Embed Size (px)
Citation preview

TAF – an overviewWho? When? How?
co-infected/ monoinfected
Dr Kosh AgarwalInstitute of Liver StudiesKing’s College Hospital
ICVH Chicago 2017

Disclosures
I am a Hepatologist
Involved in the global TAF program
EASL panel
Abbvie, Astellas, Achillion, BMS, Gilead, Merck, Intercept, Vir
Acknowledge R Byrne

3 - GILEAD CONFIDENTIAL AND PROPRIETARY DRAFT. FOR INTERNAL USE ONLY. NOT FOR DISTRIBUTION OR PROMOTION.3 - GILEAD CONFIDENTIAL AND PROPRIETARY DRAFT. FOR INTERNAL USE ONLY. NOT FOR DISTRIBUTION OR PROMOTION.
TFV
HEPATOCYTE
TFV
OAT1 & 3OAT
1 & 3
OAT 1 & 3OAT 1 & 3
RENAL TUBULAR
CELL
TFV
RENAL TUBULAR
CELL
PLASMA
~90% LOWERPLASMA TFV
ESTER
AMIDATE
DIANION
TDF(tenofovir disoproxil
fumarate)
300 mg
TAF(tenofovir
alafenamide)25 mg
TFV(tenofovir)
longer plasma half-life † - greater plasma stability
short plasma half-life†
TFV HBV
GI TRACT
Tenofovir alafenamide (TAF) – A Novel Prodrug of Tenofovir
Prodrug Pharmacology
TFV-DP
† T1/2 based on in vitro plasma data - TDF = 0.4 minutes, TAF = 30-90 minutes. Lee W et. Antimicr Agents Chemo 2005;49(5):1898-1906. Birkus G et al. Antimicr Agents Chemo 2007;51(2):543-550. Babusis D, et al. Mol Pharm 2013;10(2):459-66. Ruane P, et al. J Acquir Immune Defic Syndr 2013; 63:449-5. Sax P, et al. JAIDS 2014. 2014 Sep 1;67(1):52-8. Sax P, et al. Lancet 2015. Jun 27;385(9987):2606-15. Agarwal K et al. J Hepatology 2015; 62: 533-540; Buti M et al. Lancet G&H 2016; doi: 10.1016/S2468-1253(16)30107-8; Chan HLY et al. Lancet G&H 2016; doi: /10.1016/S2468-1253(16)30024-3
‡

Older patients: risk of co-morbidities in European real-world cohorts
1. Marcellin P, et al. Dig Dis Sci 2016;61:3072–83; 2. Petersen J, et al. Dig Dis Sci 2016;61:3061–71 DDI: drug–drug interaction
0
2
4
6
8
10
12 10.9
9.1
3.6 3.4 3.22.3 2.1
6.07.0
5.0
2.0 2.0
Pa
tie
nts
(%
)VIREAL cohort (n=440)1
Mean age 45 years (11% ≥65 years)Treatment experienced: 59%
GEMINIS cohort (n=400)2
Mean age 45 years (9% ≥65 years)Treatment experienced: 54%
Consider DDIs if using polypharmacyto manage co-morbidities
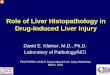
Multiple factors affect CHB disease progression
Fattovich G. Semin Liver Dis 2003;23:47–58, Fattovich G, et al. J Hepatol 2008;48:335–52
Patient
Many factors affect CHB disease progression

