Embed Size (px)
Citation preview

The role of the laboratory in the diagnosis of
autoimmune liver disease
Dr Adrian Heaps PhD FRCPath Consultant Clinical Scientist

Overview
1. Primary Biliary Cholangitis (PBC) 2. Primary Sclerosing Cholangitis (PSC) 3. IgG4-related liver disease (IgG4-RD) 4. Autoimmune Hepatitis (AIH)

• Previously known as primary biliary cirrhosis • Chronic, progressive cholestatic liver disease. • Variable natural history and outcomes. • Autoimmune pathogenesis. • Biliary Epithelial Cells (BECs) lining the small and
medium intra-hepatic bile ducts are targeted by an immune mechanism.
• Progressive BEC destruction leads to cholestasis, fibrosis and eventually cirrhosis if untreated.
1) Primary Biliary Cholangitis (PBC)
∗Most commonly affects women in their 5th and 6th decade (8:1 M:F).
∗Extremely rare under 16 years. ∗Prevalence varies significantly
geographically from 40 – 400 / million. ∗Previously thought to be more common in
Northern Europe and USA but recent data indicates similar prevalence in Asia.
PBC: Epidemiology
• The aetiology of PBC is unknown. • ?Environmental factors / infection triggering a breakdown of
immune tolerance in a genetically susceptible individual. • Theory: unknown toxin / factor / pathogen modifies Pyruvate
dehydrogenase complex E2 (PDC-E2)> ?hapten effect. • Organ-specific autoimmune disease. • CD4+, CD8+ T cells, B cells and antibodies all involved, however
T-cells predominate inflammatory destruction of intrahepatic bile ducts.
PBC: Pathogenesis
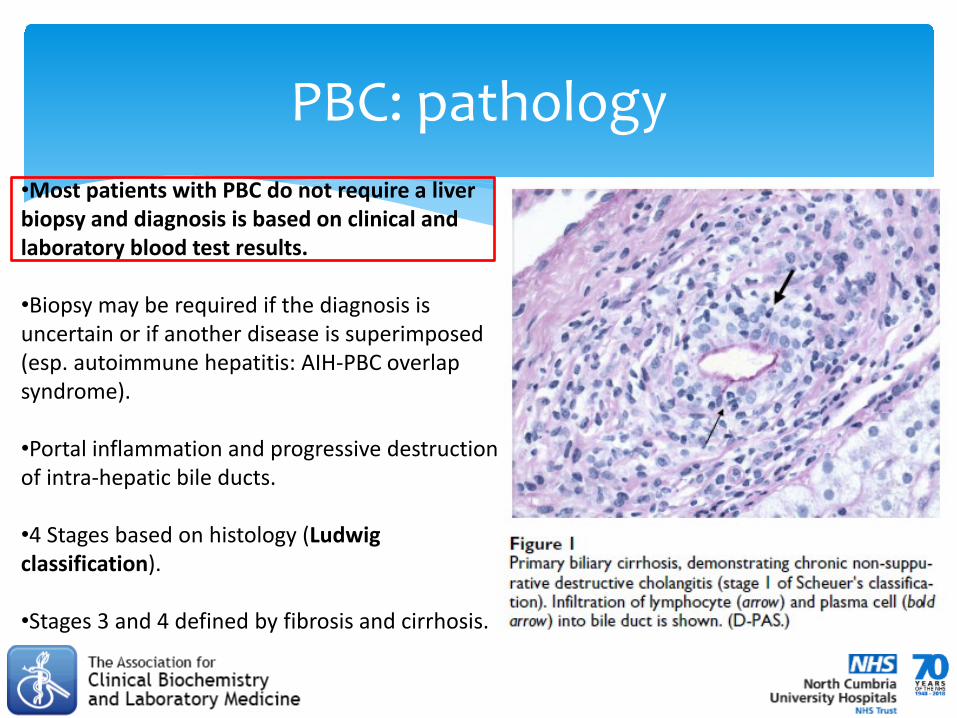
PBC: pathology •Most patients with PBC do not require a liver biopsy and diagnosis is based on clinical and laboratory blood test results.
•Biopsy may be required if the diagnosis is uncertain or if another disease is superimposed (esp. autoimmune hepatitis: AIH-PBC overlap syndrome).
•Portal inflammation and progressive destruction of intra-hepatic bile ducts.
•4 Stages based on histology (Ludwig classification).
•Stages 3 and 4 defined by fibrosis and cirrhosis.

∗ Without identification and treatment, a substantial number of PBC patients will progress to liver failure, transplant or death in 10 years.
∗ PBC can be severe and rapidly progressive in some patients.
∗ Early diagnosis and treatment is therefore essential.
PBC Diagnosis I
∗ History ∗ Physical Examination ∗ Abdominal ultrasound ∗ Serological tests ∗ Extended imaging: MRCP = magnetic
resonance cholangiopancreatography ∗ Liver biopsy ∗ Genetic testing
PBC Diagnosis II

• 60% diagnosed whilst clinically asymptomatic. • Signs at presentation can include:
– Fatigue – Pruritis (20-70%, palms and soles, worse at night) – Hepatomegaly – Splenomegaly – Hyperlipidemia (sometimes with xanthoma and xanthelasma) – Sicca syndrome (dry eyes and mouth +/- extra-glandular features>
consider Sjogren’s syndrome overlap) – Jaundice – Abdominal pains
PBC: Clinical Signs I

∗ Clinical signs of advanced disease, mostly related to long-lasting cholestasis and cirrhosis: ∗ Malabsorption ∗ Steatorrhoea (fatty, pale, loose stools) ∗ Osteopenia/osteoperosis (metabolic bone disease) ∗ Portal hypertension ∗ Hepatocellular carcinoma
∗ Association with extra-hepatic autoimmune diseases: systemic
sclerosis (scleroderma) / CREST syndrome.
PBC: Clinical Signs II

So PBC associates with almost all autoimmune diseases……but particular vigilance should be given to detect signs of systemic sclerosis including: • Raynaud’s syndrome • Dysphagia • Acid reflux • Sclerodactyly • Telangiectasia

∗ Basic blood biochemistry tests: ∗ Elevated Alkaline phosphatase (ALP) liver enzyme**. ∗ Raised gamma-glutamyl transferase (γGT), aspartate transaminase
(AST) and alanine aminotransferase (ALT) liver enzymes may also be present.
∗ High ALP:ALT ratio> cholestatic/biliary picture. ∗ Elevated cholesterol and bilirubin (seen in advanced disease).
∗ A polyclonal elevated serum Immunoglobulin M (IgM) concentration may also be present: not PBC-specific.
**Serum ALP enzyme can have different sources including bone. In practice, the hepatic origin of ALP can be confirmed by simultaneous elevation of γGT and/or conjugated bilirubin.
PBC: Serum protein studies

∗ The detection of antigen-specific autoantibodies in the patient’s serum is a key component of PBC diagnosis.
∗ Antibodies in the serum can be detected by multiple clinical laboratory methods, the most common of which is indirect immunofluorescence (IIF).
∗ The substrates used for the investigation of autoimmune liver disease are typically rodent tissue (liver, kidney, stomach) and the HEp2 cell line (anti-nuclear antibodies = ANA).
∗ Diluted patient serum is incubated on the tissue substrate, washed, then incubated with a fluorochrome-conjugated reported antibody (anti-human IgG) before a further wash to remove any non-specific background.
Autoimmune serology methods I

