Embed Size (px)
Citation preview

1
Stockport Health and Care Outcomes
Clinical and Social Outcomes shortlist and
October Expert Reference Groups
Nov/Dec 2016

2
Contents
Section Page
Overview 3
Draft shortlist of Clinical and Social Outcomes 6
Appendix 1: Expert Reference Groups 9
ERG 1 – Healthy and Acutely Ill 10
ERG 2 – Long-term Conditions 16
ERG 3 – End of Life 22
ERG 4 – Frailty and/or Dementia 26
Appendix 2: Further Information 32

3
Outcomes Framework - High Level Plan
Population Segmentation
evidence review
Clinical and Social
Outcomes selection and
sign-off
Person-Centred
Outcomes selection and
sign-off
Draft Outcomes Framework
ready for negotiation with MCP
Outcomes Framework
version 1 part of shadow
MCP contract
June – November 2016 Dec 2016 – Feb 2017 Mar 2017 – Mar 2018
October Expert Reference
Groups
January Expert Reference
Groups

4
Overview – Clinical and Social Outcomes
• A draft shortlist of Clinical and Social Outcomes (CSOMs) has been
developed following the 4 Expert Reference Groups (ERGs) in October.
• The following slides describe the steps taken to develop the draft short-list
of Clinical and Social outcomes.
• The detailed results and comments from each of the ERGs are also
included in Appendix 1.
N.B. These outcomes are only part of the whole Outcomes Framework –
Personal Outcomes will also be developed with the Expert Reference Groups
in January, with a full set of outcomes ready by March 2017.

5
Stages to develop the Clinical and Social Outcomes
(CSOMs)
Expert Reference Groups Check and Challenge Next steps
• Long-lists of >100 CSOMs
collated by Outcomes-Based
Healthcare.
• ERGs discussed and voted on
their priority outcomes (see
Appendix 1).
• The top scoring outcomes
recommended by each ERG
were then collated and
assessed together as a whole
shortlist.
A core group of ERG Clinical Leads,
Commissioner and BI Leads, and
Healthwatch representative reviewed
the shortlisted outcomes, considering:
• Spread of outcomes / duplication;
• Initial MCP focus on the over-65
population;
• Review of Stockport’s JSNA and
RightCare priorities to identify any
gaps (see Appendix 2);
• Strategic considerations, including
health inequalities and population-
wide mortality measures.
A revised shortlist was created, with
explanation of adjustments provided
below.
The shortlist of 25 Clinical and
Social Outcomes will be reviewed
and endorsed by:
• Outcomes Steering Group
22/11
• Joint Commissioning Board
7/12
• Stockport Together Executive
Board 12/12
• Health and Care Integrated
Commissioning Board (2017)
The 25 will be taken forwards for
data analysis to produce a baseline
position for each outcome.
N.B. The final Outcomes
Framework will be subject to
contractual negotiation with the
MCP.

625 Clinical and Social Outcome Measures (draft shortlist as at 30/11/16)
Healthy (5)(whole population)
H6 Reduce total no. of
episodes of ill health
that require emergency
hospital admission for
acute conditions that
should not usually
require admission
H9 Increase people's
physical activity
H11 Reduce obesity in the
population
H12 Reduce smoking in the
population
H13 Reduce alcohol
consumption in the
population
Long-Term Conditions (9)
LTC
5Premature Mortality: Decrease
deaths in people with Serious
Mental Illness
LTC
14Reduce smoking in people with LTC
and/or disability
LTC
15Reduce obesity in people with LTCs
and/or disability
LTC
16Reduce the total number of
episodes of ill health that require
emergency hospital admission in
people with LTCs, organ failure,
and/or disability
LTC
17
Reduce the number of days disrupted
by care for people with LTCs, organ
failure, and/or disability
LTC
25
Reduce strokes in people with
diabetes and/or circulatory conditions
LTC
27Reduce the complications of
diabetes (such as stroke, MI, lower
limb amputations, end-stage renal
failure (ESRF), and blindness)
LTC
30Reduce the number of
exacerbations, per person with
organ failure, that require
emergency hospital admission
LTC
42Increase proportion of cancers
diagnosed at an early stage
Frailty and/or Dementia (8)
F8 Increase the amount of time OPwF/D
spend at their place of residence
F10 Reduce new pressure ulcers in OPwF/D
at place of residence or hospital
F11 Reduce serious falls in OPwF/D
F13 Reduce the incidence of delirium in
OPwF/D
F14 Reduce the incidence of incontinence,
urinary tract infections (UTIs) and
severe constipation in OPwF/D
F15 Reduce the prevalence gap of dementia
F17 Appropriate discharge: Reduce the
number of OPwF/D being re-admitted to
hospital as an emergency within 30
days of discharge
F22 Improve recovery following fragility
fractures back to baseline 30 and 120
days after fragility fracture
End of Life (3)
EOL1 Increase in people dying
in their preferred place of
death
EOL4 Increase the proportion of
people on the Palliative
Care Register for those
who are expected to die
within the next [12
months]
EOL7 Reduce the need for
emergency hospital care
for people in their last [4
weeks] of life
Strategic indicators to be monitored
• Age standardised mortality: decrease the overall number of people dying • Mortality measures in relation to inequality
• Reduce Potential Years of Life Lost (PYLL) from causes amenable to healthcare • Reduce prevalence gap of long-term conditions:
Hypertension, Diabetes, AF, COPD and CKD• Increase Healthy Life Expectancy
Person-Centred Outcome Measures
– to be developed in Jan/Feb 2017
The full framework will be made up of both Clinical/Social and Personal
Outcomes.

