Embed Size (px)
Citation preview

Support Services for Family NeedsSupport Services for Family NeedsTheme: Improving health care: from Theme: Improving health care: from fragmentation to integration.fragmentation to integration.
Dr CheahYee ChuangMBBS (Malaya)M. Med. (Psy.) UKMM. Sc. (Psy.) UNSW Australia
Deinstitutionalization, 1950sDeinstitutionalization, 1950s Care for persons with serious mental illness
(SMI) shifted from custodial to community settings
Individuals with SMI require treatment, rehabilitation and support to function in the community
These services (e.g. medical, social services, housing, etc.) are provided by different agencies
A mechanism is needed to integrate and coordinate this care.

Two organizational mechanisms Two organizational mechanisms evolved in 1970s to address these: evolved in 1970s to address these:
1. Case management: coordination and brokerage of services
2. Assertive community treatment (ACT): integrate services through a direct provision of treatment, rehabilitation and support services by a multidisciplinary team
HospitalHospital--based Community based Community Psychiatric ServicesPsychiatric Services
Provides acute home care, assertive home care, and follow-up of difficult cases.
Include elements of psycho-education, family-based intervention, work-based intervention and illness self management skills.
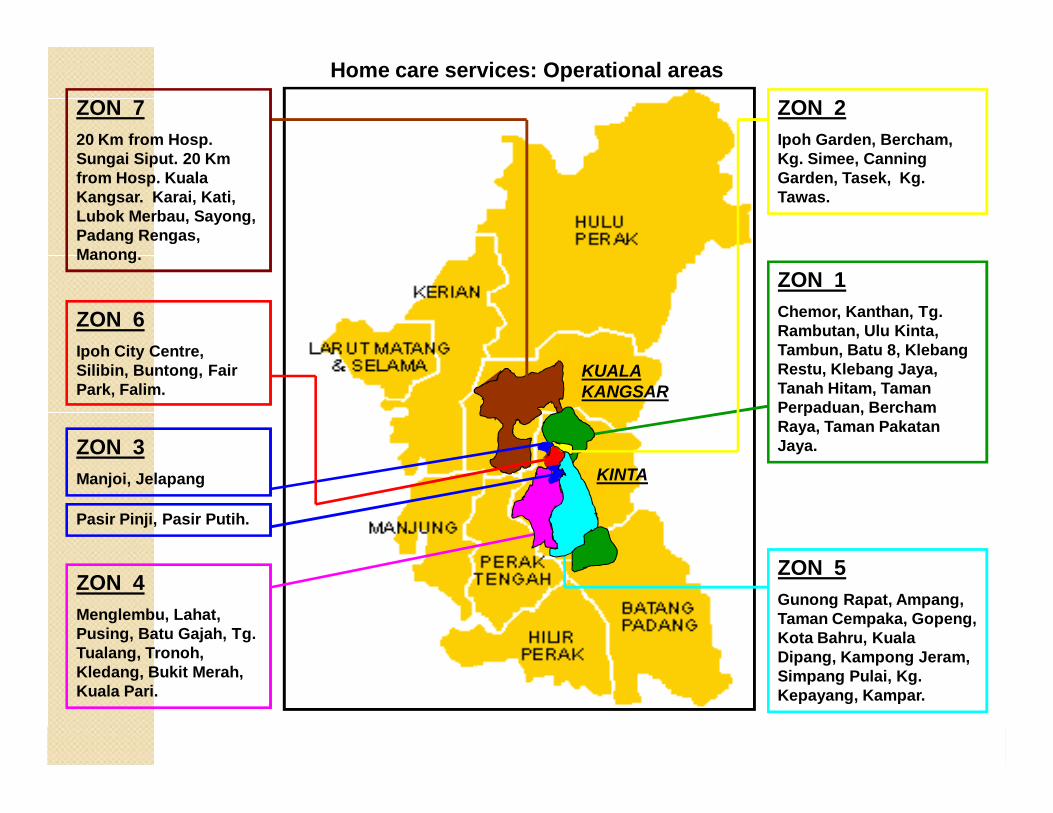
ZON 720 Km from Hosp. Sungai Siput. 20 Km from Hosp. Kuala Kangsar. Karai, Kati, Lubok Merbau, Sayong, Padang Rengas, Manong.
ZON 3Manjoi, Jelapang
ZON 4Menglembu, Lahat, Pusing, Batu Gajah, Tg. Tualang, Tronoh, Kledang, Bukit Merah, Kuala Pari.
ZON 1Chemor, Kanthan, Tg. Rambutan, Ulu Kinta, Tambun, Batu 8, Klebang Restu, Klebang Jaya, Tanah Hitam, Taman Perpaduan, Bercham Raya, Taman Pakatan Jaya.
ZON 2Ipoh Garden, Bercham, Kg. Simee, Canning Garden, Tasek, Kg. Tawas.
ZON 6Ipoh City Centre, Silibin, Buntong, Fair Park, Falim.
ZON 5Gunong Rapat, Ampang, Taman Cempaka, Gopeng, Kota Bahru, Kuala Dipang, Kampong Jeram, Simpang Pulai, Kg. Kepayang, Kampar.
Home care services: Operational areas
Pasir Pinji, Pasir Putih.
KUALA KANGSAR
KINTA

