Embed Size (px)
Citation preview

Targeted Therapies for Advanced NSCLC
Current Clinical Developments Friday, June 3, 2016
Supported by an independent educational grant from AstraZeneca
Not an official event of the 2016 ASCO Annual Meeting
Not sponsored or endorsed by ASCO or the Conquer Cancer Foundation

Disclaimer
• This slide deck in its original and unaltered format is for educational purposes and is current as of Friday, June 3, 2016. The content and views presented in this educational activity are those of the authors/presenters and do not necessarily reflect those of Creative Educational Concepts, Inc. or the supporter.
• These materials may discuss therapeutic products that have not been approved by the US Food and Drug Administration and off-label uses of approved products. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or employing any therapies or strategies described in this educational activity.

Usage Rights
• This slide deck is provided for educational purposes and individual slides may be used for personal, non-commercial presentations only if the content and references remain unchanged.
• No part of this slide deck may be published or distributed in print or electronic format without prior written permission from Creative Educational Concepts, Inc. Additional terms and conditions may apply.

1. Review the molecular pathology of lung cancer and examine its relevance for clinical practice.
2. Outline the safety and efficacy of first-line therapies for advanced NSCLC, including first generation EGFR and ALK inhibitors.
3. Evaluate treatment approaches used to overcome EGFR and ALK resistance in advanced NSCLC, including the safety and efficacy of second- and third-line therapies and recommended molecular testing.
4. Appraise emerging concepts with EGFR TKIs and ALK inhibitors, including their role in adjuvant therapy, combination therapies, and other evolving data.
Learning Objectives

Firstline Therapy for EGFR Mutant and ALK Rearranged NSCLC

Tom Stinchcombe, MD Associate ProfessorThoracic Oncology ProgramSchool of MedicineUniversity of North Carolina at Chapel HillChapel Hill, NC

• Consultant for ARIAD and Boehringer Ingelheim
• Receives Grant/Research Support from Genentech
Disclosures

Topics
• Currently available EGFR TKIs
• Treatment beyond disease progression
• EGFR TKI combinations
• ALK TKI available for first-line use: current options

Hidalgo M, et al. J Clin Oncol. 2001; Ranson M, et al. J Clin Oncol. 2002; Li D, et al. Oncogene. 2008; Kuan FC, et al. Br J Cancer. 2015; Cross DA, et al. Cancer Discov. 2014; Greig L. Drugs. 2016.
NSCLCCurrently Available EGFR TKIs
TKIsReversible
vsirreversible
EGFRm EGFRwt
HER2 [ErbB2] and
ErbB4 binding
T790Mbinding
Gefitinib,Erlotinib Reversible + + - -
Afatinib Irreversible + + + +
Osimertinib Irreversible + - - ++