7
Key messages
Health inequalities
– Outcomes concentrated in the most deprived areas will incentivise targeted support to reduce
health inequalities (e.g. smoking and alcohol consumption).
Prevalence gap of key long-term conditions
– Increased early identification (i.e. finding those who have not yet been diagnosed) will support
improvement of outcomes for long-term conditions.
Mental health
– Dementia, serious mental illness and depression in the over 65s are included in the selected
Clinical/Social Outcomes.
– Wellbeing, anxiety etc will be prioritised in the Personal Outcomes.
– All ERGs and Steering Group have emphasised the importance of mental health alongside
physical health.
Whole population outcomes:
– ‘Healthy’ segment preventative outcomes will apply to the whole population (i.e. all ages).
– Outcomes predominantly for the under 65s will be the focus of phase 2 (SMI, employment etc).

8
Detail of adjustments
Outcomes removed (duplication):
• LTC 18 - Reduce unplanned hospitalisation for chronic ambulatory care sensitive conditions
Similar to LTC 16 as a measure of emergency admissions for similar cohorts of people – full details in Appendix 2.
Outcomes added to ERG priorities during check and challenge stages:
• LTC 17 Reduce the number of days disrupted by care for people with LTCs, organ failure, and/or disability
• LTC 25 Reduce strokes in people with diabetes and/or circulatory conditions
• F10 Reduce new pressure ulcers in OPwF/D at place of residence or hospital
• F22 Improve recovery following fragility fractures back to baseline 30 and 120 days after fragility fracture
Outcomes postponed to Personal Outcomes section:
• H15 Improve self-reported well-being (satisfaction, happiness, anxiety, life feeling worthwhile)
• F18 Improve the % of adult social care users who have as much social contact as they would like
• F19 Improve health-related quality of life for older people
Outcomes held until Phase 2 (extending outcomes framework to under 65 population):
• LTC 24 Reduce incidence of self harm/injury in people with depression and/or serious mental illness
• LTC 46 Employment for those in contact with secondary mental health services
Mortality measures:
• Mortality included as balancing measures to avoid perverse incentives. These will be monitored across the whole
population but will not have payment attached to them.

9
Appendix 1
Expert Reference Groups: votes and comments

10
ERG 1Healthy and Acutely Ill

11
11
ERG 1 Healthy and Acutely Ill – Overview
ERG1 had a clear preference for 7 of their 22 outcomes, with an emphasis on local health inequalities.
Preferred outcome groupings:• Public Health Outcome Measures (#9-14) were popular, particularly physical activity, smoking, alcohol
consumption and obesity. – The group highlighted the relationship between mental health and smoking, and suggested that people with
mental illnesses should be included as a component of this outcome.– Alcohol-related liver disease (#14) was recognised as an outlier in Stockport, although it received fewer votes
than consumption.• Healthy Life Expectancy was the preferred Mortality Measure (#1-4).
– Although recognised as problematic to measure, the group liked its correlation to other outcomes, quality of life and health inequalities.
• Self-reported well-being was the preferred social outcome (#15-17), over employment or sickness absence rates.– The latter were recognised as key influencers of physical and mental health, but could potentially be less
relevant for the over 65 population. Appropriate, safe and warm housing was also suggested as a key component of this outcome.
Least preferred outcome groupings:• There were reservations about the three outcomes relating to ‘need for emergency care’ (#5-7), but #6 was
preferred, and recognised as a measure of an integrated system focused on prevention.
– This focused on reducing emergency admissions for potentially avoidable acute conditions, including infections (ear, nose, throat, kidney and urinary tract) and heart failure.
• One discussion group suggested removing the ‘discharge from hospital’ measure (#8), as too broad and only giving a snap-shot in time.
• None of the ‘acutely ill’ segment outcomes were preferred (#18-22). These were seen as too ‘process’ focused, with participants expressing a preference of focusing on other acute conditions or vaccination rates instead.
To note:• Many ERG1 outcomes are likely to be whole population measures (rather than just ‘healthy’ segment).
• Obesity, smoking and employment outcomes were also discussed in ERG 2 to focus on people with LTC.

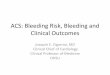
12
0
2
4
6
8
10
12
14
16
18
20
H9 H2 H12 H13 H11 H6 H15 H10 H5 H8
Vote
s
ERG 1 - Top 10 Outcomes
Top votes
Regular votes
12
ERG 1 – voting
Ref Top 10 Outcomes Top votesRegular
votesTotal votes
% of 'top 3'
votes in ERG
H9 Increase people's physical activity 12 6 18 21%
H2 Increase healthy life expectancy 10 7 17 17%
H12 Reduce smoking in the population 9 8 17 16%
H13 Reduce alcohol consumption in the population 5 12 17 9%
H11 Reduce obesity in the population 6 9 15 10%
H6
Reduce the total no. of episodes of ill health that require… emergency
hospital admission for acute conditions that should not usually require
hospital admission
5 10 15 9%
H15Improve self-reported well-being (satisfaction, happiness, anxiety, life
feeling worthwhile)4 11 15 7%
H10 Improve people's diet and nutrition 2 3 5 3%
H5Reduce the total no. of episodes of ill health that require... emergency
hospital admission and/or A&E attendance0 5 5 0%
H8Reduce the number of discharges of people, who are back in hospital on
day 30 after discharge3 0 3 5%
No. of long-list outcomes 22
Total number of people voting 22
Total votes per person 7
No. of ‘top votes’ per person 3

