Embed Size (px)
Citation preview

BrHeartj 1984; 51: 233-36
Sudden death in a patient with amyloidosis ofthe cardiacconduction system
D C ALLEN, C C DOHERTY
From the Histopathology Laboratory and Department ofNephrology, Belfast City Hospital, Belfast, Northem Ireland
SUMMARY A 54 year old man had generalised systemic amyloidosis secondary to bilateral basalbronchiectasis of the lungs. He died after an unexpected asystolic cardiac arrest. Necropsy showedextensive amyloid deposition in the cardiac conduction system.
Cardiac amyloidosis is a well established but uncom-mon cause ofhaemodynamic and electrocardiographicabnormalities.'-" Several workers have incriminatedto varying degrees the presence of amyloid depositswithin the cardiac conduction system as the underlyingpathophysiology.1" We report a case of systemicamyloidosis occurring in a 54 year old man secondaryto bilateral basal bronchiectasis, who died after asudden asystolic cardiac arrest due to direct amyloiddeposition in his conduction system. An abnormalelectrocardiogram was recorded eight months beforedeath.
Case report
A 54 year old man was admitted to Belfast CityHospital for evaluation of chronic renal failure. He hada history of bronchiectasis, and nephrogenic diabetesinsipidus had been diagnosed two years previouslyafter investigations for polyuria. The cause of his renalfailure was considered to be renal amyloidosis sincegastric and rectal biopsy specimens stained positivelywith congo red. Since his creatinine clearance was 11ml/min an arteriovenous fistula was created in anticipa-tion of the need for haemodialysis. A 12 leadelectrocardiogram recorded at this time showed a sinusrhythm of 65 beats/min with first degree heart block(PR interval 0-28 s; QRS interval 0.11 s) andincomplete left bundle branch block (Fig. 1). Anunspecific ST/T wave abnormality was also present.He was readmitted to hospital eight months latercomplaining of breathlessness and neck swelling.
Requests for reprints to Dr Derek C Allen, HistopathologyLaboratory, The Laboratories, Belfast City Hospital, BelfastBT9 7AD, Northern Ireland.
Examination showed sinus rhythm, no signs of heartfailure, and a diffuse goitre. Renal function was littlechanged with a creatinine clearance of 10 ml/min, aserum urea concentration of 16'9 mmol/l (1 0 g/l), anda serum potassium concentration of 3 7 mmol (mEq)/l.He was treated for exacerbation of bronchiectasis, butdespite initial improvement sudden cardiac arrestoccurred 24 hours later. His electrocardiogramsshowed asystole, and resuscitation was unsuccessful.
NECROPSY FINDINGSNecropsy showed enlarged emphysematous lungs withpronounced bronchiectatic changes in both bases. Theperipheral airways were dilated and congested, and theoverlying pleural cavities contained fibrous adhesions.The other organs were affected to varying degrees byamyloid infiltration. The kidneys and parathyroidglands showed an obvious waxy pallor, and a pro-nounced amyloid goitre (110 g) was evident.Histological examination showed involvement of theliver, spleen, skin, other endocrine glands, and thegastrointestinal tract. Lung deposition was minimal.The total heart weight was 580 g, and there was
moderate biventricular dilatation and hypertrophy.The aorta and coronary arteries contained only ainiimal amount ofatheroma, and wide lumen patency
was maintained at all points. The pericardium wastranslucent, and the valves were not thickened.Histological examination did not show any recent orlong standing ischaemic myocardial damage. Theventricular interstitium and its vessels contained smallamounts of congo positive amyloid. Thesubendocardial aspects of both atria contained focalamyloid deposits, but the cardiac valves, pericardium,and epicardial vessels and nerves were not affected.
233
on March 18, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.51.2.233 on 1 February 1984. D
ownloaded from

234
t"
1:4.~~t
Fig. 1 Twelve lead electrocardwogram showing (a) a prolongedPR interval (0 28 s) and (b) incomplete bundle branch block.
4 O v4t
Me f~~~~(1.NW~4.
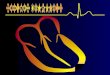
Fig. 2 Histological section showing the sinoatrial node
containing extensive amorphous amyloid deposits both
surrounding and replacing conducting myofibrils. (Haematoxylin
and eosin x300 original magnification.)
Allen, DohertyThe sinoatrial node contained extensive amyloid, andthe branches of its supplying artery were diffuselythickened (Fig. 2). The main nodal artery was notinvolved. Amyloid had also been deposited in theatrioventricular node, the His bundle as it penetratedthe central fibrous body (Fig. 3), and the left mainbundle branch. The myofibrils were intimately mixedwith homogeneous eosinophilic amyloid. The absenceof appreciable nodal and conducting element fibrosiswas confirmed using a sodium alcian blue stain. It wasinteresting to note that amyloid deposition was notablyheavier in the conduction system than in the myocar-dium.
Discussion
Dissection of the main components of the humancardiac conduction system is well documented.12 Thesinoatrial node lies at the crest of the right atrialappendage where it joins the superior vena cava. Theatrioventricular node lies anterior to the coronary sinusbeneath the right atrial endocardium, and the main Hisbundle runs forward and down through the centralfibrous body below the membranous septum. Serialblocks and examination at multiple levels are required.-The paraffin processed tissue sections in this patientwere stained orange-red with alkaline congo red, andthese amyloid deposits showed an apple greenbirefringence under polarised light. Presence ofamyloid was confirmed by staining with sodium alcianblue, and with thiioflavine T viewed for fluorescenceunder ultraviolet light (Fig. 3b). The sections were alsosensitive to potassium permanganate decolorisation, afeature considered by some to be histological confirma-tion of secondary amyloid."I
Cardiac amyloidosis is classically thought of as aninfiltrative cardiomyopathy with subsequent cardiacfailure which may be refractory to conventionaltreatment. It may mimic the clinical picture ofconstrictive pericarditis and the electrocardiographicchanges of healed infarction.III Unspecific electro-cardiographic abnormalities such as low voltage andaxis deviation have been noted. James' asserted thatthe "disturbance of cardiac function and conductionare in a significant amount due to the amyloidinfiltration directly" (that is, of the conductionsystem). He found heavy sinoatrial node deposits andatrial fibrillation in two of his five cases. Others havesince reinforced his commnents,9 10 but sinus rhythmhas also been reported in the presence of severeconduction system infiltration.6 Prolongation of thePR interval and bundle branch block are welldocumented in amyloid heart disease. Bharati et alreported a case of recurrent ventricular fibrillation andextensive cardiac conduction system deposition ofamyloid.'10 In 1960 sudden death occurred in two cases
on March 18, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.51.2.233 on 1 February 1984. D
ownloaded from