Yang JC, et al. Lancet Oncol. 2015.
LUX-Lung 3 and 6 Phase III Trials Afatinib vs Cisplatin-Based Chemotherapy
• Stage IIIB/IV adenocarcinoma of the lung• Presence of EGFR mutation in the tumor tissue*• No prior treatment with chemotherapy for advanced/metastatic
disease or EGFR inhibitors• ECOG PS 0 or 1
Randomization
Afatinib40 mg orally once daily
Primary endpoint: PFS (independent review)Secondary end points: ORR, DCR, OS, PRO, safety
2:1
LUX-Lung 3 Cisplatin + pemetrexed
up to 6 cycles
LUX-Lung 6Cisplatin + gemcitabine
up to 6 cycles
*EGFR29: 19 deletions in exon 19, 3 insertions in exon 20, L858R, L861Q, T790M, G719S, G719A and G719C (or G719X), S768I
Stratification by EGFR mutation type: Del19/L858R/other and by race (LUX-Lung 3 only): Asian/non-Asian
Yang JC, et al. Lancet Oncol. 2015.
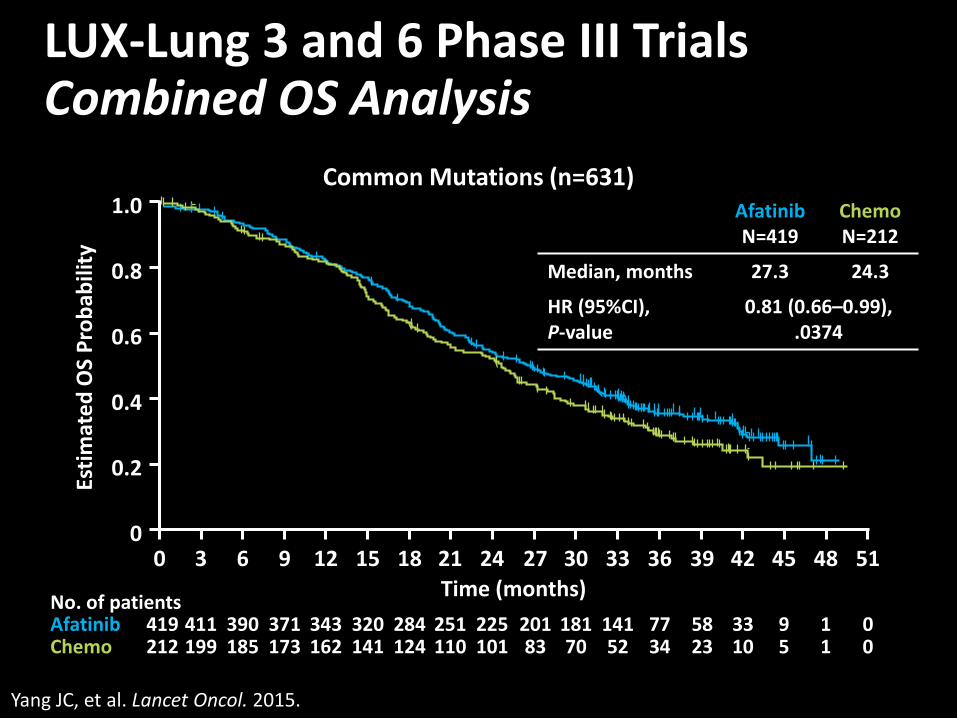
LUX-Lung 3 and 6 Phase III Trials Combined OS Analysis
AfatinibN=419
Chemo N=212
Median, months 27.3 24.3
HR (95%CI), P-value
0.81 (0.66–0.99), .0374
1.0
0.8
0.6
0.4
0.2
0
Estim
ated
OS
Prob
abili
ty
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51Time (months)
419 411 390 371 343 320 284 251 225 201 181 141 77 58 33 9 1 0212 199 185 173 162 141 124 110 101 83 70 52 34 23 10 5 1 0
AfatinibChemo
No. of patients
Common Mutations (n=631)

