Embed Size (px)
DESCRIPTION
preoperative evaluation and optimisation .
Citation preview
Cardiac Patient For Non Cardiac Surgery-Preoperative Evaluation
Dr Pankaj N Surange MBBS,MD,FICMR
Graded Specialist Anesthesia
Artemis Health Institute
REFERENCES
• ACC/AHA Guidelines 2002-updated 2006(perioperative Beta Blockade Therapy)
• BJA 95(1): 3-19 2005- perioperative Myocardial Infarction
• BJA 93: 2004-Sympathomodulatory Therapies In Perioperative Medicine
GOALS
• PT CURRENT STATUS– IDENTIFICATION OF PTS UNSTABLE CV DS
– IDENTIFICATION OF PTS WITH KNOWN AND SYMPTOMATIC CAD
– IDENTIFICATION OF PTS AT RISK OF CAD» PVD» HTN» DM» SMOKING» HYPERCHOLESTROLEMIA
GOALS
• THERAPIES TO BRING PT IN OPTIMAL CONDITION
• ANESTHETIC PLAN
• PROCEDURE • PTS PHYSIOLOGY
approachapproach
• Preoperative• Evaluation, risk stratification, and preparation
• Intraoperativesmooth induction
smooth recovery
adequate monitoring
• Postoperativelycont. monitoring and vigilance
PREOPERATIVE CARDIAC EVALUATION
• ACC/AHA GUIDELINES-5 FACTORS FOR RISK STRATIFICATION
– Recency Of Coronary Revascularization
– Recency Of Last Favourable Cardiac Evaluation
– +Nce Of Comorbidities-clinical Predictors
– Functional Status
– Risk Of Proposed Surgery
1-CORONARY REVASCULARISATION
• Complete coronary surgical revascularization -5 yrs