Acute Treatment:Acute Treatment: Offer an alternative to hospitalization Prevent harm by risk assessment & risk management Develop alliance with patient and family Prompt treatment to control disturbed behavior &
suppress symptoms Connect family and patients with follow up resources Psycho education Multidisciplinary approach

Assertive community treatment Assertive community treatment (ACT)(ACT)
Dealing with severe mental illness with severe mental illness with complex needscomplex needs
Schizophrenia, mood disorder, organic disorder, with
Disability Unable to care for self independently Cannot sustain relationships Symptoms – current or enduring Recurrent crises and frequent admissions Significant risk to self and others

Needs of People with Mental DisordersNeeds of People with Mental Disorders
©2001

Adapted from Weiden et al, J Clin Psych 1996; 57: 53-60
Response
Remission
Recovery
Functionality : New Goal in TreatmentFunctionality : New Goal in Treatment
Impact of mental illness on familyImpact of mental illness on family Family members are bonded physically and
emotionally Burden of care:◦ Objective burden◦ Subjective burden
Family require appropriate and sufficient education , training and emotional support for their care-giving role.
Burden of care: Objective burdenBurden of care: Objective burden
Behavioural disturbances with disruptive effects on family life and household routines Excessive smoking Poor personal hygiene Damage to household property Sleep reversal pattern that may keep household awake Assaultative or abusive behaviour Socially offensive or embarrassing behaviour Mood swings and unpredictability Negative symptoms of amotivation or anhedonia
Burden of care: Objective burdenBurden of care: Objective burden
Patient’s rejection of medications Time and energy in supporting patient to get
treatment and adhere to medications Social isolation Financial cost of the illness and economic strain
Burden of care: Subjective burdenBurden of care: Subjective burden
Emotional costs associated with each objective burden
Grief unfulfilled life expectations for the pre-morbid personality failed aspirations of someone they love
Feelings of stigmatization Worries of ageing parents about the future of
the mentally child who will surely outlive them
Families’ effects on patientsFamilies’ effects on patients High expressed emotion (EE) in families
(Vaughn and Leff1 ) Hostile criticism or emotional over-involvement Predictive of a greater tendency to relapse in
schizophrenia
In Vaughn’s unpublished thesis, the better clinical outcome associated with supportive comments and emotional warmth expressed by relatives towards the patient2.
1. Vaughn C. Leff J. The influence of family and social factors on the course of psychiatric illness. A comparison of schizophrenic and depressed neurotic patients. Br J Psychiatry. 1976;129:125–137.2. Falloon IRH. Expressed emotion: current status. Psychol Med. 1988;18:269–274.

