Embed Size (px)
DESCRIPTION
Citation preview

Brought to you by
Improving Clinical Outcomes Through TechnologyHow Six Sigma and Business Intelligence Support CAMC Initiatives for Reducing Medication Reconciliation Failure Rates

Thank You to Our Sponsor
The outcomes achieved by the Siemens customers described herein were achieved in the customers’ unique setting. Since there is no “typical” hospital and many variables exist (e.g., hospital size, case mix, level of IT adoption), there can be no guarantee that others will achieve the same results.

How to Participate
• Submit your questions in the GoToWebinar presentation window.
• This webinar will be recorded and available for download a few days after the webinar. The slides will also be available.

About the Panel
Karen Miller, RN, MSN, MBA; Lean Six Sigma Director; Master Black Belt; Charleston Area Medical CenterKaren Miller has over 20 years’ experience in healthcare administration, program development and project management with proven expertise in the ability to create strong functional teams for the development and execution of quality and cost improvement projects. She supervises, manages, coordinates, and integrates quality initiatives and process improvement activities to facilitate achievement of organizational goals at Charleston Area Medical Center system using Lean Six Sigma tools, methodologies and philosophy. She reports to and works closely with the Chief Quality Executive and administrators to effectively initiate and manage change.
Janet Hickman, R.T. (R),(N)(ARRT), NMTCB; Systems Analyst, Siemens Managed ServicesI’ve worked in the healthcare industry for over 38 years and am currently employed by Siemens Managed Services as a DSS System Analyst. I am based at Charleston Area Medical Center (CAMC) and act as the DSS team lead. Before working for Siemens, I was employed by CAMC as a Decision Support Consultant, Laboratory System Analyst, Nuclear Medicine Technologist, and Radiologic Technologist.
Janet M. Kennedy, ModeratorJanet M. Kennedy , CMD is the Director of Marketing and Digital Strategy for Health Vue, a big data analytics firm working in healthcare. Janet creates and presents webinar and in-person social media training for healthcare organizations through a partnership with EHR2.0. She is also the host of “Get Social Health” a podcast about social media for healthcare. Follow her @GetSocialHealth.

At the conclusion of this presentation participants should be able to: Describe the Define, Measure, Analyze, Improve, and Control
(DMAIC) Six Sigma methodology and benefits Describe the key role Healthcare Intelligence (HI) plays in the
measure phase Describe how information technology, Six Sigma, and clinical staff
collaborate to develop clinical documentation, work lists, and education for process changes
Describe how to develop and use Crystal reports to monitor improvements and maintain projects in control
Objectives
5

Charleston Area Medical Center Non-profit, 908-bed, 4-campus
teaching hospital system and tertiary regional referral center
Servicing 557,328 mostly rural population
550,000+ outpatient visits 100,000+ ED visits 40,600+ Cancer Center Visits 38,000+ inpatient discharges 5,000+ employees 600+ physicians 500+ health professional students
daily
Memorial Hospital
6
General Hospital

Charleston Area Medical Center Primary Stroke Center of Excellence Bariatric Surgery Center of
Excellence Heart & Vascular Center of
Excellence 9,469 cardiac cath procedures 1,289 open heart bypass procedures
Level I Trauma Center Only free standing Women &
Children’s Hospital in state Level III Neonatal Intensive Care Unit 3,000+ births
Women & Children’s7
Teays Valley

Six Sigma Methodology
DMAIC: To improve any existing product or process
DefineDefine MeasureMeasure AnalyzeAnalyze ImproveImprove ControlControl
Who are the customers and what are their priorities?
How is the process performing and how is it measured?
What are the most important causes of the defects?
How do we remove the causes of the defects?
How can we maintain the improvements?
8

Six Sigma MethodologyDMADV : To redesign a bad process by improving the
average and variation in the process
DefineDefine MeasureMeasure AnalyzeAnalyze DesignDesign VerifyVerify
Who are the customers and what are their priorities?
How is the process performing and how is it measured?
What are the most important causes of the defects?
How do we design or redesign a process with minimal defects?
How do we verify that the design meets the goal?
9

Allocation of Six Sigma Resources 8 full time black belts Online request for complex problem solving
Request must include scoped problem statement, aligned strategic goal, and estimated Return on Investment (ROI)
Online requests are presented by Vice Presidents at monthly executive meetings
Start dates are determined and assigned based on current workload and strategic priorities
Chief Information Officer frequent requestor of resources
10

Define Phase
Identify key stakeholders Executive sponsor, physician champion, and team
members assigned Concise problem statement and business case Team defines and prioritizes possible causes of problem
Brainstorming and fishbone diagrams
Six Sigma assigned staff contacts Healthcare Intelligence for data
D M A I C
11