∗ Liver tissue IIF slide can be manually visualised using a UV microscope.
∗ All aspects of the IIF process, from serum sample aliquoting, incubation, slide washing and (some) image analysis can now be fully automated.
∗ Despite automation the interpretation of indirect immunofluorescence patterns requires significant expert input from an experienced reader.
∗ Other commonly used antigen specific methods to detect liver autoantibodies include: ∗ Enzyme-linked immunosorbent assays (ELISA) ∗ Addressable laser bead immunoassay (ALBIA) ∗ Western blotting ∗ Multi-parameter line blots
Autoimmune serology methods II

Autoimmune serology methods III

Autoimmune serology methods IV

∗ A positive anti-mitochondrial antibody (AMA) >1/40 titre is the hallmark antibody of PBC.
∗ Specifically anti-M2 (pyruvate dehydrogenase complex E2) antibodies.
∗ Clinical sensitivity 90-95%. Clinical specificity close to 100%. ∗ Positive AMA with elevated ALP (and no elevation of AST)
has a 95% PPV of histological PBC. ∗ Typically no value in performing an AMA titre as titres do not
correlate with disease activity or severity.
PBC: Autoantibodies

Anti-mitochondrial antibodies detected by IIF on rodent tissue (LKS) and HEp2 cell line (ANA)
Parietal cells positive on rodent stomach (LKS)
Granular staining in rodent liver hepatocytes (LKS)
Granular staining in rodent kidney with stronger staining in distal tubules (LKS)
Typical “string-like” cytoplasmic staining on HEp2 cell line (ANA)
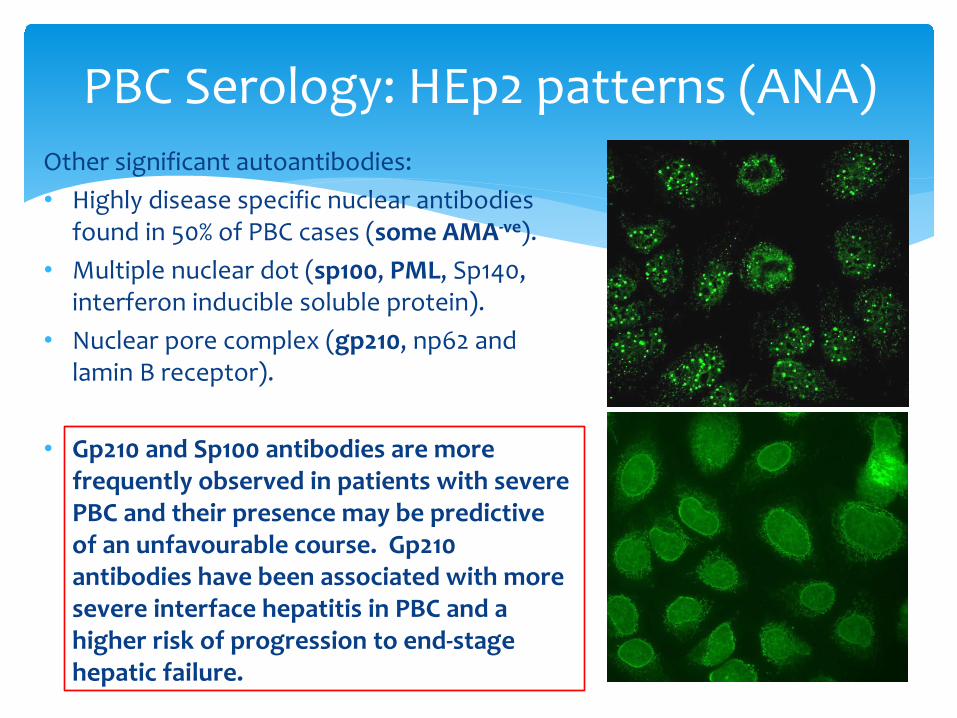
Other significant autoantibodies: • Highly disease specific nuclear antibodies
found in 50% of PBC cases (some AMA-ve). • Multiple nuclear dot (sp100, PML, Sp140,
interferon inducible soluble protein). • Nuclear pore complex (gp210, np62 and
lamin B receptor).
• Gp210 and Sp100 antibodies are more frequently observed in patients with severe PBC and their presence may be predictive of an unfavourable course. Gp210 antibodies have been associated with more severe interface hepatitis in PBC and a higher risk of progression to end-stage hepatic failure.
PBC Serology: HEp2 patterns (ANA)

Anti-M2, M2-3E(BPO)*, Sp100, PML and Gp210 PBC-specific autoantibodies can also be detected using multi-parameter line blots: ∗ Membrane strips coated with thin parallel lines of purified
antigens are used as solid phase. ∗ If the sample is positive, specific antibodies in the diluted serum
sample attach to the antigens coupled to the solid phase. ∗ In the second incubation step, the attached antibodies react
with alkaline-phosphatase-enzyme-labelled anti-human reporter antibodies.
∗ In the third step, the bound antibodies are stained with a chromogen/substrate solution which is capable of promoting a colour reaction.
∗ An intense dark band at the line of the corresponding antigen appears if the serum sample contains specific antibodies.
∗ Membrane strips are scanned to generate a semi-quantitative output that corresponds to the antibody concentration in the serum.
*Recombinant antigen (MIT3) co-expressing immunodominant epitopes of BCOADC-E2, PDC-E2 and OGDC-E2 = 3E(BPO). Higher clinical sensitivity for PBC but lower specificity compared to M2 alone (PDC-E2).
PBC: multiplex antibody detection

• Anti-centromere antibodies (ACA) have been found in up to 30% of PBC patients and 80% of patients with a PBC/SSc overlap syndrome.
• PBC patients with ACA should be carefully screened for features of SSc.
• Recent studies have shown that ACA+ PBC patients (without SSc) have more severe bile duct injury and more frequent portal hypertension.
PBC: Anti-centromere antibodies

• The diagnosis of PBC is based on a combination of clinical features:
1. An abnormal liver biochemical pattern: a cholestatic picture (^ALP/GGT) with or without a hepatitis picture (^ALT/AST) persisting for more than six months.
2. The presence of detectable AMA (>1:40) in serum. 3. The diagnosis may be confirmed by finding characteristic
histological features of PBC. • A "probable" diagnosis requires the presence of two of these three criteria, and a
"definite" diagnosis requires all three.
• AMA is negative in approximately 5-10% of patients who otherwise have all the features typical of PBC. AMA negative PBC is clinically identical to the positive variant.
PBC: Diagnostic Criteria I
∗ PBC Scenario 1: Chronic elevation of alkaline phosphatase (ALP) with a positive AMA (immunofluorescent assay titre of >1:40) in the absence of other liver diseases and systemic diseases.
∗ PBC Scenario 2: Chronic elevation of ALP with negative AMA and antinuclear antibodies (ANA) tests but a liver biopsy that shows destructive cholangitis and destruction of interlobular bile ducts.
∗ PBC Scenario 3: Chronic elevation of ALP with negative AMA but positive PBC-specific ANA (sp-100, gp-210) tests.
Younossi et al 2018
PBC: New Diagnostic Criteria 2018

