-
7/28/2019 T Dada f Imaging Do's and Donts
1/60
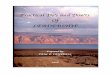
ONH and RNFL Imaging
Interpreting Results
Tanuj Dada
Additional Professor
Dr RP Centre for Ophthalmic Sciences
All India Institute of Medical Sciences
New Delhi
-
7/28/2019 T Dada f Imaging Do's and Donts
2/60
Q.Why do we need Imaging ?
-
7/28/2019 T Dada f Imaging Do's and Donts
3/60
WGA : New Glaucoma Definition
Progressive Structural
Optic Nerve Damage
is the NEW Gold Standard.
-
7/28/2019 T Dada f Imaging Do's and Donts
4/60
Undetectable Disease May Progress
to Functional Impairment
VF=visual field.
Adapted from Weinreb et al.Am J Ophthalmol.
2004;138:458-467.
Normal
Acceleration of
apoptosis
Ganglion celldeath/axon loss
RNFL change(undetectable)
RNFL change(detectable)
SWAP VF changes
SAP VF change
VF change (moderate)
VF change (severe)
Blindness
-
7/28/2019 T Dada f Imaging Do's and Donts
5/60
Does imaging add to clinical care ?
Nearly 50% of glaucoma patients did not have a disc drawing
or
photograph taken at the time of initial examination
Fremont AM, Lee PP, Mangione CM, et al. Patterns of care for
open-angle glaucoma in managed care. Arch
Ophthalmol. 2003;121:77783.
1. Baseline documentation of the disc changes
2. Evaluation of the disc size
3. Risk Assessment (OHTS CSLO study)
4. Early diagnosis
5. Documentation of progression
x Pallor, Hemorrhage
-
7/28/2019 T Dada f Imaging Do's and Donts
6/60
WGA Recommendation
The World Glaucoma Association &
American Academy of Ophthalmology
recommend
Imaging as part of routine clinical care
-
7/28/2019 T Dada f Imaging Do's and Donts
7/60
Q.
With so many high tech. machineswhy is there a problem in
diagnosing glaucoma withimaging ?
-
7/28/2019 T Dada f Imaging Do's and Donts
8/60
Normal Biological Variability ?
Large variability in optic nerve head
0.7 1.5 million optic nerve axons
This huge Normal Variability
Limits ability to differentiate between
healthy eyes and glaucoma at one point in time
-
7/28/2019 T Dada f Imaging Do's and Donts
9/60
Patient A presents with 1 million nerve fibers
Q1. Did he start of with 1 million (within normal range)
Q2. Did he start of with 1.4 million (within normal range)
Early Diagnosis : A myth
People in the statistically normal rangemayundergo optic disc
and RNFL changes over
time and yet still remain within the normal
range on the basis of any single exam alone.
-
7/28/2019 T Dada f Imaging Do's and Donts
10/60
Normative Databases are indicators and not
specific enough for definitive diagnosis
Glaucoma Diagnosis
We need to document progressivestructural loss over time
The patient is his own best normal and to
diagnose glaucoma you need to monitor
change over time
-
7/28/2019 T Dada f Imaging Do's and Donts
11/60
Q.Test Re-Test Variability
-
7/28/2019 T Dada f Imaging Do's and Donts
12/60
VariabilityScan done on 4rth march 2006 2.51 pm Scan done on
4rthmarch 2006 3.00 pm
-
7/28/2019 T Dada f Imaging Do's and Donts
13/60
Triple Scan GDx Version 6.0
-
7/28/2019 T Dada f Imaging Do's and Donts
14/60
Image Quality: Standard
Deviation< 10 m Excellent10 - 20 m Very Good
20 - 30 m Good30 - 40 m Acceptable
40 - 50 m Try to improve
> 50 m Poor quality
documentation
only
-
7/28/2019 T Dada f Imaging Do's and Donts
15/60
Image Quality Standard
DeviationHigh quality images with low Standard
Deviations (7-30 m) allow us to detect
small changes.Lower quality images i.e. higher Standard
Deviations (30-50+ m) mean there is more
noise and thus changes need to be much
bigger before we can detect them.
-
7/28/2019 T Dada f Imaging Do's and Donts
16/60
Image Quality
We want to compare similiar quality images to
be more assured that change is real and not
due to fluctuations in image quality
SD 10 SD 11 SD 12 SD 9 SD 10
-
7/28/2019 T Dada f Imaging Do's and Donts
17/60
Image Quality
We want to compare similiar quality images to
be more assured that change is real and notdue to fluctuations
in image quality
-
7/28/2019 T Dada f Imaging Do's and Donts
18/60
Review Image Quality
Standard Deviations should ideally be
within 5m of each other
Exclude outliers from the Progression Series
-
7/28/2019 T Dada f Imaging Do's and Donts
19/60
Astigmatism
Astigmatism introduces an optical rotation into theimage,
affecting image quality.
