Embed Size (px)
Citation preview

18
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
Surgical Strategy for Infective Endocarditis in This Era
อ.นพ.สรภพทพมงคล โรงพยาบาลมหาวทยาลยนเรศวร
Introduction
Infective Endocarditis (IE) เปนโรคตดเชอของเยอบหวใจ ลนหวใจ และหลอดเลอด โดยทวไปจะพบพยาธสภาพนทลนหวใจเปนสวนมาก ปจจบนคำจำกดความของโรคกลมนยงรวมไปถงสงแปลกปลอม หรออปกรณเครองมอทางการแพทยตางๆทฝงอยในรางกาย ทมอบตการณมากขนเรอยๆ เชน electrical cardiac device ตางๆเปนตน
อบตการณเกดของโรค Infective Endocarditis ทวโลกโดยประมาณ 5-15 คนตอประชากร 100,000 คนตอป โดยสดสวนจะพบในผชาย มากกวาผหญง ประมาณ 3 : 1 นอกจากนยงพบวารอยละ 75 ของคนไข IE จะมความผดปกตของหวใจอยกอนแลว1 การศกษาในป ค.ศ.1999 พบวารอยละ 38 คนไข IE จะพบพยาธสภาพท aortic valve รอยละ 34 พบท mitral valve รอยละ 8 พบทง aortic valve และ mitral valve อกรอยละ 4 พบท tricuspid valve นอกจากนยงพบในกลมคนไขโรค หวใจพการแตกำเนดประมาณรอยละ 3.52
อบตการณในประเทศไทย ขอมลจากโรงพยาบาลศรนครนทร ขอนแกน ในชวงป ค.ศ. 1990-2002 (ตารางท1) โดยจำแนกตามตำแหนง พยาธสภาพท aortic valve, mitral valve, both aortic and mitral valve และ tricuspid valve โดยประมาณรอยละ 43.8, 43.1, 2.5 และรอยละ 7.4 ตามลำดบ3 โดยพบวาพยาธสภาพเกดขนท aortic valve และ mitral valve พอๆ กนและอบตการณใกลเคยงกบตางประเทศ นอก จากนจะเหนวา สดสวนของคนไข IE รอยละ 75 จะมความผดปกตของ หวใจรวมอยกอนแลวโดยพบวา underlying heart disease ทพบไดบอย ทสดในประเทศไทย

19
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
คอ rheumatic heart disease จากขอมลของประเทศ ไทยจะพบวา congenital heart disease เปนสาเหตของ IE ประมาณรอยละ 10 นอก จาก นเชอทเปนสาเหตของ IE จากการรวบรวมขอมลโรงพยาบาลศรราช โรงพยาบาลมหาราชนครเชยงใหม โรงพยาบาลขอนแกน3-6 (ตารางท 2) ในประเทศไทยสามารถตรวจพบเชอไดประมาณรอยละ 13-48 เทานน สวน เชอทพบไดในประเทศไทย สวนใหญจะเปนเชอ Streptococci spp.ซง มความ แตกตางจากประเทศทพฒนาแลวโดยเชอสวนใหญ เปน Staphylococcus aureus
ววฒนาการและการคนพบโรค IE นเกดขนมาตงแต Lazarus Riverius (ค.ศ.1589-1655) ไดคนพบพยาธสภาพของโรคนขนครงแรก จนกระทงในป ค.ศ. 1885 Dr. William Osler ไดศกษาจนเขาใจพยาธ สภาพ ลกษณะทาง clinics ของคนไขกลมน และไดสรปความรทงหมด ลงใน Gusltonian Lectures ซงทำใหแพทยสวนใหญเขาใจโรคนไดมาก ขน 7 ในป ค.ศ. 1994 Dr. Durack และคณะ จากมหาวทยาลย Duke University Medical Center ไดมการนำเครอง Transthoracic echocardiography มาชวยใชชวยในการวนจฉย หรอทรจกกนวา Duke Criteria หลงจากนนไดมการพฒนาปรบปรงแกไขจนกระทง ป ค.ศ. 2000 ไดเกณฑในการวนจฉยเปน Modified Duke Criteria8 (ตารางท3-5) นอกจากนในปจจบนยงไดมการนำเอา Transesophageal echocardiography (TEE) ซงมประสทธภาพมากกวา Transthoracic echocardiography (TTE) มาชวยในการวนจฉยทำใหสามารถ ตรวจพบ small vegetation ไดและยงมการพฒนาปรบปรงการรกษาจนไดยาปฏชวนะ regimens ตางๆ ทมประสทธภาพ แตทวาในชวงเวลา 40 ปทผานมา อตราการเสยชวต ของคนไข left-side IE ยงคงทอยประมาณ 30%-40%ไมเปลยนแปลงถงแมวาจะมการพฒนาการวนจฉยและการรกษาดานตางๆแลวกตาม9-10

20
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
ตารางท1:ClinicalcharacteristicfromSrinagarindHospital,KhonKaen,Thailand3

21
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
ตารางท2:ThecausativeorganismscausinginfectiveendocarditisfromMaharajNakornChiangMaiHospital,Thailand4

22
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
ตารางท3:DefinitionofInfectiveEndocarditisAccordingtotheModifiedDukeCriteria8

23
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
ตารางท4:DefinitionofTermsUsedintheModifiedDukeCriteriafortheDiagnosisofIE8
24
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
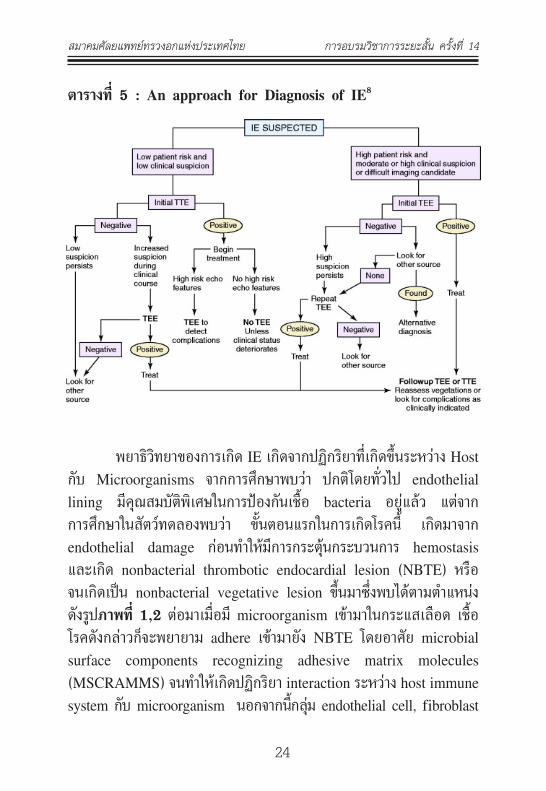
ตารางท5:AnapproachforDiagnosisofIE8
พยาธวทยาของการเกด IE เกดจากปฏกรยาทเกดขนระหวาง Host กบ Microorganisms จากการศกษาพบวา ปกตโดยทวไป endothelial lining มคณสมบตพเศษในการปองกนเชอ bacteria อยแลว แตจาก การศกษาในสตวทดลองพบวา ขนตอนแรกในการเกดโรคน เกดมาจาก endothelial damage กอนทำใหมการกระตนกระบวนการ hemostasis และเกด nonbacterial thrombotic endocardial lesion (NBTE) หรอ จนเกดเปน nonbacterial vegetative lesion ขนมาซงพบไดตามตำแหนง ดงรปภาพท1,2ตอมาเมอม microorganism เขามาในกระแสเลอด เชอ โรคดงกลาวกจะพยายาม adhere เขามายง NBTE โดยอาศย microbial surface components recognizing adhesive matrix molecules (MSCRAMMS) จนทำใหเกดปฏกรยา interaction ระหวาง host immune system กบ microorganism นอกจากนกลม endothelial cell, fibroblast

25
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
และ platelet ยงมการผลตสาร fibronectin ซงชวยทำให microorganism จบกบ vegetation ไดดยงขน15 กลไกดงกลาวนจงสามารถอธบายการเกด โรค IE ในคนไขทม underlying heart diseases แตขอมลเรารวามคนไข IE ประมาณรอยละ 30 ทไมม preexisting cardiac abnormality นำมากอน แสดงวาในกรณน เกดมาจากเชอซงมความรนแรงมากจงสามารถตดเชอเขาไปใน normal valve ได อนไดแก S. aureus, some streptococci, Salmonella, Rickettsia, Borrelia and Candida2
ภาพท 1: The steps in the development of the endocarditislesion15
ภาพท2:Sitesofhigh-velocityjetswhereendocarditisvegeta-tionsoccur15

