Embed Size (px)
Citation preview

JOURNAL OF CLINICAL MICROBIOLOGY,0095-1137/98/$04.0010
Oct. 1998, p. 3060–3065 Vol. 36, No. 10
Copyright © 1998, American Society for Microbiology. All Rights Reserved.
Subcutaneous Hyalohyphomycosis Caused byColletotrichum gloeosporioides
JOSEP GUARRO,1* TEREZINHA E. SVIDZINSKI,2 LUIS ZAROR,3 MAILY H. FORJAZ,4
JOSEPA GENE,1 AND OLGA FISCHMAN4
Unitat de Microbiologia, Facultat de Medicina i Ciencies de la Salut, Universitat Rovira i Virgili, 43201 Reus, Spain1;Servico de Micologia Medica, Departamento Analisis Clınicas, Universidade Estadual Maringa, Parana,2 and Servico
de Micologia Medica, Departamento de Microbiologia, Imunologia e Parasitologia, UNIFESP/EPM, Sao Paulo,4
Brazil; and Instituto de Microbiologıa Clınica, Universidad Austral de Chile, Valdivia, Chile3
Received 7 April 1998/Returned for modification 7 May 1998/Accepted 18 June 1998
The coelomycete Colletotrichum gloeosporioides was isolated in pure culture from subcutaneous nodules of theleft forearm and elbow of a farmer after traumatic injury. To our knowledge, we report the first case involvingthis fungus as an etiological agent of subcutaneous infection. The in vitro inhibitory activities of amphotericinB, itraconazole, ketoconazole, miconazole, flucytosine, and fluconazole were studied.
Colletotrichum Corda is a complex form genus of the formclass Coelomycetes, asexual fungi producing conidia withinfruit bodies, named conidiomata. These structures are spheri-cal (pycnidia), with conidiogenous cells lining the inner cavitywall, or are cup-shaped (acervuli), in which case, the conidiog-enous cells form a palisade on the surface of the conidiomata.This genus comprises several hundred species, mostly plantpathogens, which have been described mainly on the basis oftheir conidial morphology and the presence or absence ofsetae. The genus Colletotrichum was monographed by von Arx(16), and only a restricted number of species was accepted.Although only rarely pathogenic to humans, Colletotrichumspp. have been reported as almost exclusively causing keratitis(6–8, 11, 12), usually after an eye injury. In this report, wedescribe a diabetic man with a history of trauma who devel-oped a subcutaneous infection caused by Colletotrichum gloeo-sporioides (Penz.) Sacc.
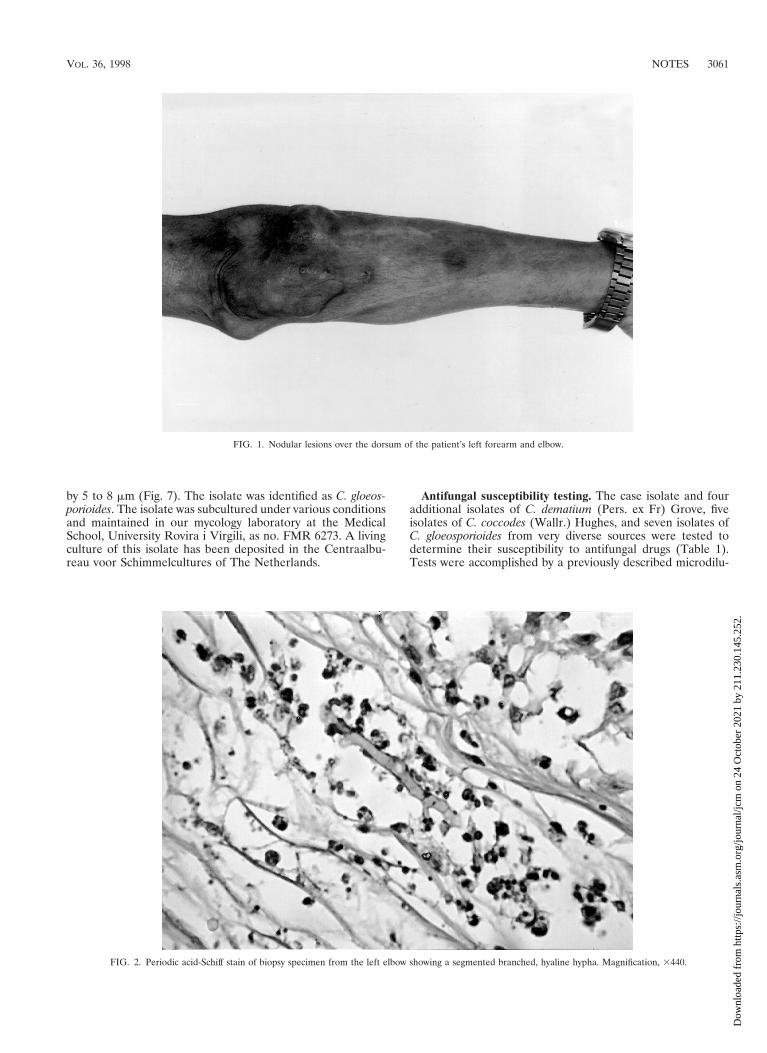