Gill, Zissimopoulos et al., J. Infect Dis. 2014
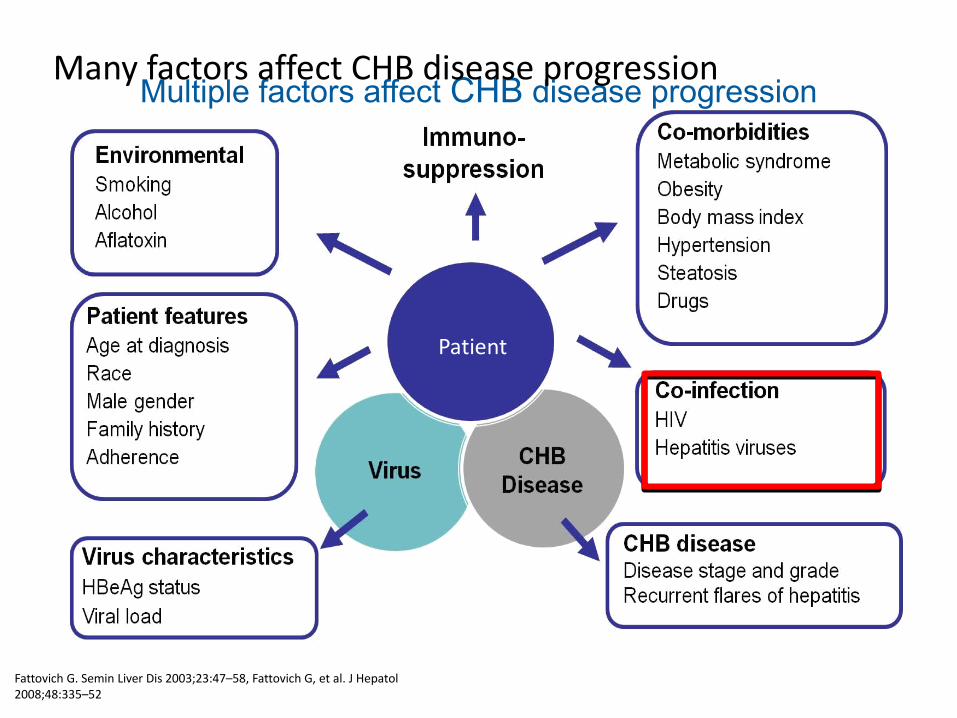
Study 108 and 110: Phase 3 CHB Studies: TAF vs TDF
Submitted to J Hep

Antiviral Efficacy of TAF and TDF at Week 48Study 108 and 110: Phase 3 CHB Studies: TAF vs TDF
Seto, AASLD 2016, Oral 67
0.0 8.0 16.024.032.040.048.056.064.072.00
20
40
60
80
100
Week
0
20
40
60
80
100
Week0.0 8.0 16.024.032.040.048.056.064.072.00
20
40
60
80
100 TAFTDF
Week
Prop
orti
on o
f Pat
ient
s, %
(95%
CI)
0
20
40
60
80
100 TAFTDF
Week
Prop
ortio
n of
Pat
ient
s, %
(95%
CI)
HBeAg+
Rates of Viral SuppressionHBV DNA <29 IU/mL
HBV DNA suppression rates were lower in HBeAg+ vs HBeAg− patients No significant difference between TAF and TDF No resistance was detected through 48 weeks
HBV DNA suppression was comparable between TAF and TDF treatment up to Week 72
Treatment difference +1.8 (-3.6, +7.2); p=0.47 Treatment difference: −3.6 (−9.8, 2.6); p=0.25
TAF: 64% TDF: 67%
TAF: 94% TDF: 93%
HBeAg-
4.0 8.0 12.0 16.0 20.0 24.0 28.0 32.0 36.0 40.0 44.0 48.0 56.0 64.0 72.00
20
40
60
80
100
TAF TDFPatie
nts W
ith A
LT N
orm
aliza
tion,
%
AASLD Criteria¤
*†
†
†‡
‡‡‡‡‡‡‡‡‡‡
*
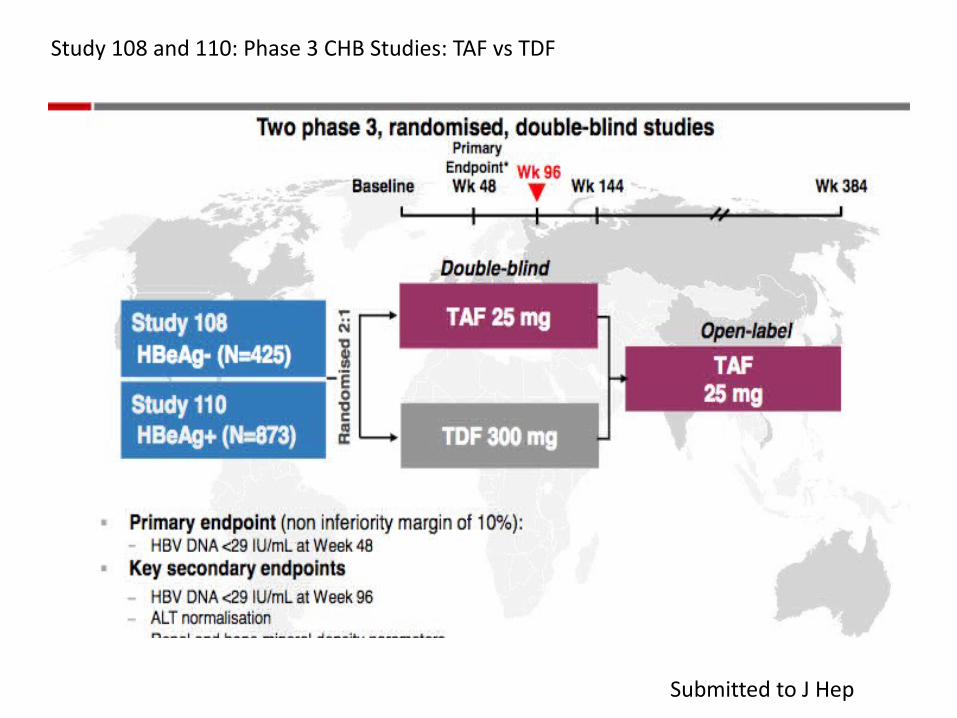
ALT Normalisation of TAF and TDF at Week 72
Fung, AASLD 2016, Poster 1852; Data on File, Gilead Sciences Inc.
Study 108 and 110: Phase 3 CHB Studies: TAF vs TDF
Significantly higher ALT normalisation rate with TAF vs TDF4.0 8.0 12.0 16.0 20.0 24.0 28.0 32.0 36.0 40.0 44.0 48.0 56.0 64.0 72.0
0
20
40
60
80
100
Patie
nts W
ith A
LT N
orm
aliza
tion,
%
*p<0.05†p<0.005‡p 0.001
Central Lab Criteria§
‡‡
‡
**
* * * * *† †
¤ <19 and <30 U/L for females and males, respectively§ 34 and 43 U/L for females and males, respectively, aged <69 y, and 32 and 35 U/L, respectively, aged >69 y
TAF: 49.1%TDF: 39.0%
TAF: 76.1%TDF: 68.4%

