Embed Size (px)
Citation preview

The Athletic Hip:Common Diagnoses and Minimally Invasive Treatments
Sanjeev Bhatia MDOrthopaedic Surgeon - Sports Medicine
Co-Director, Hip & Knee Joint Preservation CenterNorthwestern Medicine West Region
Team Physician, Northern Illinois University
Disclosures
No Pertinent Disclosures to this Talk
• Royalties with Nova Publishing - Ligamentous Injuries of the Knee, BMJ Publishing Group- “Medial Collateral Ligament Injuries”
• Stock and Ownership – Joint Preservation Innovations, LLC; Vericel; Intuitive Surgical, EDGe Surgical
• Consultant – EDGe Surgical

Hip and Knee Joint Preservation:
Because there is no substitute for your own joints

Why Joint Replacements are not Good for Younger People
Surgical Risks
Infection
Fracture
Dislocation
Blood clots
Functional Limitations
Permanently low demand
Altered mechanics with any artificial joint
Need for revision surgery
Costs to SocietyCosts of Joint
replacement surgery
Costs of revision surgeries
Costs of complications
Economic loss of productivity
“Nothing is as good as the original”

Hip Pain is Common
Early Hip pain suffers a significant inequality!
400,000 Total Knee Replacements600,000 Total Hip ReplacementsOver 1 Million Knee ArthroscopiesOver 600,000 Shoulder
Arthroscopies70,000 Hip Arthroscopies
2013 Data

Causes of Hip and Groin Pain
– Anterior Hip Pain• Muscle strains• Contusion (hip pointer)• Avulsions and apophyseal injuries• Hip dislocation/subluxation• Acetabular labral tears and loose bodies• Proximal femur fractures• Osteitis pubis• Iliopsoas bursitis• Stress syndrome• SCFE• Perthes disease• Developmental dysplasia• Osteoarthritis• Inflammatory Arthritis• Avascular Necrosis• Femoro-acetabular Impingement
– Lateral Hip Pain:• Greater trochanteric bursisits• Gluteus medius/minimus tear• ITB syndrome• Meralgia paresthetica
– Posterior Hip Pain• Lumbar spine abnormalities• Compression neuropathies• Piriformis syndrome• SI joint pathology• Ischial bursitis• Proximal hamstring strain/rupture
– Other Causes of Hip Pain:• Abdominal (sports hernias and athletic pubalgia, inguinal hernias, appendicitis)• Gynecologic (ovarian cysts, PID, pregnancy)• Urologic (testicular, scrotal)• Genitourinary (kidney stone, nephritis)
Burnett, Clohisy et al. JBJS 2006
•Average time from injury to accurate diagnosis 21 months
•Average of 3.3 providers seen before definitive treatment
Diagnostic Approach
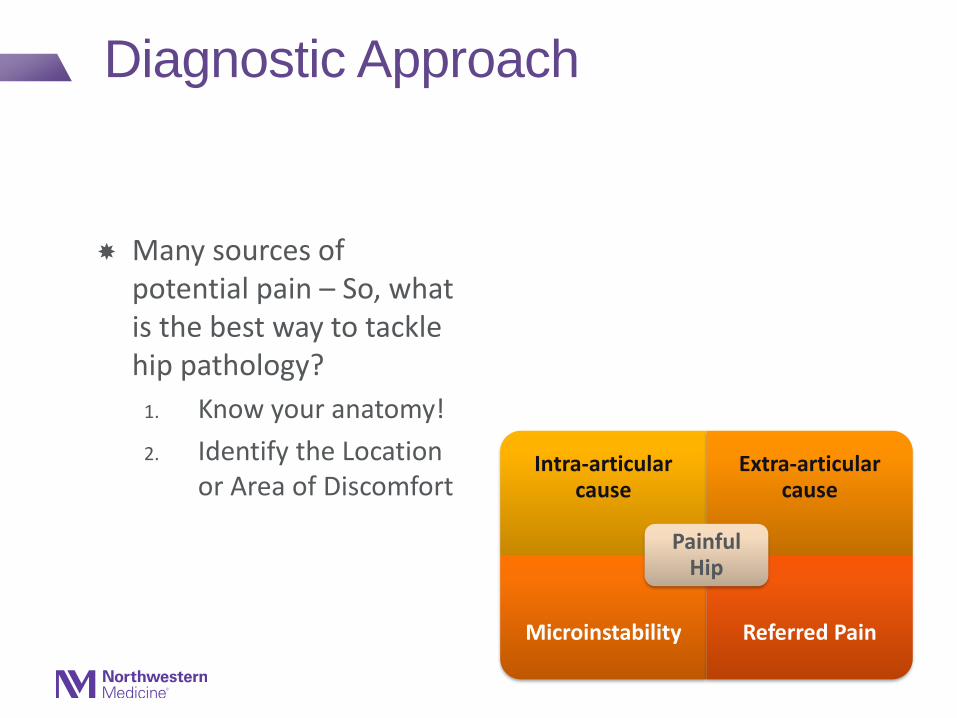
Many sources of potential pain – So, what is the best way to tackle hip pathology?
1. Know your anatomy!
2. Identify the Location or Area of Discomfort
Intra-articular cause
Extra-articular cause
Microinstability Referred Pain
Painful Hip

