Embed Size (px)
Citation preview

Targeting Survival and DNARepair Pathways in Chronic Lymphocytic LeukemiaDr. Lawrence Panasci

Potential Conflict of Interest
• Research Grant– Luitpold Pharmaceuticals / 2007-2009– Novartis Pharmaceuticals / 2009-

Raquel Aloyz PhD
Dr Lawrence Panasci MD
Department of Oncology& Program in Cancer Genetics
McGill university
Targeting Survival And DNA Repair Pathways In Chronic Lymphocytic Leukemia

Chronic Lymphocytic Leukemia (CLL)
• CLL is characterized by the accumulation in the blood of affected patients quiescent B-lymphocytes in the G0/G1 phase of the cell cycle.
• At an early stage of the disease, B-lymphocyte accumulation occurs likely as a consequence of an undefined defect in the apoptotic machinery rather than an increased proliferation of leukemic cells.
• While the patients often initially respond to conventional treatment with chlorambucil or fludarabine, they eventually become resistant to the drugs.

B-Cell Chronic Lymphocytic Leukemia (CLL)
1) Is a disease characterized by the proliferation of abnormal, developmentally regulated immature B lymphocytes that accumulate in the blood of affected patients
2) The nitrogen mustard (NM), chlorambucil (CLB), was commonly used as fist line therapy for CLL with an initial response rate of 60-80%, often to low dose CLB therapy, but eventually (usually after years of therapy), all CLL patients become resistant to CLB
3) Thus CLL is an excellent clinical model of NM drug resistance since:
an homogenous population of malignant B lymphocytes is easily obtainable
these malignant B lymphocytes are representative of the clinical status, i.e. in-vitro/in-vivo NM resistance and
the chronic nature of the drug treatment allows for the development of drug resistance


DNA INTERSTRANDCROSSLINK (ICL)
NER
Double Strand BreakDSB
HomologousRecombinational
Repair
DNA Interstrand Crosslink Repair
Chlorambucil
Interstrand Crosslink Removal
Non HomologousEnd joining
Repair
Non Limiting Step
Cyclophosphamide

Copyright ©1999 American Association for Cancer Research
Christodoulopoulos, G. et al. Clin Cancer Res 1999;5:2178-2184
Fig. 1

LINEAR REGRESSION Rad51 and Xrcc-3 Protein Level vs. LINEAR REGRESSION Rad51 and Xrcc-3 Protein Level vs. LDLD
5050ChlorambucilChlorambucil
In Chronic Lymphocytic LeukemiaIn Chronic Lymphocytic Leukemia

summary
• Resistance to DNA crosslinking agents is associated with:
a) Accelerated repair of interstrand crosslinks induced by these agents.
b) Increased drug-induced-Rad51 foci density.
c) In CLL primary lymphocytes increased protein levels of xrcc3/Rad51 and in epithelial cell lines increased levels of XPD and xrcc3.
3) Overexpression of xrcc3 results in DNA cross linking agent drug resistance.