13
ERG 1 – voting continued
Ref Remaining Outcomes Top votesRegular
votesTotal votes
% of 'top 3'
votes in ERG
H14Reduce serious illness requiring emergency hospital admissions in
people with alcohol-related liver disease0 3 3 0%
H17 Reduce sickness absence rates 0 3 3 0%
H22* Improve outcomes from planned treatments (hip replacement, knee
replacement, groin hernia, varicose veins) 0 3 3 0%
H16 Increase employment rates 0 2 2 0%
H18* Reduce deaths within 30 days following a hospital admission for
pneumonia and/or influenza 1 1 2 2%
H3 Increase life expectancy 1 1 2 2%
H19 * Reduce length of hospital admissions for pneumonia and/or influenza 0 2 2 0%
H20* Reduce readmissions in people who have needed hospital admissions
for pneumonia and/or influenza 0 2 2 0%
H4Reduce Potential Years of Life Lost (PYLL) from causes amenable to
health care0 1 1 0%
H7Reduce the total no. of episodes of ill health that require... readmission to
hospital as an emergency within 30 days of discharge0 1 1 0%
H1 Overall (crude) mortality: decrease the overall number of people dying 0 0 0 0%
H21* Reduce deaths within 30 days following emergency hospital admission
for trauma and/or injury 0 0 0 0%
TOTAL 58 90 148
*Outcomes related to Acutely Ill Segment

14
ERG 1 – detailed comments
Top Outcomes ERG Comments
General comments: Health inequalities must be considered – mentioned frequently in relation to top outcomes - 9, 2, 12, 11.
H9 Increase people's physical activity• Highest voted outcome – supports mental health and wellbeing, as well as all aspects of people’s lives.
• Also impacts on life expectancy of older people.
H2 Increase healthy life expectancy • The group liked the emphasis on 'healthy', not just 'life expectancy‘.
• Recognised that this is problematic to measure but highly correlated with other measures.
H12 Reduce smoking in the population • Group emphasised the relationship between mental health and smoking, and that people with mental
illnesses should be included as a component of this outcome.
H13Reduce alcohol consumption in
the population
• Discussion – is the better measure alcohol use or liver disease? This received more votes than #14
(emergency admissions for alcohol-related liver disease) which was described as a lag indicator and H13
being more preventative and broader.
• Comment to include drug consumption.
• Should be applied across the whole population, although issue of data availability to be explored.
H11 Reduce obesity in the population • Useful measure, and must consider health inequalities. Preferred to #10 (diet and nutrition).
H6
Reduce the total no. of episodes
of ill health that require…
emergency hospital admission for
acute conditions that should not
usually require hospital admission
• One table described this as the “best of a bad bunch” for ‘outcomes relating to need for Emergency Care’ (#5,
6, 7), which were seen by some as processes not outcomes.
• Others recognised this as a good measure of an integrated system – i.e. the whole system working well,
including strong prevention to avoid emergency admissions.
• Should consider physical and mental wellbeing.• Comments on other acute conditions and services e.g. speed of testing, increasing GP accessibility, reducing
urgent care demand in primary care etc.
H15Improve self-reported well-being
(satisfaction, happiness, anxiety,
life feeling worthwhile)
• Group highlighted importance of community wellbeing / combatting isolation e.g. people living on their own.
Links with personal outcomes – mental wellbeing, feelings of ‘being in control’, and number of social contacts.
• Mental wellbeing is crucial; Stockport has a comparatively high level of prescribing medication for people with
mental health problems - need to incentivise more talking therapies.
• Comment to include 'appropriate, safe, warm housing’ as an outcome. • WEMWEBs as a measure
• Recognition that this is self-reported via surveys so difficult to measure accurately.

15
15
ERG 1 – detailed comments continuedRef Remaining Outcomes ERG Comments
H10 Improve people's diet and nutrition• Obesity (#11) preferred. Difficult to measure - BMI and smoking are measurable.
• Influenced by access to affordable food and social networks.
H5Reduce total no. of episodes of ill health that require...
emergency hospital admission and/or A&E attendance
• Would measure admissions for all people, including those with LTC – focus on LTC in ERG2
outcomes.
H8Reduce the number of discharges of people, who are back
in hospital on day 30 after discharge
• Only gives a snapshot – difficult to relate to a specific group e.g. frequent fliers/ frail.
• One table recommended to remove this outcome.
H14Reduce serious illness requiring emergency hospital
admissions in people with alcohol-related liver disease• Recognised as an outlier in Stockport.
H17 Reduce sickness absence rates • Includes acute episodes of mental-health related issues. Is this less relevant for >65s?
H22Improve outcomes from planned treatments (hip /knee
replacement, groin hernia, varicose veins)
• People often complain about the quality of the joint replacement.
H16 Increase employment rates • Strong link to health outcomes, but is volunteering more relevant for >65s?
H18Reduce deaths within 30 days following a hospital
admission for pneumonia and/or influenza
• Some disliked this measure – preferred to focus on identification. However, some saw it as
helpful - deaths are often because adults with pneumonia are not being seen quickly enough,
so earlier diagnosis and treatment would be needed to achieve this outcome.
H3 Increase life expectancy • Problematic to measure
H19Reduce length of hospital admissions for pneumonia
and/or influenza
• Agree generally, but not in its current form - would prefer outcome on vaccination rates.
• Adults with pneumonia are not seen quickly enough.
• Disliked this measure
H20Reduce readmissions in people who have needed hospital
admissions for pneumonia and/or influenza• Disliked this measure - admission rates to be reviewed.
H4Reduce Potential Years of Life Lost (PYLL) from causes
amenable to health care
• Problematic, but useful measure.
H7
Reduce the total no. of episodes of ill health that require...
readmission to hospital as an emergency within 30 days of
discharge
• Disliked this measure - not just within 30 days, some are beyond. Too ‘process’ focused.
H1Overall (crude) mortality: decrease the overall number of
people dying• Problematic to measure.
H21Reduce deaths within 30 days following emergency
hospital admission for trauma and/or injury
• Possible to reduce trauma but difficult to prevent death within 30 days.
• Neck of femur patients - Allstrick assessment