• An “incidental” finding of anti-mitochondrial antibodies occurs without abnormal liver biochemistry or clinical signs features of PBC. It was previously thought to be predictive of future PBC development: based on limited findings from a single, small UK cohort of patients in the 1980s.
• A large scale characterisation study of incidental AMA recently performed in France (Dahlqvist et al 2017) found only 1 in 6 patients (16%) with positive AMA and normal ALP develop PBC after 5 years.
Positive AMA >1/40 is only sufficient to diagnose PBC when combined with abnormal serum liver biochemistry.
• It is recommended that individuals with incidental findings of AMA (as
defined above) are monitored periodically with repeat liver enzymes every 6-12 months to ensure they do not manifest clinical or biochemical signs of PBC. Recent data suggests the majority (~85%) will remain PBC free up to 5 years.
PBC: “Incidental” AMA

∗ .....and just to make things more complicated:
∗ It has been reported that 8-10% of patients have "overlapping“ features of PBC and Autoimmune Hepatitis (AIH).
∗ Liver biopsy is mandatory for the diagnosis of AIH-
PBC overlap syndrome. Consider in PBC patients with disproportionate elevation in ALT +/- IgG.
PBC-AIH: Overlap syndromes

• Cholestatic liver disease of unknown origin: progressive, multi-focal strictures of the extra and/or intra-hepatic bile ducts.
• Strongly associated with a specific phenotype of inflammatory bowel disease (IBD): pancolitis.
• Inflammation and subsequent obstruction of the bile ducts both inside (intrahepatic) and outside (extrahepatic) the liver.
• Fibrosis of the hepatic biliary ducts obstructs the flow of bile acids to the duodenum: choleostasis.
• Progressive disease leading to biliary cirrhosis, hepatic failure and in 6-30% of cases cholangiocarcinoma.
2) Primary Sclerosing Cholangitis (PSC)

• PSC more common in men (60:40 M:F). Unusual for an “autoimmune” disease.
• Average age at diagnosis is 40 years.
• 75% of PSC patients also have IBD (87% UC, 13% Crohns). • 5% of IBD patients have PSC.
• More common in Caucasian populations.
PSC: Epidemiology

• Largely unknown: Associates with other autoimmune diseases, HLA associations (DRB1*0301-DQB1*0201) and autoantibodies.
• But: male preponderance and a lack of response to immunosuppressive agents challenge the autoimmune hypothesis.
• Theory: inappropriate immune response to biliary tree gut microflora. ?bystander tissue damage.
• Theory: Aberrant expression of adhesion molecule and CCRs results in the infiltration of ?autoreactive T and B lymphocytes.
PSC: Pathogenesis

• Asymptomatic in the earl stages of disease. • Advanced disease:
– Fatigue – Intense pruritis – Fever – Weight loss – Abdo pain – Hepatosplenomegaly – Symptoms of malabsorption: e.g. vitamin deficiency and steatorrhea. – Hyperpigmentation
• IBD: has a unique phenotype in PSC, often asymptomatic. PSC + IBD
increases colon cancer risk. • Cholangiocarcinoma: 1% annual incidence in PSC patients. Epithelial cell
adenocarcinoma of the biliary tree (see also pancreatic and gall bladder cancer).
PSC: Clinical

• Segmental strictures (black arrows) with proximal dilation (white arrows) of bile ducts on cholangiogram.
• Classic “onion skin” fibrosis seen on liver biopsy histology (red arrow). • Patients who present with clinical, biochemical and histological features
compatible with PSC, but have a normal cholangiogram, are classified as small duct PSC.
PSC: Pathology & Imaging

• Cholestatic pattern: – Elevated serum Alkaline Phosphatase (ALP). – Mildly elevated serum Aminotransferases.
• Serum albumin and bilirubin abnormalities (advanced disease)
• ?Monitor Carcinoembryonic antigen (CEA) and Carbohydrate Antigen 19-9 (CA19-9) for cholangiocarcinoma and colon cancer.
PSC: Biochemistry

∗ Multiple autoantibodies detected in the serum of PSC patients.
∗ None are sufficiently sensitive or specific to have clinical utility.
∗ Atypical perinuclear anti-neutrophil cytoplasmic antibodies (p-ANCA) are sensitive 68% (26-94%) in some studies but generally have very low specificity (also found in AIH and UC).
∗ The antigenic target of the PSC-associated antibody that generates the atypical P-ANCA pattern has not been confirmed although β-tubulin isotype 5 is a strong candidate (Terjung et al. 2010).
∗ Atypical p-ANCA serum titre does correlate with disease activity, the extent of the disease, or with immunosuppressive therapy.
∗ Anti-myeloperoxidase (MPO) and proteinase-3 (PR3) are negative in >95% of PSC.
PSC: Serology I
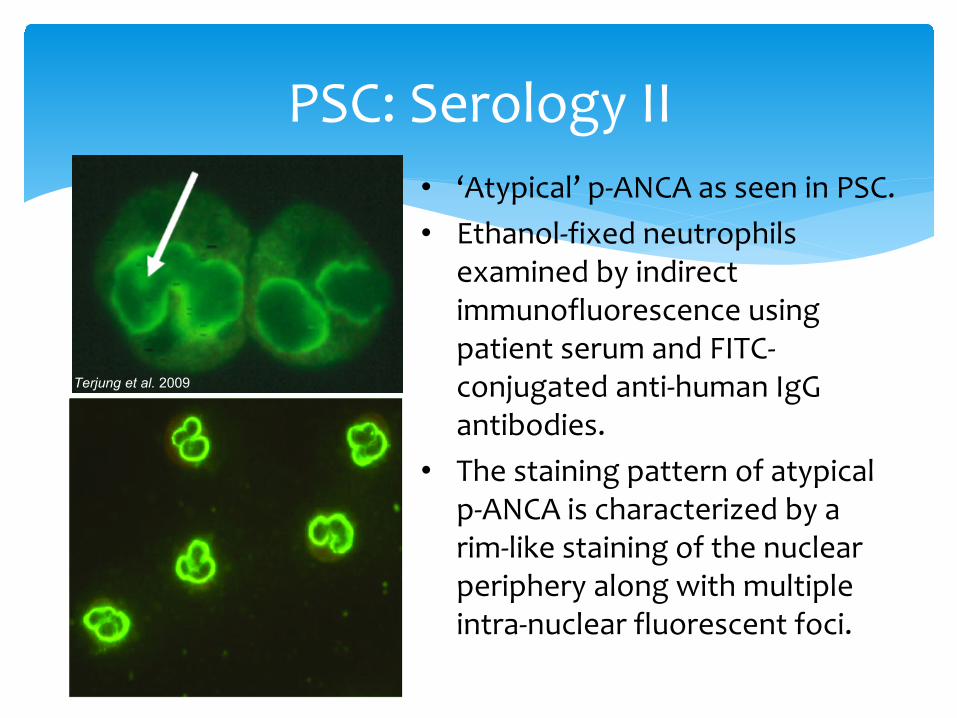
PSC: Serology II • ‘Atypical’ p-ANCA as seen in PSC. • Ethanol-fixed neutrophils
examined by indirect immunofluorescence using patient serum and FITC-conjugated anti-human IgG antibodies.
• The staining pattern of atypical p-ANCA is characterized by a rim-like staining of the nuclear periphery along with multiple intra-nuclear fluorescent foci.
Terjung et al. 2009
∗ ANCA testing NOT recommended as initial screening for autoimmune liver diseases including PSC.
∗ AMA, LKM and SLA may be of use to rule out PSC. They have close to zero prevalence in the disease.
∗ Hypergammaglobulinemia (^IgG) may be present (30%).
∗ Elevated serum IgM (up to 45%).
PSC: Serology III

