Embed Size (px)
Citation preview

Temporal/SubtemporalCraniotomyLastUpdated:March11,2018
GeneralConsiderations
Temporalcraniotomyisasimpleapproachthathasvastapplicabilitytointra-axialandextra-axialpathologies.Thesubtemporalapproachprovidesawideoperativecorridortothefloorofthemiddlefossaandupperpetroclivalterritoriesandtheirassociatedcisterns.Morespecifically,thiscorridorreachestheanteriorupperbrainstemthroughtheanteriorpetrosectomy.
Thelateralneocorticaltemporallobeandmorespecificallythedominantsuperiorandposteriorpartsofthemiddletemporalgyriaffectimportantfunctionssuchaslanguage.Theexactfunctionoftheanteriormiddletemporalgyrusisunknown,butitmaybeinvolvedinprocessessuchascontemplatingdistance,recognitionofknownfaces,andaccessingwordmeaningwhilereading(seeWikipedia).
Theinferiortemporalgyrusisinvolvedwithvisualprocessing,associatedwiththerepresentationofcomplexobjectfeatures,suchasglobalshape.Itmayalsoprocessfaceperceptionandtherecognitionofnumbers(seeWikipedia).
IndicationsfortheProcedure
Temporalcraniotomyisbeneficialforresectionofmidtoposteriorintraparenchymalandconvexitytemporallobetumors.Thisroutealsoaffordsaccesstomidhippocampallesionsthroughthetranssulcalapproachandreacheslateralthalamictumorsandbasalcisternsthroughthetranscorticaltransventriculartranschoroidal
TheNeurosurgicalAtlas byAaronCohen-Gadol,M.D.

pathway.TheexposureoftheSylvianfissureislimited.
Asubtemporalcraniotomyismoreversatileandexposesvariousneoplasticandtumorousintraduralandextraduralpathologiesofthemiddlefossafloor,anteriorbasalcisterns,andupperclivus.Middlefossameningiomas,smallacoustictumorsandtrigeminalschwannomas,low-lyingbasilarcaput/upperbasilararteryaneurysms,andupperpetroclivalmeningiomas(throughtheanteriorpetrosalapproach)aresomeexamplesoflesionsreadilyreachedviathisroute.
Inaddition,thisapproachallowsrepairofthesuperiorsemicircularcanaldehiscence.Thesubtemporalapproachcanbeusedincombinationwiththeextendedpterionalrouteforaccesstocomplexvascularabnormalitiesoftheinterpeduncularcisternsandfibrousmulticompartmentmenigniomasfillingthemedialincisuralandparachiasmaticspace.
PreoperativeConsiderations
ThelocationoftheveinofLabbeanditsdrainagesiteintothetransversesinusshouldbeestimatedpreoperativelybasedonmagneticresonance(MR)venogramforcasesthatrequireposteriorsubtemporalexposure.Thisdrainagesiteisabout1cmsuperiortoalineparalleltothesuperiorborderofthezygomaticarchand2to5cm(mean2.9cm)posteriortotheopeningoftheexternalauditorymeatus.
Thedisplacementofotherarterialandvenousstructuresalongthemedialtentoriumshouldbedefined.Thepotentialneedforacombinedapproachtotumorswithbothsupratentorialandinfratentorialextensionsshouldbeplannedpreoperatively.
Mannitol(1g/Kg)shouldbeadministeredduringskinincisionifa

“tight”brainisexpected.Ifcorticalstimulationforfunctionalmappingiscontemplated,coldlactatedRinger’ssolutionshouldbeavailable.Inexpectationofasubtemporalapproach,Igenerallyplacealumbardrainformostpatients,regardlessoftheirtumorsize,inordertominimizetheriskoftemporalloberetractioninjuryduringintraduralorextraduralelevationofthelobe.Sincethebasalcisternsarenotreacheduntilafterelevationofthelobe,alternativeroutesforearlycerebrospinalfluid(CSF)drainageisbeneficial.
Thesurgeonispositionedattheheadoftheoperatingroomtablewiththesurgicaltechnicianateithertherightorleft,dependingonthehandednessofthesurgeon.Theanesthesiologistmaybesituatedatthefootofthetable,allowingmoreworkingroomfortheassistantandmicroscopeifnecessary.
OperativeAnatomy
Dependingontheskinincision,thesuperficialtemporalarterymayormaynotbeinvolvedinexecutionoftheapproach.Thearterytypicallyrunsonefinger-breadthanteriortothetragusandbifurcatesintoitsfrontalandparietalbranchesapproximately5cmsuperiortothezygoma.Thetemporalbranchofthefacialnerveislocatedmoreanteriorlyoverthezygomaandsuperficialtothetwolayersoftheanteriorsuperficialtemporalfascia.
Therootofthezygomaisanessentiallandmarktodefinethelevelofthemiddlefossafloor.Thislandmarkshouldbeusedforplanningtheinitialburrholeandsubsequentcraniotomy.PreservationoftheveinofLabbeisessential.Itsanatomicrelationshipsareillustratedinthefollowingimages.