Case report. A 56-year-old male farmer and resident ofMaringa in the state of Parana, Brazil, presented himself to theServico de Dermatologia do Hospital Universitario Regionalde Maringa in May 1996 because of the presence of nodularlesions on his left forearm and elbow. Past medical historyrevealed that he was diabetic and hypertensive and that he wasreceiving prednisone (20 mg/day) by autoprescription. He re-ported a previous traumatic injury of his left hand by rottenwood that had required local suturing. He told of the appear-ance, approximately 1 year later, of nonpruritic nodules in thesame trauma site. He denied having suffered fever and loss ofweight. On examination, he presented tuberose-nodular, ery-thematous, violaceous, solitary or confluent lesions measuring1 to 3 cm in diameter and localized on the left forearm andelbow. In addition, several vinaceous, macular lesions of ca 1.5-cm diameter were observed, also on the dorsum of the forearm(Fig. 1). The results of routine laboratory investigations ofblood and urine were within normal limits. Radiography of thethorax showed cardiomegaly with left ventricular hypertrophyand ectasia of the aortic arch. Radiography of the left elbowshowed only soft-tissue thickening without evidence of bone or
joint lesions. A computerized tomography scan showed thepresence of an expansive, hypodense, and multilocular lesionin the soft tissue of the left elbow region. Biopsy of the lesionswas performed, and the contents of some of the nodules wereaspirated for examination. Direct examination of all specimenssampled revealed the presence of septate, acute angledbranching, irregular, hyaline hyphae. A histologic section ofthe biopsy material stained with periodic acid-Schiff and Go-mori methenamine silver stains showed a hyperplasic epider-mis with a psoriasiform pattern. The dermis showed an exten-sive granulomatous reaction with central necrosis and multiplefoci of microabscesses. Throughout the tissue, numerous irreg-ularly shaped, hyaline, septate, branched hyphae were present(Fig. 2 and 3). All of the tissue samples and the contents of thenodules were cultured on Sabouraud’s glucose agar (SGA) andpotato dextrose agar (PDA). Fungal colonies grew out in allthe cases in both media. Microscopic examination of the cul-tures demonstrated that all of them presumably belonged tothe same species. Routine bacteriological cultures and culturesfor mycobacteria were negative. While the diagnostic proce-dures were being performed, and before establishing treat-ment, the patient unfortunately died as a result of a car acci-dent. An autopsy was not performed.
