Embed Size (px)
Citation preview

“Terapia ormonale
sostitutiva in menopausa”
Prof. Cesare Battaglia

Menopause occurs when the ovarian
follicular pool is functionally
exhausted (Age/POF) or by surgical
removal of both ovaries
Differences in genetics, BMI, and body habitus may influence the estrogen and
androgen levels in post-menopause
The hypoestrogenic state may
affect estrogen target tissues
adversely including the brain,
skeleton, and skin as well as
the cardiovascular and
genitourinary systems
The concentrations and functions of
hormone receptors vary in these organs
and systems

Menopause occurs when the ovarian follicular pool
is functionally exhausted (Age/POF) or by surgical
removal of both ovaries
Differences in genetics, BMI, and body habitus may influence the estrogen and
androgen levels in post-menopause
The frequency and
severity of menopausal
symptoms and the
reaction of target tissues
to estrogen deficiency
significantly vary among
women

Women > 50 years
> 1.5 billion in 2030
12.5 / 60 millions (>20%)
Hormonal treatment (HT) of climacteric complaints is effective in
many women and may improve their quality of life
During the past years a prodigious amount of researches has taken place regarding advances in
postmenopausal women’s health, and it is reflected by equally extensive medical publications
In the early days of HRT it was believed that a woman could maintain her femininity and health
almost eternally by using estrogens

Traditionally, hormone
replacement therapy (HRT) has
been offered to aging women
Alleviation of vasomotor symptoms
Prevention of osteoporosis and fractures
Management of urogenital atrophy
Reduction of colon cancer
•Dementia
•Age-related macular degeneration
•Osteoarthritis
??? ???

1. Menopausal symptoms are tolerable
2. I don’t like taking medication
1. Weight gain
2. Breast tenderness or enlargement
3. Water retention/puffiness
4. Decrease in sex drive
5. Fear of endometrial/breast cancer
1. Physician didn’t think I needed them
2. Physician never brought this up
Patients convincements
Fear/side effects
Physician’s suggestions
Better compliants
1. Hystory of
hysterectomy
2. High level of education
3. High income
4. Previous OC users
HRT

48
41
28
25
USA UK Italy Thai
% HRT users
in 1990

During the past yrs a prodigious amount of researches has taken place
regarding advances in postmenopausal women’s health, and it is
reflected by equally extensive medical publications
Women Health Initiative
(JAMA, 2002)
Million Women Study
(Lancet, 2003)
???
• PATOLOGIE CARDIOVASCOLARI ( RR= 1.29)
•ICTUS (RR = 1.41)
•EMBOLIE POLMONARI ( RR = 2.13)
•CANCRO DELLA MAMMELLA ( RR = 1.26)

Pre WHI
(1990)
Post WHI
~ - 40%
HR
T i
n t
he
Worl
d

0
20
40
60
80
100
<6 mths 6-12
mths
12-18
mths
18-24
mths
>24 mths
Mean duration of the continous use of HRT (%)
6.7 %

1. Menopausal symptoms are now tolerable
2. I don’t like taking medication
1. Weight gain
2. Breast tenderness or enlargement
3. Water retention/puffiness
4. Decrease in sex drive
5. Fear of developing endometrial/breast cancer
1. Physician didn’t think I needed them
2. Physician never brought this up
Patients convincements
Fear/side effects
Physician’s suggestions

• Physician didn’t think I needed them
• Physician never brought this up
GynecologistG.P.
20%80%
Questionnaire: 52 specific questions with multiple answers
Menopause HRT
•GP (n°)
•Age (Yrs)
•Sex M vs F
(%)
1.287 136
47.5 48.2
77/23 67/33
Gynecol (n°)
Age (Yrs)
Sex M vs F (%)
Emilia-Romagna 2004-2008

Doc/Menopause/HRT
0
25
50
Decrease Increase Unchang ?
<E2 and Endometrial Ca
All data are expressed as %
*0
25
50
Decrease Increase Unchang ?
Gyn GP
<E2 and Breast Ca
*

Doc/Menopause/HRT
All data are expressed as %
0
25
50
75
Reduce Increase Unchang ?
Gyn GP
HRT and Endometrial Ca ?
0
25
50
Reduce Increase Unchang ?
HRT and Breast Ca ?