∗ Routine autoantibody screening is not required to establish a diagnosis of PSC.
∗Analysis of ANA and ASMA may be relevant in a subgroup of patients to support a suspicion of “autoimmune” features that may have therapeutic implications (PSC–AIH overlap syndrome).
http://www.easl.eu/research/our-contributions/clinical-practice-guidelines/detail/management-of-cholestatic-liver-diseases/report/5
PSC: EASL recommendations

∗ PSC–AIH overlap syndrome is an ill-defined immune-mediated disorder characterized by: ∗ histological features of AIH ∗ cholangiographic findings typical of PSC
∗ Predominantly found in children, adolescents and young adults.
∗ Immunosuppression recommended in PSC-AIH due to the autoimmune component.
PSC-AIH overlap syndrome
∗ Recently described biliary disease of unknown aeitiology. ∗ Biochemical & cholangiographic features indistinguishable
from PSC. ∗ Characterised by massive infiltration of IgG4+ plasma cells
and eosinophils on biopsy> histopathological diagnosis. ∗ Other organ manifestations of IgG4-RD – e.g. sialadenitis,
retroperitoneal fibrosis, GI involvement. ∗ Elevated serum IgG4 concentration. ∗ Strongly associated with autoimmune pancreatitis NOT
IBD. ∗ Typically responds to immunosuppression (unlike PSC).
IgG4-related sclerosing cholangitis (IgG4-SC)

∗ (A, B) Lymphoplasmacytic and eosinophilic infiltration in the portal tracts.
∗ The inflammatory cell infiltrates are centred predominantly around the portal veins (arrows), while the hepatic artery (white arrowhead) and bile duct epithelia (black arrowhead) are relatively intact without degenerative changes.
∗ The portal tracts are mildly fibrotic, without an ‘onion-skin’ appearance.
∗ Immunohistochemical stain for IgG4 reveals several scattered IgG4-positive plasma cells in the portal tracts (C: IgG4 immunostaining)
∗ (Ryu et al. 2011)
IgG4-SC: liver histology

∗ Serum IgG4 concentration above a cut-off of 135 mg/dL seen in ~85% of IgG4-SC cases.
∗ But.......IgG4 can also be elevated in PSC. ∗ Although elevated serum IgG4 concentration is considered a characteristic
feature of IgG4-SC it cannot reliably differentiate PSC and IgG4-SC. ∗ Examine your CZE serum protein electropherograms carefully when interpreting
polyclonal elevated gamma regions as there may be clues to an elevated IgG4:
IgG4-SC: serology
^IgG4 ^IgG1

3) Autoimmune Hepatitis (AIH)
• Autoimmune Hepatitis – Update 2015 • European Association for the Study of
the Liver (EASL) Clinical Practice Guideline (2015)
∗Non-resolving, chronic inflammation of the liver of unknown cause.
∗?environmental triggers, failure of immune tolerance and genetic predisposition.
∗T-cells specific for liver antigens. ∗ Inflammation and fibrosis.
Autoimmune Hepatitis (AIH)
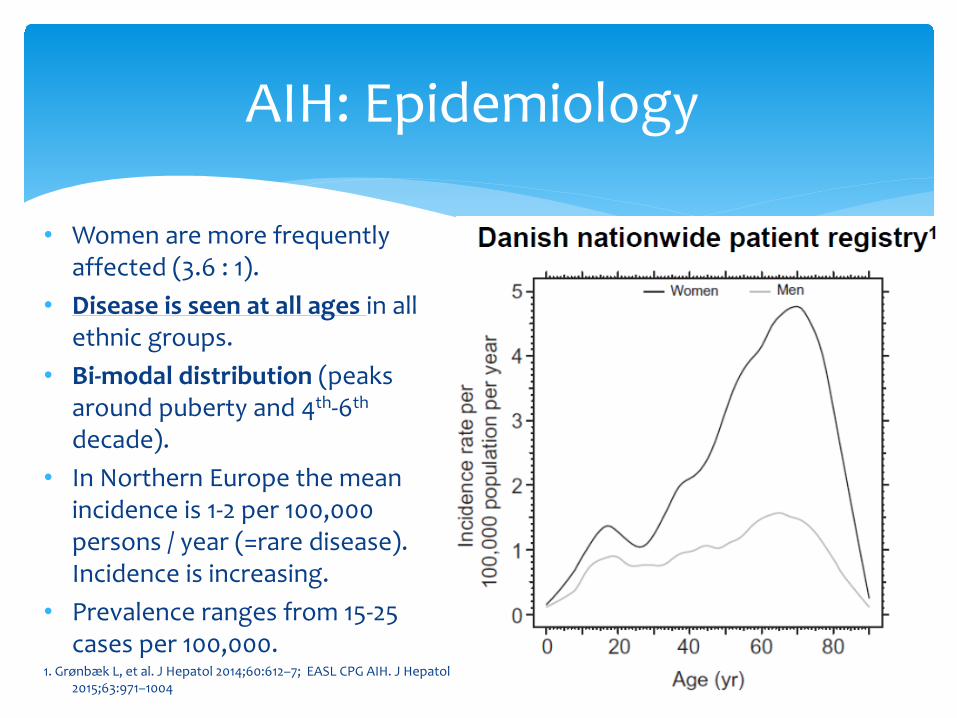
• Women are more frequently affected (3.6 : 1).
• Disease is seen at all ages in all ethnic groups.
• Bi-modal distribution (peaks around puberty and 4th-6th decade).
• In Northern Europe the mean incidence is 1-2 per 100,000 persons / year (=rare disease). Incidence is increasing.
• Prevalence ranges from 15-25 cases per 100,000.
1. Grønbæk L, et al. J Hepatol 2014;60:612–7; EASL CPG AIH. J Hepatol 2015;63:971–1004
AIH: Epidemiology

∗ Insidious onset with non-specific symptoms most common: ∗ Fatigue, lethargy, malaise, nausea, weightloss ∗ (Jaundice) ∗ Abdominal / RUQ pain ∗ Polyarthralgia (without arthritis)
∗ Wide clinical spectrum from asymptomatic to severe acute (25%) or even fulminant disease.
∗ AIH in men more likely to be asymptomatic (initially). • 40% of patients with untreated severe disease die within 6 months of diagnosis. • Oesophageal varices and haemorrhage. • Hepatic encephalopathy (confusion, altered level of consciousness, and coma as a
result of liver failure). • Cirrhosis already present in ~1/3 of patients at diagnosis
• Irrespective of the presence of symptoms • Due to delay in diagnosis (often long asymptomatic course)
AIH: Presentation

∗ Overlap syndromes exits: AIH-PBC and AIH-PSC. ∗ Pregnancy-associated AIH: can occur in pregnant women or after delivery. ∗ AIH-like disease can arise post liver transplantation . ∗ Onset of disease after viral infections has been described (inc. HBV, HCV).
∗ Development after administration of drugs, supplements or herbals (“drug-
induced” AIH – difficult to differentiate from DILI): ∗ Nitrofurantoin and minocycline ∗ Biological agents (anti-TNF-α) ∗ Interferon-α for HCV
∗ Concurrent autoimmune or immune-mediated diseases in the patient are common.
∗ An unusual form of AIH occurs in 10–20% of patients with APECED.
AIH: specific characteristics