This rotation must be corrected for using astigmatic
corrective lenses if the cylinder is more than 1D
-
7/28/2019 T Dada f Imaging Do's and Donts
20/60
Q.Impact of signal strength ?
-
7/28/2019 T Dada f Imaging Do's and Donts
21/60
Impact of Signal Strength on RNFL
Differences in signal strength were associated withdifferences
in average RNFL thickness
Even under optimal testing conditions, scan quality can
adversely effect the ability to detect change over time
Therefore, caution is warranted when detectingglaucomatous
progression using scan series
of different quality
Signal strength of > 7 is mandatory
Vizzeri G, Bowd C, Medeiros FA, Weinreb RN, Zangwill LM.
Am J Ophthalmol. 2009 Aug;148(2):249-255
-
7/28/2019 T Dada f Imaging Do's and Donts
22/60
Signal Strength
Factors influencing
Lenticular opacification
Posterior capsule opacification
Ocular surface disease dry eye
-
7/28/2019 T Dada f Imaging Do's and Donts
23/60
62 F CORTICAL
CATARACT OD
SIGNAL STRENGTH
6/10
-
7/28/2019 T Dada f Imaging Do's and Donts
24/60
patient underwent
cataract surgery
OCT 4 weeks later
Post operative SD-OCT
SIGNAL
STRENGTH 8/10
-
7/28/2019 T Dada f Imaging Do's and Donts
25/60
GDxVCC parameters pre and post
cataract surgery(Dada T et al. Indian J Ophthalmol. 2010
Sep-Oct;58(5):389-94 )
RNFL Parameters Pre operative Post operative P value
TSNIT average 49.2 14.1 56.5 7.6 0.001
Superior average 51.6 12.2 59.8 7.3 0.004
Inferior average 50.2 13.7 61.5 10.3 0.001
NFI 41.3 15.3 21.6 11.8 0.001
-
7/28/2019 T Dada f Imaging Do's and Donts
26/60
BEFORE
Phaco IOL
AFTER
Phaco IOL
-
7/28/2019 T Dada f Imaging Do's and Donts
27/60
Q.
How to increase the
signal strength ?
-
7/28/2019 T Dada f Imaging Do's and Donts
28/60
Increasing Signal StrengthEnsure the Ocular Lens is Clean
Adjust Focus
Optimize PolarizationInstruct the patient not to blink during
optimization
Ensure the scan is not too low horizontally
Stable Tear film ask patient to blink before scan is
acquired
In case of media opacity , move the pupil alignment off-center
by
clicking in a different spot on the pupil in the iris viewer
or
adjusting the chinrest position.
-
7/28/2019 T Dada f Imaging Do's and Donts
29/60
Q.Effect of Disc Size?
-
7/28/2019 T Dada f Imaging Do's and Donts
30/60
-
7/28/2019 T Dada f Imaging Do's and Donts
31/60
False Positive HRT
Large Disc CD Ratio = 0.85: 1
-
7/28/2019 T Dada f Imaging Do's and Donts
32/60
Disc Size : MRA, GPS
Jindal S, Dada T et al .Indian J Ophthalmol. 2010
Nov-Dec;58(6):487-92.Comparison of the diagnostic ability of
Moorfield's regression analysis
and glaucoma probability score using Heidelberg retinal
tomograph III in
eyes with primary open angle glaucoma (n =50)
The sensitivity increased with increasing disc sizefor both MRA
and GPS and vice versa
There was a poor agreement between the overall
MRA and GPS classifications.
-
7/28/2019 T Dada f Imaging Do's and Donts
33/60
-
7/28/2019 T Dada f Imaging Do's and Donts
34/60
Q.Effect of centration ?
-
7/28/2019 T Dada f Imaging Do's and Donts
35/60
Before you
comment on
Progression
Check
Centration
-
7/28/2019 T Dada f Imaging Do's and Donts
36/60
Q.Effect of IOP?
-
7/28/2019 T Dada f Imaging Do's and Donts
37/60
IOP lowering can impact ONH
Check IOP from exam to exam
Changes of 2 or 3 mm Hg not significant
Changes of 10 mm Hg could be significant
-
7/28/2019 T Dada f Imaging Do's and Donts
38/60
Q.Glaucoma with ARMD ?