Renal Laboratory Parameters in CHB Patients Treated with TAF or TDF
• Smaller eGFR declines with TAF vs TDF in patients with older age and those with comorbid conditions (HTN/DM/CVD)
Agarwal, AASLD 2016, Poster 1844
In patients at greater risk for kidney disease, TAF treatment resulted in smaller declines in eGFRCG and fewer patients showed CKD stage worsening compared
with TDF treatment*p-values from Wilcoxon 2-sample test; †Hypertension (HTN), diabetes mellitus (DM), and cardiovascular disease (CVD) determined by medicalhistory or concomitant medication.
Study 108 and 110: Phase 3 CHB Studies: TAF vs TDF
Age <50 y Age ≥50 y
-6
-4
-2
0
-0.4
-3.4
-4.8-5.4
Med
ian
eGFR
Cha
nge,
%
n=5 n=8
Age
n=642 n=294 n=185 n=123
P<0.001 P=0.01
No HTN/DM/CVD HTN/DM/CVD
-10
-5
0
-0.6
-3.4
-4.8
-7
Med
ian
eGFR
Cha
nge,
%
n=5 n=8
Comorbid Conditions
n=691 n=136 n=337 n=80
P<0.001 P=0.003

TAF Phase 3: Week 96 Results
TAF Group Performance Relative to TDF Group Week 48 Week 96
Viral Suppression Non-inferior Non-inferior
ALT Normalization Significantly Better Significantly Better
Bone Safety Significantly Better Significantly Better*
Renal Safety Significantly Better Significantly Better*
Viral Resistance None None
early biomarkers ≠clinical endpoints

Management of HIV co-infected patients
EASL 2017 CPG HBV, J Hepatol 2017
Recommendations:
1) All HIV-positive patients with HBV co-infection should start antiretroviral therapy (ART) irrespective of CD4 cell count. (Evidence level II-2, grade of recommendation 1)
2) HIV-HBV co-infected patients should be treated with a TDF- or TAF-based ART regimen. (Evidence level I for TDF, II-1 for TAF, grade of recommendation 1)