UntreatedB-lymphocyte
CLB treatedB-Lymphocytes
RAD51 NUCLEAR
FOCI
DNA INTERSTRAND CROSSLINK (ICL)
NER
Double Strand BreakDSB
HomologousRecombinational
Repair
c-AblBRCA1
Sensitization to ICL-inducing agents Decreased Rad51 Foci
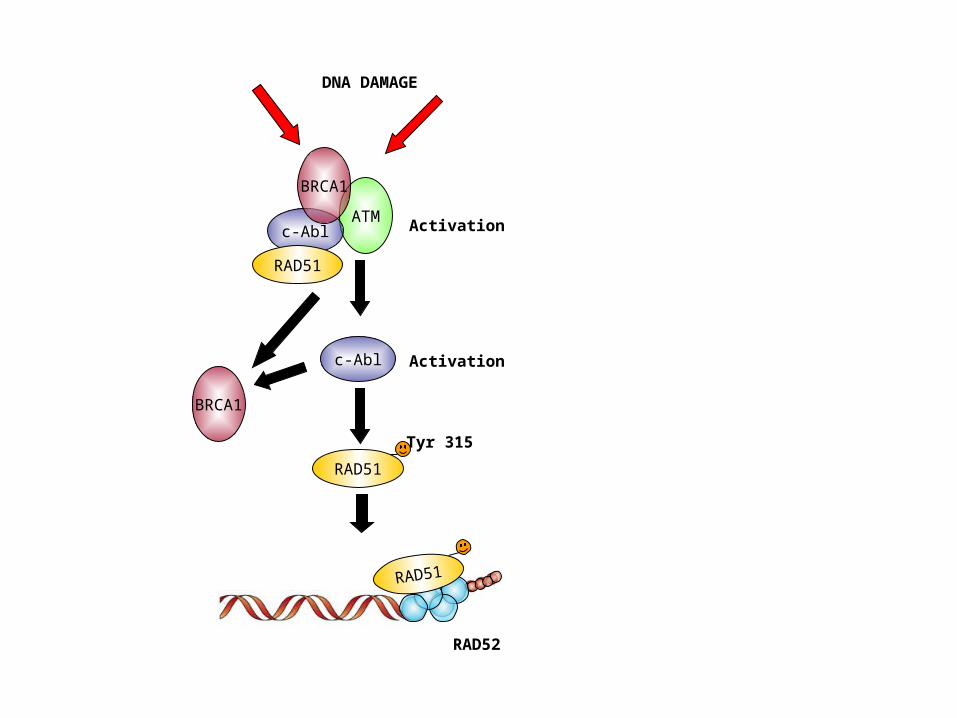
c-Abl
ATM
RAD51
DNA DAMAGE
Activation
Activation
Tyr 315
RAD52
RAD51
c-Abl
RAD51
BRCA1
BRCA1

1-c-Abl positively regulates Rad51-related Homologous Recombinational Repair
2-Homologous recombinational Repair is implicated in CLB drug sensitivity in CLL
We investigate the effect of the c-abl inhibitor Imatinib/STI571 in CLB cytotoxicity in CLL lymphocytes

STI571
REGULATED
Tyr 412
Tyr 245ACTIVE

CLB
y = 106.63e-0.026xR2 = 0.9648
IC50=29.12mM
0
20
40
60
80
100
120
0 50 100
CLB (mM)
% o
f C
on
tro
lSTI571
y = 109.53e-0.0469x
R2 = 0.9797IC50=13.72mM
0
20
40
60
80
100
120
0 20 40 60
STI571 (mM)
% o
f C
on
tro
l
CLB5mM STI571
0
20
40
60
80
100
120
0 10 20 30 40 50
CLB (mM)
% o
f Con
trol
IC50= 2.8 mM
IC50 CLB
IC50 CLB+
[ STI571]
IC50 STI571= 0.46I =
CLB5mM STI571
0
20
40
60
80
100
120
0 5 10 15
CLB (mM)
% o
f C
on
tro
l
IC50= 2.8 mM
Determination of Drug Synergy Using the MTT Assay
I< 1 Synergy I=1 Additive I> 1 Antagonism
IC50

CLB IC50 mM+ CLB IC50 mM+
5mM Imatinib 10 mM Imatinib
Patient U1 14.6 55.93 3.35; (4.0)a 0.32 3.35; (4.9) a 0.32
Patient U2 28.49 29.79 2.90; (9.6) a 0.27 2.96; (9.6) a 0.27
Patient U3 20.02 36.8 4.70; (4.2) a 0.37 4.70; (4.2) a 0.37
Patient U4 54.2 101.8 21.20; (2.6) a 0.58 21.20; (2.5) a 0.59
Patient U5 18.08 47.9 11.70; (1.5) a 0.75 13.80; (1.3) a 0.96
Patient U6 7.84 46.7 3.04; (2.5) a 0.49 ND
Patient U7 12.27 44.9 79.9 6.5 70.1 5.93
Patient T1 9.29 33.29 1.20; (7.7) a 0.28 1.09; (8.5) a 0.41
Patient T2 23.1 16.5 3.00; (7.7) a 0.42 1.10; (21.0) a 0.65
Patient T3 5.56 53.06 3.54; (1.5) a 0.72 2.67; (2.0) a 0.66
Patient T4 79.7 32.2 59.00; (1.3) a 0.88 35.20; (2.2) a 0.75
Patient T5 49.2 34 17.20; (2.8) a 0.49 ND
I ValueCLB IC50 mM Imatinib IC50 mM I Value
5.95±0.17**; (5.7) a ; 5µM STI571b
3.15±1.82**; (10.7) a ; 10µM STI571b
17.30±1.00*; (2.3) a 1.5µM STI571b
25.40±1.53*; (1.6) a ; 3µM STI571b
I Value
WSU 34.00±2.80 13.72±2.75 0.530.82
CLB IC50 mM Imatinib IC50 µM CLB IC50 CLB+Imatinib µM
I83 40.66±2.80 33.73±4.19 0.450.74
STI571(Imatinib) Sensitizes CLL cells to CLB (Chlorambucil)Independently of the clinical status