16
ERG 2 Long-Term Conditions

17
17
ERG 2 LTC overview
Overview of Outcome groupings:
• Over 80% of the ERG voted to address premature mortality in people with serious mental illness (even though this outcome applies predominantly to those aged under 65). A concern was flagged that this outcome could lead to increased use of medication for people with SMI.
– Other Mortality Outcomes (#1-13) were generally unpopular, with only #9 and 10 (reducing under 75 mortality from liver disease and cancer) gaining a couple votes.
• Risk factor outcomes (#14/15) relating to obesity and smoking in people with LTC were also common votes, with
links to mortality / liver disease / cancer mortality noted. A respondent queried the impact on over 65s with LTC.
• Of the Acute outcomes (#18-24, 49-51), #18 was the favourite: ‘reducing unplanned hospitalisation for chronic ambulatory care sensitive conditions’, for which Stockport is in the worst quartile nationally.
– These conditions include: infections, diabetes, blood diseases, dementia, convulsions and epilepsy, cardiovascular disease and respiratory conditions.
• The group generally preferred broader outcomes over specific conditions (of the 14 LTC in scope). An exception to
this was early diagnosis of cancer (#42), as well as complications relating to diabetes (#27) from #25-29, where comments drew out the need for integrated provision for co-morbidities.
• Outcomes relating to disruption by care (#16-17) both made the top 10, as patient-centred outcomes. #16 favoured in the votes as a broad measure to reduce emergency admissions across all 3 population segments. The
discussion was balanced between avoiding admissions, attendances and repeat attendances, as well as length of stay / disruption by care.
• For Segment 7 outcomes (#30-33), the broadest outcome #30 was favoured to reduce exacerbations requiring emergency admission for all people with organ failure, with the group keen to promote early management to
avoid admission.

18
18
ERG 2 LTC overview - continued
Key themes from the ERG:
• Discussion about social outcomes relating to employment and housing (even though these may be less relevant
to the >65s population), reflected the ERG’s focus on the importance of mental health outcomes. Top 15 votes included #24, 46, 48 and 13 in order: reducing self-harm, employment, appropriate accommodation and reducing suicide rate, although many participants said they would prefer to include a more general measure to focus specifically on people with mental illness.
• Personal outcomes were discussed as a crucial underpinning to many of these clinical and social outcomes. For the over 65 population, the importance a sense of purpose and reducing social isolation was highlighted (whether by employment or other community involvement).
• Some people found it difficult to make the link between outcome measures that describe acute settings (e.g.
emergency admissions) with the need for a system-wide approach to achieve the outcomes (e.g. quality community services).
• Although areas of high local performance (e.g. stroke) or low prevalence (e.g. learning disabilities in the over 65s)
were not prioritised, the ERG still recognised their importance.
• The voting shows a few clear priorities from the ERG, but the top 8-12 were relatively evenly spread. A view across all the ERGs will help to clarify the number of outcomes from this ERG.

19
0
2
4
6
8
10
12
14
LTC5 LTC27 LTC18 LTC30 LTC16 LTC15 LTC42 LTC14 LTC24 LTC17
Vote
sTop votes
Regular votesERG 2 LTC – voting
Ref Top 10 OutcomesTop
votes
Regular
votes
Total
votes
% of 'top 3'
votes in ERG
LTC5 Premature mortality: decrease deaths in people with Serious Mental Illness (SMI) 9 5 14 15%
LTC27Reduce the complications of diabetes (such as stroke, MI, lower limb amputations, end-
stage renal failure (ESRF), and blindness)11 1 12 18%
LTC18 Reduce unplanned hospitalisation for chronic ambulatory care sensitive conditions 5 4 9 8%
LTC30Reduce the number of exacerbations, per person with organ failure, that require
emergency hospital admission5 4 9 8%
LTC16Reduce the total number of episodes of ill health that require emergency hospital
admission in people with LTCs, organ failure, and/or disability.4 5 9 7%
LTC15 Reduce obesity in people with LTCs and/or disability 3 5 8 5%
LTC42 Increase proportion of cancers diagnosed at an early stage 4 3 7 7%
LTC14 Reduce smoking in people with LTCs and/or disability 3 3 6 5%
LTC24Reduce incidence of self harm/injury in people with depression and/or serious mental
illness2 4 6 3%
LTC17Reduce the number of days disrupted by care for people with LTCs, organ failure, and/or
disability3 2 5 5%
No. of long-list outcomes 51
Total number of people voting 17
Total votes per person 8
No. of ‘top votes’ per person 4

20
Ref Remaining OutcomesTop
votes
Regular
votes
Total
votes
% of 'top 3' votes
in ERG
LTC46 Employment for those in contact with secondary mental health services 3 1 4 5%
LTC48Adults in contact with secondary mental health services who live in
stable and appropriate accommodation2 3 5 3%
LTC34 Reduce emergency admissions for people with learning disability 1 3 4 1%
LTC49 Reduce deaths within 30 days following a hospital admission for stroke 0 4 4 0%
LTC19 Reduce acute symptoms related to diabetes control 1 2 3 2%
LTC13 Reduce suicide rate 1 1 2 2%
LTC45 Employment for those with learning disabilities 1 1 2 2%
LTC44 Employment for those with LTCs 0 2 2 0%
LTC9 Reduce under 75 mortality from liver disease 0 2 2 0%
LTC10 Reduce under 75 mortality from cancer 1 0 1 2%
LTC47Adults with a learning disability who live in stable and appropriate
accommodation1 0 1 2%
Outcomes with one ‘regular’ vote: 2, 3, 6, 21, 23, 25, 26, 28, 29, 31, 39, 40, 51
Outcomes with zero votes: 1, 4, 7, 8, 11, 12, 20, 22, 32, 33, 35, 36, 37, 38, 41, 43, 50
TOTAL 60 68 128
ERG 2 LTC – voting continued • Arthritis
• Asthma• Atrial Fibrillation
• Cancer• Cardiovascular
Disease (stroke)
• Chronic Kidney
Disease• COPD
• Coronary Heart Disease (MI)
• Depression
• Diabetes
• Epilepsy• Heart Failure
• Hypertension• Serious Mental
Illness
Reminder of 14 priority LTC in scope:

21
Ref Outcomes ERG Comments
LTC5Premature mortality: decrease deaths in people
with Serious Mental Illness (SMI)
• The only mortality outcome that was chosen (LTC1-13).
• Mental health measures need to consider education, information & life circumstances.
• Need to think about communication, prevention and language.
• Concern this outcome could lead to increased use of medication for people with SMI.
LTC27
Reduce the complications of diabetes (such as
stroke, MI, lower limb amputations, end-stage
renal failure (ESRF), and blindness)
• Co-morbidities should be provided for in a 'one-stop' fashion.
• Sharing information is essential - need the system to talk to each other.
• Concern that some of these will take a long time to come through e.g. amputations, hence
difficult to change in a reasonable timeframe.
• Good outcome because having diabetes often leads to many other health problems.
LTC18Reduce unplanned hospitalisation for chronic
ambulatory care sensitive conditions• Feels more like a process?
LTC30
Reduce the number of exacerbations, per
person with organ failure, that require
emergency hospital admission
• Only outcome chosen relating to Segment 7 (serious organ failure) from LTC 30-33.
• Can only achieve these outcomes by managing it early, in the community without the need for
admission.
LTC16
Reduce the total number of episodes of ill
health that require emergency hospital
admission in people with LTCs, organ failure,
and/or disability
• Acute exacerbations for any LTC
• Admissions are preventable and avoidable
• What is the impact on service users who worry about 'wasting‘ services’ time?
• Difference between admissions, attendances and chronic attendances.
• Balance between acute and LoS (LTC 17 – days disrupted by care).
LTC15Reduce obesity in people with LTCs and/or
disability
• Lifestyle risk factors – both obesity and smoking voted for (#14 and 15).
• Links also with # 1 (crude mortality), #9 (<75 mortality from liver disease), and #10 (<75
mortality from cancer)
• How much difference will this outcome make to >65s with a LTC?
LTC42Increase proportion of cancers diagnosed at an
early stage
LTC14Reduce smoking in people with LTCs and/or
disability
• See LTC 15. Prefer personal reported outcomes as needs are different.
• Life expectancy for this group is improving
• What about carers, health checks and Learning Disabilities?
LTC24Reduce incidence of self harm/injury in people
with depression and/or serious mental illness• Often related to recession i.e. employment, and usually in younger people.
LTC17Reduce the number of days disrupted by care
for people with LTCs, organ failure, disability• Patient-centred. Very important outcome from a patient perspective – currently poor
communication between primary and secondary care.
ERG 2 – detailed comments

22
ERG 3End of Life

23
23
ERG 3 EOL - overview
The ERG had a clear preference for three outcomes: #1, 4 and 7:
• #1 was the top voted outcome due to its emphasis on empowerment, choice and control. However, the ERG recognised the challenge to accurately capture a person’s preferred place of death, particularly as this can change over time and be influenced by disease/frailty.
– Until preferred place of death is routinely recorded and linked with actual death, a proxy measure must be used. Based on evidence that the majority of people do not wish to die in hospital, a pragmatic measure in the first instance is the total number of deaths in hospital compared to total number of deaths overall.
• #4 to increase people on the Palliative Care Register was recognised as a helpful measure to support the achievement of better outcomes by identifying the population cohort early enough to put in place appropriate planning and support.
– The ERG expressed a strong desire for the PCR to be more effective, built into contracts and centred on MDTs. There was recognition that the PCR can have a variable impact in practice, but that identifying the people in need of palliative care and support was an important first step.
• #7 was preferred as a broad outcome, rather than a specific focus on pain control or respiratory infections (#8/9).
– This outcome measures total number of emergency admissions in the last weeks of life, when emergency care requiring hospital admission should ideally be kept to the minimum possible. The group recognised some emergency care is genuinely required and unavoidable, but felt reducing inappropriate access could be achieved by increasing proactive support in the community.
• The ERG recorded a particular dislike for #2. Although a nationally recorded measure, a third of respondents had concern that this data would capture sudden death and misrepresent discharge to care homes.
• The ERG also felt that Patient Reported Outcome Measures may be more relevant for this population group.

24
ERG 3 End of Life – voting
Ref Outcome Top votesRegular
votes
Total
votes
% of 'top’ votes
in ERG 3
EOL1 Increase in people dying in their preferred place of death 6 13 19 55%
EOL4Increase the proportion of people on the Palliative Care Register for
those who are expected to die within the next [12 months]5 14 19 45%
EOL7Reduce the need for emergency hospital care for people in their last
[4 weeks] of life0 14 14 0%
EOL5Increase the time spent at home/place of residence in people in their
last [4 weeks] of life0 2 2 0%
EOL6Reduce the need for emergency hospital care for people on the
Palliative Care Register0 2 2 0%
EOL2 Increase in people dying in their usual place of residence 0 0 0 0%
EOL3Reduce the number of deaths in hospital from residents of care
homes0 0 0 0%
EOL8Reduce emergency hospital admissions for respiratory infections in
people in their last [4 weeks] of life0 0 0 0%
EOL9Reduce emergency hospital admissions for pain control in people in
the last [4 weeks] of life0 0 0 0%
TOTAL 11 45 56
No. of long-list outcomes 9
Total number of people voting 19
Total votes per person 3
No. of ‘top votes’ or “stars” per person 10
2
4
6
8
10
12
14
16
18
20
EOL1 EOL4 EOL7 EOL5 EOL6
Vote
s Top votes
Regular votes

