Embed Size (px)
Citation preview

State of the State: Viral Hepatitis in Tennessee
Tennessee Charitable Care NetworkDecember 1, 2017
Carolyn Wester, MD, MPH / Medical Director HIV/STDs/Viral Hepatitis
Learning Objectives
• Review the definition and epidemiology of viral hepatitis
• Recognize co-morbidities related to Tennessee’s HCV epidemic
• Review the HCV Continuum of Cure
• Identify key successes in developing a statewide response to the prevention and control of HCV
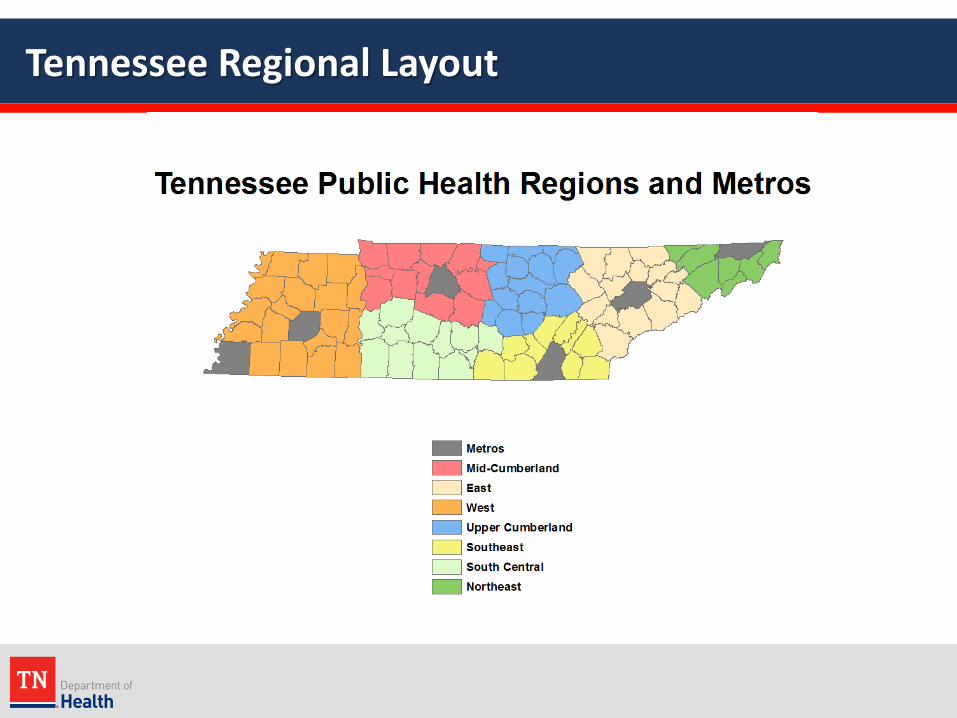
Tennessee Regional Layout

Tennessee Department of Health
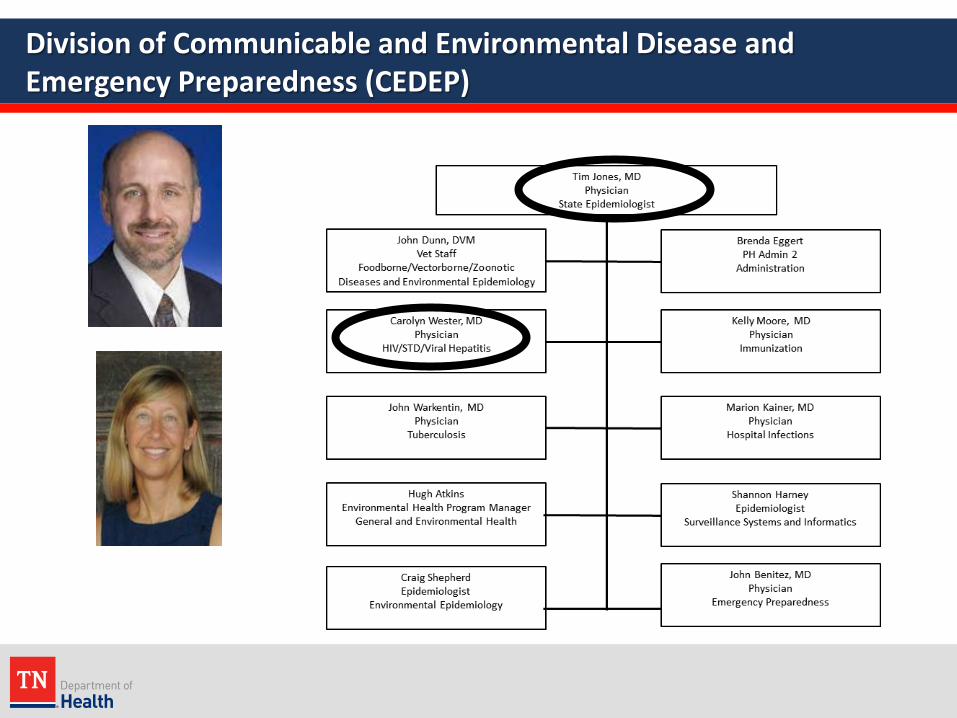
Division of Communicable and Environmental Disease and Emergency Preparedness (CEDEP)