NA for naïve CHB patients
EASL 2017 CPG HBV, J Hepatol 2017
Recommendations:
1) The long-term administration of a potent NA with high barrier to resistance is the treatment of choice regardless of the severity of liver disease. (Evidence level I, grade of recommendation 1)
2) The preferred regimens are ETV, TDF and TAF as monotherapies. (Evidence level I, grade of recommendation 1)
3) LAM, ADV and TBV are not recommended in the treatment of CHB. (Evidence level I, grade of recommendation 1)

Indications for selecting ETV or TAF over TDF*
EASL 2017 CPG HBV, J Hepatol 2017
* TAF should be preferred to ETV in patients with previous exposure to nucleoside analogues.
** ETV dose needs to be adjusted if eGFR <50 ml/min; no dose adjustment of TAF is required in adults or adolescents (aged at least 12 years and of at least 35 kg body weight) with estimated creatinine clearance (CrCl) 15 ml/min or in patients with CrCl <15 ml/min who are receiving haemodialysis.
SurvivalSurvival EfficacyEfficacy TolerabilityTolerability
HIV

Background
• Tenofovir disoproxil fumarate (TDF) is included in most recommended antiretroviral regimens, and although potent and generally well tolerated, has been associated with clinically significant renal and bone toxicity1-3
• Relative to TDF 300 mg, tenofovir alafenamide (TAF) 25 mg has 90% lower circulating plasma TFV, while maintaining high antiviral activity4
16
1. DeJesus E, et al. Lancet 2012;379:2429-38; 2. Gallant JE, et al. J Infect Dis 2013;208:32-9; 3. Sax PE, et al. Lancet 2012;379:2439-48; 4. Ruane P, et al. J Acquir Immune Defic Syndr 2013; 63:449-55.
FDA TAF Timeline
• Elvitegravir/cobicistat/emtricitabine/TAF - Genvoya; approved November 2015
• Emtricitabine/rilpivirine/TAF- Odefsey; approved March 2016
• Emtricitabine/TAF- Descovy; approved April 2016
• TAF (compensated HBV)- Vemlidy; approved November 2016

E/C/F/TAF QD
TAF as initial HIV Therapy: Studies 104 and 111
18
Tx-Naïve AdultsHIV-1 RNA ≥1000 c/mLeGFR ≥50 mL/min
1:1
E/C/F/TDF QD (Stribild, STB)
n=866
n=867
Two Phase 3 randomized, double-blind, double-dummy, active-controlled studies
– Study 104 (North America, EU, Asia), Study 111 (North America, EU, Latin America)
– Stratified by HIV-1 RNA, CD4 cell count, geographic region
Primary endpoint: proportion of patients with HIV-1 RNA <50 copies/mL (Taqman 2.0)
– Non-inferiority (12% margin) based on Week 48 FDA snapshot analysis
– Combined efficacy analysis pre-specified
– Pre-specified Week 48 safety endpoints: serum creatinine, proteinuria, hip BMD, spine BMD
Primary Endpoint
48 144960Week

Primary Endpoint: HIV-1 RNA <50 copies/mL at Week 48Studies 104 and 111: Week 48 Combined Analysis
• E/C/F/TAF was non-inferior to E/C/F/TDF at Week 48 in each study– 93% E/C/F/TAF vs 92% E/C/F/TDF (Study 104)– 92% E/C/F/TAF vs 89% E/C/F/TDF (Study 111)
Favors E/C/F/TAF
0
4.7%‒0.7%2.0%
HIV
-1 R
NA
<50
c/m
L, %
Success Failure No Data0
20
40
60
80
100 92
4 4
90
4 6
E/C/F/TAF (n=866)E/C/F/TDF (n=867)
Treatment Difference (95% CI) Virologic Outcome
‒12% +12%
Favors E/C/F/TDF
19

TAF vs. TDF Summary
HIV
-1 R
NA
<50
%
Success Failure No Data0
20
40
60
80
100 92
4 4
90
4 6
• Virologic efficacy: E/C/F/TAF non-inferior to E/C/F/TDF1
• TAF associated with:− Smaller decrease in eGFR
(-6.4 vs. -11 mL/min)− Less proteinuria− Smaller decrease in bone
mineral density (BMD)− But greater increase in
cholesterol, LDL, HDL, TGs D TC: +29 mg/dL D LDL: + 14 mg/dL D TC:HDL: same
E/C/F/TAF
E/C/F/TDF
1Sax P et al, Lancet, 2015; 2Pozniak A et al, JAIDS, 2016
• EVG/c/FTC/TAF approved for patients with CrCL down to 302