Summary of the mechanisms of action of Gleevec alone or in combination with Chlorambucil in malignant CLL-
lymphocytes
Chlorambucil Fludarabine Constitutive activation of Lyn
APOPTOSIS
•Inhibition of transcription
•Inhibition of DNA synthesis(cycling cells)
Anti apoptotic signalling DNA
damage
Survival
Dasatinib
Rad51-dependantDNA repair
c-abl kinase inhibition
Src kinase inhibition
c-Abl
Gleevec
Survivalc-abl kinaseinhibition
Chlorambucil Fludarabine Constitutive activation of Lyn
APOPTOSIS
•Inhibition of transcription
•Inhibition of DNA synthesis(cycling cells)
Anti apoptotic signalling DNA
damage
Survival
Dasatinib
Rad51-dependantDNA repair
c-abl kinase inhibition
Src kinase inhibition
c-Abl
Gleevec
Survivalc-abl kinaseinhibition
Death
SurvivalSurvival

A phase I -II Clinical Trial is in process to assess the effect of Gleevec in combination with CLB

A phase I-II trial of Gleevec (imatinib mesylate) in combination with chlorambucil in previously
treated chronic lymphocytic leukemia (CLL) patients
Study Protocol
Sponsor:Novartis Pharmaceuticals
Group/Participating Institutions:Jewish General Hospital
Hopital Notre-Dame, CHUMHopital Charles Lemoyne
Investigators: Jonathan Hebb, MD, MSc
Sarit Assouline, MD Lawrence Panasci, MD Pierre DesJardins, MD
Stephen Caplan, MD Raquel Aloyz, PhD

Rationale
• There is a synergistic effect of imatinib on CLB mediated cytotoxicity in CLL cells in vitro.
• This effect occurred at concentrations of imatinib (<10mm) that are clinically achievable.
• Drug sensitivity in CLL lymphocytes is determined in part by the repair capacity of nitrogen mustard-induced DNA interstrand cross links (ICLs).
• The regulation of this repair mechanism has been associated with a c-abl mediated phosphorylation of Rad51 which is involved in repair of CLB –induced ICLs.
• Imatinib inhibits c-abl activity; imatinib may sensitize CLL cells to CLB through inhibition of c-abl mediated DNA-repair pathways.
• Imatinib in vitro inhibits c-abl, with a resultant decrease in c-abl mediated Rad51 phosphorylation in CLB-treated CLL lymphocytes. Encouraging results from these in vitro studies provide a basis for initiating a phase I/II clinical study.

STUDY OBJECTIVES
Primary Objectives• To determine the maximum tolerated dose of Gleevec in combination with
chlorambucil(CLB).• To determine the toxicities of Gleevec in combination with CLB.
Secondary Objectives• To determine the efficacy of Gleevec at the MTD in combination with CLB. • To determine the peak/steady state plasma concentration of Gleevec at
each level, but mainly at the MTD.• To determine the amount of Gleevec sensitization of CLB in-vitro in
pretreatment lymphocytes and correlate these results with in-vivo anti-tumor activity.
• To determine the duration of response in patients who respond to Gleevec and CLB at the MTD.