Yang JC, et al. Lancet Oncol. 2015.
LUX-Lung 3 and 6 Phase III Trials OS Analysis by Mutation Type
1.0
0.8
0.6
0.4
0.2
0
Estim
ated
OS
prob
abili
ty
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
Time (months)
1.0
0.8
0.6
0.4
0.2
0Es
timat
ed O
S pr
obab
ility
Time (months)
AfatinibChemo
No of patients
93 86 82 78 75 69 61 55 50 40 32 25 20 14 9 4 1 0AfatinibChemo
No of patients
Del19Afatinib N=236
Chemo N=119
Median, months 31.7 20.7
HR (95%CI) P-value
0.59 (0.45–0.77), .0001
L858RAfatinibN=183
Chemo N=93
Median,months 22.1 26.9
HR (95%CI) P-value
1.25 (0.92–1.71) .16
236 230 223 217 202 192 173 160 145 131 117 90 50 38 22 6 1 0
119 113 103 95 87 72 63 55 51 43 38 27 14 9 1 1 0 0
183 181 167 154 141 128 111 91 80 70 64 51 27 20 11 3 0 0
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
Park K, et al. Lancet Oncol. 2016.
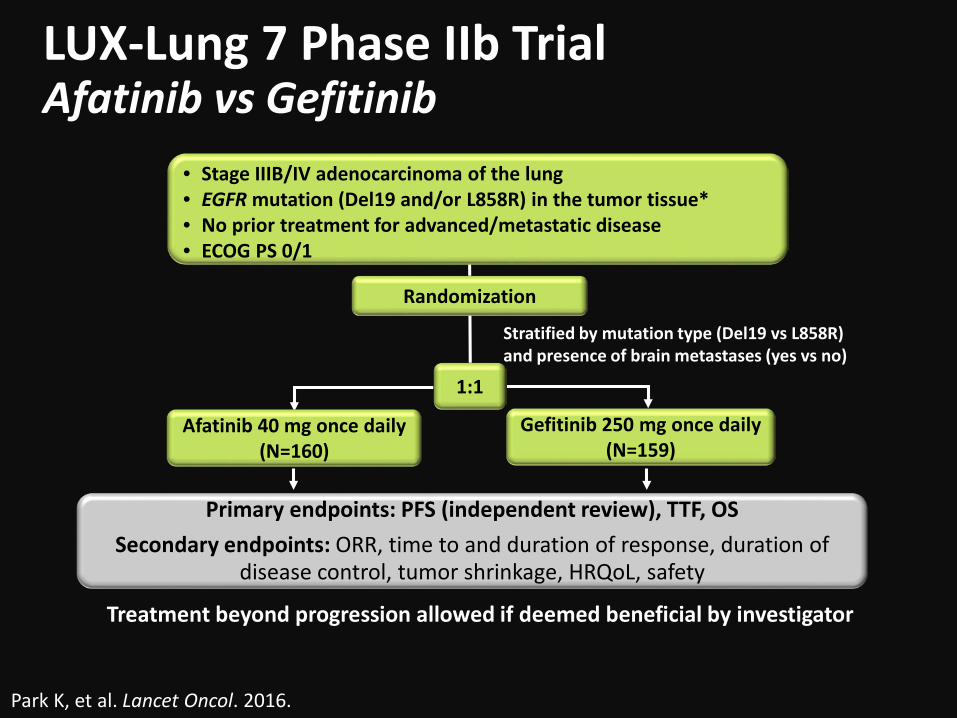
LUX-Lung 7 Phase IIb Trial Afatinib vs Gefitinib
Randomization
1:1
Afatinib 40 mg once daily(N=160)
Gefitinib 250 mg once daily(N=159)
• Stage IIIB/IV adenocarcinoma of the lung • EGFR mutation (Del19 and/or L858R) in the tumor tissue* • No prior treatment for advanced/metastatic disease• ECOG PS 0/1
Primary endpoints: PFS (independent review), TTF, OSSecondary endpoints: ORR, time to and duration of response, duration of
disease control, tumor shrinkage, HRQoL, safety
Stratified by mutation type (Del19 vs L858R)and presence of brain metastases (yes vs no)
Treatment beyond progression allowed if deemed beneficial by investigator

LUX-Lung 7 Phase IIb Trial PFS by Independent Review
Afatinib N=160
GefitinibN=159
Median PFS (months) 11 10.9
HR (95%CI), P-value
0.73 (0.57–0.95), .0165
Park K, et al. Lancet Oncol. 2016.
*P=.0176; †P=.0184
1.0
0.8
0.6
0.4
0.2
00 3 6 9 12 15 18 21 24 27 30 33 36 39 42
27%*
18%†
15% 8%
160 142 112 94 67 47 34 27 21 13 6 3 1 0AfatinibGefitinib 159 132 106 83 52 22 14 9 7 5 3 3 1 1
00
Estim
ated
PFS
pro
babi
lity
Time (months)

Park K, et al. Lancet Oncol. 2016.
LUX-Lung 7 Phase IIb Trial ORR and DCR
Efficacy Parameter Afatinib (N=160)
Gefitinib (N=159) P
ORR 70% 56% .0083(OR=1.87)
DCR 91% 87% .24(OR=1.55)
ORR Exon 19 (N=186) 73% 66%
ORR Exon 21 L858R (N=133) 66% 42%
DCR=disease control rate; OR=odds ratio; ORR=overall response rate.

Park K, et al. Lancet Oncol. 2016.
LUX-Lung 7 Phase IIb Trial Select Drug-Related AEs
AE category Gr 1-2 Gr 3 Gr 4 Gr 1-2 Gr 3 Gr 4 Diarrhea 78% 12% 1% 60% 1%
Rash/acne 79% 9% 78% 3%
Stomatitis 60% 4% 24%
Paronychia 54% 2% 16% 1%
Fatigue 15% 6% 14%
Nausea 15% 1% 14%
Vomiting 11% 3% 1%
AST/ALT increased 10% 16% 8% 1%
ILD 0% 1% 1% 1%
Afatinib Gefitinib
Drug-related AE leading to dose reduction: afatinib 39% doses reduced to 30 mg daily, 13% reduced to 20 mg
AE = Adverse Event