Acetabulum Up Close….
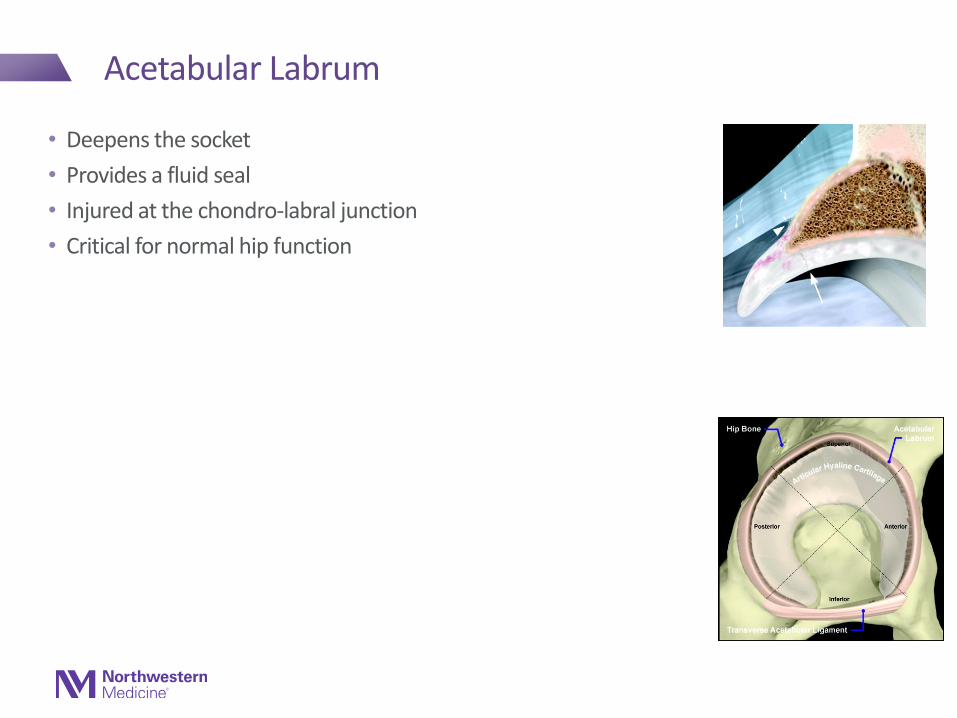
Acetabular Labrum
• Deepens the socket
• Provides a fluid seal
• Injured at the chondro-labral junction
• Critical for normal hip function

Hip Capsule – Zona Orbicularis increases stability during extension
Zona orbicularis (thick ring in capsule) tightens in extension
Courtesy of Damian Griffin MD (United Kingdom)

JBJS Am 2014
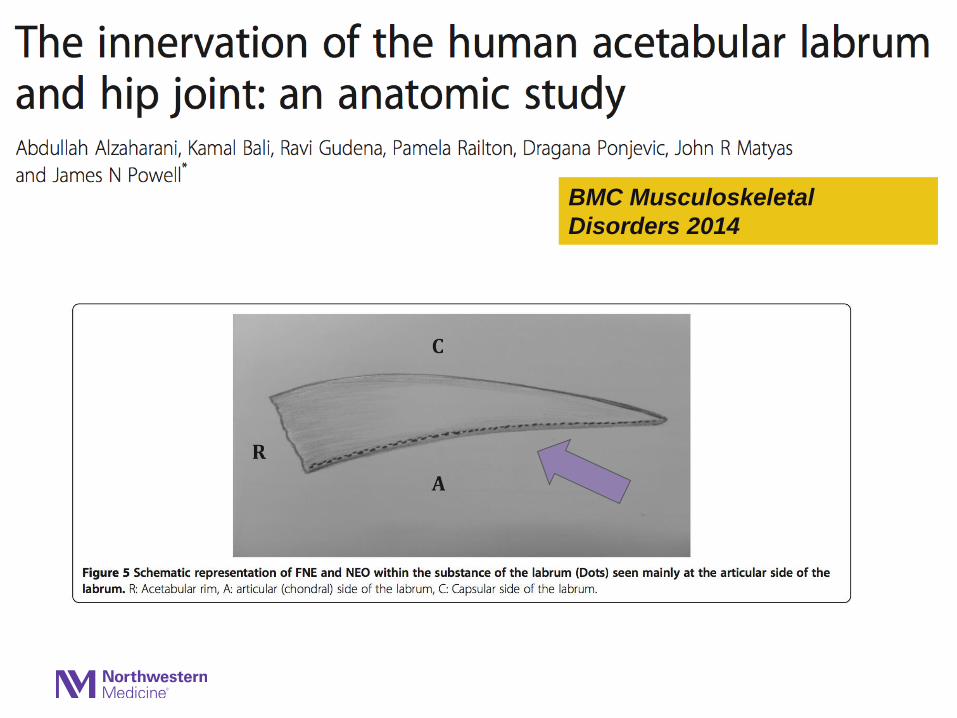
BMC Musculoskeletal
Disorders 2014