• PCI-- 6months-5 yrs
• No recurrent S/S of ischemia
• Clinical status is stable
No further cardiac testing is necessary
2-Coronary evaluation
• Past 2 years
• Invasive/non invasive tech
– Favorable– No definite change or new symptom
No further cardiac testing is necessary
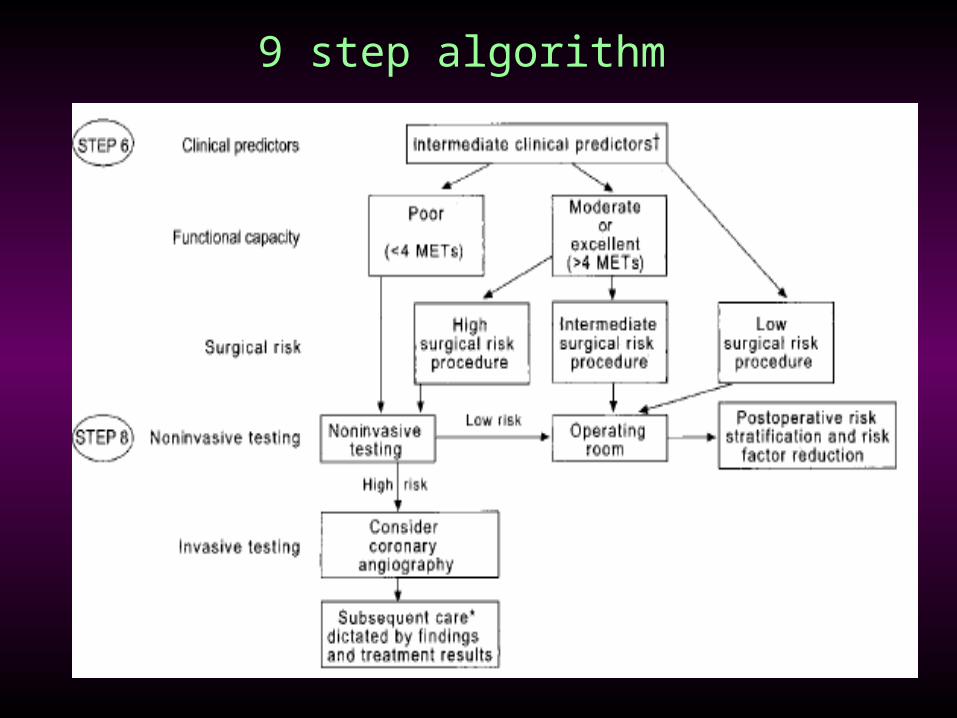
3-Clinical predictors
• Major– Unstable coronary syndromes
• recent MI with evidence for ischemia• unstable or severe angina (Canadian class III or IV)
– Decompensated CHF– Significant arrhythmia
• high grade AV block• symptomatic ventricular arrhythmia (with organic disease)• supraventricular arrhythmia with uncontrolled rate
– Severe valvular disease
• Intermediate– Mild angina pectoris (Canadian class I or II)– Prior MI by history or pathological Q waves– Compensated or prior CHF– Diabetes mellitus– Renal insufficiency (creatinine > 2)
• Minor– Advanced age– abnormal ECG (LVH, LBBB, ST-T change)– Rhythm other than sinus– Low functional capacity– History of stroke– Uncontrolled systemic hypertension
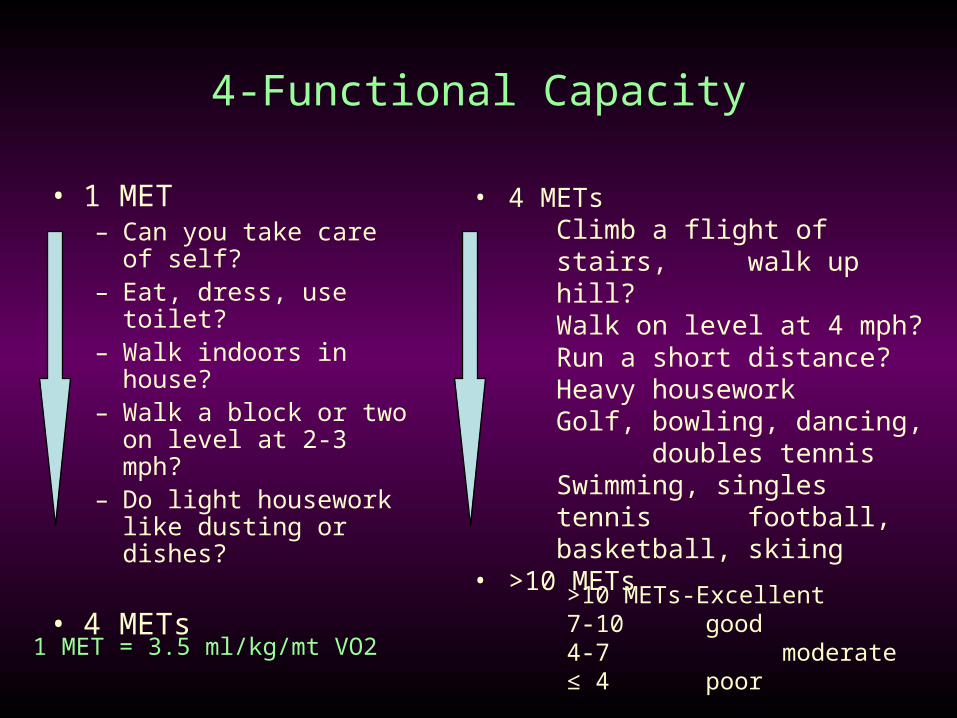
4-Functional Capacity
• 1 MET– Can you take care of
self? – Eat, dress, use toilet?– Walk indoors in house?– Walk a block or two on
level at 2-3 mph?– Do light housework like
dusting or dishes?