Treatment Beyond Disease Progression

Park K, et al. JAMA Oncol. 2016.
ASPIRATION Phase II Trial Post-Progression Erlotinib
EGFR mutant NSCLCStage 4 diseasePS 0-2(N=207)
Erlotinib 150 mg
daily
Disease progression with symptomatic progression, rapid
progression, worsening PS, or life threatening complications
93 continued erlotinib
(54%)
78 discontinued erlotinib(46%)
70 patients with PFS 2 event
14 still on erlotinib9 patients withdrew
Primary end-point: • First PFS event (PFS1)
Secondary end-points:• Second PFS event
(PFS2), ORR, OS DCR

Park K, et al. JAMA Oncol. 2016.
ASPIRATION Phase II Trial Results of Erlotinib Continuation
Median PFS1: 11.0 (95% CI, 9.2-11.0)93 patients continuing erlotinibMedian PFS2: 14.1 (95% CI, 12.2-15.9)Difference in median: 3.1 months
Patients continuing erlotinib: Patient characteristics (P<0.05):More likely to have recurrent disease at baseline, ECOG PS 0 or 1 at PFS1 Treatment characteristics (P<0.05):Longer PFS1, improved depth of response, longer time from median time from BOR to PFS10 10 20 30 40
0
0.2
0.4
0.6
0.8
1.0
Time, mo
Prog
ress
ion-
Free
Sur
viva
l Pro
babi
lity
PFS1PFS2
No. at riskPFS1 93 52 10 0 0PFS2 93 70 27 9 0
Park K, et al. Lancet Oncol. 2016.
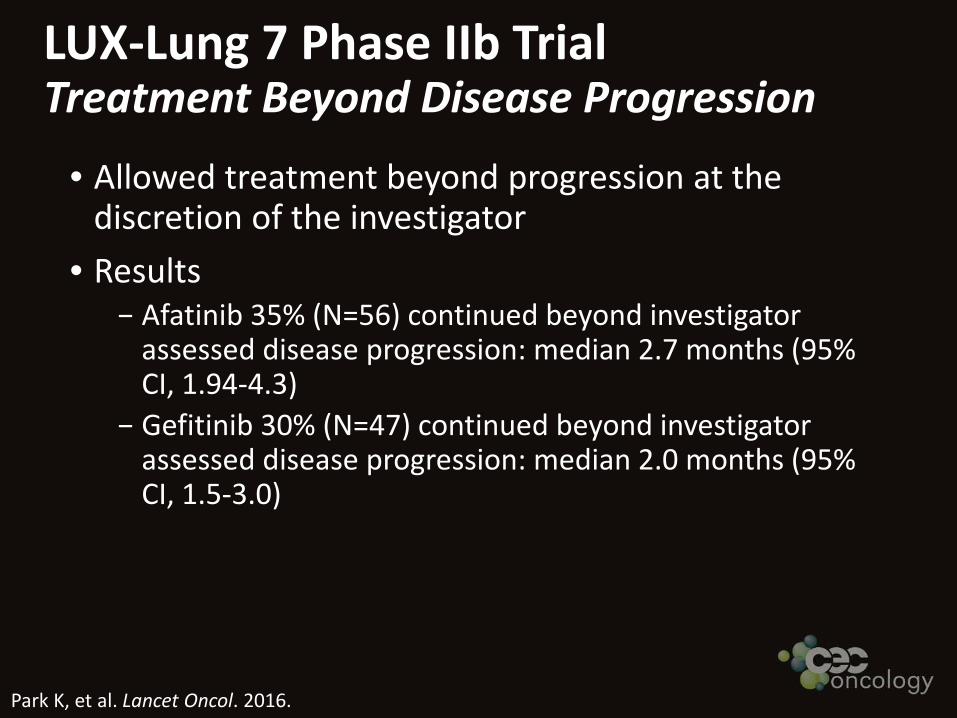
LUX-Lung 7 Phase IIb Trial Treatment Beyond Disease Progression
• Allowed treatment beyond progression at the discretion of the investigator
• Results− Afatinib 35% (N=56) continued beyond investigator
assessed disease progression: median 2.7 months (95% CI, 1.94-4.3)
− Gefitinib 30% (N=47) continued beyond investigator assessed disease progression: median 2.0 months (95% CI, 1.5-3.0)