Clinical & Radiographic Evaluation

Diagnostic Approach
Many sources of potential pain – So, what is the best way to tackle hip pathology?
1. Know your anatomy!
2. Identify the Location or Area of Discomfort

Layered Understanding of the Hip
Osteochondral Layer
Femur/Acetabulum
Dynamic Impingement (FAI)
Static Overload (Dysplasia)
Inert LayerLabrum, Capsule,
Ligaments
Dynamic Layer
All musculature
Pain from entesopathies
Neural LayerNerve compression
syndromes, referred pain
Curr Rev Musc Med 2012

Posterior / Buttock
Lateral
Anterior / Groin

Anterior Hip Pain

Anterior Hip Pain
• Extra-articular
• Intra-articular

Anterior Hip Pain
•Extra-articular
• Intra-articular

Extra-Articular Anterior Hip Pain:Hip Flexor Strain / Iliopsoas Tendinitis

• Anterior hip or groin pain, F>M • Aggravated with activity, relieved with rest• Pain with rising from a seated position,
walking up stairs or inclines, brisk walking • Pain may radiate down the anterior thigh
toward the knee.• Report an audible snap or click in hip or
groin = Internal Snapping Hip
Extra-articular Anterior Hip Pain:Hip Flexor Strain / Iliopsoas Tendinitis

Internal Snapping Hip
Iliopsoas Tendon snaps over Acetabular rim / AIIS
“Can hear it”
Treatment1. Anti-inflammatories2. Injections3. Physical Therapy4. Surgery rarely indicated
91% elite ballet dancers with painless snapping

Anterior Hip Pain
• Extra-articular
• Intra-articular
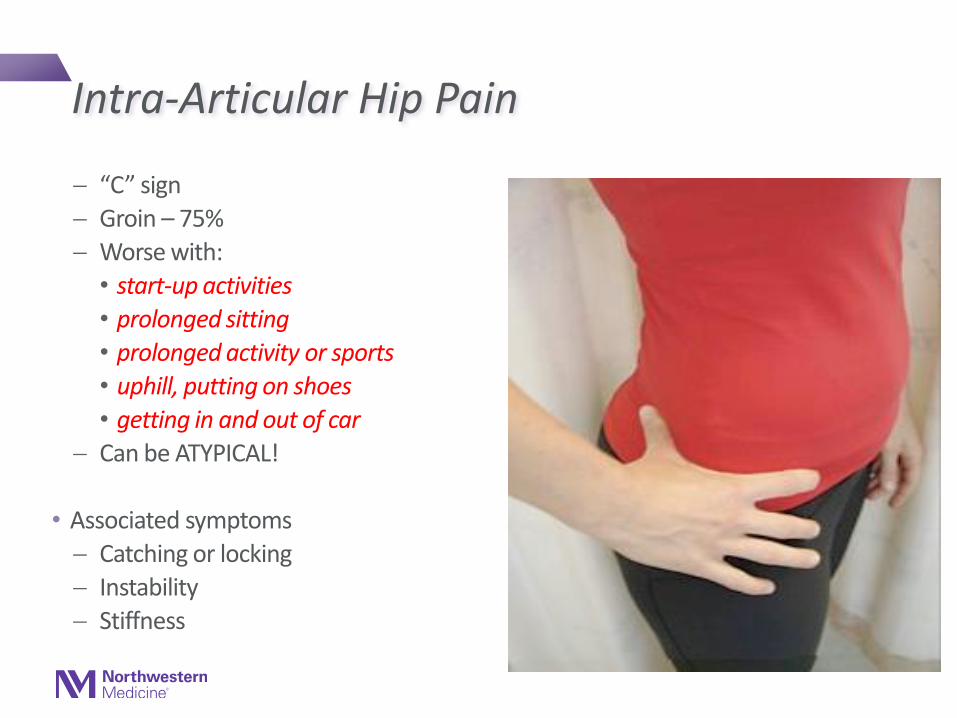
“C” sign
Groin – 75%
Worse with:
• start-up activities
• prolonged sitting
• prolonged activity or sports
• uphill, putting on shoes
• getting in and out of car
Can be ATYPICAL!
• Associated symptoms
Catching or locking
Instability
Stiffness
Intra-Articular Hip Pain