Define Example: Medication Reconciliation
D M A I C
Project Start Date: January 2011Executive Sponsor: CQOProject Process Owner: CMOPhysician Champions: Medicine, Hospitalist, and Information Services Clinical DirectorsMaster Black Belt: Karen MillerTeam Members: CPOE Design Team, Information Services, Transcription Services
Project Description/Problem Statement:Discharge medication list defects account for 50% of the total Center for Medicare & Medicaid Services (CMS) discharge instructions defects.
Project Scope: Discharge medication reconciliation CMS indicators:1. Provider dictated discharge summary
medications match discharge meds ordered2. Med list given to patient match physician
discharge meds ordered3. Documentation med list given to patient Alignment:
Strategic Vision Pillar: Best place to receive patient centered careStrategic Goal: Evidenced Based Care/ CMS Reliability TJC standards: CMS Congestive Heart Failure (CHF) discharge instruction indicator
What is the project business case? Patient Safety: Incomplete discharge medication reconciliation contributes to readmissions, patient mortality and morbidity. Financial: Part of Meaningful Use criteria for potential $6 million.
12

Define the Current ProcessD M A I C
Physician uses Home & Current Medication Order form that prints from Soarian® to order meds
Key Takeaway: Defining the current process identifies the data elements required for the measure phase and is the basis for discussion with Healthcare Intelligence resource staff
Physician uses home med and clarification lists to order meds by circling continue or discontinue?
Physician only uses physician blank order form and writes discharge meds?
Physician uses Med Administration Check™ to identify inpatient meds?
Nurse adds, deletes, and revises discharge med list based on discharge orders from multiple forms
Physician dictates discharge summary up to 30 days past discharge
Physician uses multiple forms to dictate medications in summary 13

Measure Phase Develop Excel document for data elements needed for the
Analyze Phase Meet with Healthcare Intelligence resource to explain the
project business case and expected outcomes Suggestions made for additional data elements Many of the data elements can usually be supplied by Decision
Support Revise data collection plan and send to Healthcare
Intelligence resource
Key Takeaway: Often I don’t know all data elements needed or available until my project team member asks “would you want to know this”?
D M A I C
14

Healthcare Intelligence Resource Compares data in Soarian® and Data Warehouse for
availability of each data element Helps team to import new Soarian data into warehouse if needed Validates data by comparing warehouse data to Soarian
Sends draft data to Six Sigma Six Sigma reviews data with team members and
collaborates if revisions are needed Approval received by Six Sigma to develop report Final report formatted in Excel and sent to Six Sigma for
statistical analysis
D M A I C
Key Takeaway: Frequent communication and collaboration required to meet customer needs 15

Analyze Phase
Warehouse Excel data copied to statistical software for data analysis
Data elements supplied by warehouse allow for segmentation
Segments targeted in the improvement phase for cycles of change Physician department, nurse department, time, admission source,
documenter names, etc. Example: 72% of defects were physician discharge summary
dictation of med lists and 46% of those were Hospitalists
D M A I C
Key Takeaway: Healthcare Intelligence data helps identify root causes of defects
16

Improve/Design Phase
Process mapping of future state and potential failure identification
Identify pros/cons for different options Potential failure mitigation strategies using electronic
documentation and workflows Identify education needs for process changes Implement pilots for tests of change Meet with BI people to develop data for analysis of pilots Spread of successful improvements/design
D M A D V
D M A I C
17

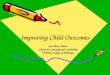
Improve/Design Outcomes Dictated provider discharge summary medication lists
matching the discharge orders is now at 2.68% defects compared to 34.21% with baseline data, which represents a 92% decrease in defects. Initially targeted Hospitalists and spread success
D M A D V
D M A I C
18
10-1
3
07-1
3
04-1
3
01-1
3
10-1
2
07-1
2
04-1
2
01-1
2
10-1
1
07-1
1
11-1
0
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Audit Date
Pro
port
ion
_P=0.0268
UCL=0.0893
LCL=0
Baseline
Hospitalists
All Physicians
Automation
Tests performed with unequal sample sizes
Provider Discharge Med Reconciliation Defects by Stage
Electronic DC Instructions

Improve/Design Outcomes Decrease in provider dictated discharge summary med
defects resulted in improvement of discharge med reconciliation CMS compliance
D M A D V
D M A I C
19

Control/Verify Phase
Development of monitoring reports to obtain outcome data Example: Physician CHF discharge summary Web Publishing
report Discharge department, status, account number, patient
name, admission and discharge date/time, discharge med list date/time, person completing med list, discharge summary date/time, physician completing, attending physician at discharge
Development of control plan Handoff to operations
D M A I C
D M A D V
20

Implementation of Electronic Medication Collection, Admission & Discharge Reconciliation
Address physician concerns about home medication collection
Address defects from nursing transcription of discharge med orders to the patient discharge med list
Executives chartered team consisting of physicians, nurses, pharmacists, IS, and Six Sigma Defined the problem Measured the current process for med collection and admission
reconciliation by completing process mapping Analyzed risks
D M A D V
D M A I C
21

Improve/Design Phase: Electronic Medication Reconciliation Implementation Multidisciplinary team collaboration Future state process mapping Risk identification and mitigation strategy
28 process issues identified for mitigation 21 of the 28 were new process issues for mitigation
Pilot on large medicine nursing department Feedback and redesign of process Education prioritization based on risks
D M A D V
D M A I C
22

