Embed Size (px)
Citation preview

STEREOTACTIC BREAST BIOPSY
Smriti Hari Associate Professor of Radiology
All India Institute of Medical Sciences New Delhi

Percutaneous Breast Biopsy
Ultrasound guided biopsy
Mammographic (Stereotactic) biopsy
MRI guided biopsy
Modality selection depends on
Visibility of the lesion
Operator preference

Principle of Stereotactic Imaging

Stereotactic imaging - Requirements
Stereo pair
Reference point
Computer

Scout image

Stereo Pair
+ 15 degrees - 15 degrees

Parallax- apparent shift of the lesion
+ 15 degrees - 15 degrees
Scout (0 degree)

Stereotactic Biopsy- Equipment
Add-on erect unit
Advantages
Cost
Space
Efficiency
Disadvantages
Access to some calcifications limited
Vasovagal episodes

Advantages
Improved access to microcalcifications in all locations
Patient comfort
Disadvantages
Cost
Space
Efficiency
Stereotactic Biopsy-Dedicated Prone Table

Stereotactic biopsy-
Careful mammographic interpretation
Planning the procedure
Informed consent
Performing the biopsy
Specimen radiography
Clip placement
Post procedural care
Assessment of histopathological concordance
Follow up imaging

Careful mammographic interpretation
Is there an indication for biopsy BIRADS 4/5 lesions
Selected BIRADS 3 lesions
Is the lesion only visible in mammography Microcalcifications
Subtle masses
Architectural distortion
Is the lesion amenable to stereotactic biopsy

Stereotactic biopsy- Limitations
Very thin breast(< 3cm compressed thickness)
Lesions close to skin
Subareolar lesions
Posterior lesions

Planning the procedure
What to target
Target on the worse looking calcifications
What approach
Shortest distance from skin to lesion

Informed consent
Performing the biopsy
Understanding the equipment
Positioning
Targetting
Needle placement errors
Acquiring samples

Hologic MultiCare Platinum and Atec Biopsy System

•360°Access
Cranio Caudal Approach
Caudo-Cranial
Approach
Lateral Approach

Reference Point
Where 3 axes (x, y, & z) intersect at right angles
0 0
50
0
+25 -25
Z axis

Positioning

Breast should be in the centre of the hole

Only one breast otherwise loss of lateral tissue

Before rotating C-arm, move breast away from the breast platform to avoid painful twisting

Positioning
Pull in lateral breast tissue
Sweep in superior breast tissue
Stabilize with both hands while bringing in the compression paddle

Positioning
There should be no gap b/w the breast and breast platform –loss of posterior tissue
Elevated inframammary fold

Positioning
Pt positioned with area of interest in the Bx window
Be alert for pt motion Mark the corners of targeted
area
Take scout image

Scout view – Straight On
Reposition if the lesion is not imaged in the center of the window















Targeted Inferior

Mulit-Pass




Targeted off the line

Targeted inferior



Scout view – Stereo Pair

Confirm reference point

Target the lesion

Transmit the target coordinates


Targeted Inferior

Stroke vs. Stroke Margin
The distance the probe moves forward starting in the cocked position to the fired position.
STROKE
The distance from the probe tip to the detector/breast platform once fired.
STROKE MARGIN

STROKE MARGIN FORMULA
T (compression thickness)
+12mm (paddle thickness)
-Stroke (biopsy device)
-Pre-fire (Z value – pull back of instrument)
= Stroke Margin

Stroke and Stroke Margin
Compression Thickness
Compression Plate Detector or Breast Platform
12 mm
Target

Compression Thickness
Compression Plate
Detector or Breast Platform
12 mm
Target
Pre-Fire
Stroke and Stroke Margin

Compression Thickness
Compression Plate
Detector or Breast Platform
12 mm
Target
Pre-Fire Post-Fire
Stroke Stroke Margin
Stroke and Stroke Margin
Stroke Margin should always be positive

Correcting Negative Stroke Margin
Compression Thickness
Compression Plate
Detector or Breast Platform
12 mm
Target
Reposition from opposite angle
Pre-Fire

Correcting Negative Stroke Margin
Compression Thickness
Compression Plate
Detector or Breast Platform
12 mm
Target
Pre-Fire Post-Fire

Correcting Negative Stroke Margin
Compression Thickness
Compression Plate
Detector or Breast Platform
12 mm
Target
Don’t dial in as far for Pre-Fire
Adjusted Pre-Fire e.g., -4
Original Pre-Fire
-2

Correcting Negative Stroke Margin
Compression Thickness
Compression Plate
Detector or Breast Platform
12 mm
Target
Pre-Fire Post-Fire

SHORT CUT FORMULA FOR
STROKE MARGIN CALCULATION
Z + (variable) must be less than or equal to compression

Set up the biopsy device
Disinfect the skin
Attach the biopsy device
Move to Z position
Align needle tip to reference point
Z-zero the needle

Vacuum assisted Biopsy Device

Needle insertion
Move to target Move the needle close to
the skin Inject LA and make a skin
nick Advance the needle into
the breast using the Z dial until the Z differential has been met
Take pre-fire images Evaluate needle position

Prefire images

Pre-fire Position
-15 +15
x x
Pre-fire Pullback -2

Is the Needle in the Correct Position?
• Pre-fire & Post-fire Needle Position – Is the Needle Aligned to the Lesion?
– Is the Needle in the Correct Position?
– Has the Lesion Moved?
– How Do I Correct the Situation?