26
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
ปจจบนไดมการตพมพแนวทางการรกษา Infective Endocarditis มากมาย โดยในป ค.ศ. 2005 โดยทาง American College of Cardiology รวมกบ American Heart Association ไดจดทำ guideline8 ขนและไดมการปรบปรงขอมลเพมเตมในป ค.ศ. 2008 สวนทางฝงดานยโรปกไดม การจดทำ guideline ในป ค.ศ. 200912 ซงมสวนทคลายคลงกน แตทวา evidence based ทเกยวกบทางดานศลยกรรมยงไมชดเจน โดยเฉพาะขอมล ทเกยวกบทางดานการผาตดโดยตรง ไมวาจะเปนขอมลเกยวกบ เวลาท เหมาะสมทควรจะนำผปวยไปผาตด หรอการผาตดวธไหนดกวากนระหวางการทำ Mitral Valve Replacement หรอ Mitral Valve Repair และ ถาตองทำ Mitral Valve Replacement ลนหวใจชนดไหนทเหมาะสมทสด หรอกรณ Native Aortic Valve Endocarditis จำเปนตองใช Aortic Allograft (Homograft)เมอไหร หรอ แนวทางในการรกษาคนไข IE ทม Neurological complications เชน Ischemic Stroke, Intracerebra hemorrhage due to ruptured Intracerebral Mycotic Aneurysm (IMAs) ซงเปนกลมคนไข IE ทมอตราตายสง แลวเราจะมแนวทางใน การรกษาคนไขกลมนอยางไร ทำใหในชวงเวลาดงกลาวนนมการตพมพ Review article, systemic reviews และ meta-analysis ออกมามากมายเพอชวยตอบคำถามเหลาน13-17 ลาสดทางสมาคม The Society of Thoracic Surgeons (STS) ไดตพมพ Clinical Practice Guidelines ขนในป ค.ศ.201118 ซงผนพนธจะขออางถง guideline อนนเปนสวนใหญ แมวาบางจดใน guideline นจะขดแยงกบ ACC/AHA Guideline 2008 กตามแตเปนมมมองทมประโยชนแกศลยแพทย แตทวาใน guideline น ยงขาดคำแนะนำบางสวนทละเอยดเกยวกบการดและคนไขทม neurologic complications จาก IE ผนพนธกจะขอนำเอาขอมลจากการ review literatures มารวมดวย

27
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
SurgeryforInfectiveEndocarditis
ศลยกรรมมบทบาทอยางมากในการรกษา Infective Endocarditis โดยถอวาเปน potential lifesaving โดย surgery มบทบาทในชวง acute โดยประมาณรอยละ 25-50 และในชวง convalescence อกประมาณ รอยละ 20-40 การผาตดในผปวย acute IE บอยครงทยากในแงของ เทคนคการ ผาตด และอกทงปจจยเสยงจากสภาวะของคนไขรวมดวย เพราะวาคนไขกลมนมกมอาการหวใจวายรนแรง สงผลทำใหอวยวะตางๆ ในรางกายทำงานบกพรอง ทำให overall surgical mortality in acute IE อยประมาณรอยละ 6-25 (ดงภาพท 3) ซงจะเหนวาในสภาวะ acute IE การรกษาโดยการใหยาปฏชวนะอยางเดยวมแนวโนมอตราตายใน 6 เดอนแรกสงกวาการรกษารวมกนระหวางยาปฏชวนะ แตอยางไรกตามการผาตด โดยเฉลย long-term survival rate อยทประมาณรอยละ 7012,19-21
รปภาพท3:Six-monthsurvivalinpatientswithendocarditisandmoderate-severeheartfailure21

28
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
ขอบงชในการผาตดสวนใหญมาจาก complications ของ IE (ตารางท6)14 โดยขอบงชสวนใหญคอ congestive heart failure (60%), refractory sepsis (40%), embolic complications (18%), and vegetation size (48%) ซงบางครงขอบงชในการผาตดอาจมจากหลายปจจยรวมกน หรออาจจำแนกได หรออาจจะแบงตามชวงเวลาซงจะชวยทำใหสามารถ นำไปปฏบตไดเขาใจงายยงขน (ตารางท 7)15
ตารางท6:Complicationsofinfectiveendocarditis15
IndicationforSurgeryinInfectiveEndocarditis15
1.Congestiveheartfailure - Congestive heart failure caused by severe aortic or mitral regurgitation or, more rarely, by valve obstruction caused by vegetations.

29
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
- Severe acute aortic or mitral regurgitation with echocar-diographic signs of elevated left ventricular end-diastolic pressure or significant pulmonary hypertension
- Congestive heart failure as a result of prosthetic dehiscence or obstruction
2.Periannularextension
- Most patients with abscess formation or fistulous tract formation
3.Systemicembolism
- Recurrent emboli despite appropriate antibiotic therapy
- Large vegetations (>10 mm) after 1 or more clinical or silent embolic events after initiation of antibiotic therapy
- Large vegetations and other predictors of a complicated course
-Very large vegetations (>15 mm) without embolic complications, especially if valve-sparing surgery is likely (re-mains controversial)
4.Cerebrovascularcomplications
- Silent neurological complication or transient ischemic attack and other surgical indications
- Ischemic stroke and other surgical indications, provided that cerebral hemorrhage has been excluded and neurological complications are not severe (eg, coma)

30
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
5.Persistentsepsis
- Fever or positive blood cultures persisting more than 5 to 7 days despite an appropriate antibiotic regimen, assuming that vegetations or other lesions requiring
- Surgery persist and that extracardiac sources of sepsis have been excluded
- Relapsing IE, especially when caused by organisms other than sensitive streptococci or in patients with prosthetic valves
6.Difficultorganisms
- S aureus IE involving a prosthetic valve and most cases involving a left-sided native valve
- IE caused by other aggressive organisms (Brucella, Staphylococcus lugdunensis)
- IE caused by multiresistant organisms (eg. methicillin-resistant S aureus or vancomycin-resistant enterococci) and rare infections caused by Gram-negative bacteria
-Pseudomonas aeruginosa IE
-Fungal IE
-Q fever IE and other relative indications for intervention
7.Prostheticvalveendocarditis
- Severe congestive heart failure secondary to valvular dysfunction not responding to inotropic support and afterload reduction

31
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
- Worsening cardiac, renal, or pulmonary function after initial improvement or stabilization
- Persistent bacteremia and sepsis despite one week of antibiotic therapy
- Embolization despite antibiotic therapy or large vegetations demonstrated on echocardiography, with a significant risk of embolization
- Progression of intracardiac or perivalvular pathology identified by echocardiogram or suggested by new or worsening conduction abnormalities
- Significant prosthetic valvular dysfunction or dehiscence or other evidence of sewing ring–native annulus infection
- Annular abscesses, paravalvular leak, sinus, or aortic true or false aneurysm
- Fungal or brucella PVE or late PVE from Staphyloccoccus aureus
-Infection with gram negative organisms or organisms with poor response to antibiotics
-Early PVE (within 2 months)
-Myocardial invasion signs such as new onset conduction abnormalities or atrioventricular block or echocardiogram showing abscesses
- Valve obstruction with vegetations

32
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
ตารางท7:TimingofSurgery15
Emergencysurgery(within24hours)
- Native (aortic or mitral) or prosthetic valve endocarditis and severe
- Congestive heart failure or cardiogenic shock caused by: acute valvular regurgitation, severe prosthetic dysfunction (dehiscence or obstruction) fistula into a cardiac chamber or the pericardial space
Urgentsurgery(withindays)
- Native valve endocarditis with persisting congestive heart failure, signs of poor hemodynamic tolerance, or abscess
- Prosthetic valve endocarditis with persisting congestive heart failure, signs of poor hemodynamic tolerance, or abscess
- Prosthetic valve endocarditis caused by staphylococci or Gram-negative organisms
- Large vegetation (>10 mm) with an embolic event
- Large vegetation (>10 mm) with other predictors of a complicated course
- Very large vegetation (>15 mm), especially if conservative surgery is available - Large abscess and/or periannular involvement with uncontrolled infection
Earlyelectivesurgery(duringthein-hospitalstay)
-Severe aortic or mitral regurgitation with CHF and good

33
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
response to medical therapy
- Prosthetic valve endocarditis with valvular dehiscence or CHF and good response to medical therapy
- Presence of abscess or periannular extension
- Persisting infection when extracardiac focus has been excluded
- Fungal or other infections resistant to medical cure
PreoperativeConsideration
ในปจจบนเปนททราบกนดวา Transesophageal echocardiography (TEE) สามารถตรวจพยาธสภาพทมขนาดเลกเทากบ 1 mm. ไดและเปนทยอมรบกนวามประสทธภาพดกวา เมอเทยบกบ Transthoracic echocar-diography (TTE) โดยพบวา sensitivity ของ TEE:TTE 96%:93% และ specificityของ TEE:TTE 95%:46% ดงนนจงม recommendation8 ดงน

34
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
ตารางท 8 :Use ofEchocardiographyDuringDiagnosis andTreatmentofEndocarditis8
สวน Cardiac catheterization โดยทวไปไมชวยในการวนจฉยโรค IE แตควรทำในคนไขผชายทมอายมากกวา 40 ปขนไป หรอผหญงทหมดประจำเดอน (postmenopausal) หรอในกรณทคนไขมประวต หรอมปจจย เสยงของโรคหลอดเลอดหวใจอดตน แตกระนนกตามกไมควรทำในกรณท ผปวยม large aortic vegetation เพราะอาจ catheter อาจทำใหเกด systemic emboli ไดอาจเปลยนมาทำ CTA หรอ MRI Coronary เพอหา evidenced ของ ischemic heart disease.
ACC/AHA guideline8 แนะนำใหหยด Oral anticoagulant ในคนไขทมอาการ neurological eventsในชวงระยะเวลา 2 สปดาห