Future State Process Risks: Electronic Discharge Med Reconciliation
Risk: Med reconciliation not completed. Solution: Alert when discharge order placed.
Risk: Duplicate inpatient and home med ordered.Solution: Default by drug sort.
Risk: Chooses inpatient home med instead of “house icon” med – prints on med list to stop home med and then start same med.Solution: Default by drug sort “house "first.
Risk: Provider adds new med under Soarian orders instead of Discharge Med ReconciliationSolution: Education, monitoring, & feedback.
Risk: Meds added in “complete” status – how will nurse know when to print? Solution: Nurse alert if DMR changed after placed in a “complete” status.
D M A D V
D M A I C
23

Risk Mitigation Implementation Strategies
Training for nurses, physicians, pharmacists Mandatory computer based training
Whole house adoption on a single day Pre loading inpatients home med list on the morning of
the conversion Two weeks of live support including Six Sigma staff Job Instructional Training (JIT) competency validation within one
month of go-live Development of 13 Single Point Lessons (SPL) placed at work
stations for visual aids
D M A D V
D M A I C
25

DMR Single Point Lesson D M A D V
D M A I C
26

Control/Verify Example Developed home med collection entry tips for high frequency problems
associated with expansive Soarian drop down menus (51% OTC meds) Web Publishing reports for daily and weekly nurse and individual provider
defect monitoring for performance management Cycles of analysis and improvements implemented from home med list
collection report 50% of patients admitted through EDs
58% of ED home med lists had missing required med components Implemented LPN home med collection in EDs resulting in 3-5%
missing required med components, representing a 131% improvement
Weekly data patient file for CHF chart audits and monthly control charts for CMS medication compliance sent to administration
D M A I C
D M A D V
27

Web Publishing Reports
Daily report for home med list completion and completion within 4 hours of admission percentages
Daily report for home meds missing required components that need corrections before discharge reconciliation
Weekly report for identification of nurses using free text and entry of home meds with missing components for follow up
Weekly report for physician completion rates for discharge medication reconciliation between 8:00 a.m. – 5:00 p.m.
D M A I C
D M A D V
28

D M A I CD M A D VPatient Home Med List
Key Takeaway: Executive patient data view for medications entered on the home medication list
% patients with completed status Home Med List (HML) % patients with free text meds on HML% patients with a required med component missing on HML (excludes free text)
% meds with required med component missing on HML
29

Patient Home Med List
Key Takeaway: Drill down to department level data to identify patients currently in the department that need home med list corrections
D M A I CD M A D V
30

Patient Home Med List
Key Takeaway: Drill down to patient to identify home med lists that need correction for hospitalization continuity of care and prep for discharge reconciliation
D M A I CD M A D V
31

Patient Home Med ListPatient location nurse dept and location HML collected
Missing required components on HML
Key Takeaway: Drill down to patient med components that need corrected
D M A I CD M A D V
32

Home Med Collection
Key Takeaway: Executive view for home med list collection performance management
D M A I CD M A D V
33

Home Med Collection
Key Takeaway: Drill down to department then to nurse/provider data for performance management
D M A I CD M A D V
34

% patients with HML not completed
Key Takeaway: Drill down to department then to nurse data for timeliness performance management
Home List Completion
% patients with HML not completed within four hours of admission
D M A I CD M A D V
35

Provider Discharge Reconciliation
Key Takeaway: Executive view of provider completion rates
% with Discharge Med Reconciliation (DMR) in complete status and any status
% initial DMR entry by physician or midlevel% last DMR entry by physician or midlevel% initial DMR entry by Privately Employed RN (PERN)% final DMR entry by Privately Employed RN (PERN)% initial DMR entry by staff RN% final DMR entry by staff RN% final DMR entry by staff RN 5:00 p.m. – 8:00 a.m.
D M A I CD M A D V
36

Provider Discharge Reconciliation
Key Takeaway: Medical Affairs and medical staff leadership view for provider completion rates
D M A I CD M A D V
37

Provider Discharge Reconciliation
Key Takeaway: Drill down to physician for identification of top performers, performance management and credentialing
D M A I CD M A D V
38

Six Sigma and Healthcare Intelligence Projects
Nursing admission assessment
Skin assessment/actions Fall assessment/actions Severe sepsis Telemetry classifications ED wait times and boarder
hours Patient discharge call
backs
Glucose value < 60 Consult orders Mortality Complications and
comorbidities Readmissions DRG physician detail Case mix index ALOS by nursing
department
Key Takeaway: 71 current Web Publishing reports being used for Six Sigma projects 39

Healthcare Intelligence Resources Benefits Access to100% of patient population Eliminate manual data abstraction for key elements Decrease measure phase time Improve analysis for critical variables Sustain gains after improvements
Key Takeaway: Collaborating with BI team member improves efficiency & effectiveness in all project phases
I ask the impossible and Healthcare Intelligence delivers! I simply couldn’t do my job without them!
40

Six Sigma Benefits
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 $-
$20,000,000
$40,000,000
$60,000,000
$80,000,000
$100,000,000
$120,000,000
$140,000,000
Financial Impact2001 - 2012
Cumulative Total Annual Improvements
Key Takeaway: $132,603,856 over 11 year period with $13 million in expenses. Net ROI of $119,603,856.
41

Questions ?
42