Most Common Causes of Intra-Articular Hip Pain
If the age of the patient is:
• >50 years, think:
– Osteoarthritis
• <50 years, think:
– FemoroacetabularImpingement (FAI)
– Labral Tear
Anterior Hip Pain Muscle strains Contusion (hip pointer) Avulsions and apophyseal
injuries Hip dislocation/subluxation Acetabular labral tears and
loose bodies Proximal femur fractures Osteitis pubis Iliopsoas bursitis Stress syndrome SCFE Perthes disease Developmental dysplasia Osteoarthritis Inflammatory Arthritis Avascular Necrosis Femoroacetabular
Impingement

Why do young patients (ages 20-50) with apparently normal anatomy
develop arthritis of the hip?
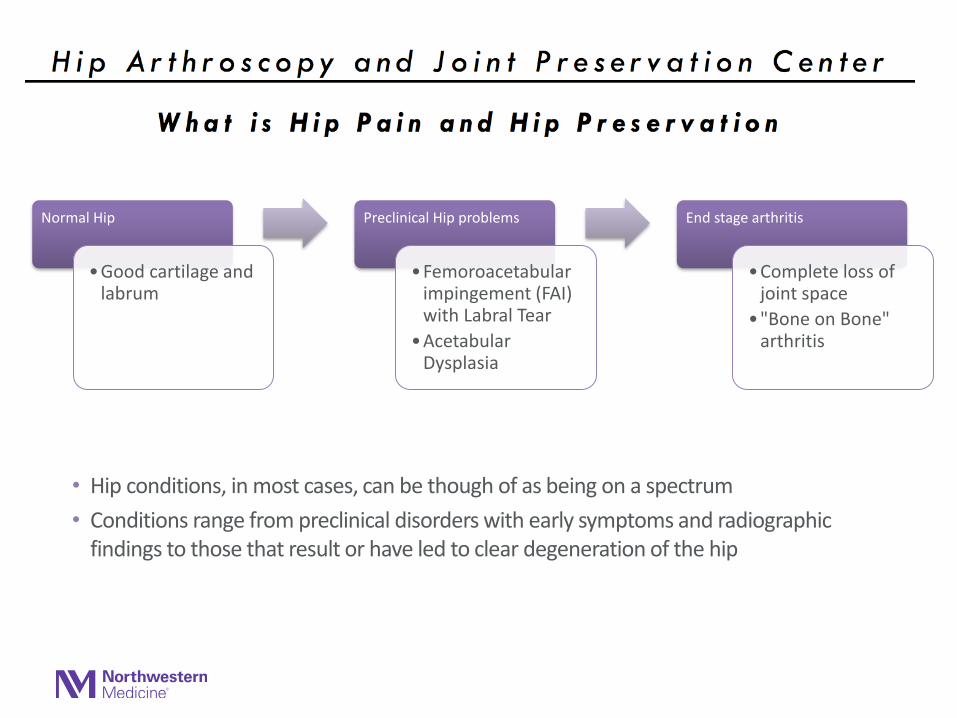
• Hip conditions, in most cases, can be though of as being on a spectrum
• Conditions range from preclinical disorders with early symptoms and radiographic findings to those that result or have led to clear degeneration of the hip
Normal Hip
•Good cartilage and labrum
Preclinical Hip problems
•Femoroacetabular impingement (FAI) with Labral Tear
•Acetabular Dysplasia
End stage arthritis
•Complete loss of joint space
•"Bone on Bone" arthritis

Cam Dominant FemoroacetabularImpingement (FAI)

”Pistol Grip” Femur - Stulberg and Harris 1975
• Stulberg SD, Cordell LD, Harris WH, Ramsey PL, MacEwen GD. Unrecognized childhood hip disease: a major cause of idiopathic osteoarthritis of the hip. In: The hip: proceedings of the third meeting of the Hip Society. St. Louis, MO: Mosby, 1975:212–228.