35
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
แรกของการเรมรกษา IE โดยเฉพาะถามสาเหตมาจากเชอ S. aureus เนอง มาจากมการศกษาพบวาชวงดงกลาวนมความสมพนธ neurologic adverse outcomes มากโดยเฉพาะ intracerebral hemorrhage or hemorrhagic transformation แตถาหากจำเปนตองใชยา anticoagulant เชนในกรณ prosthetic valve endocarditis อาจเปลยนเปนยากลม Unfractionated heparin ดงนนผเชยวชาญบางทานแนะนำใหหยด anticoagulant แมใน คนไขทไมม neurological events อนเนองมาจากพบวาคนไข IE สวน มากม silent septic emboli ประมาณรอยละ 30 โดยไมแสดงอาการ neurological events ซงอาจสงผลใหม neurological complications ทหลงได 14-15 (some literature suggested LMWH) IntraoperativeManagement
สงสำคญทตองคำนงถงคอ เวลาทเหมาะสมเมอไหรทควรเขาไป ผาตด จำเปนตองรอให antibiotic ครบกอนไหม หรอเมอเกด ischemic stroke or hemorrhagic stroke จะตองรอนานเทาไรถงจะปลอดภยทสด ถา deal กบ aortic valve endocarditis สงทตองพจารณาคอจำเปน จะ ตองใช homograft ในกรณไหน สวนถาเปน native mitral valve endocarditis จะทำการ repair or replace ดกวากน ซงจะอธบายตามหวขอตางๆ ตอไป แตทกอยางอาศยหลกการเดยวกนคอ
TheCornerstonesofsurgicaltreatmentforIE
ประกอบดวยสวนสำคญ 2 ประการ คอ
1.Radicalexcisionofallinfectedandnecrotictissue2.Repairanatomicaldefects(repairorreplacevalve)
นอกจากนสงทสำคญอกสงคอ imaging โดยเฉพาะ Intraop-erative TEE ซงจะชวยใหเราวางแผนในการผาตดไดอยางมประสทธภาพ โดยเฉพาะการตดสนใจ วาจะตอง extensive debridement หรอ การทำ

36
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
valve reconstruction ขนมาใหม โดยเฉพาะในการผาตด native mitral valve endocarditis. หลงจากการตดสวนทตดเชอออกมาแลวนน การสง ตรวจเพอยอมดเชอทนทภายหลงการผาตดกมความสำคญ ในการชวย ปรบ เปลยนยาปฏชวนะใหเหมาะสมไดทนท โดยเฉพาะในกลม Culture- Negative Endocarditis ซงอาจจะมสาเหตมาจาก rare endocarditis pathogens เชน fungal endocarditis, Bartonella species, Coxiella burnetti, Brucella species, Chlamydia species เปนตน
SurgeryforCongestiveHeartFailure
Congestive heart failure เปนสภาวะแทรกซอนทพบไดบอยท สดทงใน Native Valve Endocarditis (NVE) และ Prosthetic Valve Endocrditis (PVE) สาเหตโดยทวไปเกดจาก valve regurgitation ซงเปนผลมาจาก acute perforation of native or prosthesis valve leaflet, rupture of infected mitral chordae, prosthetic valve dehiscence นอกจากนอาจมการแตกทะลเกดเปน fistula ขนระหวางหองหวใจหรออาจทะลออกไปยง pericardial space ได จากรายงานการศกษาพบวาปจจย เสยงทสงผลทำใหเกด early mortality ในคนไข IE ไดแก male gender, DM, S aureus, embolic events, high APACHE II score.
โดยทวไปเมอเกด acute aortic regurgitation (AR) หวใจจะทำงานหนกขนอยางทนททนใด โดยปกตแลว left ventricle (LV) จะทนตอสภาวะ acute AR ไดไมนาน เนองมาจากเกด acute volume overload in LV chamber ซงไมสามารถจะผนเลอดออกไปทางไหนได เพราะ mitral valve ปดสนท ตอมาเกด acute LV distension จงสงผลทำ ให LV function ลดลงอยางรวดเรวจนเกด cardiac shock ดงนนเมอเกดสภาวะนขนจงเปนขอบงชในการผาตดอยางรบดวน (urgent surgery) โดยไมจำเปนตองคำนงถงสภาวะการตดเชอ หรอรอใหยา antibiotics กอน แตถาเปน acute mitral valve regurgitation หวใจ LV จะปรบสภาพ ไดและสามารถทนตอการเกดสภาวะ volume overload ไดมากกวา เนอง

37
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
จากสามารถทนเลอดกลบไปยงปอดได แตถาอาการ congestive heart failure เปนมากขนและไมสามารถ control ดวยยาได โดยเฉพาะยงม functional class III-IV (NYHA) กจำเปนตองรบทำ urgency surgery จะเหนวาถาเรารบนำผปวยไปผาตดรกษา IE ในสภาวะcongestive heart failure อตราการตายจะลดลงอยางชดเจนเมอเปรยบเทยบกบการรกษา ดวยยาเพยงอยางเดยว (รปภาพท 3)
ในบางสถานการณทคนไขสามารถ well-tolerated ตอสภาวะ valve regurgitation ไดดและไมมขอบงชอนๆททำใหตองรบทำการผาตด แนะนำรอใหยาปฏชวนะจนครบ course 6 สปดาหกอนแลวคอยนำผปวย มาทำการผาตดภายหลงจาก infection subside แลว
ในปจจบน The choice of valve prosthesis ในกรณ native valve or prosthesis valve endocarditis (NVE and PVE) ยงคง controversy เนองจากเราไมสามารถจะทำการศกษาแบบ randomized trials ได ดงนน several authors23-29 แนะนำวา ชนดของ prosthetic valve ทจะเปลยนใหคนไขในกลม native valve endocarditis ไมมความ สำคญเทากบการ adequate debridement รวมกบการให appropriate an-tibiotic treatment สวนการเลอกใชmechanical หรอ biological valve ควรพจารณาตาม age, compliance of anticoagulant, life expectancy and co-morbidities โดยสามารถใช bioprosthetic valve ในคนไขอาย มากกวา 60 ปไดหากไมมโรคอนรวมทสงผลทำใหเกด early bioprosthetic valve failure ไดแก Type II diabetes mellitus, high cholesterol levels (>240mg/dl), Atherosclerosis, Metabolic syndrome, Smoking, Chronic Renal failure, Young age30-34
• SurgicalmanagementofnativemitralvalveIE
Concept surgical treatment สำหรบ native mitral valve endocarditis ตองคำนงถง severity of valve และ annular destruction
38
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
โดยหลกการผาตดแลวทำได 2 วธ คอ mitral valve repair หรอ mitral valve replacement กรณถา severity ของโรครนแรง involve annulus และ leaflet เสยหายมากกจำเปนตองเปลยน valve แตถาสามารถ preserve mitral valve apparatus ไดควรทำเนองจากจะสามารถ preserve LV function ไวได
แตถาการตดเชออยแคบรเวณ valvular tissue ควรทตองทำ mitral valve repair เปนอยางยง ถงแมวายงมการกงวลเกยวกบ durability, possibility ของการเกด recurrent infection อนเนองมาจาก incomplete resection หรอการใช prosthetic annuloplasty rings35 เมอเรวๆนมขอมลการศกษา meta-analysis36 พบวา mitral valve repair ม hospital and long-term survival สงกวาการทำ mitral valve replacement รวมทงโอกาศทจะเกด recurrent endocarditis และ reoperation ตำกวาดวย นอกจากนประโยชนทไดรบจากการทำ MV repair ทไดอกคอ better preserve LV function และ ลดอบตการในการเกด prosthetic valve-related complications.35,40 แต repair rate ใน series publish อยในปจจบนประมาณรอยละ 33-94 โดยขนอยกบประสพการณของศลยแพทย และ status of disease (healed or active IE)18 สำหรบการใช prosthetic annuloplasty rings ในคนไขทไดรบการผาตด MV repair พบวาปลอดภย และ low reinfection rate37,39 นอกจากนยงมการรายงานการใช strip of autologous glutaraldehyde-treated pericardium มาแทน38
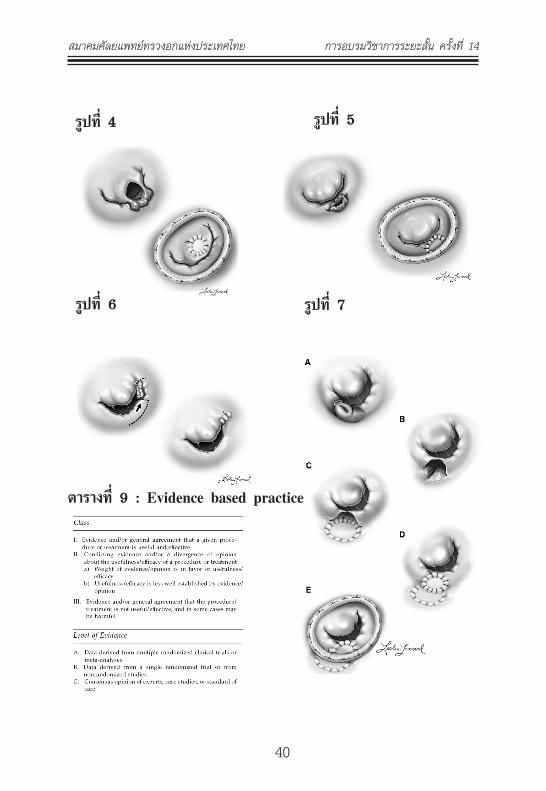
ในกรณถาการตดเชออยทเฉพาะ native mitral valve หรอ annulus ภายหลงจากเรา radical debridement infected and necrotic tissues ออกหมดแลว หากเกดม small defect เราสามารถ direct repair หรอ เยบรวบไปพรอมกบตอนเยบ prosthetic valve (รปท 10) แตถาหาก ม defect ขนาดใหญ อาจจะใช fresh autologous pericardium หรอ glutaraldehyde-fixed pericardium (รปท 4) เพอเยบปดและชวย support suture line บรเวณทเยบ prosthetic valve ได