For identification, fungal colonies from the biopsy materialand from the nodules’ contents were inoculated into SGA andother routine mycological media, such as PDA, cornmeal, maltextract, and oatmeal agars and incubated at room temperature.All of the media gave rise to white to grayish, loosely texturedcolonies with similar characteristics. Colonies on PDA grewvery quickly, occupying the whole surface of the Petri dish in 10days. They were greenish gray with pinkish to salmon patches,powdery to velutine, profusely sporulated, and with abundantproduction of conidiomata; the reverse was grayish (Fig. 4).The colonies on oatmeal agar also grew very quickly. They hada floccose texture with abundant production of white aerialmycelium. The production of conidiomata was mainly re-stricted to the central areas, and the reverse was uncolored.The conidia were borne on elongated phialides in acervularconidiomata, or, in the early stages of development, on solitaryfertile hyphae. The conidia were straight, cylindrical to slightlyclavate, hyaline, obtuse at the apex, extremely variable inlength, and measured 6 to 26 by 4 to 7 mm (Fig. 5 and 6).Numerous appressoria were also present. They were clavate,triangular or irregular, dark pigmented, and measured 8 to 15
* Corresponding author. Mailing address: Unitat de Microbiologia,Departament de Ciencies Mediques Basiques, Facultat de Medicina iCiencies de la Salut, Universitat Rovira i Virgili, Carrer Sant Llorenc,21, 43201-Reus, Tarragona, Spain. Phone: 34 77 75 93 59. Fax: 34 77 7593 22. E-mail: [email protected].
3060
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 24
Oct
ober
202
1 by
211
.230
.145
.252
.
by 5 to 8 mm (Fig. 7). The isolate was identified as C. gloeos-porioides. The isolate was subcultured under various conditionsand maintained in our mycology laboratory at the MedicalSchool, University Rovira i Virgili, as no. FMR 6273. A livingculture of this isolate has been deposited in the Centraalbu-reau voor Schimmelcultures of The Netherlands.
Antifungal susceptibility testing. The case isolate and fouradditional isolates of C. dematium (Pers. ex Fr) Grove, fiveisolates of C. coccodes (Wallr.) Hughes, and seven isolates ofC. gloeosporioides from very diverse sources were tested todetermine their susceptibility to antifungal drugs (Table 1).Tests were accomplished by a previously described microdilu-
FIG. 1. Nodular lesions over the dorsum of the patient’s left forearm and elbow.
FIG. 2. Periodic acid-Schiff stain of biopsy specimen from the left elbow showing a segmented branched, hyaline hypha. Magnification, 3440.
VOL. 36, 1998 NOTES 3061
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 24
Oct
ober
202
1 by
211
.230
.145
.252
.

tion method (10) performed mainly according to the NationalCommittee for Clinical Laboratory Standards’ guidelines foryeasts, by using RPMI 1640 medium (buffered to pH 7.0 with0.165 M morpholinepropanesulfonic acid [MOPS]), an inocu-lum of 4.4 3 104 to 2.8 3 105 CFU/ml, a temperature ofincubation of 30°C, a second-day reading (48 h), and an addi-tive drug dilution procedure.
Discussion. Colletotrichum spp. are typical fungi pathogenicfor plants and causing anthracnosis, necrosis, leaf spot, andfruit rot. The diseases caused are commonly seed borne. Somespecies cause latent infections on woody plants, and the in-fected plants often show poor growth, and their fruits may rot(17). The species are anamorphs of the genus GlomerellaSpauld. & H. Schrenk, classically considered as belonging tothe order Phyllachorales, although some evidence exists abouttheir relationship with the Sordariales (15), both orders of theAscomycota. von Arx (16) delimited the most important spe-cies of Colletotrichum, considering their most distinctive char-acteristics to be the shape and size of the conidia and theirspecific hosts. However, further studies have enlarged the ge-nus (13). The taxonomy of the genus is still unclear, and acomprehensive review of the numerous species described isneeded. Sutton (14) pointed out that in vitro studies are re-quired to determine the nature of the most representativemorphological features, such as sclerotia, setae, and appresso-ria, in order to compare them with those shown in the hostplant, because some differences have been reported. C. gloeo-sporioides is one of the commonest plant-pathogenic fungi tooccur in the tropics and subtropics and is found worldwide. Itconstitutes a very heterogeneous taxon. von Arx (16) has givenmore than 600 synonyms for this species and has recognizednine forms, but probably many more can be differentiated by acombination of cultural characteristics, morphology, hostrange, and pathogenicity. Several molecular techniques havebeen used for a better characterization of the plant-pathogenicstrains of this fungus (1, 5). Up to now, four species of Colle-totrichum were known to have caused infections in humans orother animals (2). They are C. coccodes, C. dematium, C.gloeosporioides and C. graminicola (Ces.) Wilson. These specieshad been associated exclusively with keratitis (6–8, 11, 12), butrecently Midha et al. (9) described a case of disseminatedinfection in a neutropenic patient probably caused by an un-identified Colletotrichum sp. Hence, the case of infection re-
FIG. 3. Methenamine silver stain of the skin biopsy specimen showing toruloid, septate hyphal elements with irregular forms. Magnification, 3440.