EGFR TKI Combination Trials for First-line Therapy

Seto T, et al. Lancet Oncol. 2014.
JO25567 Phase II TrialErlotinib +/- Bevacizumab
• Stage IIIB/IV NSCLC• EGFR exon 19 deletion
or exon 21 L858R• No brain metastases
Erlotinib 150 mg daily (N=75)
Erlotinib 150 mg daily +bevacizumab 15 mg/kg every 3 weeks (N=75)Primary end-point: PFS by IRC
Secondary end-points: OS, ORR,DCR, QoL

Seto T, et al. Lancet Oncol. 2014.
JO25567 Phase II Trial PFS by Independent Review
1.0
00
75 72 69 64 60 53 49 38 30 20 13 8 4 4 077 66 57 44 39 29 24 21 18 12 10 5 2 1 0E
EBNumber at risk
Time (months)4 8 122 6 10 14 18 22 2616 20 24 28
0.2
0.4
0.6
0.8
PFS
prob
abili
ty
9.7 16.0
EBE
*log-rank test, two-sided
EB E
Median, months 16 9.7
HR P-value*
0.54 (95% Cl, 0.36–0.79) .0374
Seto T, et al. Lancet Oncol. 2014.
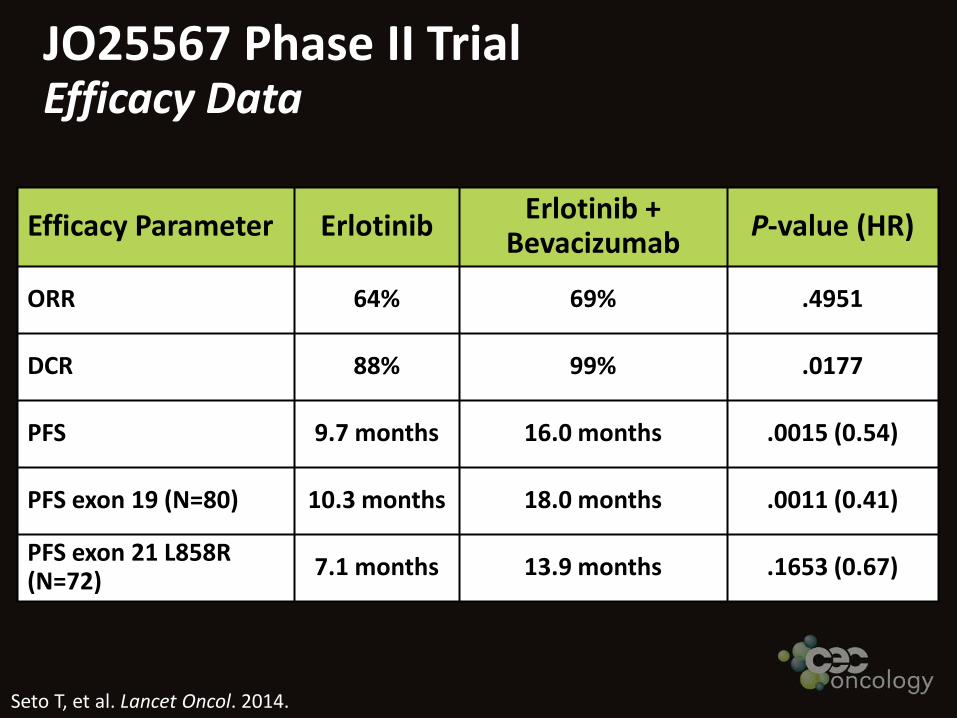
JO25567 Phase II Trial Efficacy Data
Efficacy Parameter Erlotinib Erlotinib + Bevacizumab P-value (HR)
ORR 64% 69% .4951
DCR 88% 99% .0177
PFS 9.7 months 16.0 months .0015 (0.54)
PFS exon 19 (N=80) 10.3 months 18.0 months .0011 (0.41)
PFS exon 21 L858R(N=72) 7.1 months 13.9 months .1653 (0.67)

Seto T, et al. Lancet Oncol. 2014.
JO25567 Phase II Trial Safety Data
Adverse event Grade 3 Grade 4 Grade 3 Grade 4Rash 25% 0% 19% 0%
Diarrhea 1% 0% 1% 0%
Paronychia 3% 0% 4% 0%
Dry skin 3% 0% 0% 0%
Stomatitis 1% 0% 3% 0%
Liver tests 7% 1% 9% 9%
Hypertension 60% 0% 8% 0%
Hemorrhagic event 3% 0% 0% 0%
Proteinuria 8% 0% 0% 0%
Erlotinib + Bevacizumab (N=75)
Erlotinib(N=77)