Doc/Menopause/HRT
0
25
50
75
<1 yr <5 yrs <10 yrs >10 yrs ?
Gyn GP
How long HRT ?

Doc/Menopause/HRT
1. Although Doctors correctly answered to many
questions, important cultural and comportamental errors
rose
2. The Experts need to better interact with GP and
General Gynecologyst
3. Formative and Informative meetings have to increase
and improve
4. It is mandatory that Doctors are not only informed by
Media and Industries

1. Menopausal symptoms are tolerable
2. I don’t like taking medication
1. Weight gain
2. Breast tenderness or enlargement
3. Water retention/puffiness
4. Decrease in sex drive
5. Fear of endometrial/breast cancer
1. Physician didn’t think I needed them
2. Physician never brought this up
Patients convincements
Fear/side effects
Physician’s suggestions
Better compliants
1. Hystory of
hysterectomy
2. High level of education
3. High income
4. Previous OC users
HRT

DROSPIRENONE
Is derived from spironolactone and
is, essentially, an
antimineralcorticoid progestin. In
addition, it has some
antiandrogenic actions.
In rats, the antimineralcorticoid activity was associated with reduction in
sodium and water retention due to partial suppression of the renin-
angiotensin-aldosterone system
Drospirenone has been associated with weight loss rather than weight gain
as observed in other HRT.
In a small randomised study in postmenopausal women with hypertension
treated with enalapril, Drospirenone produced an additive antihypertensive
effect.
Estranes:

-1,6
-1,2
-0,8
-0,4
0
0,4
0,8
1,2
Estradiol Angeliq
1 3 6 12 Mths
Kg
0
25
50
75
100
Abdom bloating Breast tendern Swelling of extrem
Improvement in severity of somatic
symptoms 6 mths after a HRT
switch
Weight modifications

0
20
40
60
80
Pre 8 12 16 Wks
Placebo EE+DRSP 1mg
EE+DRSP 2 mg EE+DRSP 3 mg
HOT FLASHES AND THERAPY
n°

N=15 N=15

0
40
80
120
160
Dia Mean Sys
Ang Act
8-24 h
mm
Hg6 Mths
0
40
80
120
160
Dia Mean Sys
Ang Act
24-8 h
mm
Hg

0
2
4
>140 >90 >140 >90 >120 >8024 h 8-24 h 24-8 h
%
mmHg
6 Mths Blood Pressure
Wake-up: 116±2 mmHg vs 120±3 mmHg; p=0.067
Ang
Act

34
36
38
40
42
44
Pre 30" 60" 120"
Act Ang
mm
Brachial Artery Flow-mediated
Vasodilation
Time Cuff-release
Normal flow-mediated vasodilation is approximately >10% using the
upper-arm occlusion technique
6 Mths

1
2
3
4
5
Pre 30" 60" 120"
Act Ang
PI
Brachial Artery Flow-mediated
Vasodilation
Time Cuff-release
The decreased vascular compliance may be attributable to nonenzymatic glycation of elastin and collagen in the tunica
6 Mths

1
1,5
2
Ang Act
PI
Ophthalmic Artery
Doppler Analysis
6 Mths

Traditionally, hormone
replacement therapy (HRT) has
been offered to aging women
Alleviation of vasomotor symptoms
Prevention of osteoporosis and fractures
Management of urogenital atrophy
Reduction of colon cancer
•Dementia
•Age-related macular degeneration
•Osteoarthritis
??? ???