SAMPLE SIZE
• Up to 18 patients will be enrolled in the phase I portion of this study, with three patients tested at each dose level of Gleevec.
• Cohorts will be expanded to 6 patients if there is one dose limiting toxicity in the first three patients enrolled in a given cohort.
• Once the maximum tolerated dose has been determined, a total of 16 patients will be enrolled in the phase II component of the study.

PATIENT POPULATION
Patients with CLL in whom treatment is clinically indicated and who have been previously treated with one or more of the following regimens:
• CLB, with a progression free survival of at least 6 months.• Fludarabine or any fludarabine containing regimen.• Any other treatment regimen including monoclonal antibodies,
corticosteroids, immunotherapies, or radiation.

Patient Eligibility
• Patients with B-cell chronic lymphocytic leukemia (a) Rai Stage 0-II with indication for treatment by NCI Working Group Criteria; or (b) Rai Stage III or IV.
• The diagnosis of CLL must be pathologically verified according to the WHO classification of hematological malignancies.
• Received a minimum of one prior chemotherapy regimen. Additionally, prior treatment with corticosteroids, immunotherapies, monoclonal antibodies or radiation therapy is permitted.
• WBC count of > 25 x 109/L.

DOSAGE REGIMEN
• Gleevec at three dose levels: 300mg, 400mg, or 600mg daily for 10 days (from day 1 to day 10), and a total fixed dose of CLB 8 mg/m2 daily x 5 days (day 3 to day 7) will be administered. The treatment will be administered every 28 days. Patients may receive up to 6 cycles of therapy.
• Dose Level Gleevec CLB No of patients -1300mg 6mg/m2 3*
1 300mg 8mg/m2 3* 2 400mg 8mg/m2 3* 3 600mg 8mg/m2 3*

Lymphocyte counts for CLL patients on protocol GL-CLB-001 (treatment started at Week 0)
0
20
40
60
80
100
120
-1 1 2 3 4 5 6 7 8 12 16 20 24 36
Ly
mp
ho
cy
te c
ou
nts
(x
10
^9
/L)
03-0103-0203-03
0
50
100
150
200
250
300
-1 1 2 3 4 5 6 7 8 12 16 20 24 36
0
50
100
150
200
250
300
350
-1 1 2 3 4 5 6 7 8 12 16 20 24 36
01-0303-05 03-0601-04
01-05
Dose Level 1 (300 mg Gleevec)
03-0401-02
Dose Level 2 (400 mg Gleevec)
Dose Level 3 (600 mg Gleevec)
Weeks