∗ Diagnosis of AIH requires presence of characteristic clinical and laboratory features: • Compatible history • Autoantibodies • Hypergammaglobulinaemia (a selectively polyclonal elevated IgG in
the absence of IgA and IgM elevation is particularly suggestive of AIH).
∗ Exclusion* of other causes of chronic hepatitis (e.g. drugs and alcohol).
∗ Exclusion* of infectious cause (HBV, HCV). ∗ Exclude* PBC, PSC, hereditary disease (A1AT def / Wilson’s
/Haemochromatosis (HFE)).
AIH: Diagnosis
*co-morbidity is possible!
• Aminotransferases (ALT/AST) and Alkaline phosphatase (AP): • Low AP:(AST/ALT) ratio in AIH > HEPATIC PATTERN • Include gamma-GT in children to determine bone/biliary origin of AP>
distinguish liver/biliary inflammation from bone metabolism (e.g. growth spurt).
• Neither AP/GGT will discriminate the presence or absence of
cholangiopathy in children with AIH (overlap syndromes).
• Albumin: reduced
• Gamma-globulins (IgG): polyclonal elevated
AIH: Laboratory assessment

∗ Histological demonstration of hepatitis is a prerequisite for the diagnosis of AIH and needs to be part of the initial diagnostic work-up (EASL 2015).
∗ Interface hepatitis with lymphoplasmacytic infiltrate > NOT specific for AIH.
∗ Fibrosis and cirrhosis. ∗ Rarely see granulomas. ∗ Bile ducts usually spared.
∗ Features of AIH, PBC and PSC can
all be present!
AIH: Liver Histology

Score ≥7 = Definite AIH Score ≥6 = Probable AIH
International AIH Group (IAIHG): simplified scoring system
Hennes EM, et al. Hepatology 2008;48:169–76
∗ Suitable for rapid diagnosis in a clinical setting

∗ Prominent role in AIH Diagnosis (like PBC, unlike PSC) ∗ Conventional serological repertoire (first line):
• ANA: targets not defined in AIH. Type 1 AIH. • Smooth Muscle Antibodies (SMA): e.g. F-Actin Type 1 AIH. • Liver Kidney Microsome 1 (LKM1): P450 2D6 Type 2 AIH. Highly Specific for
AIH. • Liver Cytosol 1 (LC1): formimino-transferase cyclodeaminase Type 2 AIH.
∗ First line testing can be achieved with ANA (HEp2)/LKS IIF + ELISA or
immunoblot for SLA/LP antibodies: ∗ 90% AIH will be ANA+ and/or SMA+ (+/- SLA/LP) ∗ Remaining 10% will be LKM1+ and/or LC1+ (+/- SLA/LP)
AIH: First line antibody screen

∗ Second line testing if first line antibody tests are negative and clinical suspicion remains:
∗ ANCA immunofluorescence (for atypical p-ANCA) ∗ Specific immunoassays for the following antibodies:
∗ LKM1 ∗ LKM3* ∗ LC1 ∗ SLA/LP ∗ F-actin* ∗ Ro52 ∗ Gp210** ∗ Sp100**
AIH: Second line antibody screen
*Note that clinical assays for LKM3 and f-actin antibodies are not routinely available in the UK. **Gp210 and Sp100 antibodies are used to exclude classical AIH> highly specific for PBC.
∗ Autoantibodies not specific for AIH> almost all can be present in chronic Hep C (B + D).
∗ Low titres do not exclude AIH. ∗ High titres do not establish a diagnosis of AIH in
isolation. ∗ In adults antibody titres of limited use. ∗ In children (≤18 years old) titres are useful
biomarkers of both disease activity and treatment response (particularly LC1 antibodies).
AIH: antibodies continued...

∗ In adults a liver autoantibody titre by IIF of >1:40 is clinically relevant.
∗ In children: • 1:20 for ANA and SMA • 1:10 for LKM (antibody reactivity infrequent in healthy
children)
∗ High titre LKM1 strongly supports diagnosis of AIH.
AIH: antibody titres

Other autoantibodies> in patients who lack the conventional serological findings:
∗ Soluble liver antigen (SLA SepSecS*): highly specific for AIH. AKA Liver-pancreas antigen (LP-1). ∗ Very rarely found as an isolated antibody in AIH > more commonly found in association
with conventional autoantibodies. ∗ Only autoantibody considered specific (diagnostic) for AIH. ∗ But > may indicate a more severe disease and worse outcome. ∗ SLA almost always (>95%) found in conjunction with Ro52 antibodies.
∗ pANCA (atypical): nuclear lamina proteins (nuclear membrane = pANNA) ?tubulin-β chain isotype 5. ∗ “ANCA should be tested by indirect immunofluorescence (IIF) in cases of suspected AIH where
ANA, ASMA, LKM1, LC1 and SLA/LP antibodies are negative”. EASL 2015. ∗ P-ANCA can be the ONLY antibody present in AIH.
AIH: non-conventional antibodies
*O-phosphoseryl-tRNA:selenocysteine-tRNA synthase

EASL 2015: proposed diagnostic algorithm for AIH

∗ Sub-classification based on autoantibody profile alone ∗ Validity and clinical implication are uncertain
AIH: sub-classification controversy
*Possibly more severe. EASL CPG AIH. J Hepatol 2015;63:971–1004
∗ Autoimmune serology using indirect immunofluorescence with rodent LKS and HEp2 cell line (ANA) substrate is the main, routine test for the diagnostic work-up of AIH
∗ Considered by the liver community to be the Achilles’ heel in the diagnostic work-up. Why? ∗ Time consuming ∗ Requires highly skilled interpretation ∗ Insufficiently standardised
Indirect immunofluorescence

AIH immunofluorescence Patterns: I
LKM1: staining in rodent kidney: only proximal tubules exhibit strong signal. AIH specific. Uncommon.
AMA: staining of both distal and proximal tubules in the kidney with stronger signal in the distal tubules. Granular staining pattern. PBC specific. Common.

AMA: granular staining also present in the GPC of rodent stomach. Absent in LKM1. Other staining features in kidney and liver help to distinguish a positive AMA from a LKM1 + GPC stain. A favourite of NEQAS> always check for variegated staining of tubules in the kidney and granularity of liver stain.
AIH immunofluorescence Patterns: II
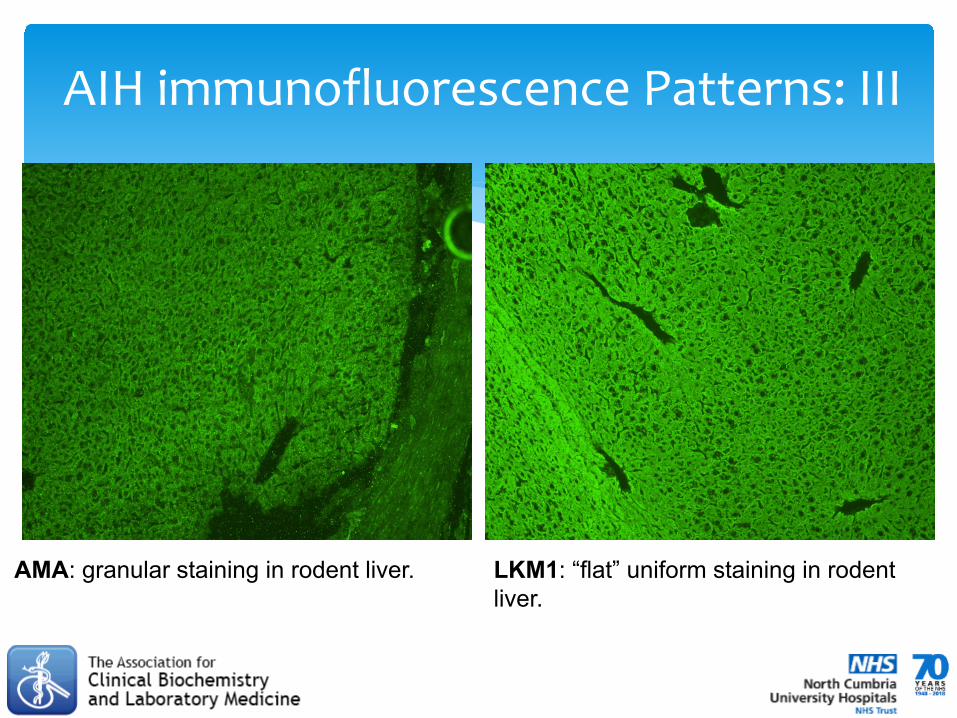
AMA: granular staining in rodent liver. LKM1: “flat” uniform staining in rodent liver.
AIH immunofluorescence Patterns: III