• FAI occurs when the femoral neck
and acetabular rim abut at the
extremes of motion due to deformity of
the femoral neck (CAM), acetabulum
(pincer), or both
• FAI leads to early OA
• Prevalence of FAI = 15%
• Up to 70-90% of ALL hip arthritis
cases thought to be caused by FAI or
hip dysplasia

British J Sports Med 2016
- Best summary on FAI syndrome
for patients, healthcare providers
- International consensus statement

British J Sports Med 2016
What is FAI syndrome?
• A motion-related clinical disorder of the hip with a triad of symptoms, clinical signs and imaging findings.
• It represents symptomatic premature contact between the proximal femur and the acetabulum
Femoroacetabular Impingement
Due to a mismatch between ball (femoral head) and cup (acetabulum)
CAM Lesion

Femoroacetabular Impingement
• Due to a overcoverage of the acetabulum with a normal femoral head/neck
Pincer Lesion

Etiology of FAI
Genetic / Inherited
➢ Siblings of patients with CAM deformity have 2.8x RR of having same deformity
➢ Siblings of patients with Pincer deformity have 2.2x RR of having same deformity (Pollard JBJS Br 2010)
• Acquired
• Athletes with Open physes increased risk of CAM lesion compared to non-athletes
85% of patients with sxatic FAI have bilateral bone abnormalities, 25% symptomatic on other side

Femoroacetabular Impingement
Typical patient:➢ Young Active Adults ➢ Athletes ➢ Runners ➢ Dancers

Symptoms
Anterior Hip / Groin Pain
Worse with flexion activities, sitting for long periods of time
Limited motion (flexion, IR)
Clicking or locking of the hip or a feeling of hip suddenly “giving out.”

British J Sports Med 2016
Clinical Signs
• Hip impingement tests usually reproduce pain
• The most commonly used test, FADIR test, is sensitive but not specific
• There is typically restricted internal rotation in flexion.

Clinical Exam

British J Sports Med 2016
Diagnostic imaging
• An AP pelvis and a lateral femoral neck view
• Can quickly review joint space, identify cam or pincer morphologies
• Advanced imaging shows cartilage, labral lesions, and bone pathology

Always Assess Joint Space on a Standing AP Radiograph – Make sure arthritis not already advanced!
Measure this space
Ideally want >3mm Joint space with no subchondral cysts

CAM Deformity
On plain AP radiographs, this pathology may easily be missed.

CAM Deformity
• Alpha angle on Dunn lateral
radiograph.
– Normal = 42º
– CAM > 50º
• Alpha angle = Poor
interobserver reliability
(0.40) Nepple, Philippon AJSM 2014
a
Nötzli, H et al. JBJS, 84-B:556, 2002.

MRA and CT
• MRI:
– Labral tears
– Articular cartilage lesions
– Herniation pits
– Sensitive + Specific
for Chondral Lesions but not labral pathology
• CT (Preoperative Planning):
– Detailed bony anatomy
– Acetabular and femoral neck road map

Treatment

British J Sports Med 2016
What is the appropriate treatment of FAI syndrome?
• Activity modification, rehabilitation or surgery
• Rehabilitation aims to improve hip stability, neuromuscular control, strength, ROM and movement patterns
• Surgery, usually arthroscopic, aims to improve the hip morphology and repair damaged tissue

Griffin DR. British J
Sports Med 2016

Treatment – My Initial Approach
Conservative, non-surgical treatment is ALWAYS the first course of action in treating hip pain.
This includes anti-inflammatories, physical therapy, chiropractic therapy and injections.➢ Diagnostic/Therapeutic Injections
• Huge part of my decision-making and treatment protocol • Intra-articular U/S guided lidocaine / cortisone injection• 90% accuracy for determining intra-articular pathology

Non-operative Treatment
1. Treat inflammation➢ Oral NSAIDS, steroids➢ Injections
2. Address functional deficits➢ Physical therapy➢ Chiropractic therapy
3. Reduce aggravating factors➢ Sitting➢ Running

Intra-articular Hip Injections
Indications
FAI Syndrome
Osteoarthritis
Diagnostics
Injection types
Steroid + Numbing
agent
PRP
Visco off label
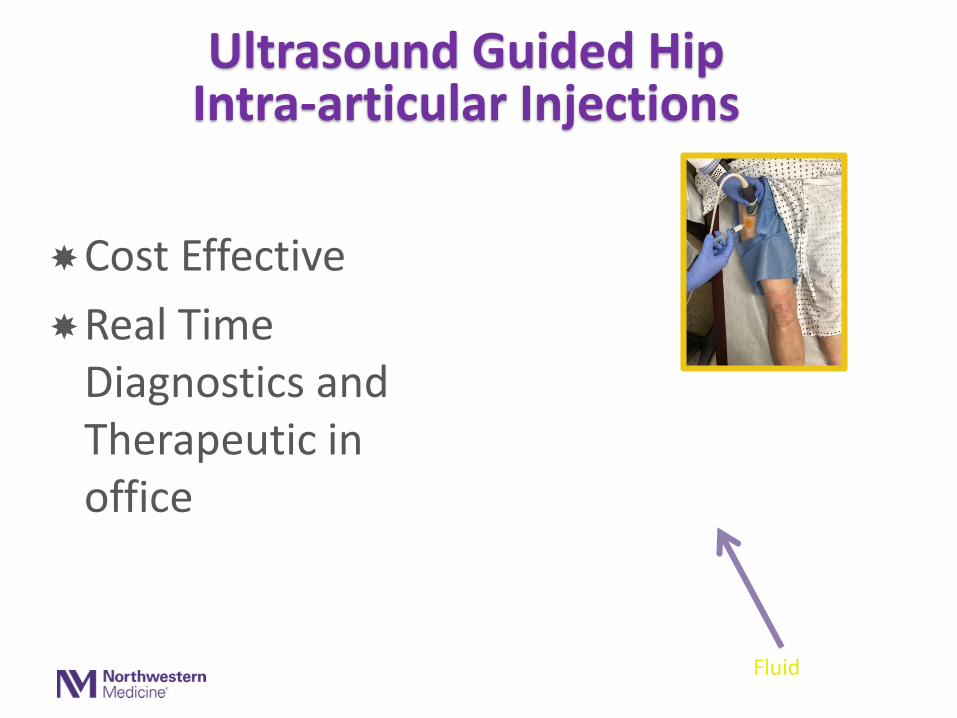
Cost Effective
Real Time Diagnostics and Therapeutic in office
Ultrasound Guided Hip Intra-articular Injections
Fluid