Stahel RA, et al. ECC. 2015.
BELIEF Phase II Trial Firstline Erlotinib/Bevacizumab
Patient cohort Number of patients ORR Median PFS (months)Intent-to-treat 109 76% 13.8 (95% CI, 10.3-21.3)
T790M positive 37 70% 16.0 (95% CI, 13.1-NE)
T790M negative 72 79% 10.5 (95% CI, 9.2-16.2)
• Stage IIIB/IV• Exon deletion 19
or exon 21 L858R
Erlotinib 150 mg daily + bevacizumab 15 mg/kg
every 3 weeks
• Primary end-points: PFS in pretreatment T790M+ and T790M-
• T790M mutations centrally tested using TaqMan assay in presence of PNA

Ichihara E, et al. J Thorac Oncol. 2015.
1001 Phase II TrialFirstline Gefitinib/Bevacizumab
Efficacy parameter Results
ORR 73.8% (95% CI, 58-86.1)
Median PFS 14.4 (95% CI, 10.1-19.2)
1-year PFS 56.7% (95% CI, 39.9-70.5)
Exon 19 (N=24) vs L858R (N=16) 18.0 vs 9.4 months, P=.006
• Stage IIIB/IV • Exon 19 deletion
or exon 21 L858R
Gefitinib 250 mg daily + bevacizumab
15 mg/kg every 3 weeks (N=42)
Primary end-point:
1-year PFS rate

Janjigian YY, et al. Cancer Discov. 2014.
Dual EGFR InhibitionPhase Ib Trial: Afatinib + Cetuximab
• Prior erlotinib or gefitinib within 30 days
• EGFR mutation required in MTD cohort
• T790M+ and T790M− patients enrolled
Afatinib 40 mg daily and
cetuximab500 mg/m2 every
2 weeks(N=126)

Janjigian YY, et al. Cancer Discov. 2014.
Afatinib + CetuximabEfficacy and Safety Data
Cohort ORR PFSExpansion cohort (N=126) 29% 4.7 months
T790M+ (N=71) 32% (95% CI, 21.8-44.5) 4.8 months
T790M– (N=53) 25% (95% CI, 13.8-38.3) 4.6 months
Adverse event All Grades Grade 3 Grade 4Rash 90% 20% 0%
Diarrhea 71% 6% 0%
Nail effects 57% 0% 0%
Stomatitis 56% 1% 0%
Fatigue 47% 2% 1%
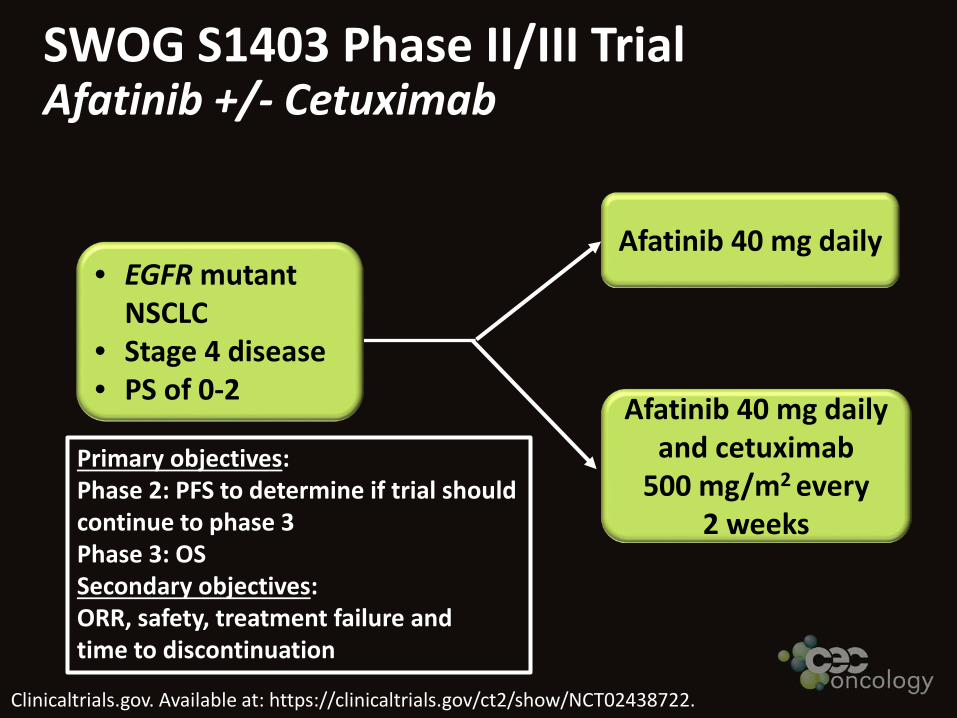
Clinicaltrials.gov. Available at: https://clinicaltrials.gov/ct2/show/NCT02438722.
SWOG S1403 Phase II/III TrialAfatinib +/- Cetuximab
• EGFR mutant NSCLC
• Stage 4 disease• PS of 0-2
Afatinib 40 mg daily
Afatinib 40 mg daily and cetuximab
500 mg/m2 every 2 weeks
Primary objectives:Phase 2: PFS to determine if trial shouldcontinue to phase 3Phase 3: OSSecondary objectives:ORR, safety, treatment failure and time to discontinuation