25
25
Ref ERG Comments
General comments – want to understand what the ‘building blocks’ to achieving the outcomes are.
EOL1
‘Increase in people dying in their preferred place of death’
• Top voted outcome due to emphasis on empowerment, choice and control.
• Challenge to capture/ accurately measure personal preference - CSF register needs to be recorded and regularly updated.
• Personal preference can change – how to manage this in practice?
• Place of death is influenced by disease/frailty. Also good symptom control e.g. if family are struggling then preferred place may change.• Need resources to enable this – can be limited by social care / lack of carers.
EOL4
‘Increase the proportion of people on the Palliative Care Register for those who are expected to die within the next [12 months]’
• Popular vote – ERG emphasised need for an effective palliative care register centred on MDTs.
• Important that the PCR is useful as it defines the cohort – want it to be incorporated into contracts.
• Increasing registered people is not technically an outcome, but helpful proxy that supports the achievement of other outcomes.
• Debate in the ERG about how effective the register is: – Variable impact on care in practice – can be just a ‘tick-box’
– Used effectively it helps to identify deteriorating course and brings people together to discuss support and plan appropriate care.
– Need useful definitions of ‘care’ and ‘support’ for the register.
• Wording: suggestion to focus on ‘effective Gold Standard Framework’, rather than ‘proportion’.
EOL7
Reduce the need for emergency hospital care for people in their last [4 weeks] of life
• Preferred over EOL8 & EOL9 which are closely related.
• Wording: instead of 'reduce need', suggestion to have 'reduce inappropriate access'' – need to differentiate between appropriate access.
• How will this be measured?
• Achievable by increasing support, e.g. out of hospital palliative care 24/7.
EOL5 • Time spent at home - benefit of increasing patient control, but this received few votes.
EOL6 • Responses suggested this outcome could be fairly subjective, and were unclear how to measure ‘need’.
EOL2
• Dying in usual place of residence is a nationally recorded measure.
• However, a third of respondents highlighted that they would definitely not want this outcome included.
• Concern that the data captures sudden death, and misrepresents discharge to care home.
• Potential overlap with ERG4 - this outcome is generally worse if the person is frail.
EOL3• No votes specific to care homes – preferred increase time spent at home/residence than number of deaths in hospital.
• Potential benefit of more control for the person.
EOL8
EOL9
• No votes – some concern that these could become a perverse measure.
• EOL 7 was preferred to a specific focus on pain control or respiratory infections.
ERG 3 End of Life – comments

26
ERG 4 Frailty and Dementia

27
27
ERG 4 Frailty and Dementia overview
• None of the mortality outcomes (#1-4) were a key priority, as the ERG preferred to focus on quality of life over mortality. Of these, #3 (reduce excess winter deaths) was of most interest.
• Improved out of hospital support for people with dementia and/or frailty was a key theme of discussion, reflected in votes for outcomes seen as indicators of joined up care and preventative support across the system:
– #8 was the highest voted outcome of the ERG, emphasising time spent at home (#5-8). As well as being patient-centred, it was seen as a measure for appropriate integrated care and improved communication, but needs to be balanced with necessary admissions during the initial “window of opportunity” where appropriate.
– #6 and 7 were variants of a measure to reduce emergency admissions (#6/7). Taken together, these would move into contention for 8th place on the shortlist.
– Similarly, appropriate and sustainable discharge (#16/17) to reduce hospital readmissions were both
highlighted, with a slight preference for readmissions within 30 days of discharge over 91 days of discharge.
– However, some expressed concern that addressing admissions would not necessarily lead to better care for people at home.
• Complications of frailty (#9-14) were of high priority for the ERG. The reduction of serious falls, delirium and incontinence/UTIs/severe constipation all gained high votes. They were recognised as being closely related to each other, with significant impact on quality of life and needing increased preventative education. Delirium during treatment for hip fracture (#21) was also the most popular of the acute outcomes.
• Almost half of the ERG chose reducing the prevalence gap of dementia as a regular vote but not top 3 priority. Comments also asked how to address the time between diagnosis and follow-up.
• Outcomes related to well-being and quality of life (#18/19) were also popular, with ERG emphasis on social
isolation, awareness of care needs and prevention of deterioration, despite limitations of the NASCS survey.
• The voting revealed some higher priorities, but the top 8-12 outcomes were relatively evenly spread.

28
ERG 4 Frailty/Dementia voting
Ref Top 10 Outcomes (ordered by total votes)Top
votes
Regular
votes
Total
votes
% of 'top 3'
votes in ERG
OPwF8 Increase the amount of time older people with frailty and/or dementia spend
at their place of residence
13 7 20 22%
OPwF11 Reduce serious falls in older people with frailty and/or dementia 7 8 15 12%
OPwF13 Reduce the incidence of delirium in older people with frailty and/or dementia 7 6 13 12%
OPwF19 Improve health-related quality of life for older people 7 5 12 12%
OPwF14 Reduce the incidence of incontinence, urinary tract infections (UTIs) and
severe constipation in older people with frailty and/or dementia
5 7 12 8%
OPwF17 Appropriate discharge: Reduce the number of older people with frailty and/or
dementia being re-admitted to hospital as an emergency within 30 days of
discharge
3 9 12 5%
OPwF15 Reduce the prevalence gap of dementia (reducing the gap between people
diagnosed with dementia, and the estimated number of people with dementia)
2 10 12 3%
OPwF16 Sustainability of discharge: Reduce the number of older people with frailty
and/or dementia who are back in hospital on day 91 after discharge
2 6 8 3%
OPwF3 Reduce excess winter death rates 1 7 8 2%
OPwF21 Reduce the incidence of delirium who are undergoing treatment for hip
fracture
1 6 7 2%
No. of long-list outcomes 22
Total number of people voting 22
Maximum votes per person 7
No. of ‘top votes’ per person 3
02468
101214161820
Vo
tes
Top votes
Regular votes