• 4 METs
• 4 METsClimb a flight of stairs,
walk up hill?Walk on level at 4 mph?Run a short distance?Heavy houseworkGolf, bowling, dancing,
doubles tennisSwimming, singles tennis
football, basketball, skiing
• >10 METs
1 MET = 3.5 ml/kg/mt VO2
>10 METs-Excellent7-10 good4-7 moderate≤ 4 poor
5-Surgical risk
High (reported cardiac risk > 5%)
•emergent major operations, esp. in elderly
•aortic and other major vascular procedures
•peripheral vascular procedures
•anticipated prolonged procedure with large fluid shift/blood loss

• Intermediate (reported cardiac risk < 5%)
– carotid endarterectomy
– head and neck
– intraperitoneal & intrathoracic
– orthopedic
– prostate
• Low (reported cardiac risk < 1%)
– endoscopic procedures
– superficial procedure
– cataract
– breast
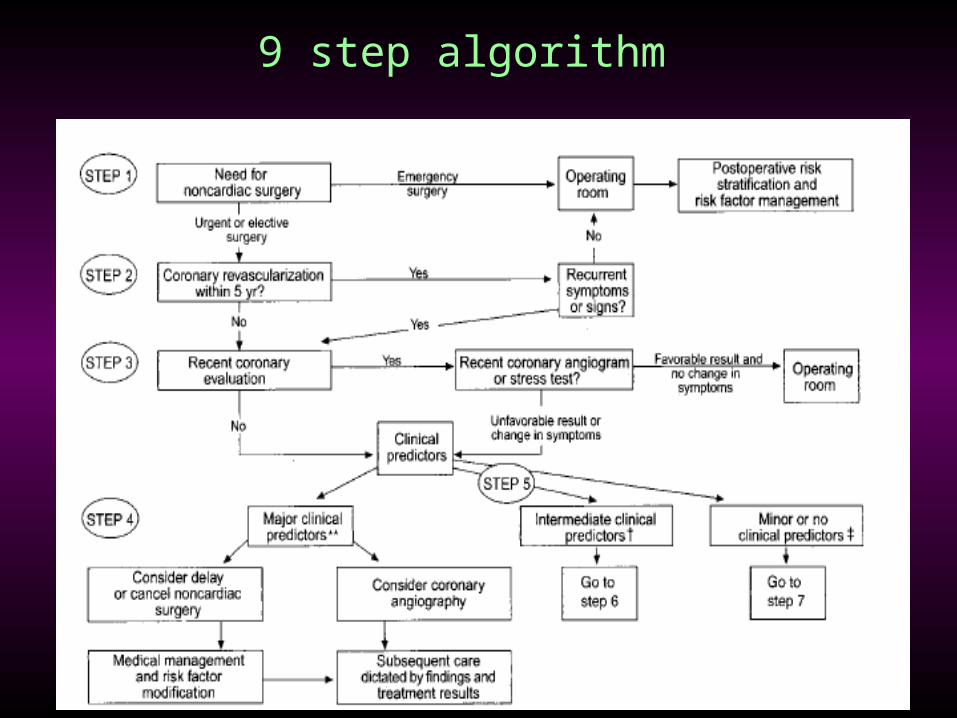
9 step algorithm
9 step algorithm
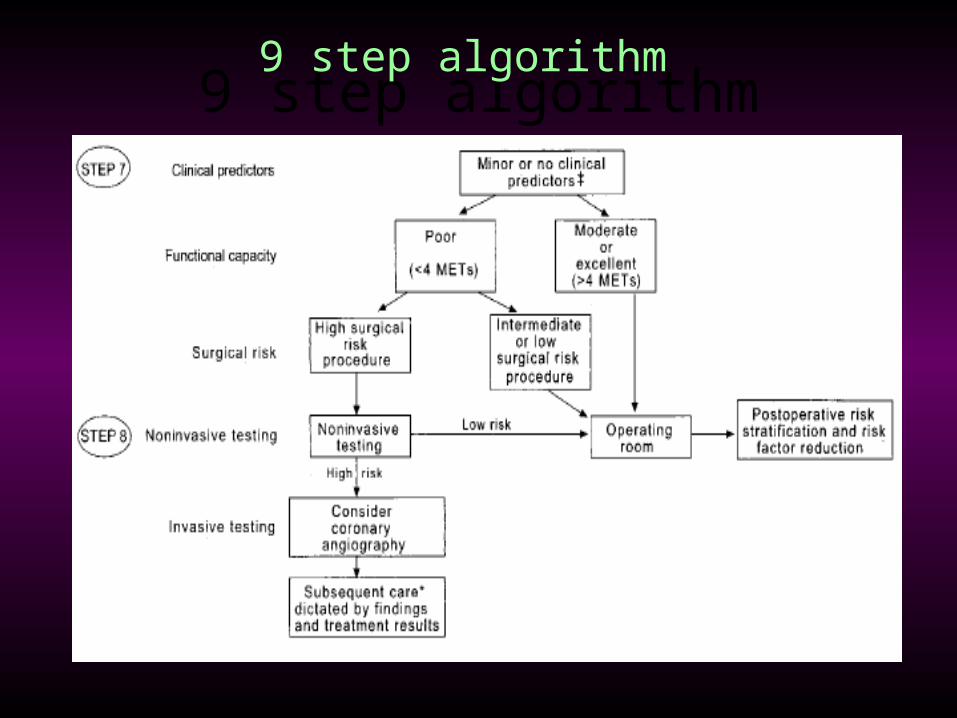
9 step algorithm9 step algorithm
PREOP TESTING
• ECG
• DETECT LVH,BBB & CONDUCTION DEFECT
• PREVIOUS MI
• BASELINE FOR INTRA AND POST OP COMPARISON
• INCREASED PERIOP RISK• ST DEPRESSION MORE THAN .5 MM• LVH WITH STAIN PATTERN• LBBB

• EXERCISE STRESS TEST
• STRONGEST DETERMINANT OF RISK AND NEED FOR INVASIVE MONITORING