39
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
Dr. Evans from Maryland40 ได described ลกษณะ IE ทเกดกบ mitral valve ไว 4 pattern (ดงรป4-7) โดย pattern ท 1 พบไดมากทสดคอ มการ perforate ท anterior leaflet และมเนอเยอยนออกมาเหมอน wind sock vegetation ซงเปนชนดทพบไดมากทสด บางครง lesion อาจกวางมากกวารอยละ 50 ของพนท anterior leaflet กสามารถซอมไดโดยใช 0.625 glutaraldehyde-treated autologous pericardium patch และเยบดวย 5-0 monofilament แบบ running และเสรมดวย prosthetic annuloplasty ring (ดงรปท4) สวนชนดทสอง เปน posterior leaflet destruction สามารถทำ resection และ posterior augmentation (ดงรปท 5) สวนชนดทสาม involve commissural part ซงเปน type ทคอนขาง challenge โดย resection สวนนนออก และกรดขยายสวน base ของ posterior leaflet แลวพยายาม advance flap ไปยง commissure (ดงรปท 6) ชนดทสเปนชนดท involve annulus เชน abscess หรอ หลง debridement แลวตดออกหมดแมกระทง annulus type นจำเปนตอง reconstruction atrioventricular groove (AV groove) ขนมาใหมโดยใช fresh autologous pericardium patch โดย desire patch ใหกวางกวา lesion และเยบลกไปจนถง LV free wall ให cover AV groove จนถง posterior left atrial wall โดย 4-0 monofilament running suture หลงจากนนก patch reconstruction valve และเสรมดวย prosthetic annuloplasty ring (ดงรปท7)
40
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
รปท4 รปท5
รปท6 รปท7
ตารางท9:Evidencebasedpractice

41
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
ในกรณทจำเปนจะตองทำ mitral valve replacement เราจะเลอก ใช bioprosthetic valve หรอ mechanical valve มการศกษามากมาย เปรยบเทยบระหวางการใช prosthetic valve ทงสองกลมน สรปวาไมมความ แตกตางกนในเรองของ survival rate and freedom from re-infection23-29 โดย rate ในการเกด recurrent IE ในกลม mechanical valve 2.1% per patient-year และกลม bioprosthetic 2.3 per patient-year24 แตทวา risk of reoperation นนพบไดมากกวาในกลมทใช bioprosthetic valve เนองมาจากการเสอมของ valve เองตามอายทมากขน แตถาหากทำ mitral valve replacement.ในกลมคนไขทอายมากกวา 70 ปขนไป freedom from reoperation ระหวางสองกลมนจะไมแตกตางกน18 กรณถา severity ของโรครนแรง involve annulus และ leaflet เสยหายมากแลวจำเปนตอง เปลยน valve ควรพยายาม preserve mitral valve apparatus ไวเพอ preserve LV function ไว40 (ดงรปท8-11)
รปท8:Smallannularabscesscavities(widelessthan 10mmindiameter)canberepairedwithapericardial buttressingstrip44

42
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
รปท9: Pericardialpatchreconstruction44
รปท10:Largemitralannulardefectscanberepairedbyconstructingapseudoannuluswithacircumferentialpericardialpatch.(fromDavidTE)44

43
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
ในป ค.ศ. 2011 ทางสมาคม Society of Thoracic Surgeons (STS) published clinical practice guideline ออกมาเกยวกบ surgical management of endocarditis ซงขอมลสวนใหญอางองตาม evidence based (ตารางท9)NativeMitralValveEndocarditis(STSClinicalPracticeGuideline2011)
1. When technically feasible, mitral valve repair is recommended to treat native mitral valve endocarditis. (ClassI,LevelofevidenceB)
2. When surgery is indicated, mechanical or stented tissue valves can be useful for mitral valve replacement as appropriate given age, life expectancy, and comorbidities. (ClassIIa,LevelofevidenceB)
• SurgicalmanagementofnativeaorticvalveIE สวน Native aortic valve endocarditis (NAVE) ปญหาทสำคญทเราคำนงถงคอ เมอไหรจะใช aortic homograft โดยสรปไดดงน โดยทวไป NAVE ภายหลงจากทเรา extensive debridement infected and necrotic tissueออกหมดแลว หากยงเหลอ healthy annular tissue เหลออยกสามารถใช mechanical หรอ stented bioprosthetic valve ได ไมจำเปนตองใช homograft (แตแนะนำวาในขณะทเยบถาไมจำเปนไมควรใช pledget เนองจากเปน foreign body อาจทำใหเพม risk ตอการเกด re-infection ได)
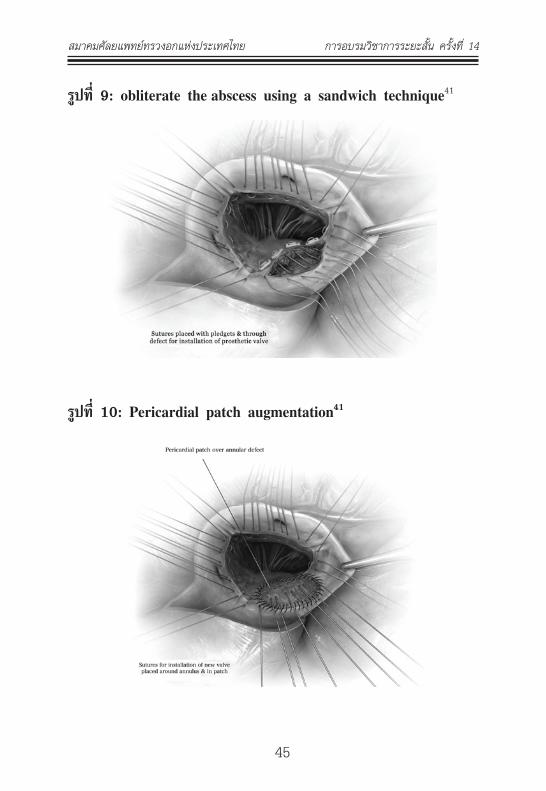
กรณถา lesion extensive to annulus or peri-annular abscess ภายหลงจาก extensive debridement หากเปน small abscess อาจ obliterate ตอนเยบ valve เลยกได41 (ดงรปท8-9) แตถาหาก large

44
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
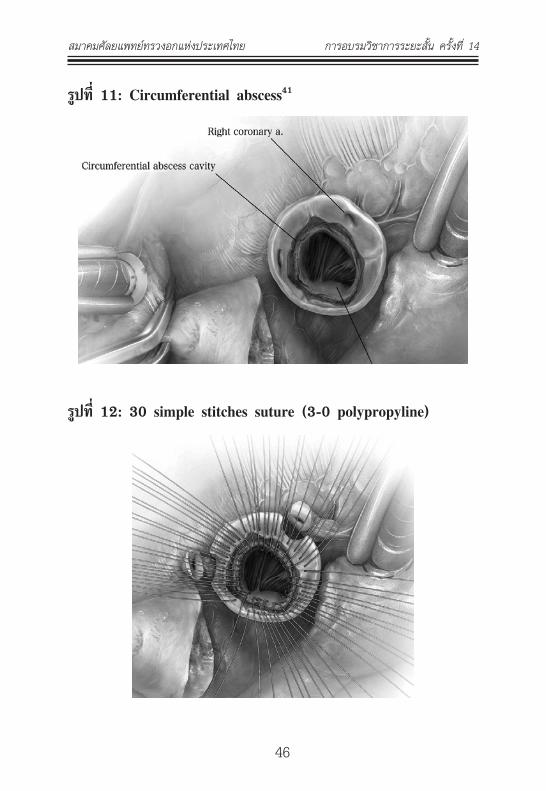
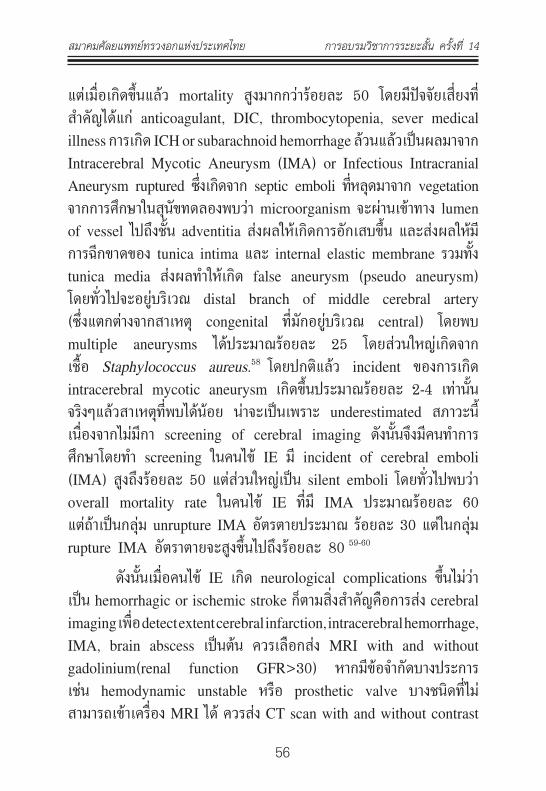
abscess สามารถ repair โดยใช autologous pericardium (ดงรปท10) หรอกรณ circumferential abscess around aortic annulus กสามารถซอมได (ดงรปท11-12) แตในกรณจำเปนตองทำ aortic root replacement กยงแนะนำใหใช composite valve with Dacron graft (Modified Bentall Operation โดยจะเปน mechanical or bioprosthetic ขนกบ age, life expectancy, comorbidities) หากสามารถ debridement ไดหมด แตผเชยวชาญบางทานแนะนำการใช homograft for native aortic valve endocarditis (รปท 13) โดยเฉพาะในกรณ extensive aortic-ventricular discontinuity และประโยชนของ homograft คอ easier to handle และ resistance to infection in early after operation( first 6 weeks)42-43
รปท8:Abscesscavityisidentifiedonremovalofthecusps41
45
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
รปท9:obliteratetheabscessusingasandwichtechnique41
รปท10:Pericardialpatchaugmentation41
46
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
รปท11:Circumferentialabscess41
รปท12:30simplestitchessuture(3-0polypropyline)