29
ERG4 Frailty/Dementia voting continued
Ref Remaining OutcomesTop
votes
Regular
votesTotal votes
% of 'top 3'
votes in ERG
OPwF18 Improve the percentage of adult social care users who have as much social
contact as they would like
1 5 6 2%
OPwF10 Reduce new pressure ulcers in older people with frailty and/or dementia at
place of residence or in hospital
2 3 5 3%
OPwF6 Reduce the emergency hospital admissions rate per older person with frailty
"emergency admission- overall rate measure"
3 1 4 5%
OPwF7 Reduce the rate of emergency hospital admissions per admitted older person
with frailty - "emergency admission- readmission measure"
3 1 4 5%
OPwF9 Reduce potentially avoidable infections (C Difficule, MSSA, MRSA, E Coli) in
older people with frailty and/or dementia
1 2 3 2%
OPwF4 Increase life expectancy at age 75 0 2 2 0%
OPwF5 Reduce the proportion of older people with frailty requiring at least one
emergency hospital admission - "emergency admission- population proportion
measure"
0 2 2 0%
OPwF22 Improve recovery following fragility fractures back to baseline 30 and 120
days after fragility fracture
1 0 1 2%
OPwF1 Overall crude mortality - decrease the number of people dying in older people
with frailty and/or dementia
0 1 1 0%
OPwF12 Reduce fragility fractures in older people with frailty and/or dementia 0 1 1 0%
OPwF2 Age of death - increase the average age of death in older people with frailty
and/or dementia
0 0 0 0%
OPwF20 Reduce deaths within 30 days after hip fracture 0 0 0 0%
TOTAL 59 89 148

30
Top Outcomes ERG Comments
8 Increase the amount of time OPwFD
spend at their place of residence
• Top-voted outcome for this group - seen as a measure for appropriate care.
• A few commented that care at home should include regular GP reviews.
• Improving communication between disciplines will ease worry about treating people out of hospital.
• Linked to #17 (reduce emergency readmissions within 30 days of discharge).
• Some admissions are necessary in people with frailty or dementia – first 4 days as the ‘window of opportunity’.
11 Reduce serious falls in OPwFD • Loss of confidence after a fall linked to an increase demand on services (rehab, primary & community care).
• Keen to incentivise preventative agendas (including nutrition and exercise).
13 Reduce the incidence of delirium in
OPwFD
• Delirium was highlighted as having a significant impact on quality of life.
• Close links between #13 and #14 i.e. delirium and incontinence/UTIs/severe constipation (hydration).
• Delirium is observed by families and often not picked up by clinicians.
• Education for prevention of delirium is needed.
14 Reduce incidence of incontinence, UTIs
and severe constipation in OPwFD
• From a patient perspective, these issues have a huge impact on people’s quality of life – very important
outcome
• Close links with #13 above.
• If managed well, would impact on #16 (sustainable discharge).
19 Improve health-related quality of life for
older people
• Emphasised social isolation and prevention of future deterioration, which needs increased awareness
of care needs, expectations etc.
• Several comments on limitations of the annual NASCS (survey) - currently only sent to individuals who
have care packages, and needs to be expanded and more frequent.
• Links with #18 (social contact in adult social care users), and #4 (increase life expectancy at age 75).
17 Appropriate discharge: Reduce no. of
OPwFD being re-admitted to hospital
as an emergency within 30 days of
discharge
• Indicator of joined up care - need to support preventative action.
• Linked to #8 (time spent at residence) and #16 (sustainable discharge).
• Danger that sorting out hospital admissions won’t necessarily lead to better care – how can we improve
people’s care at home?
15 Reduce the prevalence gap of
dementia
• Already a national focus
• Need to address the time between diagnosis and follow-up .
• How quickly can dementia be picked up when a patient presents to A&E without a carer?
ERG 4 Frailty / Dementia – detailed comments

31
Outcomes ERG Comments
16 Sustainability of discharge: Reduce
the number of OPwFD who are back
in hospital on day 91 after discharge
• Indicator of joined up care and requires system-wide partnership working to achieve.
• Suggestion to combine #16 and #17.
• Closely related to management of continence and hydration (links with #14).
3 Reduce excess winter death rates • Preferred mortality outcome (out of 4) if pushed to choose.
• Moderately frail people can be extremely affected by winter and need practical support.
• Other mortality outcomes (#1-4): why increase life expectancy – should be about quality > quantity.
21 Reduce the incidence of delirium
who are undergoing treatment for
hip fracture
• Concern about the increasing frequency of incidence.
• Suggestion to combine #20 and #21 (reduce deaths within 30 days after hip fracture).
Other Outcomes
9 Reduce potentially avoidable
infections (C Difficule, MSSA,
MRSA, E Coli) in OPwFD
• Already measured nationally.
• Some cynics – hospital contact increases risk but antibiotic resistance is a quick fix.
10 Reduce new pressure ulcers in
older people with frailty and/or
dementia at place of residence or in
hospital
• Long recovery time-frame.
• Need to educate carers to prevent incidence.
ERG 4 Frailty / Dementia – detailed comments continued

32
Appendix 2Further Information

33
Indicative segment information
Segment CriteriaEstimated number of
people over 65 yrs% Total
1Healthy
No diagnosis 14,255 24.6%
3 Acutely Ill Not available
4
Long-Term
conditions
Arthritis, Hypertension, CHD,
Stroke /TIA, Depression, HF, AF, COPD, Asthma, CKD,
Diabetes, Epilepsy, Cancer, SMI
42,366 73%
5 Serious DisabilityLD, Downs Syndrome,
Sensory disability, Mobility Impairment
2,300 4%
6 End of Life Not available
7Limited Reserve
and ExacerbationsNot available
8Frailty and/or
DementiaDementia, HisFall 7,738 13.3%
Total >65 population
in Stockport = 57,966
Estimates taken from JSNA GP data analysis