LC1: on rodent liver shows cytoplasmic staining of hepatocytes with a weakening of the stain around central vein.
AIH immunofluorescence Patterns: IV
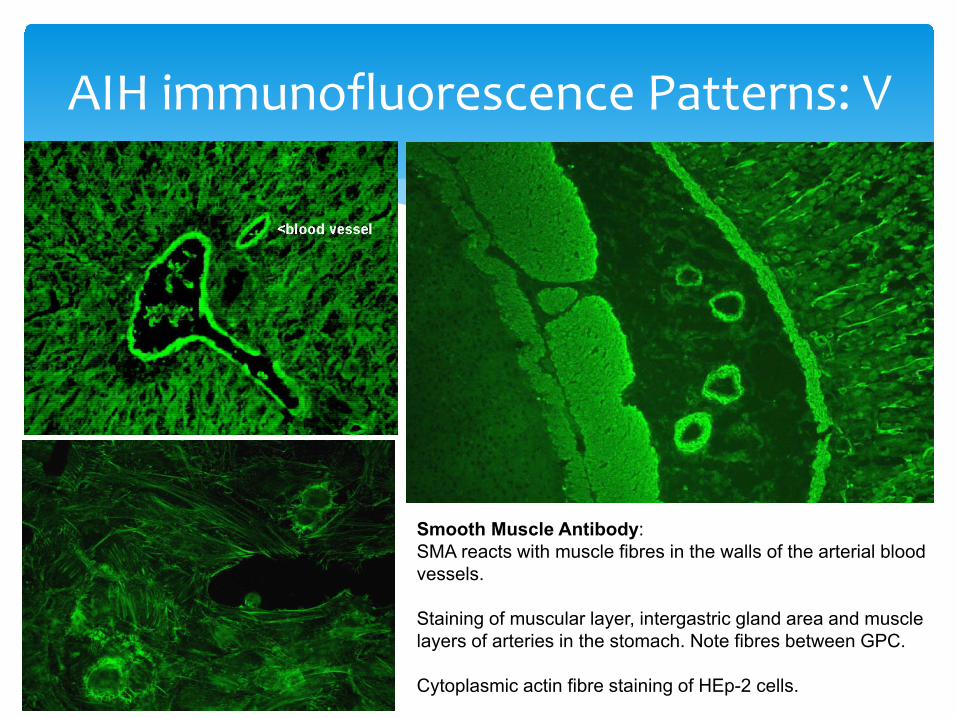
Smooth Muscle Antibody: SMA reacts with muscle fibres in the walls of the arterial blood vessels. Staining of muscular layer, intergastric gland area and muscle layers of arteries in the stomach. Note fibres between GPC. Cytoplasmic actin fibre staining of HEp-2 cells.
AIH immunofluorescence Patterns: V

AIH immunofluorescence Patterns: VI
∗ Smooth muscle antibodies can be sub-classified based on the indirect immunofluorescence pattern on rodent LKS substrate (Bottazzo et al. 1976).
∗ In addition to positive staining in the muscular layer and inter-gastric gland area: ∗ Blood vessel walls also positive = SMA-V (vessels) ∗ Vessel walls and glomeruli = SMA-G (glomerular) ∗ Vessel walls, glomeruli and tubules = SMA-T
(tubular)
∗ No SMA pattern was specific for AIH-I, however SMA-V (most common pattern) primarily associated with miscellaneous, non-liver related disease including viral infections.
∗ SMA-G more specific for liver disease with high-titre SMA-T with actin (HEp2) the most specific pattern for AIH.
∗ Based on work from 1976, no longer widely reported. Useful for excluding non-specific, incidental SMA-V.
SMA-G
SMA-T

Clinical cases: 01 Patient AP
∗ Patient AP, 52 year old woman, presented to GP with intense pruritus, worse at night.
∗ No associated skin rash or obvious precipitant. ∗ Initial investigations showed elevated alkaline
phosphatase (ALP) of 236 (nr 30-130). ALT and bilirubin were normal.
∗ What further immunology tests? ∗ Indirect immunofluorescence on rodent liver kidney
stomach showed a strong anti-mitochondrial pattern at 1:80. Also seen in HEp2 cytoplasm. Confirmed as M2 antibodies by immunoblotting.
∗ Polyclonal elevated IgM also present at 6.14 g/L (NR 0.43 – 1.90).
∗ Conclusion: classic presentation of primary biliary cholangitis (PBC).
∗ Patient was started on a trial of UDCA.
Clinical cases: 02 Patient BL
∗ Patient BL, 60 year old man, presented to GP with 2 month history of joint pains. ∗ An “autoantibody screen” was performed> anti-mitochondrial antibodies detected at 1:80 on
rodent LKS, later determined as AMA-M2 by immunoassay. ∗ LFTs are within the reference range. No clinical signs of liver disease. Normal immunoglobulins. ∗ How should you report this result?
∗ Remember: Positive AMA >1/40 is only sufficient to diagnose PBC when combined with
abnormal serum liver biochemistry. This is an incidental finding of AMA. It is NOT predictive for the development of PBC in the majority of individuals: ~1 in 6 individuals with an incidental AMA will go onto develop PBC over 5 years (see Dahlqvist et al 2017)
∗ “?significance of positive anti-mitochondrial antibodies (AMA-M2 subtype) in the context of normal liver biochemistry and no clinical features of liver disease. AMA-M2 antibodies can appear before the development of deranged liver function and clinical signs of primary biliary cholangitis (PBC) in a minority of individuals. Suggest check liver function annually to monitor.”
∗ Why was the test requested in the first place? AMA-M2 and other PBC-associated antibodies are highly specific when requested in the appropriate context. They are not suitable for population screening.

Clinical cases: 03-I Patient KB
∗ Patient KB, 28 year old woman, presented to GP TATT, dyspepsia, headache, recurrent abdo pain, constipation and pyrexia.
∗ Initial investigations showed elevated ALT of 127 (nr <40). ALP and bilirubin within reference range.
∗ What further tests? ∗ Viral serology negative (HAV, HBV, HCV). ∗ A1AT and ceruloplasmin within reference range. ∗ HFE point mutations not detected> no family Hx of haemochromatosis. ∗ H.pylori faecal antigen negative. Giardia not detected. ∗ What further immunology tests to investigate an unexplained transaminitis? ∗ Coeliac serology (IgA-tTG antibody) negative. Duodenal biopsy also performed which
was negative for features of coeliac disease> what are these histological features? ∗ Mild polyclonal elevated IgG also present at 16.20 g/L (NR 5.80 – 15.40).