47
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
รปท13:Homograftforaorticrootreconstruction
นอกจากนมการศกษาเปรยบเทยบ ระหวางการใช Sentless root replacement กบ homograft41 พบวา การใช homograft ม rate structural failure and reoperation สงกวาชดเจน แตขอมลนไมไดทำการศกษาในคนไข IE แตผเขยนตองการชใหเหนวา ในการเลอกใช homograft นอกจากคำนงถง resistance to infection แลวตองยงคำนงถง long term patency ภายหลงจากทเปลยน homograft ไปแลวดวย โดยเฉพาะ younger patient เปนตน

48
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
NativeAorticValveEndocarditis(STSClinicalPracticeGuideline2011)
1. When surgery is indicated, a mechanical or stented tissue valve is reasonable in native aortic valve endocarditis if the infection is limited to the native aortic valve or to the aortic annulus. Valve choice should be based on age, life expectancy, comorbidities, and compliance with anticoagulation. (ClassIIa,LevelofevidenceB)
2. A homograft may be considered in native aortic valve endocarditis when the infection is limited to the native aortic valve or to the aortic annulus. (ClassIIb,LevelofevidenceB)
Nativeaorticvalveendocarditiswithperiannularabscess(STSClinicalPracticeGuideline2011)
1. When periannular abscess is associated with IE, it is reasonable to use a mechanical or stented tissue valve if radical debridement is carried out and the valve can be anchored to healthy and strong tissue. (ClassIIa,LevelofevidenceB)
2. It may be reasonable to use a homograft in native aor-tic valve endocarditis with periannular abscess and extensive an-nular or aortic wall destruction requiring aortic root replacement/ reconstruction or extensive aortic-ventricular discontinuity. (ClassIIb,LevelofevidenceB)
SurgeryforProstheticValveEndocarditis Prosthetic valve endocarditis (PVE) ภาวะแทรกซอนทรนแรงมากภายหลงการเปลยนลนหวใจ โดยทวไปเกดไดประมาณรอยละ 10-30 โดยเฉลย

49
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
overall incidence 0.1-2.3 % per patient-year หรอพบไดประมาณรอยละ 1.4-3.1 โดยเฉลยทหนงปของการผาตด และพบอกรอยละ 3-5.7 โดย เฉลยทหาปแรกของการรกษา46 ในอดต PVE มอตราตายคอนขางสง ประมาณรอยละ 25-60 แตระยะหลงมการพฒนาเกยวกบเทคนคการรกษา การปองกน IE ทำใหอตราตายลดลงอยางชดเจน ปจจยเสยงททำใหเกด PVE ไดแก type of prosthesis (homograft higher resistance),previous native valve endocarditis, male gender, long CPB, S.aureus.48
PVE แบงออกไดเปน Early กบ late PVE โดยใชระยะเวลาเปนตวแบงท 60 วน แตบาง literature กมการแบงทระยะเวลา 1 ป ลาสด Dr. Karchmer 48แนะนำใหมการแบงออกเปน 3 ชวงเวลา คอ Early (2 months), Transient (2-12 months) and Late (>12 months) ตามลกษณะเชอทพบ โดยเชอทเปนสาเหตสวนใหญททำใหเกด Early PVE คอ เชอในกลม nosocomial infection ไดแก methicillin-resistant Staphylococcus epidermidis, gram-negative bacilli, fungi, and other HACEK group organisms (Haemophilus, Actinobacillus, Cardio-bacterium, Eikinella, Kingella) and fungal infection ดงตารางท10
ตารางท10:MicroorganismCausingPVE48

50
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
ซงสาเหต early PVE มาจาก wound infection, intravascular catheter infection, UTI, pneumonia เปนตน โดยเชอทพบจะเปนเชอทรนแรงและมกจะจำเปนตองรกษาโดยการผาตด แตกรณ Late PVE มกจะเปน เชอจากผวหนง เชอจากการทำฟน ไดแก Streptococcus viridans and Staphylococcus epidermidis. นอกจากนกลไกในการเกด early PVE กบ Late PVE กตางกน โดยพบวาสวนใหญแลว early PVE พยาธสภาพมกไมไดอยท leaflet อยางเดยวเหมอน late PVE บอยครงมกจะ involve sewing ring and annulus สงผลทำใหเกด paravalvular leakage, valve dehisence, paravalvular abscess หรอรนแรงจนเกด fistulous tract ตามมาทำใหเกด worse prognosis ในกลม early PVE มากกวา โอกาศเกด recurrent PVE ประมาณรอยละ 6-1550
โดยปกตแลว mechanical valve ทำมาจาก metal and pyrolyte carbon ซงปองกนการเกาะตดของ microorganism ไดตลอดไป นาน พอๆ กบการปองกนการเกาะตดของ thrombus จงเชอกนวากลไกการเกด infection ใน mechanical valve เกดจาก microorganism มการสราง biofilms ทำใหเกด resistance ตอ antibiotics โดยพบวาสวนใหญการ ตดเชอมกเกดขนทบรเวณ sewing ring หรอ ตรงบรเวณทมการเกาะของ thrombus สงผลทำใหเกด paraprosthetic valve leakage, ring abscess ตามมา โดยพบอบตการณของการเกด myocardial abscess and paravalvular abscess ใน early mechanical PVE ประมาณรอยละ 38 และรอยละ 63 ตามลำดบ โดยพบวา เชอ Staphylococci เปน most common organism ทเปนสาเหตของ paravalvular abscess และสงผลทำใหอตราการตายสงขนอยางชดเจน
สวน bioprosthesis valve นนการตดเชอสวนใหญมกจะ involve เฉพาะ leaflet ทำใหสามารถรกษาดวย antibiotics ได มกไมจำเปนตองรกษาดวยการผาตด และผปวยมกมา present ดวยเรอง Late เนองจาก leaflet degeneration เปนสวนใหญ48

51
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
สำหรบ Mitral Prosthetic Valve Endocarditis เคยมการศกษา IE ป ค.ศ. 1981-1985 โดยศกษา rate of Prosthetic valve endocar-ditis โดยพบวา mechanical prosthetic valve มโอกาศเกด early PVE ไดมากกวา bioprosthetic valve ในชวงหนงปแรก แตหลงจาก 5 ปไปแลว อตราการเกดไมแตกตางกน47 เปนประโยคทอาจจะอานพบไดใน textbooks of cardiology หลายๆเลม แตขอมลในปจจบนพบวา อตราการเกด PVE ไมมความแตกตางกนระหวาง สองกลม18,23-25 ซงอาจจะเกดจากการพฒนาการใหยาปฏชวนะ เทคนคในการผาตด เลยทำใหไมมความแตกตางกน23
Prosthetic Mitral Valve endocarditis (STS Clinical PracticeGuideline2011)
1. When surgery is indicated for prosthetic mitral valve endocarditis, either mechanical or stented tissue valves may be considered for valve replacement. The choice of whether either a tissue or mechanical valve should be implanted should be based primarily on consideration of age, life expectancy, and presence of comorbidities. (ClassIIb,LevelofevidenceC)
สำหรบ Aortic PVE ภายหลงจากการทำ aggressive debridement แลวหากจำเปนจะตองทำ aortic root replacement หรอม severe disruption of anatomy หรอ จำเปนจะตองปดรทะล fistulous tract (VSD) หรอ mitral perforation การใช Aortic homograft ถอวาเปน ideal substitute25,42 แตกรณถาพบพยาธสภาพ involve limited to prosthesis and no annular destruction การใช mechanical or stented tissue valve กสามารถยอมรบได18

52
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
Prosthetic aortic valve endocarditis (STS Clinical PracticeGuideline2011)
1. When surgery is indicated, in patients with aortic PVE limited to the prosthesis without aortic root abscess, and no annular destruction, it is reasonable to implant a mechanical or stented tissue valve. (ClassIIa,LevelofevidenceB)
2. A homograft can be beneficial in aortic PVE when periannular abscess or extensive ventricular-aortic discontinuity is present, or when aortic root replacement/reconstruction is necessary because of annular destruction or destruction of anatomical structures. (ClassIIa,LevelofevidenceB)
SurgeryforIntravenousDrugUsersandRight-SidedEndocarditis
Injection Drug User (IDU) พบไดบอยในคนไขอายนอย โดยทวไป overall incidence IE ในคนไข IDUประมาณรอยละ 1-5 ตอป โดยพบวา tricuspid valve มโอกาศตดเชอไดมากทสดโดยไมม พยาธสภาพท tricuspid valveนำมากอน โดยสดสวนเกด IE ท tricuspid valve ประมาณรอยละ 46-78 รองลงมาคอ mitral valve รอยละ 24-32 ตอมาคอ aortic valve รอยละ 8-1951 อยางไรกตามพบวาแนวโนมการ เกด IE ในกลมคนไข IDU มสดสวนในการเกด left-sided IE สงขน และ เชอทพบไดบอยทสด ทเปนสาเหตคอ S. aureus จากการศกษาพบวา การพยากรณในคนไขกลมนคอนขางด อตราตายตำมาก (mortality < 5%) อนเนองมาจาก สวนใหญเปนในคนอายนอย และมกเกดทางดาน right side heart (ยกเวน ถาคนไขตดเชอ HIV รวมดวย การพยากรณโรคจะ ขน CD4 count) โดยทวไปมกทำการรกษาไดดวยยาปฏชวนะ และการ conservative treatment เปนการรกษาหลกของคนไขกลมน (Right-sided