Success Rates of Nonoperative Tx
Intra-ArticularLabral tears/FAI/OA
• Less than 50% success
• PT alone often worsens symptoms
• Maximum one intra-articular injection
• Careful about prolonged pain and dysfunction
Extra-ArticularMuscle strain/snapping hip
• > 90% success
• PT is hallmark of treatment
• Focus on strengthening and stretching of opposing muscle groups
• Pelvic tilt / balance re-training

“Hey Doc, I have FAI and a labraltear but therapy has made it
worse! What’s the next step???

Treatment
If fail to improve with nonoperative treatment modalities, consider surgery
Hip Arthroscopy
vs
Open Hip Surgery

Hip Arthroscopy Indications
Who is the Ideal Patient for Isolated Hip Arthroscopy? Greater than 2mm (Ideally > 3mm) of joint space on
standing AP Pelvis radiographs Tonnis Grade 0 or 1 Intra-articular symptomatic FAI syndrome
➢ Hip and groin pain with symptoms that occur during hip flexion and/or internal rotation
➢ Limitations in ROM compared to c/l side
Failed physical therapy +/- injection No dysplasia or severe hip instability

Hip Arthroscopy – What Can I Treat?
FAI Labral Tears Cartilage Defects Loose Bodies Septic Joint Abductor Tears Iliopsoas tendon release Trochanteric Bursectomy
and IT band resection

