Embed Size (px)
Citation preview

STROKEProf. Univ. Dr. Jianu Dragoș Cătălin
Timișoara

Definition
➢ It is characterized by the sudden onset of a focal neurologic
impairment that can be ascribed to a specific location in the
brain, retina or spinal cord
➢ Can be subdivided into ischemic and hemorrhagic stroke

Hemorrhagic stroke
- Subarachnoid hemorrhage (SAH) –
caused by rupture of an intracranial
aneurysm
- Nontraumatic intracerebral
hemorrhage (ICH)
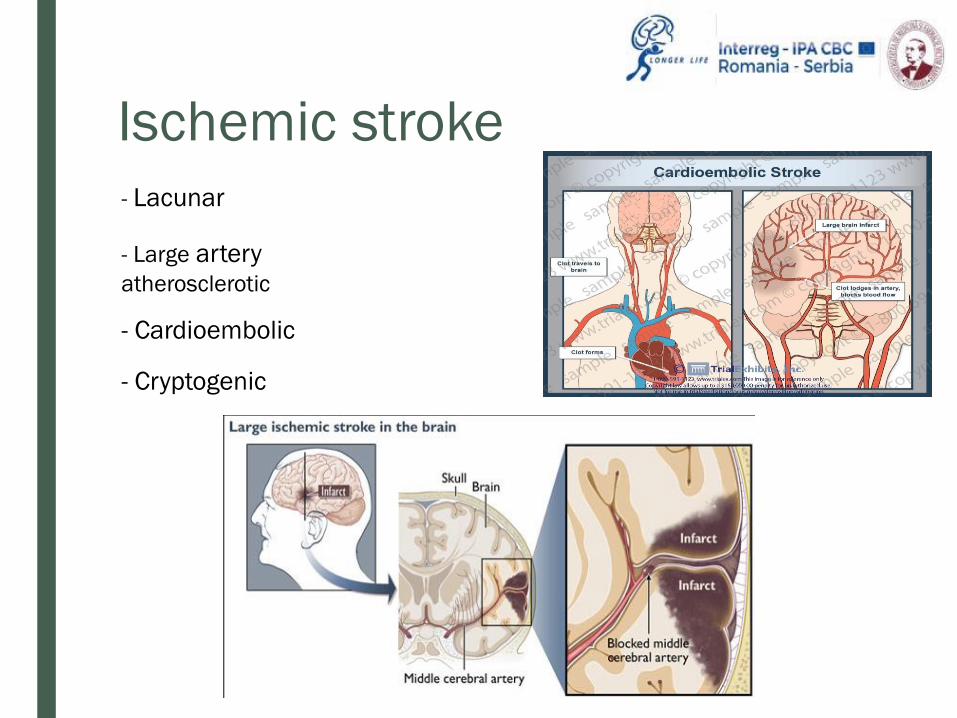
Ischemic stroke
- Lacunar
- Large arteryatherosclerotic
- Cardioembolic
- Cryptogenic

Diagnosis of Ischemic Stroke
➢ A complete neurologic examination – to localize the deficit to thecentral nervous system and inform prognosis
➢ In acute stroke – validated scales for measuring neurologicimpairment
➢ A noncontrast CT scan of the head will readily identify ICH andSAH – the initial test of choice
➢ Any patient suspected of SAH with normal CT lumbarpuncture
➢ MRI – the presence of cerebral infarction CT scan is notinformative; it can provide additional information about previousstroke or other intracranial pathology

Diagnosis of Ischemic Stroke
➢ MRI is rarely the initial imaging technique of choice
➢ CT with contrast is rarely helpful in the evaluation of brain
parenchyma
➢ Neurologic examination can provide specific neuroanatomic
localization of the stroke
➢ The examination is not sufficiently sensitive or specific to
identify the subtype of ischemic stroke vessel imaging
and cardiac evaluation are required

Diagnosis of Ischemic Stroke
■ Neurosonology

Transient Ischemic Attack (TIA)
➢ Transient focal neurologic symptoms from brain, retinal or spinalcord ischemia, was initially defined as lasting < 24 hours
➢ The absence of infarction on CT, independent of symptom duration
➢ Symptoms: are short lasting, usually 5 min to one hour
sudden-onset hemiparesis
hemisensory loss
change in speech function
loss of vision
inability to walk