• LEAD SELECTION
• ECG CRITERIA– 1 M M OF J POINT DEPRESSION
– 2MM OF ST DEPRESSION AT 80 MS FROM J POINT
– ST ELEVATION
– NON ECG RESP• LOW ACHIEVED HR• SYSTOLIC HYPOTENSION• INABILITY TO EXERCISE FOR MORE THAN 3 MIN
PHARMACOLOGICAL STRESS TEST
• Two Categories– Dobutamine Stress Echo-incr. Mvo2
– New/Incr In Rwma– More Than 5/16 Lt Ventricular Segm Involvement
– Dipyridamole Thallium-mimics Coronary Art Dialatation Resp Associated With Exercise
– Infarcted Area-fixed Defect– Ischemic Area-reversible Defect
ECHOCARDIOGRAPHY
– LVEF– RWMA– Valvular Abn– Cong Cardiac Defects
CORONARY ANGIOGRAPHY
• Non Invasive Testing-high Risk Of Adverse Outcome
• Angina Unresponsive To adequate Medical Therapy
• Unstable Angina-intermediate And High Risk Sx
• High Clinical Predictor In High Risk Sx
PERIOP THERAPY
• BETA BLOCKERS– CVS EFFECTS
• ↓ HR-(diastolic Time)• ↓ Contractility• Plaque Stabilization- ↓ Shear Forces• Antiarrythmic Effect
– ELIGIBILITY CRITERIA• CLINICAL -ANY 2
– AGE>65– HTN– CHR SMOKER– SER CHOLESTROL>240 mg/dl– DM
• CARDIAC RISK INDEX CRITERIA– HIGH RISK SX PROCEDURE– IHD– CVA– DM– CRF
OTHER THERAPIES
• Alpha-2 Adrenergic Agonist
• Regional Anesthesia
– Epidural