Conclusions
Studies 104 and 111: Week 48 Combined Analysis
• 92% of patients treated with E/C/F/TAF achieved virologic suppression through Week 48 (combined analysis)– Virologic response for E/C/F/TAF, 93% (Study 104) and 92%
(Study 111)
– E/C/F/TAF was non-inferior to E/C/F/TDF
– High and similar response rates, irrespective of age, sex, race, HIV-1 RNA, and CD4 cell count
• Low rates of virologic failure, with resistance <1% in both arms
• Both drugs were well tolerated and safe
─ Discontinuations due to AEs were low in both arms
─ 0.9% (8) for E/C/F/TAF vs 1.5% (13) for E/C/F/TDF
─ No proximal tubulopathy cases
─ Common AEs similar between treatment arms 21

GS-US-292-0112 - single-arm, open-label Phase 3 study of HIV-1-infected participants with mild-moderate renal impairment (eGFRCG 30-69 mL/min) who switched to
E/C/F/TAF
• Phase 3, 96-week, multicenter, open-label study of virologically suppressed adults switching from TDF- or non-TDF–containing regimens to E/C/F/TAF
• Eligibility: stable eGFRCG (30–69 mL/min)
• Primary endpoint: change from baseline in eGFR at Week 24
– Actual GFR assessed with iohexol clearance in a participant subset
Primary Endpoint
E/C/F/TAF QD N=242
24 96480 12Week
A Pozinak J Acquir immun Def Syn 2016

Proteinuria: Change From Baseline to Week 48
23
85
100
20
40
60
80
100
120
140
160
180
200
78
10
110
14
Med
ian
(mg/
g)
105
160
188
166 2140
500
1000
1500
2000
2500
3000
3500
151 207197 221
Med
ian
(µg/
g)
228
801
1525 1563
3477
399
Tubular Proteins
b-2-m:CrUPCR UACR RBP:Cr
*All Total and TDF changes statistically significant; †all non-TDF changes not statistically significant.
2941
18
Total* TDF* Non-TDF†
Baseline
Week 48

BMD: Mean Change from Baseline to Week 48
24*p<0.05 by two-sided Wilcoxon signed-rank test.
Spine Hip
Me
an
(S
D)
% Δ
Sp
ine
BM
D
2.95*
2.29*
0.99
1.85*
1.47*
0.70
Me
an
(S
D)
% Δ
Hip
BM
D
Week 24n=226
Baselinen=236
Week 48n=214
Week 24n=225
Baselinen=236
Week 48n=216
TDF Non-TDFTotal

Conclusions
• Participants on TDF at time of switch had
– No change in actual GFR– Significant improvements in urinary markers of
renal function – Significant improvements in BMD – Significant increases in lipids
• Participants not on TDF at time of switch had
– No changes in actual GFR– Stable urinary markers of renal function and BMD– Significant decreases in cholesterol fractions
25

HIV/HBV co-infection data
• Limited• GS US 292–1249 - open-label, small sample,
noncomparative switch study evaluating the efficacy and safety of E/C/F/TAF in HIV suppressed, HBV co-infected participants– At 48 weeks, 91.7% of the 72 participants
maintained or achieved virologic suppression (HIV-1 RNA <50 copies/mL; HBV DNA <29 IU/mL)
Gallant J Acquir immun Def Syn 2016

GS US 292–1249
• Participants maintained high rates of HIV and HBV suppression, had improved renal function, and reduced biomarkers of bone turnover, consistent with other E/C/F/TAF studies
• E/C/F/TAF was well tolerated with no discontinuations because of renal events• Seroconversion occurred in 2.9% of HBsAg-positive participants and 3.3% of
HBeAg-positive participants• 40% of those with abnormal ALT normalized by week 48; which is lower than
the percentage seen in naive HBV-monoinfected populations and similar to treatment-experienced coinfected populations
• There were no ALT flares, and assessments of other liver-related parameters did not suggest increased hepatic risk.
E/C/F/TAF was effective against HIV and HBV, well tolerated, and demonstrated improvements in renal and bone safety consistent with the clinical profile of TAF.