Cochrane Systematic Review on Family Cochrane Systematic Review on Family Intervention Intervention ((PharoahPharoah F et. al, 2007, Level 1)F et. al, 2007, Level 1)
Improved compliance with medication (NNT 7) Decrease relapse rates (NNT 8), Reduced hospital admission (NNT 8) Other outcomes:
• Less negative EE• Reduced feeling of blame• Greater adaptability• Better intra-family communication
Clinical practice guidelines: Management of Schizophrenia in adults (2009)
Family intervention is an integral part in the psychosocial management of schizophrenia
It aims to improve family atmosphere and functioning, provide emotional support to family members and help with limits setting.
Recommends that family intervention should be make available to all families of people with schizophrenia (Grade A).
http://www.moh.gov.myhttp://www.acadmed.org.myhttp://www.psychiatry-malaysia.org

GarispanduanGarispanduan program program intervensiintervensi keluargakeluargabagibagi pesakitpesakit mental (2001), mental (2001), KementerianKementerianKesihatanKesihatan MalaysiaMalaysia..
Family intervention program (FIP) refers to helping the family members to cope better with a sick member who is suffering from a mental illness.
The family member is taken as an ally in treating the mentally ill.
Family Intervention programFamily Intervention program
EngagementEngagementEnlist family members in active management of patients, Build on the strength available in the family
Communication TrainingCommunication Training EducationEducation Problem solvingProblem solving
Engagement:Engagement:
1. Carers: Who will hold and supervise medications? Who will bring patient for follow-up?
2. Patient: Agree that carer will supervise medication, and attend follow-up.

In Malaysia, a psychoeducational package is available in five training modules covering aspects of illness, treatment and side effects of medications, role of the family, maintaining wellness and managing crisis.
FIP: 2. Psychoeducation
BehaviouralBehavioural tailoringtailoring
Is helping consumers fit taking medication into daily routines by building in natural reminders, which improve medication adherence and can prevent relapses and rehospitalization.
Illness management
Relapse prevention trainingRelapse prevention training
teaching consumers how to recognize situations that trigger relapses and the warning signs of a relapse
developing a plan for responding to those signs
MengenaliMengenali tandatanda--tandatanda amaranamaran awalawalpenyakitpenyakit ahliahli keluargakeluarga andaanda....
Tanda amaran awal adalah:1._________________2. _________________3.__________________
Jika saya melihat tanda-tanda ini, saya akanmenghubungi_________________, no. talipon________________.