Clinical cases: 03-II Patient KB
∗ Indirect immunofluorescence on rodent LKS shows a non-granular fluorescence in the proximal tubules of the kidney and liver.
∗ HEp2 cells showed a high titre ANA >1:640 with no specific antibody detected.
∗ What is the likely diagnosis?
∗ Autoimmune Hepatitis (type II): IFA patterns on LKS substrate is Liver Kidney Microsome (LKM)> confirmed as LKM1 antibodies by immunoblotting.
∗ Patient is currently awaiting a liver biopsy to confirm a diagnosis of AIH.

Clinical cases: 04 Patient EB
∗ Patient EB, 77 year old woman, investigated by her GP for ?palindromic rheumatism (??).
∗ Found to have deranged LFTs: ALP = 308 (NR 30-130) with normal ALT and bilirubin.
∗ Viral serology (HAV, HBV, HCV) negative. ∗ Autoantibody screen (rodent LKS) was negative. ∗ HEp2 ANA reported as showing “dots in nucleoplasm” ∗ Polyclonal elevated IgM 4.48 g/L (NR 0.71-2.30) ∗ ?Significance of these results: What further tests? ∗ Immunoblotting (antibody immunoassay) showed high
titre anti-Sp100 and anti-PML antibodies consistent with the multiple nuclear dot ANA pattern.
∗ ANAs including Sp100 and Gp210 (nuclear pore/membrane) are highly specific for PBC and can occur in the absence of AMA.
∗ Diagnosis: AMA-negative PBC.
Note: some studies report that PBC-specific ANA such as Gp210 and Sp100 antibodies are predictive for a more aggressive PBC phenotype.

Clinical cases: 05-I Patient JN
∗ Patient JN, 53 year old woman, investigated by her GP for inflammatory back pain.
∗ Found to have deranged LFTs: ALP = 169 (NR 30-130) ALT = 112 (NR <40).
∗ Viral serology (HAV, HBV, HCV) negative. ∗ Marked polyclonal elevated IgG 23.00 g/L (NR 5.80-15.40) and
IgM 12.60 g/L (NR 0.71-2.30). ∗ Autoantibody screen on rodent LKS substrate showed a
strong AMA at 1:80. ∗ ?Significance of these results: Any further tests? ∗ Although an high titre AMA is present, the liver biochemistry
and immunoglobulins are not consistent with PBC alone (^^IgG and ^^ALT). Is the AMA masking another pattern?
∗ Liver antibody immunoblotting revealed high titre AMA-M2 (+++) and anti-liver cytosol 1 (LC1) (+++) antibodies. Obscured on the LKS IIF (liver tissue) by the AMA.
∗ Patient has PBC-AIH (type II) overlap syndrome
LC
AMA

Clinical cases: 05-II Patient JN
∗ Patient JN> liver biopsy report extract: ∗ The appearances suggest a florid inflammatory cholangiopathy with features of granulomatous
cholangitis. There is duct loss affecting less than a third of bile ducts and only very mild chronic cholestasis. In addition, there are unusual multinucleated giant cells containing retractile material. There is associated, at least moderate chronic hepatitis and focal portal-portal bridging fibrosis. While overall slightly unusual, in particular the multinucleated giant cells containing retractile material, in the given clinical context the appearances are most consistent with primary biliary cholangitis associated with a significant hepatitis that would suggest an overlap with autoimmune hepatitis.
∗ Please correlate very closely with clinical, laboratory and imaging findings.
∗ Note: liver histology finding during the investigation of autoimmune liver disease (particularly PBC and AIH) can be quite non-specific and typically support a diagnosis. Often the underlying cause cannot be established with certainty based on histology alone.
∗ The diagnostic specificity of the investigation for autoimmune liver disease relies heavily on autoantibody results.

Clinical cases: 06 Patient BC ∗ Patient BC, 51 year woman, joint pains and diarrhoea. PMHx underactive thyroid and pernicious
anaemia. ∗ Found to have deranged LFTs: ALT = 131 (NR <40) with normal ALP and bilirubin. ∗ Viral serology (HAV, HBV, HCV) negative. Coeliac serology negative. ∗ Marked polyclonal elevated IgG 23.00 g/L (NR 5.80-15.40)> IgG1 pattern on electropherogram. ∗ Autoantibody screen showed a fine speckled ANA at 1:160. ENA testing revealed an anti-Ro
antibody. ∗ Rodent LKS IIF was negative except for the fine speckled ANA. ∗ ?Significance of these results: Any further tests? ∗ Liver biochemistry and immunoglobulins suggestive of autoimmune liver disease but no
antibodies other than anti-Ro, determined as Ro52> this is a clue! There is also a history of other autoimmune diseases (PA).
∗ Liver antibody immunoblotting revealed high titre anti-soluble liver antigen (SLA +++) antibodies. Anti-SLA antibodies cannot be detected on rodent LKS substrate but almost always occur in combination with Ro52 (>95% of cases). If there’s a high index of suspicion consider immunoassay testing for liver-specific antibodies> SLA can be the only AIH-specific antibody.
∗ Patient has AIH (SLA type) confirmed by liver biopsy findings. Currently treated with azathioprine.

∗ EASL Clinical Practice Guidelines: The diagnosis and management of patients with primary biliary cholangitis. Journal of Hepatology, Vol. 67, Issue 1, p145–172.
∗ EASL Clinical Practice Guidelines: Autoimmune hepatitis. Journal of Hepatology, Vol. 63, Issue 4, p971-1004.
∗ Autoimmune hepatitis – Update 2015. Manns et al. Journal of Hepatology, Vol. 62, Issue 1, Supplement, Pages S100–S111.
∗ Diagnosis and Management of Paediatric Autoimmune Liver Disease: ESPGHAN Hepatology Committee Position Statement. Mieli-Vergani et al. J Pediatr Gastroenterol Nutr. 2017 Nov 3.
∗ International Autoimmune Hepatitis Group Report: review of criteria for diagnosis of autoimmune hepatitis. Alvarez et al. J Hepatol. 1999 Nov;31(5):929-38.
∗ Simplified Criteria for the diagnosis of autoimmune hepatitis. Hennes EM, et al. Hepatology 2008;48:169–76.
∗ Diagnosis and management of autoimmune hepatitis. Manns et al. Hepatology. 2010 Jun;51(6):2193-2213
Some useful guidelines