First-line Therapy for ALKRearranged NSCLC

PROFILE 1014 Phase III StudyFirstline Crizotinib vs Chemotherapy
Solomon BJ, et al. N Engl J Med. 2014.
Key Entry Criteria● ALK-positive by
central FISH testing● Locally advanced,
recurrent, or metastatic non-squamous NSCLC
● No prior systemic treatment for advanced disease
● ECOG PS 0−2● Measurable disease● Stable treated brain
metastases allowed
Crizotinib250 mg twice daily
PO, continuous Dosing (N=172)
Pemetrexed 500 mg/m2
+ cisplatin 75 mg/m2
or carboplatin AUC 5–6 every 3 weeks
for ≤6 cycles(N=171)
Endpoints
● Primary– PFS (RECIST 1.1,
independent radiologic review [IRR])
● Secondary– ORR– OS– Safety – Patient-reported
outcomes (EORTC QLQ-C30, LC13)
RANDOMIZE
Crossover to crizotinib permitted after progression

PFS
prob
abili
ty (%
)
100
80
60
40
20
00 5 10 15 20 25 30 35
Time (months)172 120 65 38 19 7 1 0171 105 36 12 2 1 0 0
No. at riskCrizotinibChemotherapy
PROFILE 1014 Phase III StudyPFS as Assessed by IRC
Solomon BJ, et al. N Engl J Med. 2014.
CrizotinibChemotherapy
CrizotinibN=172
Chemo N=172
Events, n (%) 100 (58) 137 (80)
Median, months 10.9 7
HR (95%CI) 0.45 (0.35–0.60)
ORR 74% 45%
P-value <.0001

J-ALEX Phase III Study Alectinib vs Crizotinib
• ALK + NSCLC• ALK treatment naive • ALK positive by
central testing• PS 0-2
Crizotinib 250 mg po twice daily
Alectinib 300 mg po BID
Primary end-point: PFS by IRRSecondary end-point:OS, ORR, CNS progression, HRQoL
JAPIC Clinical Trials Information. Available at: http://www.clinicaltrials.jp/user/showCteDetailE.jsp?japicId=JapicCTI-132316.

J-ALEX Phase III Study Alectinib vs Crizotinib
• ALK + NSCLC• ALK treatment naive • ALK positive by
central testing• PS 0-2
Crizotinib 250 mg po twice daily
Alectinib 300 mg po BID
Primary end-point: PFS by IRRSecondary end-point:OS, ORR, CNS progression, HRQoL
JAPIC Clinical Trials Information. Available at: http://www.clinicaltrials.jp/user/showCteDetailE.jsp?japicId=JapicCTI-132316.
Closed by IDMC at preplanned interim analysis after207 patients enrolled since primary end-point of PFS met
Nokihara et al Abstract 9008: Oral abstract sessionMonday June 6th 9:45-12:45
Arie Crown Theater
Conclusions
• Erlotinib, gefitinib, and afatinib are all options in the first-line setting.
• Combination trials reveal promising activity • Continuing therapy beyond disease
progression is an option for select patients.−Most likely delays a change in therapy by 2-3
months • Crizotinib is the standard for ALK+ NSCLC,
but I eagerly await Monday’s presentation.

Thank you!Please visit us at: www.ceconcepts.com





