Figure1:RelationshipofthecranialsuturestothetemporallobeandSylvianfissure(Topimage).NotethesquamosalsutureoverlyingtheSylvianfissure,inadditiontodelineatingthesuperiorlimitofthetemporallobe.Also,theimportanceofperformingthecraniectomytothelevelofthezygomaticarchisillustratedinthisdissection.Corticaltopographyofthetemporallobeisillustratedintheotherimages(ImagescourtesyofALRhoton,Jr).
Figure2:VenousanatomyofSylvianandposteriortemporalregions.TheveinofLabberunsavariablecoursetowardthetransversesinus,butmustalwaysbepreserved,especiallyduringcombinedapproachestotheposteriortemporalregion.Locatingthisvesseliscriticalforpreventingitsinjuryandtemporallobevenousinfarction.MiddletemporalveinshouldnotbeconfusedwiththeveinofLabbe(ImagecourtesyofALRhoton,Jr).

TEMPORAL/SUBTEMPORALCRANIOTOMY
Appropriateheadpositionisparamountforsurgeryondeepskullbaselesions.Thepatient’sheadpositionshoulddirectthesurgeontotheregionofinterestthroughapaththatallowsadequateexposureofthelesion,minimizesbrainretraction,andaffordsflexibleworkingangles.Furthermore,thepatient’sheadpositionshouldenableacomfortableergonomicbodypostureforthesurgeonduringtheoperation.
Figure3:Thepatientisfrequentlyplacedinthesupineposition(ifthepatient’sneckissupple)orrarelyinthelateralposition,iftheneckisrelativelyrigid.Thepatient’sneckshouldberotatedasmuchaspossiblewhileutilizingalargeshoulderrollunderneaththeipsilateralshouldertominimizenecktorsion.Nonphysiologicneckrotationleadstocompromisedjugularvenousreturnandpostoperativeneckpain.
Olderandheavy-setpatientsshouldbeplacedinalateralposition.Ifthepatienthasahistoryofsignificantcervical

spondylosis,thisdictatestheneedforalateralposition.Theheadisthentilted~20degreestowardthefloorforgravityretractiontomobilizethetemporallobeawayfromthemiddlefossa.
Theexactlocationandsizeofthelesionwilldeterminethecorrespondingskinincision.Ingeneral,smallerlesionsthatarewithinthesuperiorormiddletemporalgyriareamenabletolinearincisions,whereaslargesubtemporallesionsbenefitfromahorseshoe-shapedincision.Forlesionsthatrequireaccesstotheanteriortemporalpole,asmallreversequestionmarkincisionwouldbeappropriate.

Figure4:Alternativeincisionstylesandpinplacementfortemporalandsubtemporalcraniotomies.Anincisionthatextendstothelevelofthezygomashouldsparethemaintrunkofthesuperficialtemporalartery.Manualpalpationofthearteryguidesplanningofthescalpflap.Ipreferalinearincisionwhenpossiblesincethistypeofincisionhealsmorereadily.Horizontaldisconnectionofthetemporalismuscleattachmentsfromthesuperiortemporallinethroughthelinearincisionoftenmaximizesretractionofthescalpflapsandprovidesadequate

bonyexposure.
Afterplacingageneroussingleburrholejustaboveherootofthezygoma,Iusea#3Penfielddissectortomobilizetheduraawayfromtheinnertableofthecalvariuminpreparationforthecraniotomy.Ifanextraduralapproachtothemiddlefossaisplanned,itisessentialtoavoidearlyinjurytothedurainordertoprotectthelobeduringextraduralsubtemporaldissectionandpetrosectomy.
Iftheduraisadherenttotheinnerskullbone,Iplacenumerousburrholes.Thelumbardrainisusedtoremove~30to40ccofCSFgradually(in10–20ccaliquots)torelaxthebrain.Thisdrainagefacilitatesdissectionofthedurafromthecalvariumandreducestheriskofaduraltear.Acraniotomeisthenusedtocompletethecraniotomy.

Figure5:Notethelocationoftheinitialburrholenearthesigmoidsinusforlinear(top)andhorseshoe(bottom)incisions.Inthecaseofasubtemporaloperativecorridor,thecraniotomyshouldbecreatedasclosetothemiddlefossaflooraspossible.Thistaskmaybeaccomplishedbyidentifyingoneimportantlandmark:theupperedgeoftherootofzygomamarksthelevelofthemiddlefossafloor.Itisalsoimportanttorememberthatthefloorofthemiddlefossaisobliqueandslopesslightlysuperiorlyfromtheanteriortoposteriordirection.Therefore,theinferioredgeofthecraniotomyshouldbeonlyslightlyabovethelevelofthezygoma.