Hip Arthroscopy - Portals
Portal Placement Typically use
2-3 Portals

Hip Arthroscopy - Access
AL Portal least traumatic way to access central compartment
Spinal needle Nitinol Wire 4.5mm Cannula Scope
Avoid piercing labrum and hitting femoral head
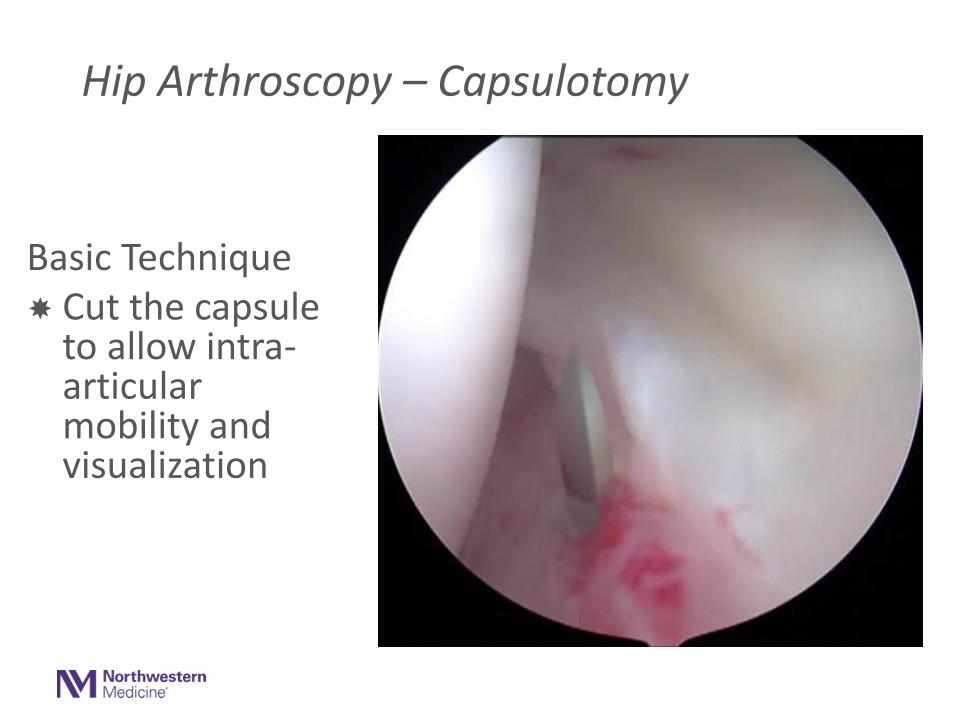
Hip Arthroscopy – Capsulotomy
Basic Technique Cut the capsule
to allow intra-articular mobility and visualization
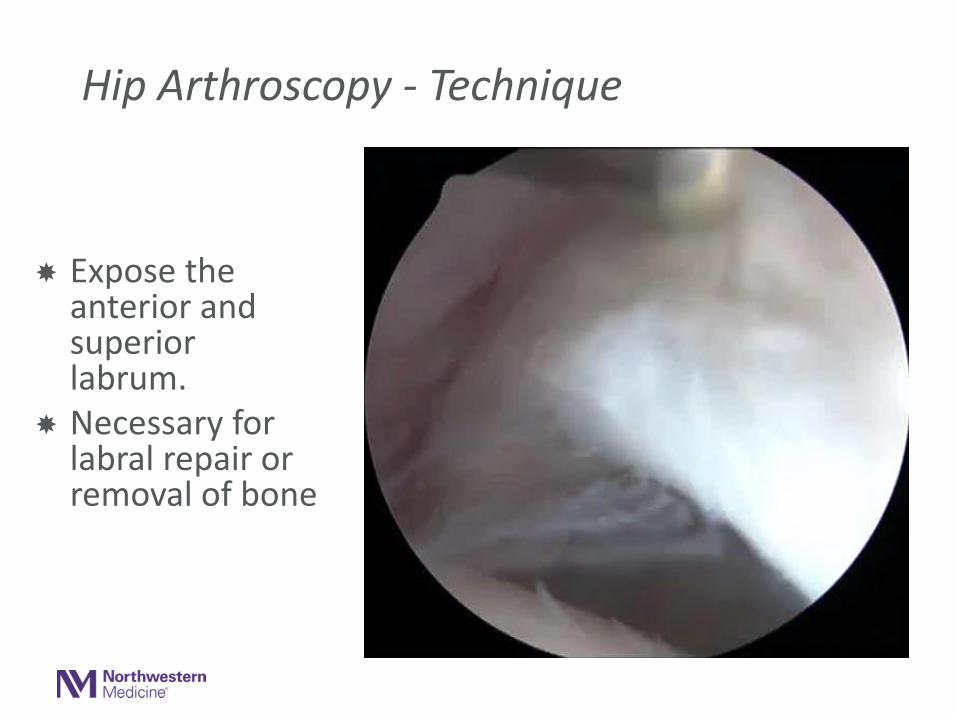
Hip Arthroscopy - Technique
Expose the anterior and superior labrum.
Necessary for labral repair or removal of bone

Hip Arthroscopy - Technique
Remove bone from anterior superior acetabulum
Repair labrum

Labral Treatment Algorithm During Hip Arthroscopy
Address FAI
• Very important to concomitantly address
• 96% labraltears due to FAI
Labral Repair
• Most cases labrum torn
• Usually use 3-4 anchors
• Preservation of labrum truly joint protective
Labral Debridement
• Done in situations of labral degeneration when suction seal intact
LabralReconstruction
• Rarely needed
• Mostly for revision cases
• Can use allograft or autograft
• Kite Technique

Hip Arthroscopy - Technique
Remove the impinging CAM lesion

• No guidelines to define CAM
correction goal
• Excessive bone resection can
compromise suction seal or structural
integrity of femoral neck
• Can be difficult to translate 2D
perspectives seen on preoperative AA
assessment to 3D FAI assessment
• Intra-op assessment may be easier
and more fruitful in guiding resection
Preoperative Dynamic Exam
Postoperative Dynamic Exam (same patient)
Intra-op Dynamic Exam to Guide Cam Resection

What Works?
• Early PROM and Hip Arthroscopy Specific Rehab
What Doesn’t Work?
• Limited Rehab without PROM
Hip Arthroscopy

• 1264 hip arthroscopy surgeries
• Patients undergoing rehab without circumduction were 4.2x more likely to have symptomatic intra-articular adhesions seen during revision arthroscopy
KSSTA 2014
40F with capsulolabral adhesions

4 Phases of PT Protocol
1. Protection = Weeks 0-4➢ PRICE➢ CPM, FFWB 20# x 2-3 wks, Hip Brace➢ Avoid Hip Flexor Irritation
2. Initial Strengthening = Weeks 4-10➢ Non-compensatory gait and
progressions➢ Aquatic program if possible
3. Advanced Strengthening ➢ Week 10 – Sports Test Completion➢ Return to Pre-Injury Level of
Function4. Return to Sport
➢ Usually at 5-7 months➢ Safe and Successful RTP is Main Goal

Previous patient: 21 year old female college soccer player

Outcomes
Surgical Outcomes following hip arthroscopy for FAI
• 85-90% good to excellent results in our hands
• Durable at 5 years• Evolving techniques and
understanding• Outcomes depend on
Indications!