FIG. 4. C. gloeosporioides colony growing on PDA after 10 days of incuba-tion.
3062 NOTES J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 24
Oct
ober
202
1 by
211
.230
.145
.252
.

ported here is the second one concerning an extraocular in-fection caused by a member of this genus. This change in thespectrum of the infection has also been noted in other fungi,first associated with keratitis, such as Fusarium (3) and Acre-monium (4) spp. among others. The species pathogenic forhumans were recently described and illustrated, and a key fortheir identification was also included (2). The other three
pathogenic species can be easily differentiated from C. gloeos-porioides by their setose conidiomata. In particular, C. dema-tium and C. graminicola are clearly distinguished by their fal-cate conidia, similar to those of Fusarium spp., althoughunicellular. The ascigerous state of C. gloeosporioides, Glomer-ella cingulata (Stoneman) Spauld. & H. Schrenk has been re-ported as developing on PDA (8).
FIG. 5. Conidia of C. gloeosporioides. Stain, lactophenol cotton blue. Magnification, 3440.
FIG. 6. Conidia of C. gloeosporioides. Magnification by Nomarski optics, 31,440.
VOL. 36, 1998 NOTES 3063
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 24
Oct
ober
202
1 by
211
.230
.145
.252
.

Of the nine previously reported clinical cases of infectionattributed to Colletotrichum spp., one was caused by C. dema-tium (6), one was caused by C. graminicola (11), three werecaused by C. coccodes (reported as C. atramentarium) (7),three were caused by C. gloeosporioides (8, 12), and one wascaused by a Colletotrichum sp. (9). Only the last one was ex-traocular; the other eight were typical cases of keratitis. All ofthese cases followed an ocular injury, except one in which thepatient had been treated with general and topical corticoste-roid therapy for 3 years because of uveitis (8). The data con-
cerning these cases are very scanty, and the results from thedifferent treatments applied were variable. One patient wassuccessfully treated with topical amphotericin B (6). In anothercase, the same treatment together with general therapy withflucytosine also resolved the infection (8). However, in a thirdcase, the use of a combination of an amphotericin B suspen-sion and miconazole nitrate eye ointment was ineffective (12).In the invasive case, the patient died despite treatment withamphotericin B and itraconazole (9). In one case, the patientwas cured after topical treatment with 4% piramicin (8), and in
FIG. 7. Appressoria of C. gloeosporioides. Stain, lactophenol cotton blue. Magnification, 3440.