3*
600mg
Not available---PD at
Cycle3
CLB (Unk, 1 course)Flud (Unk, 1 course)Flud/Retuximab (Toxto chemo after C1)
Rai II7601-05P-O
3*600mg
N/A---Off-study at
C1(low platelets)
Chlorambucil (PR)Fludarabine (CR)Cycloph (PD)
Rai IV7701-04M-D
3*600mg
N/A
Fludarabine (PR)Cycloph/Flud (SD)R-FCM (PR)R-CHOP (PR)
Rai 15903-06M-H
3600mg
5.0 - 5.6PRPRPRFludarabine (CR)Rai I7803-05L-L
3600mg
N/A--off study (SAE - disseminated
herpes)PR
Chlorambucil (PR)CLB/Pred (PR)
Rai III8001-03F-Z
3600mg
7.0 -08.1PD (6 mth F/U)FU not done. Pt
decisionPR PRChlorambucil (PR)Chlorambucil (PR)Fludarabine (PR)
Rai III7301-02L-S
2400mg
4.5 - 8.9---
Unk Off-study at C2
(SAE-pneumonia)
Fludarabine (CR)Chlorambucil (PR)Cycloph/Fludar (PR)
Rai Ibulky
adenop49
01-01LHT
2400mg
3.8 - 6.2--PD at Cycle 4
Increased Lymphocytes
SDFludarabine (CR)Rai III8603-04T-P
2400mg
3 - 4.4CR (9 mth F/U)CR (1 mth F/U)PR PRFludarabine (PR)Rai II5703-03M-B
1300mg
6 - 9.7PD (9 mth F/U)SD (6 mth F/U)off study
(AE neutropenia)
SDFludarabine (PR)Cycloph/Flud (CR)
Rai II7103-02R-C
1300mg
10 - 14
Pt developed HodgkinsDied of pneumonitis rltdto bleomycin
PR (6 mth F/U)PR SDChlorambucil (PR)Rai II7103-01L-G
1300mg
Plasma Concentration*
2 - 4huM
Long Term Follow-Up
Best Response at Follow-up
Response on Gleevec/Chlorambucil at Cycle
5
Response on Gleevec/Chlorambucil at Cycle
3
Prior TxCurrent Staging
AgePatient
#Dose Level
3*600mg
Not available---PD at
Cycle3
CLB (Unk, 1 course)Flud (Unk, 1 course)Flud/Retuximab (Toxto chemo after C1)
Rai II7601-05P-O
3*600mg
N/A---Off-study at
C1(low platelets)
Chlorambucil (PR)Fludarabine (CR)Cycloph (PD)
Rai IV7701-04M-D
3*600mg
N/A
Fludarabine (PR)Cycloph/Flud (SD)R-FCM (PR)R-CHOP (PR)
Rai 15903-06M-H
3600mg
5.0 - 5.6PRPRPRFludarabine (CR)Rai I7803-05L-L
3600mg
N/A--off study (SAE - disseminated
herpes)PR
Chlorambucil (PR)CLB/Pred (PR)
Rai III8001-03F-Z
3600mg
7.0 -08.1PD (6 mth F/U)FU not done. Pt
decisionPR PRChlorambucil (PR)Chlorambucil (PR)Fludarabine (PR)
Rai III7301-02L-S
2400mg
4.5 - 8.9---
Unk Off-study at C2
(SAE-pneumonia)
Fludarabine (CR)Chlorambucil (PR)Cycloph/Fludar (PR)
Rai Ibulky
adenop49
01-01LHT
2400mg
3.8 - 6.2--PD at Cycle 4
Increased Lymphocytes
SDFludarabine (CR)Rai III8603-04T-P
2400mg
3 - 4.4CR (9 mth F/U)CR (1 mth F/U)PR PRFludarabine (PR)Rai II5703-03M-B
1300mg
6 - 9.7PD (9 mth F/U)SD (6 mth F/U)off study
(AE neutropenia)
SDFludarabine (PR)Cycloph/Flud (CR)
Rai II7103-02R-C
1300mg
10 - 14
Pt developed HodgkinsDied of pneumonitis rltdto bleomycin
PR (6 mth F/U)PR SDChlorambucil (PR)Rai II7103-01L-G
1300mg
Plasma Concentration*
2 - 4huM
Long Term Follow-Up
Best Response at Follow-up
Response on Gleevec/Chlorambucil at Cycle
5
Response on Gleevec/Chlorambucil at Cycle
3
Prior TxCurrent Staging
AgePatient
#Dose Level

DNA INTERSTRANDCROSSLINK (ICL)
NER
Double Strand BreakDSB
HomologousRecombinational
Repair
DNA Interstrand Crosslink Repair
Chlorambucil
Interstrand Crosslink Removal
Non HomologousEnd joining
Repair
Non Limiting Step
Cyclophosphamide

Non Homologous End Joining (NHEJ) Pathway
DNA damage recognition and processing:
•H2X2• Ku70/80•DNA-PKcs•Artemis
Ligation:
• Ku70/80•DNA-PKcs•Ligase IV/xrcc4

LINEAR REGRESSION Ku86 Protein Levels and DNA-PK activity LINEAR REGRESSION Ku86 Protein Levels and DNA-PK activity vs LDvs LD
5050ChlorambucilChlorambucil
In Chronic Lymphocytic LeukemiaIn Chronic Lymphocytic Leukemia
DN
A-P
K A
cti
vit
y (
Arb
itra
ry U
nit
s)
0
10
20
30
40
50 60
70
1
2
3
4
5
6
y=7.51x+4.0 r=0.875
y = 0.024x + 0.625
0
0.5
1
1.5
2
2.5
0 10 20 30
Ku
86
Le
ve
ls
r=0.5225
Chlorambucil IC50 (mM) Chlorambucil IC50 (mM)
Muller C et al. Blood. 1998 Oct 1;92(7):2213-9