TIA
➢ Patients suspected of TIA should undergo neuroimaging:noncontrast MRI (DWI, Flair) or CT within 24 hours
➢ Is considered a neurologic emergency
➢ A noncontrast CT is required to rule out hemorrhagic stroke
➢ All patients with suspected TIA expedited evaluation within48 hours, both cerebrovascular imaging and cardiac examination
➢ Patients who had a transient ischemic attack, the risk of strokeincreases as the ABCD2 score increases
➢ Hospital admission is recommended for an ABCD2 ≥ 3 or greater



Cardioembolic Stroke
➢ The most common cause is atrial fibrillation
➢ Other potential cardioembolic sources:
➢ reduced left ventricular ejection fraction
➢ severe mitral stenosis
➢ ventricular thrombus
➢ apical aneurysm
➢ congenital abnormalities
➢ Several findings on neuroimaging suggest a cardioembolic cause,such as involvement of the cortical surface in the absence ofcerebral artery atherosclerosis
➢ Cardiac evaluation: electrocardiography, in-hospital telemetry,transthoracic echocardiography, transesophageal echocardiography

Large Artery Atherosclerosis
➢ Commonly occurs after local thrombus formation in the area of
plaque rupture with subsequent distal embolization
➢ Common causes – extracranial internal carotid artery
atherosclerosis has the highest risk of recurrent stroke in the
first 2 weeks
➢ The risk is highest when the stenosis > 70%; stenosis in the 50%
to 70% range has a moderate risk of recurrence
➢ Prompt vascular imaging is recommended for patients with TIA or
a carotid territory infarction seen on neuroimaging
➢ Imaging modalities: ultrasonography, magnetic resonance
angiography (MR-A), CT-A or catheter digital subtraction
angiography

➢ Carotid ultrasonography is useful because of its high sensitivity forhemodynamically significant stenosis
➢ The anatomic location should be confirmed with either CT angiographyor MRA without contrast
➢ Unless carotid artery angioplasty with stenting is planned, catheterangiography is not routinely necessary
➢ Stoke arising from atherosclerosis of the intracranial arteries occurswith stenosis > 70% in the vertebro-basilar, intracranial internal carotidand middle cerebral arteries
➢ Intracranial atherosclerosis is associated with a high long-term risk ofrecurrent stroke

Small Subcortical Infarcts (Lacunes)
➢ Are commonly < 1.5 cm in size and arise from occlusion of
small perforating arteries emanating from the large
intracranial vessels
➢ Presents only motor or sensory findings on examination
➢ Cortical hemispheric symptoms (visual field cuts, aphasia,
hemispatial neglect are lacking)
➢ The main risk factor: hypertension associated
pathologic changes at the origin of perforating arteries
➢ Vascular imaging is required in affected patients

Cryptogenic and Rare Causes of Stroke
➢ Sizeable proportion of patients will have a cerebral infarction
with no definitive cause identified on cardiac or vascular
diagnostic testing
➢ Prolonged cardiac rhythm monitoring or interrogation of a
pacemaker may reveal undiagnosed paroxysmal atrial
fibrillation
➢ Headache preceding stroke in younger patients without
cardiovascular disease risk factors (particularly those with
recent head/neck trauma) suggests extra/endocranial
arterial dissection

➢ Testing for autoimmune and hypercoagulable disorders
➢ Echocardiography may reveal a PFO – present in up to 25% of the
general population
➢ In younger people, a PFO is likely to be causally related to stroke
(generally are at a low risk of subsequent stroke in the absence of
hypercoagulable disorder)

Acute Stroke Therapy

Ischemic Stroke Treatment
Thrombolysis
➢ The initial goal is to establish eligibility for intravenous thrombolysis
➢ The primary determinant of eligibility is the time since stroke onset – determined
by either self report or the time when the patient was last witnessed at a
prestroke baseline
➢ Thrombolysis aims to restore cerebral blood flow to the ischemic penumbra
➢ Intravenous thrombolysis is indicated
within 4,5 hours of onset in patients
with measurable deficit who do not
meet any of the exclusion criteria and
is most effective the earlier it is
administered

Thrombolysis
➢ A focused history, physical examination and a fingerstick
measurement of blood glucose level can determine any of the
exclusion criteria
➢ Rapid imaging with
noncontrast CT is required
to exclude ICH
➢ Laboratory testing: complete blood count, coagulation profile and
basic metabolic profile – suspicion of coagulopathy or
thrombocytopenia
➢ The optimal time to initiate the treatment with thrombolysis is 60
minutes or less from onset – marker of high-quality care