53
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
endocarditis)พยายามหลกเลยงการผาตดถาไมมขอบงชทชดเจน เพราะ เนองจากวาคนไขกลมน มกม compliance ตอการกนยาไมดถาหากผาตดแลวจำเปนตองเปลยนลนหวใจ จะเกดปญหาตามมาไดมาก52
ขอบงชในการผาตด Fungal IE, persistent (> 3 weeks) or recurrent bacteremia, vegetation larger than 2 cm and severe right side heart failure (failed medication) สวนภาวะ recurrent pulmonary emboli ถอวาไมไดเปนขอบงชในการผาตด เนองมาจากวา Pulmonary septic emboli โดยทวไปเกดขนประมาณรอยละ 66-75 ในกลมคนไขทตดยา53 เมอจำเปนมขอบงชจะตองผาตดจรงๆ การผาตดทถอวาเปน treatment of choice คอ tricuspid valve repair เพราะการเปลยนลนหวใจ tricuspid valve ในคนไข IDU สงทจะตามมาคอ thrombus formation, high rate recurrent IE เนองจากคนไขในกลมน poor medical compliance โดยปกตแลวการผาตด tricuspid valve repair ไมคอยมปญหาเทาไร ยกเวน กรณทพยาธสภาพ involve มากกวา 2 leaflet หรอ lesion เกนครงหนงของ anterior TV leaflet (โดยเฉพาะจาก marginal cords) ในกรณทจำเปนจะตองทำ tricuspid valve replacement จรงๆ สวน ใหญผเชยวชาญมกจะเลอก bioprosthetic valve เนองมาจากคนไขกลมนมก poor compliance ในการกนยา warfarin แตสงทตามมากคอ re-operation rate สงมาก ผเชยวชาญบางทานแนะนำวา ในบางครงคนไขม extensive TV endocarditis มาก การทำ vulvulectomy of TV โดยยงไมใส prosthetic valve กสามารถทำได รอ control infection และแกไขปญหาตดยากอน คอยมาทำ second stage tricuspid valve replacement ทหลง18

54
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
Native tricuspid valve endocarditis (STS Clinical PracticeGuideline2011)
1. When surgery is indicated, tricuspid valve repair is recommended for native tricuspidvalve endocarditis. (Class I,LevelofevidenceB) 2. Mechanical or stented tissue valves can be useful in native tricuspid valve endocarditis, if the valve cannot be repaired. (ClassIIa,LevelofevidenceC)
Surgery for Systemic Septic Embolism and NeurologicalComplications
Systemic embolization จาก IE เปนภาวะแทรกซอนทพบ บอยอนดบสองรองมาจาก congestive heart failure Ischemic stroke เปน systemic embolism complication ทพบไดบอยทสด พบได ประมาณรอยละ 20 ของคนไข IE โดยสวนใหญเกดจาก vegetation ท mitral valve มากกวาท aortic valve54,55 จากการศกษาวา อตราการ เกด systemic emboli จะลดลงอยางชดเจนภายหลงจากไดเรมการรกษาดวยยาปฏชวนะทเหมาะสม (13 events per 1000 patient-days in the first week to less than 1.2 events per 1000 patient-days after second week of treatment)56 โดยพบวา cerebral embolism สวนใหญเกดท Cerebral or cerebellar cortex ประมาณรอยละ 60-9018 คนไขสวนใหญมกมอาการ decrease level of conciousness, seizure แตสงทนาสะพรงกลวมากทสดคอ อตราการเกด hemorrhagic transformation สงสดถงรอยละ 50 ดงนน ACC/AHA guideline8
จงแนะนำใหคนไข IE ทม neurological events ใหหยดยา anticoagulant ในชวง 2 สปดาหแรกของการเรมรกษา เนองมาจากอตราในการเกด re- cerebral emboli กบ hemorrhagic transformation คอนขางสง (โอกาศท

55
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
septic emboli จะทำใหเกด brain abscess นอยมาก) แตถาหากม ความจำเปนตองใช anticoagulant เชน prosthetic valve endocarditis ใหเปลยนไปใช unfractionated heparin แทน18 ในกรณนเปนปญหา ทสำคญ ทถกเถยงกนมานานวาเมอไหรเปนเวลาทเหมาะสมในการทจะนำ ผปวยไปผาตด valve surgery ภายหลงจากทผปวยมอาการ neurological complications เพราะการผาตดหวใจตองใชเครอง heart-lung machine ตองใช heparinในขณะผาตดจะสงผลทำใหคนไขแยลงจาก hemorrhagic transformation หรอไม และอาจจะทำใหคนไขแยลงจาก decrease cerebral perfusion ในขณะผาตดกเปนได นอกจากน ยงพบวาคนไขกลมนมกม clinical congestive heart failure รวมดวยถาทงไวนานรอให neurological complication improve กอาจทำใหคนไขเสยชวตจากหวใจได ไดมการ รายงานในป ค.ศ. 200457 พบวา ภายหลงจากการเกด cerebral in-farction ความเสยงทจะทำให neurological condition แยลงอนเนอง มาจากการผาตดหวใจนน ความเสยงจะลดลงอยางชดเจนภายหลง 1 เดอนไปแลว (After brain infarction this risk is 20% within three days, 20-50% between day 4 and 14, but declines to < 10% after 14 days and < 1% after 4 weeks) ดงนนจงเปนทมาวา คนไขทจำเปน ตองเขารบการรกษาโดยการผาตดหวใจ แตมปญหา ischemic stroke หากไมมภาวะแทรกซอนอนๆทตองรบผาตดใหรออยางนอย 1 เดอน จาก ขอมลดงกลาว57 ผเขยนรายงานฉบบนไดสรปวาสามารถทำการผาตดผปวย ไดภายใน 3 วนแรกไดในกรณทคนไขเปน small infarct, transient ischemic attack, silent infarct แตโดยสวนตวผเขยนไมเหนดวย เพราะความเสยงใน ชวงสามวนแรกกยงคงมากอยถงรอยละ 20 จากขอมลดงกลาวม authority บางทานแนะนำวาในกรณทผปวยมสภาวะ moderate to severe congestive heart failure รวมกบม ischemic stroke รวมดวยอาจรอเพยงแคสอง สปดาหกเพยงพอทจะนำผปวยเขารบการผาตด18
Intracerebral hemorrhage(ICH) เปน neurological complication ทพบไดบอยเปนอนดบสอง (15% of neurological complications)
56
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
แตเมอเกดขนแลว mortality สงมากกวารอยละ 50 โดยมปจจยเสยงท สำคญไดแก anticoagulant, DIC, thrombocytopenia, sever medical illness การเกด ICH or subarachnoid hemorrhage ลวนแลวเปนผลมาจาก Intracerebral Mycotic Aneurysm (IMA) or Infectious Intracranial Aneurysm ruptured ซงเกดจาก septic emboli ทหลดมาจาก vegetation จากการศกษาในสนขทดลองพบวา microorganism จะผานเขาทาง lumen of vessel ไปถงชน adventitia สงผลใหเกดการอกเสบขน และสงผลใหม การฉกขาดของ tunica intima และ internal elastic membrane รวมทง tunica media สงผลทำใหเกด false aneurysm (pseudo aneurysm) โดยทวไปจะอยบรเวณ distal branch of middle cerebral artery (ซงแตกตางจากสาเหต congenital ทมกอยบรเวณ central) โดยพบ multiple aneurysms ไดประมาณรอยละ 25 โดยสวนใหญเกดจาก เชอ Staphylococcus aureus.58 โดยปกตแลว incident ของการเกด intracerebral mycotic aneurysm เกดขนประมาณรอยละ 2-4 เทานน จรงๆแลวสาเหตทพบไดนอย นาจะเปนเพราะ underestimated สภาวะน เนองจากไมมกา screening of cerebral imaging ดงนนจงมคนทำการศกษาโดยทำ screening ในคนไข IE ม incident of cerebral emboli (IMA) สงถงรอยละ 50 แตสวนใหญเปน silent emboli โดยทวไปพบวา overall mortality rate ในคนไข IE ทม IMA ประมาณรอยละ 60 แตถาเปนกลม unrupture IMA อตรตายประมาณ รอยละ 30 แตในกลม rupture IMA อตราตายจะสงขนไปถงรอยละ 80 59-60
ดงนนเมอคนไข IE เกด neurological complications ขนไมวา เปน hemorrhagic or ischemic stroke กตามสงสำคญคอการสง cerebral imaging เพอ detect extent cerebral infarction, intracerebral hemorrhage, IMA, brain abscess เปนตน ควรเลอกสง MRI with and without gadolinium(renal function GFR>30) หากมขอจำกดบางประการ เชน hemodynamic unstable หรอ prosthetic valve บางชนดทไม สามารถเขาเครอง MRI ได ควรสง CT scan with and without contrast

57
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
แทน สาเหตทเลอกสง MRI เปนอนดบแรกเพราะ MRI สามารถ detect พยาธสภาพไดมากกวา CT ดงนนหากทำ CT ไมพบความผดปกต ไมสามารถ rule out ได (รปท 14) แตในกรณทตองการ screening test Intracerebral Mycotic Aneurysm (IMA) ในคนไข IE สามารถทำ CTA18 (รปท 15) หรอ MRA ได ซงคำแนะนำดงกลาวตรงกนขามกบ ACC/AHA guideline8 โดยทาง AHA ไมแนะนำการทำ screening ในคนไข asymp-tomatic IMA อยางไรกตามทาง Society of Thoracic Surgery (STS)18 ใหเหตผลวา การผาตดหวใจจำเปนตอง on heparin ซงแนนอนในกรณ unrupture IMA คนไขไมมอาการแนนอน แตถาหากไปผาตดแลวคนไข เกดแตกออกขณะ on heparin จะเกด devastating ICH complications จนคนไขอาจเสยชวตไดจงแนะนำใหทำ screening test ในคนไข IE ท absence clinical sign of embolism สำหรบผเขยนเหนวา การ screening test กดแตตองทำในคนไข IE ทกคนเลยหรอ นาทจะเลอกเปนรายๆ ไป โดยม criteria สำหรบคนไข HighriskforIMA ดงน (1) previous neurological evemts (2) microorganism especially S.aureus (3) Large vegetation > 1 cm. (4) mitral valve lesion ทางผเขยนจง ไดสรปเปน Algorithm ดงรปท16และนอกจากนไมควรสง catheter angiography เปน routine แตสงในกรณทจะทำ intervention for treatment IMA (endovascular treatment)