ModulKemahiranKesihatan
Mental
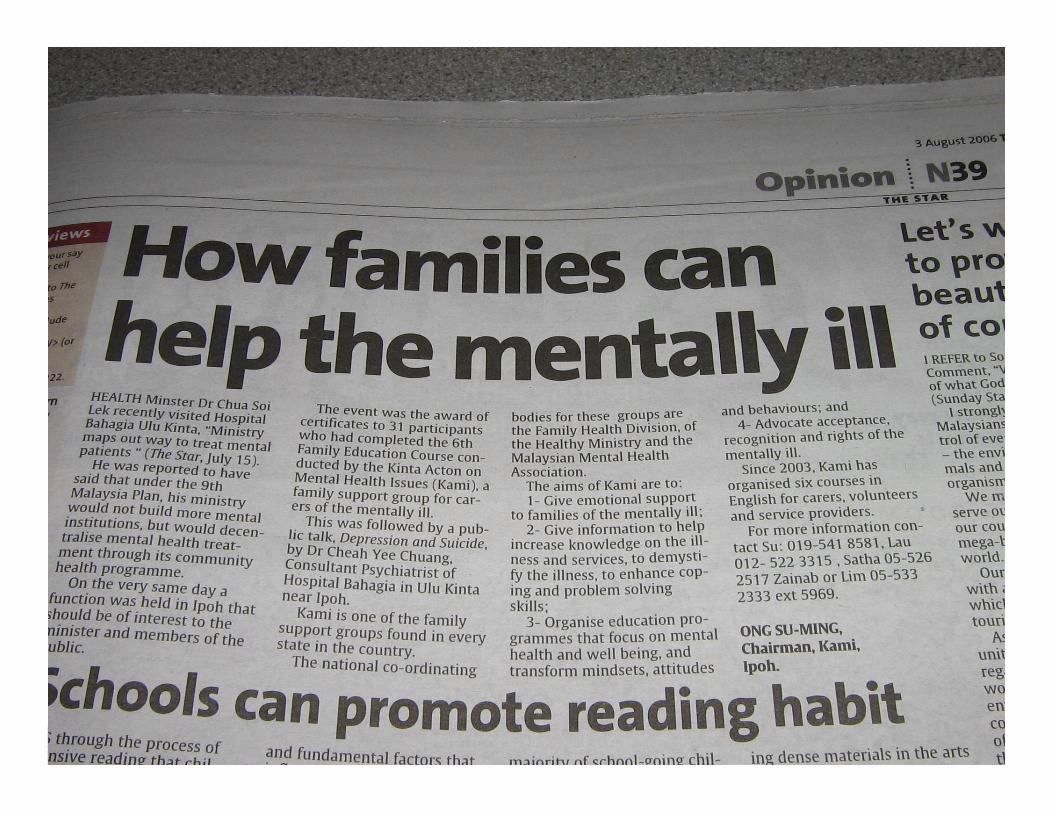

Kinta Alliance for Mentally IllKinta Action on Mental Health Issues
Kumpulan Kumpulan SokonganSokongan KeluargaKeluarga

National Alliance for Mentally Ill (NAMI): Principles of helping families come through trauma
1. The basic focus in the course is on the family member, not the ill person
2. Encouraging families to regain primacy of their own lives
3. Expressing anger and grief: the crux of self care4. We teach empathy as the means of gaining acceptance
of loss5. Because we are family members, we can help each
other to let go

Family support group movement
Self help group, initiated by Malaysia Mental Health Association (March 2003)
Equal partners in care delivery Aims towards promotive, preventive and recovery
oriented care Aims to bring about best practices in care

Benefits of support groups
Opportunities for disclosure Empathic connection Shared goals Psychological adjustments Direct benefits related to needs Demystify illness

The Changing Needs of carers
Onset of Schizophrenia
Understand illnessDon’t knowwhat to do
InformationBasic coping
Education
What to do with voicesetc
Assist withObjective burden
Support group
Feel sadFeel isolated
Support with subjective burden
Support group
Want to help others
Share knowledge from personal experience
Help others
Angry at lack of services
Political action
Advocacy
PROBLEM
NEEDSOLUTION

Family support groups:
SELF HELP GROUPSSELF HELP GROUPS• Emotional support• Information provision Help increase knowledge on illness and services,
demystify illness, enhance coping and problem solving• Advocacy Potential for power and influence
• Education – psychoeducation and family education

1. Majority are in the productive age of 20-40 years.
2. About 70% were never employed or unemployed at the time of registration.

Supported employment: Supported employment: Individual Placement & SupportIndividual Placement & Support
Rapid job search rather than extensive pre-vocational assessment and skills training (Job search)
Attention to patient preferences (Job match) Ongoing support and on going training for the
job without a time limit (Job coach)

From “Family Rejection” to From “Family Rejection” to “Patient living with family and working in the “Patient living with family and working in the community”community”

Encik CCKEncik CCK
33 years old Chinese Single Man, odd jobs on & off
Refuses to live with family past 9 years (he lived in a garage behind a shop)
Felt that his mother loved his brother & sister more than him
Refused to greet his family even if he met them in town
HospitalizationHospitalization
Earlier on treatment in Jelapang Health Clinic
Defaulted treatment 2 years Disturbed public & public made police
report and he was admitted

Family interventionFamily intervention
Try to the address where patient lived (i.e. garage)
Obtained information and help to find his family
Family claimed that no way that they can look after patients as evidenced by the fact that for the past 9 years, he refused to acknowledge them
His mother is also very fearful of him

Family interventionFamily intervention
Regular home visit done to discuss case Patient’s family come to hospital to
discuss plan
PatientPatient Refuse to acknowledge parents Optimization of medication◦ Risperidone 4 mg on◦ Benzhexol 2 mg prn◦ Im flupenthixol 40 mg monthly
Contract with patient: live at home with family and allow family to supervise medications
He was in the hospital for one month before discharge
After dischargeAfter discharge Live with family Keep to himself in the room Not friendly towards mother Still unemployed and occasionally he was
supported financially by his mother Regular with follow-up

Supported employmentSupported employment
Keep encouraging patient to search for work
He was able to work in a small factory making iron gate, earning about RM60-RM80 a day.

1.Wellness
2.Person focus
3.Informed person
4.Self care
5. Close to home
6. Seamless
7. Tailored
8. Effective, efficient
Ministry of Health, Ministry of Health, Malaysia: Service goalsMalaysia: Service goals
Thank you…Thank you…





