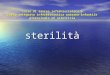
POST-VOID URINE VOLUME
V= AxBxCx0.523
VOCAL
Sono AVC

Fattori organici
Il crollo degli estrogeni e degli androgeni possono: a) influenzare negativamente
il desiderio e la risposta sessuale; b) indurre atrofia dell’epitelio vaginale con
obliterazione dei fornici e delle pliche vaginali e conseguente accorciamento
della vagina (maggiore tendenza alle infezioni)
Fattori psicologico-culturali
La cessazione delle mestruazioni e la perdita della fertilità sono vissute dalla
donna come segnali di “definitivo” invecchiamento. Pertanto il sesso, di
esclusiva pertinenza ed interesse “giovanile” va assolutamente evitato
Frequenza
e Piacere
Sessuale

2-D Ultrasonography
H.E. O’Connell, J Urol 2005
• Less Expensive and time-consuming
•Equally accurate
•Noninvasive technique
Linear array transducer was placed
on the upper part of the vulva

3-D Ultrasonography
•Less Expensive and time-consuming
•Equally accurate
•Noninvasive technique

DOPPLER US and CLITORAL BLOOD FLOW
The Clitoris is highly vascularized, and many vessels branch out in each
clitoral artery structure
Color flow images of the dorsal clitoral
artery were sampled, in a longitudinal
plane, on the outer surface of the clitoral
body
The course of the
artery was always
detectable in the
clitoral
neurovascular
bundle

DOPPLER US and CLITORAL BLOOD FLOW
The Clitoris is highly vascularized, and many vessels branch out in each
clitoral artery structure
Color flow images of the dorsal clitoral artery were sampled, in a longitudinal
plane, on the outer surface of the clitoral body

Clitoral Artery
Clitoral Vascularization at Menopause: the role of HT
1.2
1.6
2.0
18-25 yrs >50 yrs
p<0.001
Dyspareunia was present
in 57% of >1 yr
menopausal womem

Clitoral Artery
1.2
1.6
2.0
18-25 yrs Angeliq
Clitoral Vascularization at Menopause: the role of HT
0
20
40
60
MFSQ Part MFSQ Sex
Pre Post
<0.001
0.002
Dyspareunia significantly decreased
after 6 mths HT
Estrogens restore normal vaginal pH as well as
thickness and revascularize the epithelium.
Furthermore, they positively affect the Vaginal
Maturation Index (increase of superficial cells
and decrease of parabasal cells) and alleviate the
subjective symptoms of atrophy (dryness,
irritation, pruritis, urinary urgency and
dyspareunia)
Angeliq and


Clitoral Body Volume evidenced no significant differences between Groups I and II patients neither at baseline (061
0.52 mL vs. 0.65 0.38 mL) nor at the end of the study (0.64 0.55 mL vs. 0.62 0.53 mL). The resistances registered at
the level of the Dorsal Clitoral Artery did not show any differences between Group I and Group II before (1.75 0.44
vs. 1.64 0.35) and after the 3-month treatment (1.79 0.43 vs.1.65 0.29).
Genistein 45 mg/day

