forces in ananterior cruciate ligament graft. J Orthop Res2002;20:1016–1024
22. Arnoczky SP, Torzilli PA, Marshall JL: Biomechanicalevaluation of anterior cruciate ligament repair in the dog: ananalysis of the instant center of motion. J Am Anim HospAssoc 1977;13:553–558
23. Shelburne KB, Torry MR, Pandy MG: Contributions ofmuscles, ligaments, and the ground reaction force tofemorotibial joint loading during normal gait. J Orthop Res2006;24:1983–1990
24. Lewis PB, Williams JM, Hallab N, et al: Multiple freeze–thaw cycled meniscal allograft tissue: a biomechanical,biochemical and histologic analysis. J Orthop Res 2008;26:49–55
25. Hill CM, Conzemius MG, Smith GK, et al: Bacterial cultureof the canine stifle joint following surgical repair of rupturedcranial cruciate ligament. Vet Comp Orthop Traumatol1999;12:1–5
Veterinary Surgery 39 (2010) 343–349 c� Copyright 2010 by The American College of Veterinary Surgeons 349
Tonks et al Contact Pressures after Extra-Articular Stabilization