NHEJ in CLL NM drug resistance
• KU80 protein levels and DNA-PK activity correlate directly with CLB drug resistance in-vitro in CLL lymphocytes
• These results suggest that NHEJ may play a role in CLB drug resistance in CLL
• In order to investigate this, we utilized relatively specific inhibitors of DNA-PK

NU7026
• Wortmannin, a nospecific DNA-PK inhibitor’ sensitizes CLL lymphocytes to chlorambucil.
• Wortmannin is a noncompetitive, irreversible inhibitor of DNA-PK , whereas NU7026 (2-(morpholin-4-yl)-benzo[h]chomen-4-one) is competitive inhibitor of the ATP site of DNA-PK
• Although Wortmannin is primarily a PI 3-K inhibitor, being 90-fold more active against PI 3-K than DNA-PK or ATM, NU7026 is more selective for DNA-PK with a 60-fold greater potency against this enzyme than PI 3-K and inactive against both ATM and ATR. Thus, in contrast to Wortmannin, NU7026 demonstrates excellent specificity for DNA-PK.

Effects of NU7026 and CLB on survival and DNA-PK phosphorylation
a
c
b
DNA-PK expression in I83 cell line after48h drugs treatment. NT: UntreatedBar: 10mM
a
c
b
a
c
b
DNA-PK expression in I83 cell line after48h drugs treatment. NT: UntreatedBar: 10mM
Amrein L et al J Pharmacol Exp Ther. 2007 Jun;321(3):848-55.

IC50 CLB
IC50 CLB+
[ NU7026]
IC50 Nu7026I =
I< 1 Synergy I=1 Additive I> 1 Antagonism
•We determine the IC of CLB or NU7026 alone and CLB in combination with 1, 5 or 10 mM NU7026 in vitro in a cohort of 19 B-CLL patients (14 untreated and 5 treated patients)
•The IC50 (mM) range for the drugs was: CLB 7.14 to 61.17 (I value: 0,4-2,0)NU7026 17.35 to 67.48 (non toxic (>100 mM) in 50 % of patients)
•NU7026 sensitizes the B-CLL lymphocytes to chlorambucil in all the patients but one. The effect of 1, 5 or 10 mM NU7026 on chlorambucil sensitivity was synergistic (I value<1) in 14 patients additive in one patient (I=1) and antagonistic (I>1).
NU7026 (a DNA-PK inhibitor)Sensitizes Primary B-CLL Lymphocytes to CLB in Vitro
Amrein L et al J Pharmacol Exp Ther. 2007 Jun;321(3):848-55.