TABLE 1. Antifungal susceptibility of Colletotrichum strains
StrainMIC (mg/ml) at 48 h/MIC at 72 h (MLC [mg/ml] at 48 h)
Amphotericin B Flucytosine Fluconazole Itraconazole Ketoconazole Miconazole
C. gloeosporioidesCBS 465.83 0.06/0.06 (0.06) 16/64 (16) 4/8 (64) ,0.03/0.06 (0.25) 0.125/0.25 (1) 4/4 (4)FMR 3383 0.06/0.06 (0.06) 16/64 (16) 4/8 (64) 0.06/0.125 (0.25) 0.125/0.25 (1) 4/4 (4)FMR 6273 0.125/0.25 (4) .128/.128 (.128) .64/.64 (.64) .16/.16 (.16) 2/4 (.16) 2/2 (16)CBS 147.28 0.125/0.25 (0.5) .128/.128 (.128) .64/.64 (.64) 0.5/0.5 (16) 2/4 (16) 2/4 (8)CBS 160.50 0.03/0.06 (0.06) .128/.128 (.128) 16/16 (.64) 0.25/0.25 (1) 0.25/0.5 (2) 0.25/0.25 (1)CBS 572.97 0.06/0.06 (0.06) .128/.128 (.128) .64/.64 (.64) 1/.16 (.16) 2/4 (16) 2/2 (16)CBS 953.97 0.25/0.25 (0.25) .128/.128 (.128) .64/.64 (.64) 4/.16 (.16) 4/4 (.16) 4/4 (4)
C. coccodesIMI 136601 ,0.03/,0.03 (0.25) .128/.128 (.128) 32/64 (.64) 0.5/2 (.16) 1/2 (.16) 2/4 (8)CBS 122.25 0.06/0.06 (0.25) .128/.128 (.128) 8/16 (.64) 0.06/0.25 (.16) 0.125/0.25 (.16) 0.5/0.5 (.16)CBS 125.57 4/.16 (.16) .128/.128 (.128) .64/.64 (.64) .16/.16 (.16) 16/.16 (.16) 8/.16 (.16)CBS 527.77 0.03/0.06 (0.06) .128/.128 (.128) 8/16 (.64) 0.25/0.25 (.16) 8/16 (.64) 0.5/0.5 (8)CBS 528.77 0.06/0.06 (0.06) .128/.128 (.128) 32/65 (.64) 0.5/0.5 (.16) 0.5/1 (.16) 2/2 (8)
C. dematiumCBS 167.49 0.125/0.125 (0.25) .128/.128 (.128) 8/8 (.64) 0.25/0.25 (8) 0.25/0.25 (2) 2/2 (4)CBS 170.59 1/1 (1) .128/.128 (.128) .64/.64 (.64) .16/.16 (.16) 16/16 (.16) 4/8 (4)CBS 351.73 0.06/0.06 (0.125) 16/34 (.128) .64/.64 (.64) .16/.16 (.16) 8/16 (.16) 4/4 (.16)CBS 714.95 0.5/0.5 (0.5) .128/.128 (.128) .64/64 (.64) .16/.16 (.16) 16/16 (.16) 8/8 (8)
3064 NOTES J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 24
Oct
ober
202
1 by
211
.230
.145
.252
.

the most recent case, the patient was also cured after combinedtreatment with topical natamycin, intracameral amphotericinB, and oral fluconazole (11).
The data obtained from the antifungal susceptibility testingof the isolate from the patient and 15 comparison isolatesdemonstrated, in general, that the MICs for the organismswere low, with the exception of those of flucytosine and, to alesser degree, fluconazole. For only one isolate was the MIC ofamphotericin B higher than 1 mg/ml. For two isolates, theMICs of miconazole were higher than 4 mg/ml, and for keto-conazole and itraconazole, there were only four isolates, ineach case, for which the MICs exceeded such values. Differ-ences between MICs read at 48 h and at 72 h were generallynot important. Usually the values were the same after the tworeadings, and in only one case were the differences higher than2 dilutions. Examination of the minimal lethal concentrations(MLCs) showed that the majority of isolates displayed a majordegree of resistance. They were, however, mainly susceptibleto amphotericin B. Only one strain (C. coccodes CBS 125.57)was clearly resistant to all of the drugs tested. No major dif-ferences were observed among the MICs and MLCs for thethree species tested.