-
7/28/2019 T Dada f Imaging Do's and Donts
39/60
Scanning Laser Polarimetry (780 nm)
with variable corneal compensation
Is based on the principle that polarized light ischanged as it
passes through the Retinal Nerve
Fiber Layer
Variable Corneal Compensation eliminates
the effect of Corneal Polarization
GDx VCC
-
7/28/2019 T Dada f Imaging Do's and Donts
40/60
GDx VCC
Macular scan is performed
Henle fibers = uniform
birefringence
Abnormal Birefringence pattern
of Henle s Layer yields corneal
birefringence
Corneal birefringence is then
eliminated to give actual
RNFL thickness measurement
Macular birefringence
note bow tie pattern
without compensation
-
7/28/2019 T Dada f Imaging Do's and Donts
41/60
Parameter Protocol I (a) Protocol II (b)p value
a vs. bProtocol I (c) Protocol II (d)
Normal Abnormal Macula
TSNIT Average 51.9 4.7 52.8 5.1 0.02 78.6 33.3 53.9 8.4
Superior Average 63.1 7.1 66.1 6.9 0.003 82.7 32.1 62.0 12.1
Inferior Average 58.8 7.5 59.9 6.7 0.2 77.7 31.9 59.9 10.7
NFI 22.7 9.2 19.3 8.6 0.01 14.2 14.1 25.8 16.9
Dada T , Dave V ARVO 2010
-
7/28/2019 T Dada f Imaging Do's and Donts
42/60
Standard
Scan
Protocol
Irregular
Scan
Protocol
-
7/28/2019 T Dada f Imaging Do's and Donts
43/60
Q.Effect of Peripapillary Atrophy?
-
7/28/2019 T Dada f Imaging Do's and Donts
44/60
False Negative
Supra - Normal
Peripapillary
Atrophy
Problems with
GDxVCC
-
7/28/2019 T Dada f Imaging Do's and Donts
45/60
J Glaucoma (2009)
3 scan diameter scans
2.4 - 3.2 mm
3.2 - 4.0 mm
4.0 - 4.8 mm
-
7/28/2019 T Dada f Imaging Do's and Donts
46/60
Q.
Correlate fundus examination
with imaging and perimetry ?
-
7/28/2019 T Dada f Imaging Do's and Donts
47/60
-
7/28/2019 T Dada f Imaging Do's and Donts
48/60
Correlation of structure & function
-
7/28/2019 T Dada f Imaging Do's and Donts
49/60
Does an Abnormal Scan
indicates Glaucoma ?
-
7/28/2019 T Dada f Imaging Do's and Donts
50/60
44 yr male open angle, CCT 530, IOP 20-22 mmHg
-
7/28/2019 T Dada f Imaging Do's and Donts
51/60
-
7/28/2019 T Dada f Imaging Do's and Donts
52/60
-
7/28/2019 T Dada f Imaging Do's and Donts
53/60
-
7/28/2019 T Dada f Imaging Do's and Donts
54/60
A Word of Caution !
Imaging
Does not replace your clinical examination
Provides additional clinical information which is
useful in the diagnosis and management ofyour patients
-
7/28/2019 T Dada f Imaging Do's and Donts
55/60
Take Home Message
Imaging is critical in diagnosis and
management of glaucoma
Expert operator and expert interpreter
Use your own eyes and brain in
conjunction with machinery
Check image quality at each visit and correlate
structural changes with functional deficits
Thank You
-
7/28/2019 T Dada f Imaging Do's and Donts
56/60
Thank You
-
7/28/2019 T Dada f Imaging Do's and Donts
57/60
Q.How to identify Progression ?
How to Diagnose :
-
7/28/2019 T Dada f Imaging Do's and Donts
58/60
How to Diagnose :
Glaucoma progression
Exam 1 : RNFL thickness = 100 microns
December 2010
Exam 2 : RNFL thickness = 97 microns
July 2011
Logical Conclusion = 3 microns loss of RNFL thickness
Patient has progressed : Initiate or escalate treatment
-
7/28/2019 T Dada f Imaging Do's and Donts
59/60
Glaucoma progression
Must know test re-test variability
Exam 1 : RNFL thickness = 100 microns
Exam 2 : RNFL thickness = 97 microns
Exam 3 : RNFL thickness = 103 microns
Truth : Normal Test Re-Test Variability is 6 microns
so you cannot take 3 micron loss as progression
-
7/28/2019 T Dada f Imaging Do's and Donts
60/60
Baseline Imaging Exam
Must do test re-test variability to
establish range of variability
If change during follow up is more than
test re-test variability -
Only then can you call it a progression