Figure6:Thecraniotomyinrelationtotherootofzygoma(*)isevident(top).Mostoften,theinferioredgeofthecraniotomyleavesastripofoverhangingbone,obscuringaclearoperativepathtowardthemiddlefossafloor.Subsequently,aLeksellrongeurmaybeusedtoremovethisoverhangingboneuntiltheedgeofthecraniotomyisatthelevelofthefloor(bottom).A

handhelddrillfurtherassistswiththistask.
Figure7:Removaloftheoverhangingboneovertheinferiorcraniotomywillallowanunobstructedviewofthemiddlefossafloor,minimizingtheneedfortemporalloberetraction.Thelocationoftherootzygoma(*)ismarked.ThetemporalboneandmastoidaircellsarethoroughlywaxedtopreventdevelopmentofapostoperativeCSFfistula(arrows).DuralTackupsuturesareplaced.

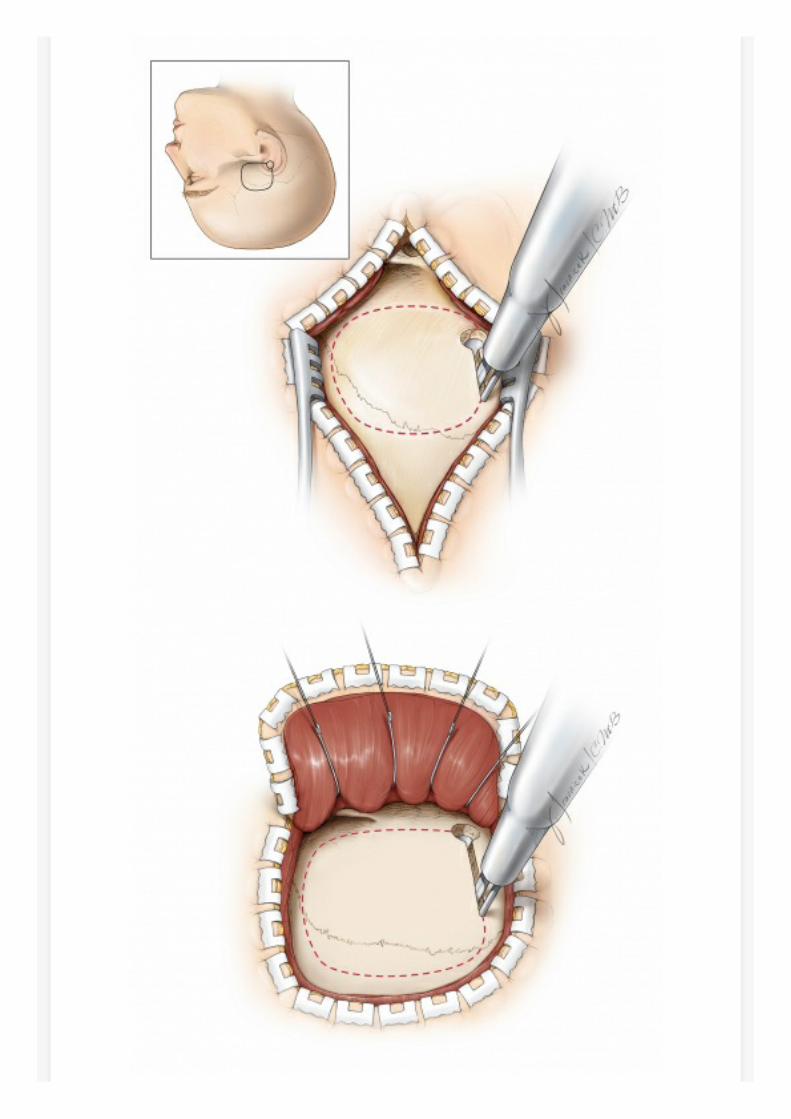
Figure8:Theduramaynowbeincised,asillustrated,forresectionofintraparenchymallesions.
Alternatively,anextraduraldissectionalongthemiddlefossamayberesumedforskullbaselesions.Importantly,thelocationoftheveinofLabbeshouldbeestimatedpreoperatively.Theduralopeningandextraduraltemporallobeelevationshouldbeadjustedforprotectionofthisvitalvenousstructure.AdditionalCSFmaybereleasedthroughthelumbardraintofurtherrelaxthelobe.
PleaserefertotheAnteriorPterosectomychapterforfurthersteps