We thank L. Ajello from Emory University School of Medicine(Atlanta, Ga.) for reviewing the manuscript and Luis A. Quiroz andJose C. da Silva from the Universidade Estadual de Maringa (Maringa,Brazil) for their kind help in the preparation of this article.
This work was supported by the “Fundacio Ciencia i Salut” (Reus,Spain).
REFERENCES
1. Braithwaite, K. S., J. A. G. Irwin, and J. M. Manners. 1990. Ribosomal DNAas a molecular taxonomic marker for the group species Colletotrichum gloeos-
porioides. Aust. Syst. Bot. 3:733–738.2. de Hoog, G. S., and J. Guarro (ed.). 1995. Atlas of clinical fungi. Centraal-
bureau voor Schimmelcultures, Baarn, The Netherlands.3. Guarro, J., and J. Gene. 1995. Opportunistic fusarial infections in humans.
Eur. J. Clin. Microbiol. Infect. Dis. 14:741–754.4. Guarro, J., W. Gams, I. Pujol, and J. Gene. 1997. Acremonium species, new
emerging opportunists: in vitro antifungal susceptibilities and review. Clin.Infect. Dis. 25:1222–1229.
5. He, C. Z., A. M. Masel, J. A. G. Irwin, S. Kelemu, and J. A. Manners. 1995.Distribution and relationship of chromosome-specific dispensable DNA se-quences in diverse isolates of Colletotrichum gloeosporioides. Mycol. Res.99:1325–1333.
6. Liao, W. Q., J. Z. Shao, S. Q. Li, T. Z. Li, S. X. Wo, U. Z. Zhang, and Q. T.Chen. 1983. Colletotrichum dematium caused keratitis. Chin. Med. J. 96:391–394.
7. Liesegang, T. J., and R. K. Forster. 1980. Spectrum of microbial keratitis inSouth Africa. Am. J. Ophthalmol. 90:38–47.
8. Matsuzaki, O., M. Yasuda, and M. Ichinohe. 1988. Keratomycosis due toGlomerella cingulata. Rev. Iber. Micol. 5(Suppl. 1):30.
9. Midha, N. K., Y. Mirzanejad, and M. Soni. 1996. Colletrotrichum sp.: plantor human pathogen? Antimicrob. Infect. Dis. Newsl. 15:26–27.
10. Pujol, I., J. Guarro, C. Llop, L. Soler, and J. Fernandez-Ballart. 1996.Comparison study of broth macrodilution and microdilution antifungal sus-ceptibility tests for the filamentous fungi. Antimicrob. Agents Chemother.40:2106–2110.
11. Ritterband, D. C., M. Shah, and J. A. Seedor. 1997. Colletotrichum gramini-cola: a new corneal pathogen. Cornea 16:362–364.
12. Shukla, P. K., Z. A. Khan, B. Lal, P. K. Agrawal, and O. P. Srivastava. 1983.Clinical and experimental keratitis caused by Colletotrichum state of Glomer-ella cingulata and Acrophialophora fusispora. Sabouraudia 21:137–147.
13. Sutton, B. C. 1962. Colletotrichum dematium (Pers. ex Fr.) Grove and C.trichellum (Fr. ex. Fr.) Duke. Trans. Br. Mycol. Soc. 45:222–232.
14. Sutton, B. C. 1980. The Coelomycetes. Commonwealth Mycological Insti-tute, Kew, United Kingdom.
15. Uecker, F. A. 1994. Ontogeny of the ascoma of Glomerella cingulata. Myco-logia 86:82–88.
16. von Arx, J. A. 1957. Die Arten der Gattung Colletotrichum. Phytopathol. Z.29:413–468.
17. von Arx, J. A. 1987. Plant pathogenic fungi. Beih. Nova Hedwigia 87:1–288.
VOL. 36, 1998 NOTES 3065
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 24
Oct
ober
202
1 by
211
.230
.145
.252
.





