34
LTC for over 65s
ConditionNo. of
>65s
% of people
with condition
who are >65
Chronic Kidney Disease (CKD) 6,948 90.3%
Atrial Fibrillation (AF) 4,984 84.4%
Heart Failure (HF) 2,321 82.5%
Stroke or Transient Ischaemic Attack (TIA) 4,897 78.7%
Coronary Heart Disease (CHD) 9,302 75.6%
Chronic Obstructive Pulmonary Disease (COPD) 4,827 69.4%
Cancer 5,087 63.7%
Hypertension 27,556 63.2%
Rheumatoid Arthritis (16+) 828 55.9%
Diabetes 8,255 55.7%
Epilepsy 577 24.2%
Severe mental health 551 22.6%
Asthma 4,427 22.2%
Depression (18+) 4,073 15.6%
Learning disability 93 6.2%
Cerebral palsy 14 5.1%
Downs syndrome 4 1.7%
Autism 11 1.2%
Total >65 population 55,600

35
Priorities indicated in RightCare (all ages)
Trauma and Injuries
Gastro-intestinal
Maternity
Mental Health
Musculoskeletal
As taken from the RightCare “Where to Look” pack for October 2016, under the ‘Outcomes’ heading on page 13.
This outcome priority includes the following
quality measures:
• Mortality from accidents all ages;
• Injuries due to falls in people aged 65+;
• Unintentional and deliberate injury
admissions, 0-24 years;
• All fracture admissions in people aged 65+.
This outcome priority includes the following
quality measures:
• Mortality for liver diseases under 75 years;
• Alcohol specific hospital admissions;
• Emergency admissions for alcoholic liver
disease condition (19+)
• Admissions for C related end-stage liver
disease/HCC;
• Reported C-Diff cases.
Not relevant as only analysing over-65 population for ST in phase 1 of outcomes.
This outcome priority includes the following
quality measures:
• Physical health checks for patients with SMI;
• Mental health hospital admissions (quarterly
opportunity);
• Emergency hospital admissions for self-
harm;
• Mortality with dementia 65+;
• Rate of emergency admissions aged 65+
with dementia.
This outcome priority includes the following
quality measures:
• % patients 75+ years with fragility fracture
treated with BSA;
• Hip replacement emergency readmissions 28
days;
• % fractured femur patients returning home
within 28 days;
• Hip fracture emergency readmissions 28
days.
Text highlighted in green indicates where
outcomes are linked to these priorities

36Priorities indicated in Joint Health and Wellbeing Strategy/JSNA
Stockport Health Needs
Stockport Health Priorities
As taken from the Stockport Joint Health and Wellbeing Strategy 2017-20, pages 6-8 – the Stockport Health Needs and Priorities are taken from the
Stockport JSNA
Overview:• Stockport has oldest age profile in Greater
Manchester – currently 19.4% people are
aged 65+, likely to rise to 21.8% by 2024, an
additional 9,681 people.
• Cancer most common cause of death
(causing 29% of all deaths and 42% of early
deaths; 40% of cancer is preventable).
Key facts – health determinants:• 18% smoke (41% in Brinnington).
• 26% drink unhealthily (7,000 alcohol related
admissions per year).
• 25% are obese (62% are overweight or
obese).
Key facts – mortality causes:• 2,700 deaths a year.
• 29% of cancer; 28% of heart disease; 14%
of lung disease.
Key facts – LTCs:
• 43,000 with hypertension.
• 19,600 with asthma.
• 14,200 with diabetes (17+).
Key facts – mental wellbeing:• 16,400 with depression (18+).
• 2,400 with dementia.
• 2,400 with psychosis.
The overall objectives for health and
wellbeing in Stockport are to improve life
expectancy and reduce health inequalities.
For all ages:• Increasing levels of physical activity as an
effective preventative action at any age.
• Focus on improving healthy life expectancy
for all as the priority, focusing especially in
the most deprived areas.
• Continue work to integrate and improve
care systems, especially minimising the use
of unplanned hospital care.
For Ageing Well:• Supporting healthy ageing across
Stockport, recognising that preventative
approaches that promote self care and
independence are essential at every life
stage.
• Aim to prevent and delay the need for care
whilst responding to the complexity of needs
that older people with multiple long term
conditions may have.
• Continuing to improve the identification of
and support available to those with dementia
and their carers.
Text highlighted in green indicates where
outcomes are linked to these priorities

37
Removal of LTC 18 (duplicate)
Assessment of LTC 18, 30 and 16• LTC18 – Unplanned hospitalisation (emergency admissions) for chronic ACS conditions
• LTC 16 – Emergency admissions for people with LTCs, disability and/or organ failure
LTC16 and LTC18 are similar in that they measure total number of emergency admissions (admissions rate) for similar cohorts of
people.
Both LTC16 and LTC18 include:
• Asthma, Heart Failure, Diabetes, COPD, Angina/Chronic IHD, HTN, Epilepsy
Conditions exclusive to LTC16:
• Arthritis, AF, Cardiovascular Disease, Learning and Physical Disabilities, Neurological end stage disease (MND, Parkinson’s,
MS), CMD, CKD
Conditions exclusive to LTC18:
• Chronic viral hep B, anaemia, and dementia
Due to the overlap, we would recommend selecting one of these and not both.
• LTC18 is defined by the NHS as including those conditions that are more amenable to proactive management. Since it’s a national measure, there will also be benchmark data available. However, it is possible to look at this outcome for people
aged 65 and over (in which case, benchmark data is unavailable as the NHS measure looks at all people including children).
• LTC16 will give greater coverage and includes all conditions defined by Stockport’s segmentation work.
LTC30 – Average number of exacerbations per person with organ failure, that require emergency hospital admission
This is different from LTC16 and LTC18 primarily because it’s a frequency of admissions measure (rather than a pure admissions
rate measure). i.e. it will be an average number of emergency admissions per year, for people in segment 7 only.
• Important to note, that information used to define segment 7 (e.g. to exclude mild forms of COPD, heart failure and so on) is
principally held in primary care, so although a value can be obtained from SUS data alone, a more accurate value can be obtained with primary care data access.