Sudden death in cardiac amyloidosis"a'i,-Fig. 3 Histological section showing the main His bundle penetrating the centralfibrous body and extensive amyloid deposition
intimately mixed with conducting elements (haematoxylin and eosin x 125 original magnification); and (b) a higher power view of the
His bundle with the centralfibrous body in the top right corner; abundant amyloid is confirmed (thioflavine T viewed under ultraviolet
light x400 original magnification).
of primary cardiac amyloidosis associated with atrio-ventricular node and His bundle infiltration.'4 In a
series by Wright and Calkins"3 30% of their patientswith primary amyloidosis died suddenly, probablyfrom arrhythmic cardiac involvement. This dangerhad been noted elsewhere but not substantiated byconduction system dissection in either case.' Suddendeath occurred in our patient in the absence of severeatheromatous disease or electrolyte abnormalities andin the presence of conduction system amyloid infil-trates.Two main aetiological factors have been suggested
for dysfunction in amyloid heart disease. The coronaryor intramyocardial vessels may be thickened causingischaemic lesions,5 and the amyloid deposition mayatrophy the parenchyma directly. The latter mecha-nism leads to a less compliant and contractilemyocardium with haemodynamic disturbances. Ourpatient had amyloid throughout his conduction sys-tem, increasing the functional implications of the
deposits. This was confirmed by an abnormal electro-cardiogram showing first degree heart block andincomplete left bundle branch block.
This case therefore illustrates the potential hazard ofsudden death from conduction system disease inpatients with generalised systemic amyloidosis.
We thank Dr J D Biggart for his advice on thepathological specimens and DrM E Scott for reviewingthe electrocardiogram. We also thank Mr John Orchinfor his technical and photographic expertise.
References
1 Wessler S, Freedburg AS. Cardiac amyloidosis;electrocardiographic and pathologic observations. ArchIntern Med 1948; 82: 63-74.
2 Mulligan RM. Amyloidosis of the heart. Archives ofPathology 1958; 65: 615-30.
235
on March 18, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.51.2.233 on 1 February 1984. D
ownloaded from

236
3 Cassidy JT. Cardiac amyloidosis. Two cases with digitalissensitivity. Ann Intern Med 1961; 55: 989-94.
4 Farrokh A, Walsh TJ, Massie E. Amyloid heart disease.AmJ Cardiol 1964; 13: 750-6.
5 James TN. Pathology of the cardiac conduction system inamyloidosis. Ann Intemn Med 1966; 65: 28-36.
6 Garcia R, Saeed SM. Amyloidosis. Cardiovascular mani-festations in five illustrative cases. Arch Intern Med 1968;121:259-66.
7 Buja LM, Khoi NB, Roberts WC. Clinically significantcardiac amyloidosis. Clinicopathologic findings in 15patients. AmJ Cardiol 1970; 26: 394-405.
8 Ridolfi RL, Bulkley BH, Hutchins GM. The conductionsystem in cardiac amyloidosis. Clinical and pathologicfeatures of 23 patients. Amj Med 1977; 62: 677-86.
9 Isokane N, Fukushima N, Miyazaki T, Dohi I. A case ofsick sinus syndrome in primary systemic amyloidosis. J
Allen, Doherty
Electrocardiol 1978; 11: 191-6.10 Bharati S, Lev M, Denes P, et al. Infiltrative
cardiomyopathy with conduction disease and ventriculararrhythmia: electrophysiologic and pathologic correla-tions. AmJ7 Cardiol 1980; 45: 163-73.
11 Davies MJ. Pathology of conducting tissue of the heart.London: Butterworths, 1971: 105-6.
12 Pomerance A, Davies MJ. The pathology of the heart.London: Blackwell Scientific Publications, 1975: 26-31.
13 Wright JR, Calkins E. Clinical-pathologic differentiationof common amyloid syndromes. Medicine (Baltimore)1981; 60: 429-48.
14 Lumb G, Shacklett RS. Human cardiac conduction tissuelesions. AmJ Pathol 1960; 36: 411-29.
15 Kyle RA, Bayrd ED. Amyloidosis: review of 236 cases.Medicine (Baltimore) 1975; 54: 271-99.
Notice
British Cardiac SocietyThe Annual General Meeting for 1984 will take place inLeicester on 11 and 12 April 1984, and the closing datefor receipt of abstracts was 3 January 1984.The Autumn Meeting in 1984 will be held on 3 and 4
December 1984, and the closing date for receipt ofabstracts will be 15 August 1984.
on March 18, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.51.2.233 on 1 February 1984. D
ownloaded from