How Do We Know We Have A Needle Error ?
Select view stage cursors to
determine lesion/patient movement
Retarget if concerned about the position of the lesion





X or Horizontal Error
Sampling should be increased between 12 and 6 o’clock going through 3 o’clock

X or Horizontal Error
Sampling should be increased between 12 and 6 o’clock going through 9 o’clock

Y or Vertical Error
Sampling should be increased between 9 and 3 o’clock going through 12 o’clock

Y or Vertical Error
Sampling should be increased between 9 and 3 o’clock going through 6 o’clock

Z or Depth Error
The depth must be increased by advancing the probe

Z or Depth Error
The depth must be decreased by pulling back the probe

Fire the biopsy gun
Take post-fire images
Evaluate needle position

Post Fire

Post Exam

Post-fire Position
-15 +15
x x

Obtain multiple tissue cores
Take post-biopsy stereo images


Specimen Radiography
Confirms calcification retrieval
Caner can be missed, if calcification is not demonstrated* Miss rate 1% with retrieval
11% without retrieval
Recommended for US guided biopsies also
*Radiology 2004;233:251-54

VAB: Marker Clip Deployment
Deployed at the end of VAB If complete removal of lesion is
expected
If biopsy diagnosis is cancer, metallic clip facilitates hook wire localization
Also recommended prior to chemotherapy in LABC For any size of mass

Clip placement


Images for Documentation
Scout (straight on)
Scout (stereotactic pair)
Pre-fire (stereotactic pair)
Post-fire (stereotactic pair)
Specimen radiograph
Post clip placement
Post procedure mammogram (two view)

Post Procedure
Light compression at biopsy site (not at the puncture site) for 10 minutes
Patient to avoid strenuous ipsilateral arm movements for 24 hours (lifting, pushing)
Observe for local bleed/ breast enlargement
Complications of breast biopsy are rare Bleed, hematoma, infection Vasovagal attack

Misdiagnoses can be minimized Accuracy depends on showing representative
microcalcifications on specimen X-ray
Histology must be correlated with imaging
If biopsy results do not match expectation (imaging histology discordance) Re-biopsy
Malignancy in up to 33%*
Surgical excision, if high risk lesion on biopsy Malignancy in up to 31%#
Two years follow-up of benign biopsy results
*Breast Cancer Res Treat 2007;101:291-97
#Am J Surg 2006;192:534-37

Take Home Message
Accurate and reliable breast biopsy can be performed using stereotactic technique
All biopsy results must be correlated with imaging. If results are not concordant - follow up!
Radiologist should be responsible for initiating, performing and auditing results of image guided breast

Problem lesions
Lesions near the chest wall

Lesions near chest wall
Pt relaxed
Vigorous breast traction and firm compression
Arm through hole
Helps with lateral lesions
Remove the table pad
Helps with medial lesions
Arm through hole with special angled compression paddle

Special Positioning Techniques

Drop the shoulder in to view axillary tissue

Compression ~55 mmCompression ~55 mm
Compression ~55 mmCompression ~55 mm
Superficial lesion Pre-fire
Superficial lesion Post-fire

Thin breast – petite needle Pre-fire
Thin breast - petite needle Post -fire
Compression
~25 mm
Compression
~25 mm
Compression
~25 mm
Compression
~25 mm

Bolstering to increase compression thickness

Rolling towards breast platform while applying compression


Easing the breast to bring in posterior tissue
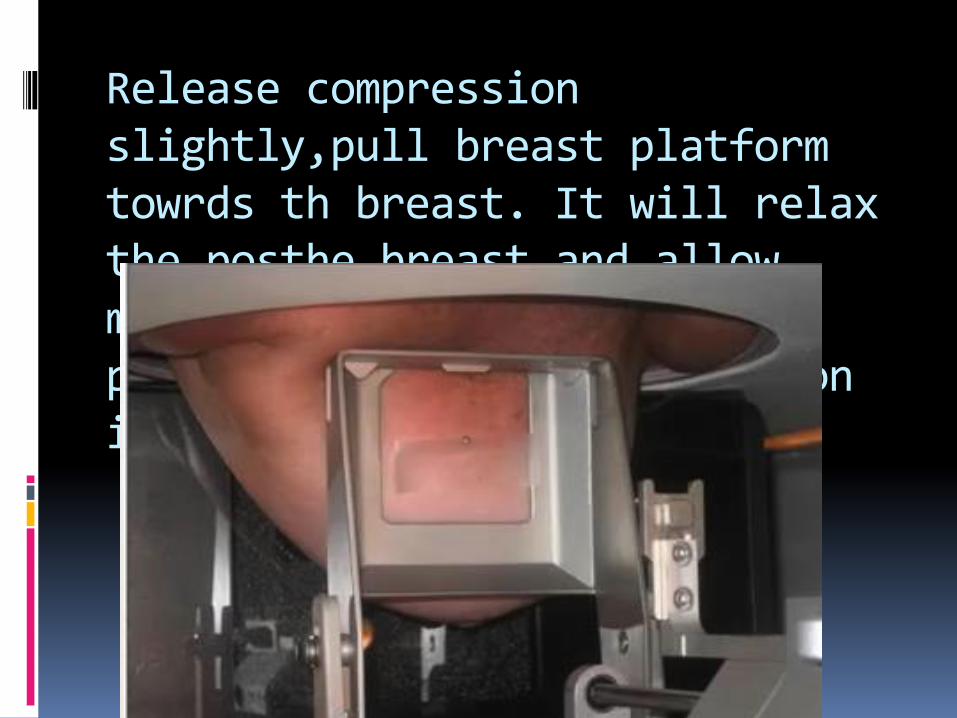
Release compression slightly,pull breast platform towrds th breast. It will relax the posthe breast and allow more posterior tissue to be pulled in before recompression is reapplied





