PatientsIC50
(mM)CLB alone
IC50 (mM)
NU7026 alone
IC50 (mM)
CLB+1mM NU7026
Synergy Value I
IC50 (mM)
CLB+5mM NU7026
Synergy Value I
IC50 (mM)
CLB+10mM NU7026
Synergy Value I
U1 16±4.3 17±3.2 11± 3.5 (1.4)a 0.76±0.17 6±2.9 (2.6)a 0.68±0.10 3±0.4 (4.6)a 0.79±0.14
U2 27±3.7 > 100 23± 1.3 (1.2)a 0.86±0.14 12±2.8 (2.2)a 0.46±0.21 4±0.3 (7.6)a 0.13±0.03
U3 17±3.1 > 100 17± 6.4 (1.0)a 0.99±0.19 17±1.1 (1.0)a 1.00±0.12 13±3.6 (1.4)a 0.72±0.16
U4 47±5.4 41±0.2 42±4.9 (1.1)a 0.92±0.21 34±6.4 (1.4)a 0.84±0.20 7±1.3 (6.3)a 0.40±0.09
U5 25±2.0 65±4.7 29±2.3 (0.9)a 1.17±0.16 26±1.1 (1.0)a 1.11±0.18 11±2.4 (2.2)a 0.60±0.06
U6 24±6.3 67±2.7 11±3.2 (2.2)a 0.47±0.05 2.6±0.3 (9.2)a 0.18±0.04 2.3±0.8 (10.1)a 0.25±0.05
U7 52±2.8 48±5.6 29±7.8 (1.8)a 0.58±1.13 19±3.8 (2.7)a 0.47±0.07 17±3 (3.0)a 0.55±0.03
U8 9±0.8 20±2.0 24±2.3 (0.4)a 2.73±0.22 34±1.5 (0.3)a 4.05±0.20 16±4.1 (0.6)a 2.27±0.57
U9 44±3.5 > 100 29±1.4 (1.5)a 0.65±0.05 31±2.8 (1.4)a 0.71±0.14 28±1.3 (1.6)a 0.63±0.05
U10 61±3.7 39±4.8 25±1.3 (2.5)a 0.43±0.04 9.6±4.4 (6.4)a 0.28±0.02 6.8±1.1 (9.0)a 0.37±0.01
U11 7.1±2.3 20±1.7 5.1±1.0 (1.4)a 0.77±0.19 4.4±0.9 (1.6)a 0.87±0.04 2.9±0.07 (2.4)a 0.92±0.15
U12 32±3.3 33±3.9 22±1.7 (1.5)a 0.72±0.02 13±1.7 (2.5)a 0.55±0.01 12±1.6 (2.7)a 0.67±0.01
U13 31±3.1 > 100 26±2.5 (1.2)a 0.83±0.14 27±0.2 (1.1)a 0.89±0.07 21±1.1 (1.4)a 0.70±0.11
U14 12±2.8 > 100 5.9±0.2 (2.1)a 0.48±0.12 8.8±1.8 (1.4)a 0.72±0.18 6.3±1.6 (1.9)a 0.52±0.02
T1 24±5.5 24±6.2 12±3.4 (2.0)a 0.54±0.15 6.9±1.4 (3.5)a 0.49±0.09 5.9±1.9 (4.0)a 0.66±0.18
T2 59±2.8 > 100 49±5.2 (1.2)a 0.84±0.05 40±2.7 (1.5)a 0.68±0.03 17±4.5 (3.4)a 0.30±0.05
T3 32±2.2 > 100 30±3.1 (1.1)a 0.95±0.13 22±3.7 (1.4)a 0.70±0.07 14±1.3 (2.2)a 0.45±0.01
T4 43±6.0 > 100 66±5.8 (0.6)a 1.54±0.12 48±12 (0.9)a 1.11±0.37 29±2.3 (1.5)a 0.67±0.20
T5 16±0.7 > 100 10±0.8 (1.4)a 0.71±0.07 6.9±0.4 (2.1)a 0.48±0.05 5.3±1.0 (2.7)a 0.37±0.07
Effect of NU7026 on CLB cytotoxicity in lymphocytes from CLL patients
Using the MTT assay, we evaluated the effect of NU7026 on CLB cytotoxicity in malignant B lymphocytesfrom CLL patients. The I-value, I<1 or I>1, indicates that the CLB and NU7026 act synergistically orantagonistically, respectively. a Ratio between CLB IC50 alone/CLB IC50 in the presence of NU7026.The results are expressed as the mean value ± s.d. Amrein L et al J Pharmacol Exp Ther. 2007 Jun;321(3):848-55.

Copyright ©2001 American Association for Cancer Research
Panasci, L. et al. Clin Cancer Res 2001;7:454-461
Fig. 1

Dr Aloyz and myself would like to Acknowledge the following scientists
Lilian Amrein Annette HollmannTiffany A Hernandez David Davidson
CIHR- “ Dasatinib Cytotoxicity and sensitization to standard therapy in CLL” Operating Grant to R Aloyz & Leukemia & Lymphoma Society “Inhibition of DNA-PK to improve the efficacy of CLB in CLL”. Translational Research Grant to L Panasci
James JohnstonSpencer GibsonManitoba CLL tissue bank