Management of HIV co-infected patients
EASL 2017 CPG HBV, J Hepatol 2017
Recommendations:
1) All HIV-positive patients with HBV co-infection should start antiretroviral therapy (ART) irrespective of CD4 cell count. (Evidence level II-2, grade of recommendation 1)
2) HIV-HBV co-infected patients should be treated with a TDF- or TAF-based ART regimen. (Evidence level I for TDF, II-1 for TAF, grade of recommendation 1)

• When should you definitely use TAF over TDF?– Patient with osteoporosis or osteopenia– Patient with renal disease (eGFR >30) or evidence for proximal
tubular dysfunction (e.g. proteinuria)– Growing proportion of patients: ‘greying of the epidemic’
• When should you definitely not use TAF?– Patient on rifamycin (may decrease TAF levels)– Pregnant women– For pre-exposure prophylaxis (PrEP)??
TAF or TDF

Should TAF replace TDF?
• TAF is virologically as effective as TDF.
• Compared with TDF, TAF has more favorable effects on renal and bone markers.
− Particularly important in patients who already have renal or bone disease or who are at high risk of these complications.
• Cost of TAF- and TDF-regimens currently similar
Reasons to choose TAF
• Compared with TAF, more and longer-term data with TDF, particularly in studies in treatment naïve patients.
• More favorable lipid effects.• Renal and bone marker advantages
of TAF not yet known to translate into better clinical outcomes.
• TDF-regimens likely to be cheaper than TAF when TDF goes generic.
Reasons to choose TDF

Issues?
• Cost and access• NAFLD/Lipids• Cost/generic TDF• Long term data• Short term data - ?significant clinical
outcomes


KOSH FYI – current NHSE policy for TAF in HIV
• NHSE have approved funding of TAF for the following categories of patients:1. Patients with definite contra-indication or intolerance to tenofovir disoproxil fumarate (TDF) and abacavir.
– Confirmed osteoporosis on DEXA or a high risk of major fracture as determined by FRAX– Renal disease based on NICE definition CKD stage G3 or stage G1/2 plus stage A3 proteinurea – Previous renal toxicity or intolerance of TDF
– 2.Patients with relative contra-indication or intolerance to TDF and abacavir– Approaching threshold of osteoporosis – Renal markers approaching thresholds where TAF is thought to be more appropriate
VC referral??• Category 1 – Virtual clinic referral NOT required• Patients with a definite contra-indication or intolerance to tenofovir disoproxil and abacavir
– Confirmed osteoporosis on DEXA or a high risk of major fracture as determined by FRAX (FRAX score >10%)– Renal disease based on NICE definition CKD stage G3 (eGFR < 60ml/min) or stage G1/2 plus stage A3 proteinurea (eGFR >60ml/min plus severe proteinurea). Switch to TAF
should generally be based on more than an isolated reading for renal disease. – Previous renal toxicity or intolerance of TDF
• Patients starting or switching to TAF who fall in category 1 do not require referral and approval by the virtual clinic. • The reason for the choice of TAF as opposed to tenofovir disoproxil or abacavir must be clearly documented in the notes by the prescriber, for future audit
purposes.• • Category 2 – virtual clinic referral required• Patients with relative contra-indication or intolerance to TDF and where abacavir is not a suitable alternative
– Where there is an increased risk of bone disease and fracture probability: children and young people below age of peak bone mass (approx. 25 years), post-menopausal women, those on long-term glucocorticoid therapy or those who have already had a low-trauma fracture or who fall frequently.
– Renal disease based on NICE definition CKD G1 or 2 plus A2 proteinurea (eGFR> 60mls/min and moderate proteinurea) and one of the following additional risk factors: older age, diabetes, cardiovascular disease and hypertension. Other co-morbidities and concomitant nephrotoxic medication should be considered if associated with a higher risk of chronic renal disease progression.
• Patients who are starting or switching to TAF under category 2 must be referred to the virtual clinic for approval. Ideally this should be done prospectively. If TAF is required urgently then this must be discussed with agreed with a consultant physician and a retrospective referral made to the virtual clinic.
• The reason for the choice of TAF as opposed to tenofovir disoproxil or abacavir must be clearly documented in the notes by the prescriber, for future audit purposes.