The guidelines state that patients should receive endovascular therapy
with a stent retriever if they meet all the following criteria (class I; level
of evidence A):
• Prestroke modified Rankin Scale (mRS) score 0 to 1;
• Acute ischemic stroke with receipt of intravenous recombinant tPA
within 4.5 hours of onset;
• Causative occlusion of the internal carotid artery or proximal (M1)
middle cerebral artery (MCA);
• Age 18 years or older;
• National Institutes of Health Stroke Scale (NIHSS) score of 6 or greater;
• ASPECTS score of 6 or greater; and
• Treatment that can be initiated (groin puncture) within 6 hours of
symptom onset.
Criteria for Eligibility for
Thrombectomy

➢ Main risk factors: protocol violations, notably treatment beyond the
time window and blood pressure above recommended targets
➢ Blood pressure <180/110 mmHg before thrombolysis – achieved
with intravenous labetalol or nicardipine
➢ After the initiation of intravenous thrombolysis using recombinant
tissue plasminogen activator, adherence to strict monitoring
protocols – blood pressure < 180/105 mmHg and to detect signs
of symptomatic ICH
➢ Other precautions – withholding all antithrombotic agents until a
repeat had CT or MRI performed within 24 hours after the
procedure excludes ICH and monitoring for angioedema

Antiplatelet, Anticoagulant and Other Agents
➢ Aspirin is appropriate – only after a dysphagia evaluation
documenting the ability to safely swallow; if unable to swallow –
rectal formulation of aspirin
➢ Aspirin taken within 48 hours of ischemic stroke onset modestly
reduces the risk of recurrent ischemic stroke at 2 weeks without
significantly increasing the risk of intracerebral hemorrhage
➢ In patients with a high-risk TIA (ABCD2 score ≥ 4) or minor
ischemic stroke (National Institute of Health Stroke Scale ≤ 3), a
21-day course of aspirin+clopidogrel or clopidogrel monotherapy
for 90 days, decrease the risk of subsequent stroke –
administrated within 24 hours of onset, compared with aspirin
monotherapy

➢ Heparinoids do not reduce the risk of recurrent stroke in the
acute setting for either cardioembolic or noncardioembolic
stroke
➢ Acute intravenous heparin occasionally is used in patients
with rare cause of stroke (dissection or a hypercoagulable
state), or in patients with mechanical valves – risk of
hemorrhage into the infarct is low

Antithrombotic Therapy After Ischemic Stroke
➢ In patients with infarcts without petechial hemorrhage and with
involvment < one third of the middle cerebral artery distribution +
atrial fibrillation, anticoagulation can be started before hospital
discharge (between 2-14 days).
➢ Warfarin is not recommended for patients with symptomatic
intracranial atherosclerosis unless another high-risk condition; is
associated with increased mortality.
➢ In noncardioembolic ischemic strokes, warfarin and antiplatelet
agents are equivalent in terms of efficacy; antiplatelet agents – are
considered first-line agents because of ease of use.

➢ For noncardioembolic stroke, low-dose (81mg/d) aspirin
monotherapy – often first-line therapy for patients not
previously taking antiplatelet agents
➢ Clopidogrel or aspirin + dipyridamole – patients who have a
recurrent ischemic stroke, despite adequate control of other
stroke risk factors, while taking aspirin monotherapy