AJSM 2010
28 NHL Hockey players undergoing hip arthroscopy with labral repair➢ 3.4 months was avg time to return to skating➢ All players returned to sport➢ mHHS 7095

AJSM 2017
87% (52/60) returned to play professional football after hip arthroscopy
➢ Athletes who returned went on to play an average of 3.2 seasons after surgery

• 21yo Div 1 collegiate basketball player planning to play professionally
• 6 mo right hip pain
• Failed 6 mo of PT, injections, cessation of sports
Case 1
Large cam
lesion
Labral
tear

• Labral repair
• Femoral osteoplastySurgery
Labrum being repairedLabral tear with Grade III
chondromalacia

• Labral repair
• Femoral osteoplastySurgery
Femoral
osteoplastyFocal cam
lesion

Outcome – 1.5 years post-op
Preoperative sharp pain gone within first 2 weeks
Back to dunking and cutting
Playing basketball professionally overseas
Instrument Preop 3 mopostop
12 mopostop
mHHS 67 91 100
Vail Hip Score 53 89 100
HOS-ADL 81 99 100
HOS-Sport 78 100 100

• 42yo male with 2 years of hip pain and severe mechanical symptoms
• Diagnosis of synovial chondomatosis (loose bodies) on MRI
Case 2
Large loose bodies –
synovial chondromatosis

• Labral repair
• Femoral osteoplasty
• Microfracture of acetabularcartilage defect
• 35 Loose bodies removed (synovial chondromatosis)
Surgery
10x10 loose bodies throughout jointLabral tear with Grade IV
chondromalacia

• Labral repair
• Femoral osteoplasty
• Microfracture of acetabularcartilage defect
• 35 large loose bodies removed (synovial chondromatosis)
Surgery
35 loose bodiesLabral repair

Summary
Hip pain is common and commonly missed
➢ C-sign or groin = intra-articular, but can be atypical
Location, location, location
➢ Anterior/Groin with C-sign – Intra-articular
➢ Lateral – Trochanteric Bursitis/Gluteus mediustendinopathy
➢ Posterior/Buttock – Lumbar spine pathology/SI joint

Summary
Physical Therapy always first line treatment
➢ Injections PRN - can be used diagnostically and therapeutically
➢ PT Protocol depends on location/cause:
• FAI/Arthritis/Intra-articular pain – Posterior pelvic muscle strengthening
• Lateral hip pain/Troch Bursitis – IT band stretching, gluteus medius strengthening, soft tissue mobs

Summary
Treatments
➢ Non-operative treatment
• Greater than 90% success for extra-articular causes
• Only 50% success for intra-articular causes (FAI/OA)
➢ Surgery has excellent results in right hands (90% good to excellent)
• Hip Arthroscopy
• PAO indicated when dysplasia +/- Microinstability

Hip Preservation: A Team Approach!
Orthopaedic Sports Medicine
Athletic Training
Treatment
Physical Therapy
Joint Replacement

NM West RegionHip & Knee Joint Preservation Center at CDH
• NM West Region Hip & Knee Joint Preservation Center aims to provide patients from the Midwest region and beyond with a cutting edge, multidisciplinary approach to optimizing joint function
• Goal is to provide patients with the best evidence-based non-arthroplasty treatment for relieving hip and knee pain, especially those experiencing accelerated progression towards end stage arthritis

NM West RegionHip & Knee Joint Preservation Center at CDH
• A true multidisciplinary approach to optimizing joint function
- MSK Radiology
- PM&R
- PT
- Chiropractic Care
- Primary Care Sports Medicine
- Ortho Sports Medicine
- Rheumatology
- Adult Reconstruction
Current Research Initiatives
• Create a robust database with computerized patient reported outcomes collection and surgical procedure data
Outcomes Registry Creation
• Registry will facilitate research
• Clinical studies can then be developed
Clinical Trials and Studies

NM West RegionHip & Knee Joint Preservation Center at CDH
• Mission:
To provide patients with the best evidence-based non-arthroplasty treatment for relieving hip and knee pain, especially those experiencing accelerated progression towards end stage arthritis

Sanjeev Bhatia MDOrthopaedic Surgeon, Sports Medicine
Cell 312-404-4903
Please contact us!!





