• Hov JR, Boberg KM, Karlsen TH. Autoantibodies in primary sclerosing cholangitis. World J Gastroenterol. 2008 Jun 28;14(24):3781-91. Review. PubMed PMID: 18609700; PubMed Central PMCID: PMC2721433.
• Rudic JS, Poropat G, Krstic MN, Bjelakovic G, Gluud C. Ursodeoxycholic acid for primary biliary cirrhosis. Cochrane Database Syst Rev. 2012 Dec 12;12:CD000551. doi: 10.1002/14651858.CD000551.pub3. Review. PubMed PMID: 23235576.
• Hirschfield GM, Gershwin ME. The immunobiology and pathophysiology of primary biliary cirrhosis. Annu Rev Pathol. 2013 Jan 24;8:303-30. doi: 10.1146/annurev-pathol-020712-164014. Review. PubMed PMID: 23347352.
• Kumagi T, Heathcote EJ. Primary biliary cirrhosis. Orphanet J Rare Dis. 2008 Jan 23;3:1. doi: 10.1186/1750-1172-3-1. Review. PubMed PMID: 18215315; PubMed Central PMCID: PMC2266722.
• Nakamura M, Kondo H, Mori T, Komori A, Matsuyama M, Ito M, Takii Y, Koyabu M, Yokoyama T, Migita K, Daikoku M, Abiru S, Yatsuhashi H, Takezaki E, Masaki N, Sugi K, Honda K, Adachi H, Nishi H, Watanabe Y, Nakamura Y, Shimada M, Komatsu T, Saito A, Saoshiro T, Harada H, Sodeyama T, Hayashi S, Masumoto A, Sando T, Yamamoto T, Sakai H, Kobayashi M, Muro T, Koga M, Shums Z, Norman GL, Ishibashi H. Anti-gp210 and anti-centromere antibodies are different risk factors for the progression of primary biliary cirrhosis. Hepatology. 2007 Jan;45(1):118-27. PubMed PMID: 17187436.
• Liberal R, Grant CR, Sakkas L, Bizzaro N, Bogdanos DP. Diagnostic and clinical significance of anti-centromere antibodies in primary biliary cirrhosis. Clin Res Hepatol Gastroenterol. 2013 Jul 19. doi:pii: S2210-7401(13)00092-2. 10.1016/j.clinre.2013.04.005. [Epub ahead of print] PubMed PMID: 23876351.
• Wesierska-Gadek J, Penner E, Battezzati PM, Selmi C, Zuin M, Hitchman E, Worman HJ, Gershwin ME, Podda M, Invernizzi P. Correlation of initial autoantibody profile and clinical outcome in primary biliary cirrhosis. Hepatology. 2006 May;43(5):1135-44. PubMed PMID: 16628641.
• Chazouilleres O, Wendum D, Serfaty L, Montembault S, Rosmorduc O, Poupon R: Primary biliary cirrhosis-autoimmune hepatitis overlap syndrome: clinical features and response to therapy. Hepatology 1998, 28:296-301.
• Talwalkar JA, Keach JC, Angulo P, Lindor KD: Overlap of autoimmune hepatitis and primary biliary cirrhosis: an evaluation of a modified scoring system. Am J Gastroenterol 2002, 97:1191-1197.
• Grønbæk L, et al. J Hepatol 2014;60:612–7; EASL CPG AIH. J Hepatol 2015;63:971–1004. • Bottazzo GF, Florin-Christensen A, Fairfax A, Swana G, Doniach D, Groeschel-Stewart U. Classification of smooth muscle
autoantibodies detected by immunofluorescence. J Clin Pathol. 1976 May;29(5):403-10. • Younossi ZM, Stepanova M, Golabi P, Epstein RS, Strauss ME, Nader F, Racila A. Factors Associated With Potential Progressive
Course of Primary Biliary Cholangitis: Data From Real-world US Database. J Clin Gastroenterol. 2018 Aug 24. • Manns et al. Diagnosis and management of autoimmune hepatitis. Hepatology. 2010 Jun;51(6):2193-2213
Bibliography I

∗ Alvarez F, Berg PA, Bianchi FB, Bianchi L, Burroughs AK, Cancado EL, Chapman RW, Cooksley WG, Czaja AJ, Desmet VJ, Donaldson PT, Eddleston AL, Fainboim L, Heathcote J, Homberg JC, Hoofnagle JH, Kakumu S, Krawitt EL, Mackay IR, MacSween RN, Maddrey WC, Manns MP, McFarlane IG, Meyer zum Büschenfelde KH, Zeniya M, et al. International Autoimmune Hepatitis Group Report: review of criteria for diagnosis of autoimmune hepatitis. J Hepatol. 1999 Nov;31(5):929-38.
∗ Obermayer-Straub P, Perheentupa J, Braun S, Kayser A, Barut A, Loges S, Harms A, Dalekos G, Strassburg CP, Manns MP. Hepatic autoantigens in patients with autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. Gastroenterology. 2001 Sep;121(3):668-77.
∗ Floreani A, Liberal R, Vergani D, Mieli-Vergani G. Autoimmune hepatitis: Contrasts and comparisons in children and adults - A comprehensive review. J Autoimmun. 2013 Oct;46:7-16.
∗ Liberal R, Mieli-Vergani G, Vergani D. Clinical significance of autoantibodies in autoimmune hepatitis. J Autoimmun. 2013 Oct;46:17-24
∗ Ryu HS, Kim H. IgG4-related sclerosing cholangitis: liver biopsy findings. Korean J Hepatol. 2011 Mar;17(1):76-9. ∗ Hennes EM, et al. Simplified Criteria for the diagnosis of autoimmune hepatitis. Hepatology 2008;48:169–76; ∗ EASL Clinical Practice Guidelines: The diagnosis and management of patients with primary biliary cholangitis. Journal of
Hepatology, Vol. 67, Issue 1, p145–172. ∗ EASL Clinical Practice Guidelines: Autoimmune hepatitis. Journal of Hepatology, Vol. 63, Issue 4, p971-1004. ∗ Manns MP, Lohse AW, Vergani D. Autoimmune hepatitis – Update 2015. Journal of Hepatology, Vol. 62, Issue 1, Supplement,
Pages S100–S111. ∗ Terjung B, Spengler U. Atypical p-ANCA in PSC and AIH: a hint toward a "leaky gut"? Clin Rev Allergy Immunol. 2009
Feb;36(1):40-51. ∗ Terjung B, Söhne J, Lechtenberg B, Gottwein J, Muennich M, Herzog V, Mähler M, Sauerbruch T, Spengler U. p-ANCAs in
autoimmune liver disorders recognise human beta-tubulin isotype 5 and cross-react with microbial protein FtsZ. Gut. 2010 Jun;59(6):808-16.
∗ Mieli-Vergani G, Vergani D, Baumann U, Czubkowski P, Debray D, Dezsofi A, Fischler B, Gupte G, Hierro L, Indolfi G, Jahnel J, Smets F, Verkade HJ, Hadzic N. Diagnosis and Management of Paediatric Autoimmune Liver Disease: ESPGHAN Hepatology Committee Position Statement. J Pediatr Gastroenterol Nutr. 2017 Nov 3. doi: 10.1097/MPG.0000000000001801. [Epub ahead of print] PubMed PMID: 29112085.
∗ Dahlqvist G, Gaouar F, Carrat F, Meurisse S, Chazouillères O, Poupon R, Johanet C, Corpechot C; French network of Immunology Laboratories. Large-scale characterization study of patients with antimitochondrial antibodies but nonestablished primary biliary cholangitis. Hepatology. 2017 Jan;65(1):152-163.
Bibliography II


![Application for inclusion of tenofovir disoproxil fumarate ... · et al AASLD 2014; Corsa et al, AASLD 2014] o Regression of liver fibrosis and reversal of cirrhosis [Marcellin et](https://img.dokumen.tips/doc/110x75/5c4aa6de93f3c34c50653abc/application-for-inclusion-of-tenofovir-disoproxil-fumarate-et-al-aasld-2014.jpg)


