Revascularization
either endarterectomy or stenting– in patients with > 70% stenosis and low
cardiovascular risk, as long as the operative complication rate is < 3%
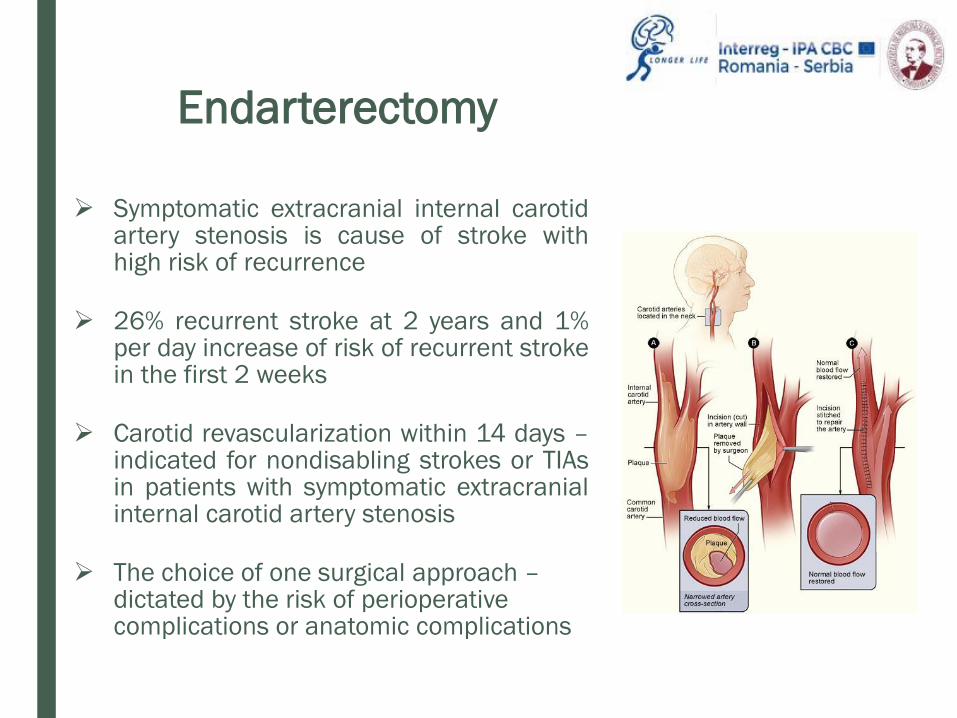
➢ Symptomatic extracranial internal carotidartery stenosis is cause of stroke withhigh risk of recurrence
➢ 26% recurrent stroke at 2 years and 1%per day increase of risk of recurrent strokein the first 2 weeks
➢ Carotid revascularization within 14 days –indicated for nondisabling strokes or TIAsin patients with symptomatic extracranialinternal carotid artery stenosis
➢ The choice of one surgical approach –dictated by the risk of perioperative complications or anatomic complications
Endarterectomy

➢ Angioplasty-stenting – performed in patients at high risk for
periprocedural cardiopulmonary complications, restenosis
and previous radiation therapy
➢ Using angioplasty-stenting – not recommended for patients
with symptomatic intracranial artery stenosis because of the
high risk of periprocedural stroke and the high efficacy of
optimal medical therapy
Angioplasty -
Stenting

Lifestyle and Medical Management
➢ Treatment of modifiable vascular disease risk factors lead to asignificant decrease in the risk of recurrent stroke.
➢ Antihypertensive therapy for stable patients with a sustainedblood pressure ≥ 140/90 mmHg, including those older > 60years with preexisting cardiovascular disease
➢ Patients with recent lacunar infarct => systolic blood pressure≤ 130 mmHg

Lifestyle and Medical Management
➢ All patients with stroke require comprehensive lifestyle changes
(improving physical activity, diet, tobacco use)
➢ Statins are recommended for patients with plasma LDL
cholesterol level ≥ 100 mg/dL (2.59 mmol/L)
➢ Statins have been associated with high risk of hemorrhagic
stroke and may be contraindicated in patients with lobar ICH –
amyloid angiopathy
➢ Statins are indicated for patients at high risk for ischemic
events

Prognosis and Recovery
Neurologic Complications

Neurologic Complications
➢ Patients with a middle cerebral artery
infarction involving > 50% of the arterial
territory – high risk for malignant cerebral
infarction with associated edema and
cerebral herniation
➢ Hemicraniectomy –associated with
significant reduction in mortality and
severe disability compared with the best
medical therapy - considered early in
patients with malignant cerebral
infarction (exhibit impaired alertness,
least one pupil reactive to light)

➢ Aspiration pneumonia can be prevented by maintaining the head
of bed at 30 degrees and instituting oral hygiene protocols
➢ DVT prevention – required for all hospitalized stroke patients
unless they are fully ambulatory
➢ Subcutaneous unfractionated or low-molecular-weight heparin –
started in al patients with impaired mobility by hospital day 1 for
ischemic stroke and by hospital day 4 (if no active bleeding is
documented) in hemorrhagic stroke




















![Conventional MRI and MR Angiography of Stroke€¦ · compared with 52% sensitivity for noncontrast CT in detecting a dense MCA sign [3]. Contrast-enhanced T1-weighted images show](https://img.dokumen.tips/doc/110x75/5b5b68bc7f8b9a24038e8e4a/conventional-mri-and-mr-angiography-of-stroke-compared-with-52-sensitivity.jpg)