58
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
รปท14: T2*-weighted MRI sequences to the detection of microbleeds in the setting of infectious endocarditis. Left thalamic and right posterior parietal subacute hematomas (black arrows) and multiple asymptomatic microbleeds (white arrows)60
รปท15:IMAduetosepticembolifromIE

59
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14

60
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
NeurologicComplicationsinEndocarditis(STSClinicalPracticeGuideline2011)
A)Radiographicevaluationofpatientswithstrokeandendocarditis
1. Brain imaging is required if there is suspicion of stroke in the setting of endocarditis. Either magnetic resonance imaging (MRI) or computed tomography (CT) is an acceptable initial study. (ClassI,LevelofevidenceB)
2. If MRI is chosen, diffusion weighted imaging, FLAIR imaging, gradient echo imaging, and a postcontrast study, should be performed. (ClassI,LevelofevidenceB)
3. If MRI is not feasible, CT should be performed. (ClassI,LevelofevidenceB)
4. Vascular imaging should be performed contemporaneously with brain imaging. Magnetic resonance angiography (MRA) and computed tomography angiography (CTA) are both acceptable vascular imaging modalities to screen for mycotic aneurysm in patients without evidence of intracranial hemorrhage. (ClassI,LevelofevidenceC)
5. It is reasonable to reserve catheter angiography for patients with evidence of intracranial bleeding, or noninvasive vascular imaging suggestive of mycotic aneurysm. (Class IIa,LevelofevidenceC)
B) Timing of surgery in patients with neurologiccomplications
61
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
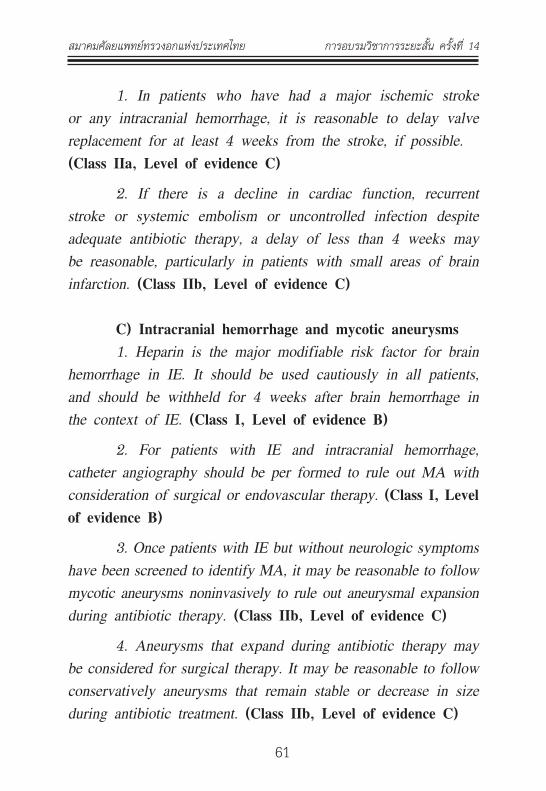
1. In patients who have had a major ischemic stroke or any intracranial hemorrhage, it is reasonable to delay valve replacement for at least 4 weeks from the stroke, if possible. (ClassIIa,LevelofevidenceC)
2. If there is a decline in cardiac function, recurrent stroke or systemic embolism or uncontrolled infection despite adequate antibiotic therapy, a delay of less than 4 weeks may be reasonable, particularly in patients with small areas of brain infarction. (ClassIIb,LevelofevidenceC)
C)Intracranialhemorrhageandmycoticaneurysms 1. Heparin is the major modifiable risk factor for brain hemorrhage in IE. It should be used cautiously in all patients, and should be withheld for 4 weeks after brain hemorrhage in the context of IE. (ClassI,LevelofevidenceB)
2. For patients with IE and intracranial hemorrhage, catheter angiography should be per formed to rule out MA with consideration of surgical or endovascular therapy. (ClassI,LevelofevidenceB)
3. Once patients with IE but without neurologic symptoms have been screened to identify MA, it may be reasonable to follow mycotic aneurysms noninvasively to rule out aneurysmal expansion during antibiotic therapy. (ClassIIb,Levelof evidenceC)
4. Aneurysms that expand during antibiotic therapy may be considered for surgical therapy. It may be reasonable to follow conservatively aneurysms that remain stable or decrease in size during antibiotic treatment. (ClassIIb, LevelofevidenceC)

62
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
นอกจากน complication of systemic emboli ยงทำใหเกด splenic infarction ไดซงจะเหนเปน wedge area, multiple lesion ซงตรงขามกบการเกด splenic abscess ซงมกเปนจดเดยวและม ring enhancement ซงเปนสาเหตททำใหเกด persistent fever ในคนไข IE ได สวนการรกษา multivlvular endocarditis กคงใชหลกการเดยวกนกบ recommendation ใน valve แตละชนด นอกจากวธการรกษาทกลาวมาขาง ตนแลวนนยงมการผาตดโดยวธอนไดอก เชนกรณ คนไขเดก เปน extensive infection aortic prosthetic valve endocarditis จะหาลนหวใจแบบ ไหนทเหมาะสมมาแทน literture กลาวถงการทำ Ross Operation ใน คนไขกลมน หรอในกรณคนไข IE บางคนม recurrent IE third or fourth episode ของการรกษา prosthetic valve endocarditis or recurrent multiple PVE การผาตดเปลยนลนหวใจซำอาจไมสามารถกำจดเชอ ออกไปไดหมด ดงนนในคนไขกลมนเราสามารถรกษาไดโดยการทำ heart transplantation
การดแลผปวยภายหลงการผาตดกมความสำคญ ตาม European guideline61 ไดแนะนำเกยวกบการใหยา antibiotic ในการรกษา IE โดย ใหนาน 6 weeks โดยไมคำนงถงวาผาตดเมอไหร แตในทางปฏบตแลวสวนมากเราเรมนบใหมภายหลงการผาตด ตามหลกเหตผลทวาเราเพงกำจดเชอออกไป หรอแมแตผลเพาะเชอจากลนเนอเยอทสงตรวจไปเพาะขนเชอ เราจะทำยงไงตองเรมใหมอก 6 สปดาหไหม ตาม guideline แนะนำวาใหครบ 6 สปดาห โดยไมตองนบหนงใหม ยกเวนบางกรณทคนไขมาทำผาตด elective ภายหลงให antibiotic ครบ 6 สปดาหแลวสง hemoculture ยงขนเชออยอาจตอง discussion กบทาง infectious วาอาจจะตองให antibiotic ตอไปใหมอก 6 สปดาหภายหลงจากการผาตด นอกจากนการปองกนกมความสำคญในการลด incident prosthetic valve endocarditis ดงนนควรใหการศกษาผปวยเกยวกบ IE prophylaxis รวมทงแนะนำและ เนนยำแกบคลากรทางการแพทย รวมทงแพทยเวชศาสตรครอบครวดวย15

63
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
References1. Moreillon P, Que YA. Infective endocarditis. Lancet 2004;
363:139-149.
2. StuesseD.C.,VlessisA.A, et al.Epidemiology of nativevalveendocarditis:AMultidisciplinaryApproach toModernTreatment,Armonk,NY:FuturaPublishing;1999:77-84.
3. Orathai Pachirat, Songsak Kiatchoosakun, PloenchanChetchotisakd, et al. Effect of Changes in Diagnosis andManagementofActiveInfectiveEndocarditisontheClinicalOutcome at Srinagarind Hospital. J MedAssoc Thai 2005;88(4):498-504.
4. Romanee Chaiwarith, Somboon Jeenapongsa, ThiraSirisanthana.InfectiveEndocarditisatMaharajNakornChiangMai Hospital, 2002-2003. J Infect Dis Antimicrob Agents2006;23:75-81.
5. Somporn Srifuengfung, Thitiya Yungyuen and PodjaneeKomolpis.Bacterialisolationandantimicrobialsusceptibilitiesinpatientswithinfectiveendocarditis.SoutheastAsianJTropMedPublicHealth2004;35(4):897-901.
6. Pornthep Lertsapcharoen, Apichai Khongphatthanayothin,Pairoj Chotivittayatarakorn, et al. Infective Endocarditis inPediatric Patients:An Eighteen-Year Experience from KingChulalongkornMemorialHospital. JMedAssocThai2005;88(Suppl4):S12-6.
7. Levy D, Centenary of William Osler’s 1885 GulstonianLecturesandtheirplaceinthehistoryofbacterialendocarditis.JRSocMed.1985;78:1039-1046.

