Embed Size (px)
Citation preview

Errfish Journal of Plaslic Surger.v (1983) 36, 425-427 C 1983 The Trusteer of British Association of Plastic Surgeons
The anatomical vascular basis of the axillary fascio- cutaneous pedicled flap
G. C. CORMACK and B. G. H. LAMBERTY
Department of Anatomy, University of Cambridge and the Department of Plastic Surgery, Addenbrooke’s Hospital, Cambridge
Summary-The reliability of the axillary fascia-cutaneous flap recently described in this Journal was attributed to the presence of vessels in a fascial plexus. This paper describes the findings in anatomical studies of the vasculature in this region and highlights an important directional component in the fascial plexus at this site. Comparisons are made with other regions of the posterior trunk and the implications for pedicled fascia-cutaneous flaps elsewhere are discussed.
Tolhurst and Haeseker (1982) have recently reported in this Journal 15 clinical cases in which fascia-cutaneous flaps had been raised on the postero-lateral chest wall and transposed into the axilla for the release of post-burn scar con- tractures. All the flaps had a length to breadth ratio of 3 : 1 or more and survived in their entirety. In some cases up to 50% of the width of the base of the flap consisted of scarred skin, constituting evidence for the importance of an arterial plexus at the level of the deep fascia in maintaining blood flow to the distal part of the flap.
In that paper the authors made two statements with which we disagree. Firstly it was stated that although the fascial plexuses were first described in the leg there was no reason why they should not be present elsewhere. Secondly it was stated that there is no need to embark upon the labour of mapping the blood vessels supplying the deep fascia al1 over the body. Furthermore, there was no mention of the crucial importance of the direction of vessels at the level of the deep fascia.
This paper describes the findings in anatomical studies of the fascial plexus in this region and seeks to clarify the above points.
Method
Approximately 1,200 ml of 100% w/v barium sulphate suspension were injected into the right common carotid artery of a fresh cadaver at a pressure of 7 to 8 pounds/sq inch (4.8-5.5 x 10“ Newtons/m’) with a Lear embalming pump. The skin, fat and deep fascia were dissected off the chest wall with ligation of the majority of per- forating vessels which were labelled and their
positions recorded photographically and in writing.
The radiographic appearances of two such specimens are shown (Figs. 2 and 5). The fascial surface of each specimen was then allowed to dry in order to facilitate dissection of the fascia away from the subcutaneous fat. The fascial specimens were then X-rayed and the radiographic appear- ances are shown (Figs. 3 and 6).
Findings
The presence of a parascapular artery arising as a terminal branch of the circumflex scapular artery is not a new finding. The presence of this constant artery descending along the lateral border of the scapula was described for the first time by Nassif et
al. (1982) and used as the basis for a free flap. What this study establishes is the level beneath
the skin surface at which this vessel runs. The illustrations show how this vessel emerges by passing along the fascial septum between muscles to then turn inferiorly and travel parallel to the skin surface at the level of the deep fascia. This is a distinctly different arrangement from that per- taining in direct cutaneous flaps such as the groin flap or deltopectoral flap and fits into the current concept of fascia-cutaneous flaps. Figures 3 and 6 which are of the fascia alone, show that the parascapular artery does not lie in the sub- cutaneous fat but on the deep fascia. Lying at this level the vessel is unlikely to be affected by post-burn scarring and this enables it to support a pedicled flap for transposition into the axilla for the release of contractures.
One of the two possible arrangements is shown (Figs. l-3). In the last illustration (Fig. 3) the vessel
425
426 BRITISH JOURNAL OF PLASTIC SURGERY
Fig. 1
Fig. 2 Fig. 5
Fig. 3 Fig. 6
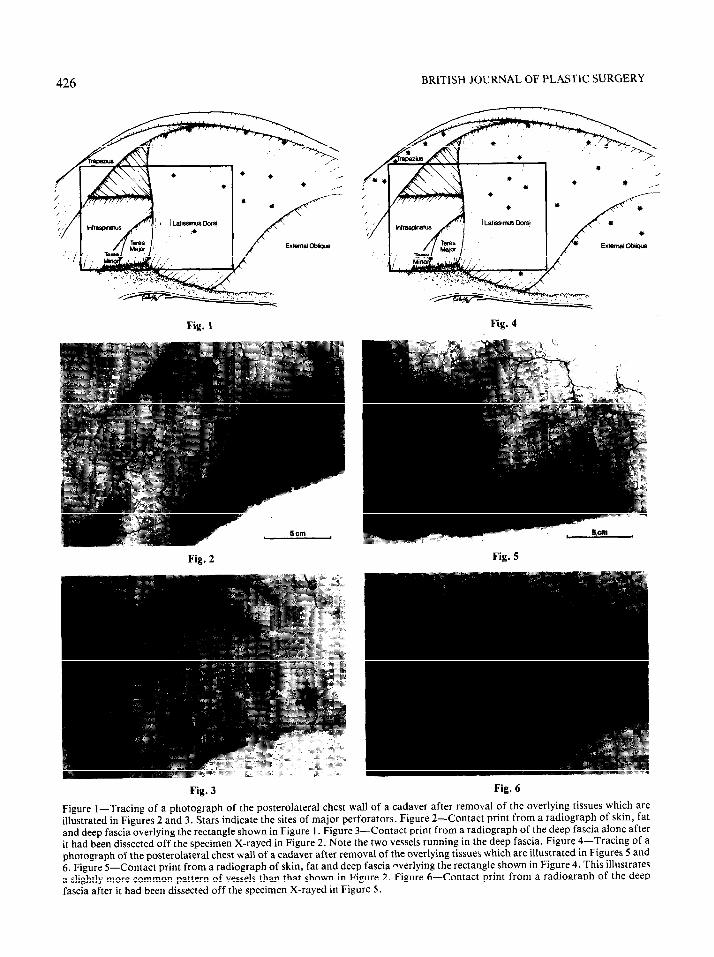
Figure l-Tracing of a photograph of the posterolateral chest wall of a cadaver after removal of the overlying tissues which are illustrated in Figures 2 and 3. Stars indicate the sites of major perforators. Figure 2-Contact print from a radiograph of skin, fat and deep fascia overlying the rectangle shown in Figure 1. Figure 3-Contact print from a radiograph of the deep fascia alone after it had been dissected off the specimen X-rayed in Figure 2. Note the two vessels running in the deep fascia. Figure 4-Tracing of a photograph of the posterolateral chest wall of a cadaver after removal of the overlying tissues which are illustrated in Figures 5 and 6. Figure 5-Contact print from a radiograph of skin, fat and deep fascia nverlying the rectangle shown in Figure 4. This illustrates
a slightly more common pattern of vessels than that shown in Figure 2. Figure 6-Contact print from a radiograph of the deep fascia after it had been dissected off the specimen X-rayed in Figure 5.