Labium Major
Labium Minus
Vaginal Introitus
Clitoral
Hood
A
B
L Maj
L Min
L Min
Clitoral Hood
Introitus
Labia Majora
Intro
itus
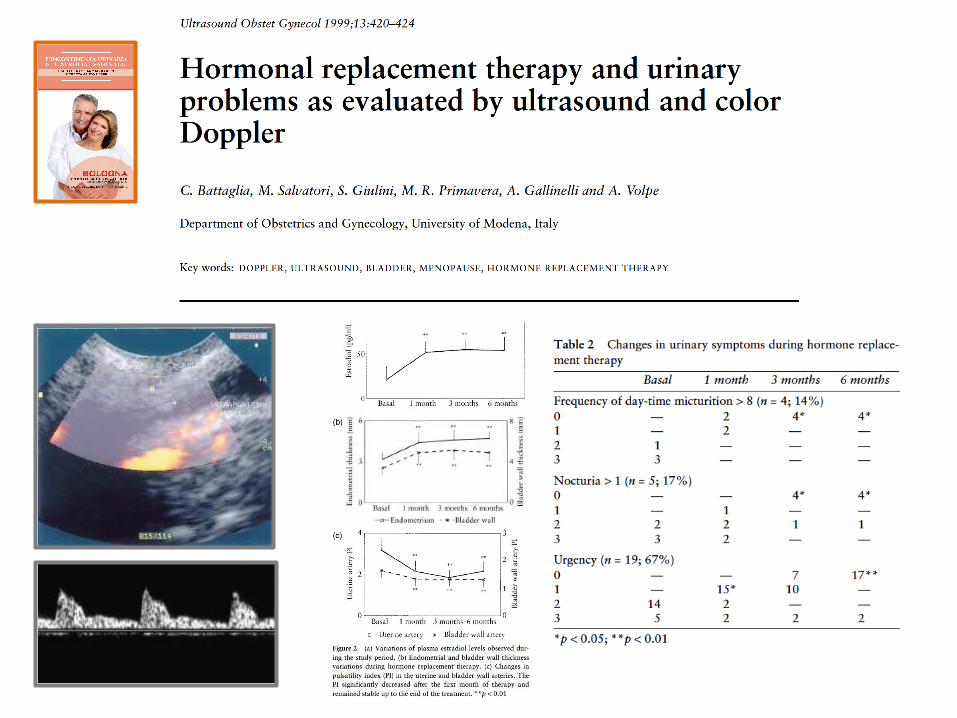
Labia Minora
C

La
bia
Min
ora
Labia Minora Vascularization

• Valutare se il calo della libido causa problemi
• Valutazione della componente psico-sociale
• Malattie croniche
• Depressione
• Anamnesi ginecologica completa
• Esame obiettivo ginecologico
• Biochimica: tiroide, anemia, PRL, profilo estrogenico
e androgenico
Management delle pazienticon calo della libido

• E vaginali -atrofia, lubrificazione
• E o EP sistemici alleviano i disturbi menopausali uro-ginecologici ma non agiscono
sulla libido
• P non benefici sfera sessuale
• T aumenta la libido, l’eccitazione e la risposta orgasmica
Approccio terapeutico

Total satisfying sexual activity at 24 weeks in
the preceding 7 days
Increased desire at 24
weeks
Donne in postmenopausa chirurgica in HRT
Donne in postmenopausa naturale
in HRT

• Tp cognitivo-comportamentale mancano studi controllati e
randomizzati
• DHEA non ci sono evidenze di efficacia
• Raloxifene non ha effetti sulla sfera sessuale
• Tibolone possibile alternativa a E+T ma servono ulteriori dati
• Flibanserin 100 mg/gg (5-HT1A agonista/5-HT2A antagonista) migliora
HSDD
• Mirtazapina (antagonista R 5HT e α2-adrenergici) migliora HSDD
nelle donne depresse ma può far nascere nuovi problemi sessuali
• Bupropione (inibitore della ricaptazione di NA e D) migliora libido,
eccitazione e orgasmo
• Bremelanotide (agonista R melanocortina) migliora desiderio e
eccitazione in donne in pre-menopausa
Ci sono alternative alla terapiaandrogenica?

Donne in
premenopausa con
HSDD
50 mg/gg
Flibanserin a tutte
Flibanserin: open label phase (sett 0-24) R Nappi

“Terapia ormonale sostitutiva in menopausa”
Prof Cesare Battaglia
Conclusions
Hormonal treatment (HT) of climacteric complaints has a low cost
and is effective in many women and may improve their quality of
life:
• Alleviation of vasomotor symptoms
• Prevention of osteoporosis and fractures
• Management of urogenital atrophy
Alternative methods as Laser Theraphy