64
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
8. LarryM.Baddour,WalterR.Wilson,ArnoldS.Bayer,etal.InfectiveEndocarditis:Diagnosis,AntimicrobialTherapy,andManagementofComplications.Circulation2005;111:e394-e433.
9. Hasbun R, Vikram HR, Barakat LA, et al. Complicatedleft-sided native valve endocarditis in adults: Risk classification formortality.JAMA2003;289:1933-1940.
10. López J, Revilla A, Vilacosta I, et al. Age-dependent profile of left-sided infective endocarditis: A 3-center experience.Circulation2010;121:892-897.
11. RobertO.Bonow,BlaseA.Carabello,KanuChatterjee,etal.2008FocusedUpdateIncorporatedIntotheACC/AHA2006Guidelines for the Management of Patients With ValvularHeartDisease.J.Am.Coll.Cardiol.2008;52;e1-e142.
12. Gilbert Habib, Bruno Hoen, Pilar Tornos, et al. Guidelineson the prevention, diagnosis and treatment of infectiveendocarditis.EuropeanHeartJournal2009;30:2369–2413.
13. Stuart J Head, M Mostafa Mokhles, Ruben LJ Osnabrugge,et al. Surgery in current therapy for infective endocarditis.VascularHealthandRiskManagement2011;7:255–263.
14. Thomas M. Bashore, Christopher Cabell, Vance Fowler.Update on Infective Endocarditis. Curr Probl Cardiol 2006;31:274-352.
15. Bernard D. Prendergast, Pilar Tornos. Surgery for InfectiveEndocarditis Who and When? Circulation 2010; 121:1141-1152.
16. RhysPBeynon,VKBahl,BernardDPrendergast.Clinical

65
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
review:InfectiveEndocarditis.BMJ2006;333:334–339.
17. PilarTornos,TeresaGonzalez-Alujas,FrankThuny.InfectiveEndocarditis: The European Viewpoint. Curr Probl Cardiol2011;36:175-222.
18. John G. Byrne, Katayoun Rezai, Juan A. Sanchez, et al.SurgicalManagementofEndocarditis:TheSocietyofThoracicSurgeonsClinicalPracticeGuideline.AnnThoracSurg2011;91:2012–9.
19. PrendergastBD.Thechangingfaceofinfectiveendocarditis.Heart2006;92:879–885.
20. MurdochDR,CoreyGC,HoenB,etal.Investigators.Clinicalpresentation,etiology,andoutcomeof infectiveendocarditisin the 21st century: the International Collaboration onEndocarditis-Prospective Cohort Study. Arch Intern Med2009;169:463–473.
21. HasbunR,VikramHR,BarakatLA,etal.Complicatedleft-sided native valve endocarditis in adults: risk classification for mortality.JAMA2003;289(15):1933-40.
22. ChuV, CabellC, BenjaminD, et al. Early predictors of in-hospitaldeathininfectiveendocarditis.Circulation2004;109:1745-1759.
23. DavidTE,GavraG, FeindelCM, RegestaT, el al. Surgicaltreatment of active infective endocarditis: a continuedchallenge.JThoracCardiovascSurg2007;133:144–9.
24. Moon MR, Miller DC, Moore KA, et al. Treatment ofendocarditis with valve replacement: the question of tissue

66
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
versusmechanicalprosthesis.AnnThoracSurg2001;71:1164–71.
25. DelayD,PellerinM,CarrierM, et al. Immediate and long-term results of valve replacement for native and prostheticvalveendocarditis.AnnThoracSurg2000;70:1219–23.
26. Kaiser SP, Melby SJ, Zierer A, et al. Long-term outcomesinvalve replacement surgery for infectiveendocarditis.AnnThoracSurg2007;83:30–5.
27. TugtekinSM,AlexiouK,WilbringM,etal.Nativeinfectiveendocarditis: which determinants of outcome remain aftersurgicaltreatment?ClinResCardiol2006;95:72–9.
28. Aagaard J, Andersen PV. Acute endocarditis treated withradicaldebridementandimplantationofmechanicalorstentedbioprostheticdevices.AnnThoracSurg2001;71:100–4.
29. Alexiou C, Langley SM, Stafford H, Haw MP, LiveseySA, Monro JL. Surgical treatment of infective mitral valveendocarditis: predictors of early and late outcome. J HeartValveDis2000;9:327–34.
30. LorussoR,GelsominoS,LucáF,etal.TypeIIdiabetesmellitusisassociatedwithfasterdegenerationofbioprostheticvalve:Results from a propensity score-matched Italian multicenterstudy.Circulation2011;on-linepublicationavailable.
31. BriandM,Pibarot P,Despres JP, et al.Metabolic syndromeisassociatedwithfasterdegenerationofbioprostheticvalves.Circulation2006;114:I-512-I-517.
32. Nollert G, Miksch J, Kreuzer E, et al. Risk factors for

67
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
atherosclerosisandthedegenerationfopericardialvalvesafteraorticvalvereplacement.JThoracCardiovascSurg2003;126:965-68.
33. FarivarRS,CohnLH.Hypercholesterolemia is a risk factorfor bioprosthetic valve calcification and explantation. J Thorac CardiovascSurg2003;126:969-75.
34. FlamengW,HerregodsM,VercalsterenM,etal.Prosthesispatientmismatchpredictsstructuralvalvedegenerationinbioprostheticheartvalves.Circulation2010;121:2123-29.
35. Ruttmann E, Legit C, Poelzl G, et al. Mitral valve repairprovides improved outcome over replacement in activeinfectiveendocarditis. JThoracCardiovascSurg2005;130:765–71.
36. Feringa HH, Shaw LJ, Poldermans D, et al. Mitral valverepairandreplacementinendocarditis:asystematicreviewofliterature.AnnThoracSurg2007;83:564–570.
37. de Kerchove L, Vanoverschelde JL, Poncelet A, et al.Reconstructive surgery in active mitral valve endocarditis:feasibility, safety and durability. Eur J Cardiothorac Surg2007;31:592–9.
38. DoukasG,OcM,AlexiouC,SosnowskiAW,SamaniNJ,SpytTJ. Mitral valve repair for active culture positive infectiveendocarditis.Heart2006;92:361–363.
39. Ruttmann E, Legit C, Poelzl G, et al. Mitral valve repairprovides improved outcome over replacement in activeinfectiveendocarditis. JThoracCardiovascSurg2005;130:765–71.

68
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
40. Charles F. Evans, James S. Gammie. Surgical ManagementofMitralValveInfectiveEndocarditis.SeminThoracicSurg2011;23:232-240.
41. John S. Ikonomidis. Surgery forAortic Valve Endocarditis.Operative technique in thoracic and cardiovascular surgery2011;16(3):226-241.
42. Grinda JM, Mainardi JL, D’Attellis N, et al. Cryopreservedaortic viable homograft for active aortic endocarditis. AnnThoracSurg2005;79:767–71.
43. YankahAC,KloseH,PetzinaR,MusciM,SiniawskiH,HetzerR.Surgicalmanagementofacuteaorticrootendocarditiswithviablehomograft:13-yearexperience.EurJCardiothoracSurg2002;21:260–7.
44. Marc R. Moon, Edward B. Stinson, and D. Craig Miller. SurgicalTreatmentofEndocarditis.ProgressinCardiovascularDiseases1997;40(3):239-264.
45. El-Hamamsy I, Clark L, Stevens LM, et al. Late outcomesfollowingFreestyleversushomograftaorticrootreplacement:resultsfromaprospectiverandomizedtrial.JAmCollCardiol2010;55:368–76.
46. CalderwoodSB,SwinskiL,WaternauxC,etal.Riskfactorsforthedevelopmentofprostheticvalveendocarditis.Circulation2002;72(1):31-7.
47. ArvayA,LengyelM. Incidenceandrisk factorsofprostheticvalveendocarditis.EurJCardiothoracSurg.1988;2(5):340-6.
48. Balakrishnan Mahesh, Gianni Angelini, Massimo Caputo.

69
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
Prosthetic Valve Endocarditis. Ann Thorac Surg 2005; 80:1151–8.
49. KarchmerA.Infectionsofprostheticvalvesandintravasculardevices. In: Mandell GL, Bennett JE, Dolin R, editors.Principles and Practice of Infectious Disease. New York:ChurchillLivingstone,2000.907-17.
50. LytleBW,SabikJF,BlackstoneEH,SvenssonLG,PetterssonGB, Cosgrove DM. Reoperative cryopreserved root andascendingaortareplacementforacuteaorticprostheticvalveendocarditis.AnnThoracSurg2002;74(Suppl):1754–9.
51. Miró JM, del RíoA, Mestres CA. Infective endocarditis inintravenousdrugabusersandHIV-1 infectedpatients. InfectDisClinNorthAm.2002;16:273–295.
52. WilsonLE,ThomasDL,AstemborskiJ,FreedmanTL,VlahovD.Prospectivestudyofinfectiveendocarditisamonginjectiondrugusers.JInfectDis.2002;185:1761–1766.
53. Musci M, Siniawski H, Pasic M, et al. Surgical treatmentof right-sided active infective endocarditis with or withoutinvolvementoftheleftheart:20yearsinglecenterexperience.Eur J Cardiothorac Surg.2007;32:118–125.
54. Anderson DJ, Goldstein LB, Wilkinson WE, et al. Strokelocation,characterization,severity,andoutcomeinmitralvsaorticvalveendocarditis.Neurology2003;61(10):1341-6.
55. CabellCH,PondKK,PetersonGE,etal.Theriskofstrokeanddeathinpatientswithaorticandmitralvalveendocarditis.AmHeartJ2001;142(1):75-80.

70
สมาคมศลยแพทยทรวงอกแหงประเทศไทย การอบรมวชาการระยะสน ครงท 14
56. MathewJ,AddaiT,AnandA,etal.Clinicalfeatures,siteofinvolvement, bacteriologic findings, and outcome of infective endocarditis in intravenous drug users. Arch Intern Med1995;155(15):1641-8.
57. Angstwurm K, Borges A, Halle E,et al. Timing the valvereplacement in infective endocarditis involving the brain. JNeurol2004;251:1220–6.
58. PhilipJPeters,TaylorHarrison,JeffreyLLennox.Adangerousdilemma: management of infectious intracranial aneurysmscomplicating endocarditis. Lancet Infect Dis 2006; 6: 742–48.
59. Gammie JS, O’Brien SM, Griffith BP, Peterson ED. Surgical treatmentofmitralvalveendocarditisinNorthAmerica.AnnThoracSurg2005;80:2199–204.
60. LaurentDerex.EricBonnefoy.Franc¸oisDelahaye.Impactofstrokeontherapeuticdecisionmakingininfectiveendocarditis.JNeurol2010;257:315–321.





