THE ANATOMICAL VASCULAR BASIS OF THE AXILLARY FASCIO-CUTANEOUS PEDICLED FLAP 427
labelled (a) is the cutaneous scapular artery which passes between teres minor and teres major and is the basis of the scapular flap. The vessel labelled (b), also from the circumflex scapular artery, passes below teres major to run inferiorly as the parascapular artery. It is more common for these two to emerge between teres major and minor as a common trunk which then divides (Figs. 4-6).
Discussion
It is our contention that the fascial plexus is not equally prevalent throughout the body. Where the blood supply of skin is dependent on musculo- cutaneous perforators from underlying flat muscles (for example, trapezius and latissimus dorsi) there is little evidence of a fascial plexus over the muscles. The perforators run almost perpen- dicular to the surface and pass directly to the subcutaneous plexus without spreading out at the level of the deep fascia. In terms of their vascular support, flaps overlying such a region may be either musculo-cutaneous or random-cutaneous in type. The deep fascia may be raised with the flap but it makes no significant contribution to the blood supply of the skin.
By contrast, in areas where the skin is supplied with blood by perforators which emerge from between longer and thinner muscles there is a fascial plexus. These fascia-cutaneous perforators do not run directly up to the overlying skin but instead branch out at the level of the deep fascia and may travel for a considerable distance at this level. In such regions elevation of the deep fascia with the flap will clearly contribute significantly to the vascular support of the overlying skin.
It is, therefore, incorrect to assume that because fascial plexuses have been shown to exist in the lower leg they must also exist everywhere else.
There is evidence from the lower leg and else- where that in a skin territory nourished by fascio- cutaneous perforators a flap will survive to a greater length for a given width if the long axis of the flap lies in the same direction as the pre- dominating direction of the fascial plexus. This statement presupposes that the fascial plexus has a clear directional component and in more recent studies (unpublished), we have shown this to be the case not only in this area but in others. It is,
therefore, our opinion that not only is it important to know where there is a fascial plexus but it is also essential to know in what direction it is running.
As we have shown, the axillary fascia-cutaneous flap coincides with an area in which a fascial vascular element is present and is directed in- feriorly approximately along the long axis of the flap.
Conclusions
Skin flaps raised to include the deep fascia in the expectation of increasing reliability, safety, and length to breadth ratios, must not be raised in a random manner but must be planned to take into account the scientific evidence for the anatomical vascular basis of fascia-cutaneous flaps. In prac- tice this means that one must know where there is a plexus and in what direction it runs.
Acknowledgements
We would like to thank Mr T. Crane, Mr R. Liles and Mr R. Overhill, AIMBI for the preparation of the illustrations and Mrs P. Morley for typing the manuscript.
References
Nassif, T. M., Vidal, L., Bovet, J. L. and Baudet, J. (1982). The parascapular flap: a new cutaneous microsurgical free flap. Plastic and Reconstructive Surgery, 69, 591.
Tolhurst, D. E. and Haeseker, B. (1982). Fascia-cutaneous flaps in the axillary region. British journalof Plastic Surgery, 35,430.
The Authors
G. C. Cormack, FRCSEd, Department of Anatomy, University of Cambridge, Cambridge.
B. G. H. Lamberty, MA, FRCS, Consultant Plastic Surgeon, Addenbrooke’s Hospital, Cambridge.
Requests for reprints to: Mr B. G. H. Lamberty, FRCS, Addenbrooke’s Hospital, Trumpington Street, Cambridge CB2 1QE.
This paper forms part of an essay entitled “Fascia-cutaneous Vessels” which was awarded joint First prize in the clinical category for the 1983 Scholarship Contest awarded by the Plastic Surgery Educational Foundation of the United States of America.





