regardingextraduralmiddlefossadissectionandpetrosalosteotomy.
Closure
Inthepresenceofaircells,Ipreferawatertightduralclosureprimarilyorsecondarilyusingapieceofduralallograft.AdiposetissuewithitsglobulartextureisoneofthebestbarriersagainstCSFleakage.Inthecaseofsubtemporalskullbaseexposuresthatrequireremovalofthetumor-infiltratedduraandbone,stripsofadiposetissueareplacedacrosstheduralopeningtosealtheduraldefect.Beforeplacementoftheadiposegrafts,allaircellsmustbemeticulouslywaxed.
Alternatively,avascularizedmuscleflappreparedfromtheposterioraspectofthetemporalismusclemayberotatedtofillthedefectwithintheboneordura.Thislattermethodisusedduringrepeatoperationsforpatientswhohavepreviouslyundergoneradiationtreatment.
Anyadditionalmastoidandtemporalaircellarerewaxed.Finally,theboneflapisreplacedandthescalpisclosedinanatomiclayers.
PostoperativeConsiderations
Postoperatively,thepatientisadmittedtotheICUforneurologicandbloodpressuremonitoringandpaincontrol.Frequentandcarefulneurologicexamsareparamountbecausetemporallobehematomascanoccurduetolobarretractioninjuryorvenousdrainagecompromise,leadingtorapidbrainstemcompression.
Thepatientisusuallytransferredtotheregularwardonthefirstorsecondpostoperativeday.LumbardrainagemaybecontinuedifthereisahighsuspicionofCSFleakage.Duetomanipulationofthetemporallobe,theuseofprophylacticantiepilepticmedicationsforatleastoneweekaftersurgeryishighlyrecommended.

PearlsandPitfalls
Duringpositioning,tiltingthepatient’sheadtowardthefloorisakeymaneuvertomaximizetheuseofgravityretractionandobtainappropriatesubtemporalexposure.Theupperedgeofthezygomaisagoodlandmarkforlocatingthelevelofthemiddlefossafloor.Removaloftheoverhanginginferioredgeofthecraniotomyisimportantforpreparinganobstructedoperativetrajectorytowardthemiddlefossafloor.ThelocationoftheveinofLabbeshouldbeestimatedpreoperatively.Duralopeningandextraduraltemporallobeelevationshouldbeadjustedforprotectionofthisvitalvenousstructure.
DOI:https://doi.org/10.18791/nsatlas.v2.ch05
References
Apuzzo.M,BrainSurgery:ComplicationAvoidanceandManagement,Volume1.ChurchillLivingstone,1983.
CamperoA,TróccoliG,MartinsC,Fernandez-MirandaJC,YasudaA,RhotonALJr.Microsurgicalapproachestothemedialtemporalregion:Ananatomicalstudy.Neurosurgery.2006;59(Suppl2)S279-308.
RhotonALJr.Thecerebralveins.Neurosurgery.2002;51(Suppl4)S159-205.
RelatedVideosAnteriorPetrosectomyforUpperPetroclivalMeningioma

RecurrentEpidermoid:AnteriorPetrosalApproach
SuperiorSemicircularCanalDehiscence
MiddleFossaCholesteatoma
TemporalCraniotomy
TemporalGlioma:MappingWernicke'sArea
RhotonCollection:NavigatingtheTemporalBone
RhotonCollection:CavernousSinusandMiddleFossa
TentorialdAVF:SubtemporalApproach
MiddleFossadAVF
HippocampalAVM
SuperiorSemicircularCanalDehiscence:SubtemporalCraniotomy

RelatedMaterialsOtherAtlases
AvailableThroughtheAtlas
UnavailableThroughtheAtlas
MeyerAtlas:TemporalApproach
Surgicaltreatmentoftrigeminalschwannomas
Extraduraltemporopolarapproachtolesionsoftheupperbasilar...
Surgicalresectionofintrinsicinsulartumors:Complicationavoi...
Cranialbaseapproachestoposteriorcirculationaneurysms
Retrogradedissectionofthetemporalismusclepreventingmuscle...
Subfascialandsubmuscularmethodsoftemporalmuscledissection...
Anteriortranspetrosal-transtentorialapproachforsphenopetrocli...
Surgicalapproachestothecavernoussinus:Amicrosurgicalstudy
Transpetrosalapproach:Surgicalanatomyandtechnique
Surgicalmanagementofacuteepiduralhematomas
Surfaceandsuperficialsurgicalanatomyoftheposterolateralcr...
Transtemporalapproachtotheskullbase:Ananatomicalstudy

Theanteriorsubtemporal,medialtranspetrosalapproachtotheup...
Orbitozygomatictemporopolarapproachforahighbasilartipaneu...
Themiddlefossatranspetrousapproachtotheanterior-superiorc...
MicrosurgicalApproachestotheMedialTemporalRegion-AnAnato...