HIV/STD/Viral Hepatitis
Dr. Meredith Brantley


Viral Hepatitis Overview
https://www.cdc.gov/hepatitis/resources/professionals/pdfs/abctable.pdf

Hepatitis B (HBV)

Incidence of Acute HBV (U.S. and 3 Appalachian States, 2006 – 2013)
MMWR, Jan 2016

Reported Cases of Acute HBV in Tennessee
http://www.cdc.gov/hepatitis/statistics/2015surveillance/pdfs/2015hepsurveillancerpt.pdf* per 100,000 population
2011 2012 2013 2014 2015
US case rate* 0.9 0.9 1.0 0.9 1.1
cases 2,903 2,895 3,050 2,953 3,370
TN case rate* 3.0 3.7 4.0 3.5 3.7
cases 192 240 262 232 243
rank 3rd 3rd 3rd 3rd 2nd

Hepatitis C (HCV)

HCV: Burden of Disease
• 3.5 Million Infected– Seroprevalence
• Birth cohort represents ~75% cases (b: 1945-1965)– New Infections
• Driven primarily by IDUs (<30 years old, white, male and female,non-urban)

The Natural History of HCV
Cirrhosis may take >20 years to develop but can be faster in the presence of immunodeficiency or alcohol use
These statistics do notapply to HIV/HCV or HBV/HCV co-infected patients
www.cdc.gov/hepatitis/HCV
Modes of Transmission of HCV
• Injection Drug Use– ~ 50% people living with HCV in U.S. are associated w/ IDU
• Healthcare-Associated– 239 outbreak-associated cases reported to CDC 2008-2015
• Perinatal– HCV mono-infected mother: ~6% transmission risk
• Sexual– Low risk among discordant heterosexual couples– HIV (+) MSM 8x higher risk than HIV (-) MSM
• Other– Non-injection drug use, unregulated tattoos
CDC, Division of Viral Hepatitis, 107 Webinar 02/23/2017

Who Is At Risk For HCV?
• Hepatitis C is usually spread when blood from a person infected with HCV enters the body of someone who is not infected– It is 10 times more infectious than HIV– It can live outside of the body for up to 30 days
• HCV can be transmitted by: – contact with objects that have even small amounts of infected blood
on them (syringes, snorting straws, medical equipment, personal items),
– unsanitary piercing or tattooing equipment, – unprotected sex, – mother-to-child transmission,– blood transfusion or organ transplant prior to 1992,– hemodialysis, and/or– occupational exposure

Signs and Symptoms of HCV
• Symptoms of early (or acute) viral hepatitis include:– Fever, headache, malaise, anorexia, nausea, vomiting, diarrhea, and
abdominal pain
• Signs of early (or acute) viral hepatitis include:– Yellowing of skin or eyes (jaundice) and/or,– Elevated liver enzymes (ALT > 200)
Note: HCV has an incubation period of up to 6 months and >70% of acutely infected persons are asymptomatic

Screening Process
1 For persons who might have been exposed to HCV within the past 6 months, testing for HCV RNA or follow-up testing for HCV antibody is recommended. For persons who are immunocompromised, testing for HCV RNA may be considered.
2 To differentiate past, resolved HCV infection from biologic false positive for HCV Ab, testing with another HCV Ab assay may be considered. Repeat HCV RNA testing if the person testing is suspected to have had HCV exposure within the past 6 months or has clinical evidence of HCV disease, or if there is concern regarding the handling or storage of the test specimen.
Source: CDC. MMWR 2013;62(18)

The Syndemic of Acute HCV and Opioid Abuse(< 30 year olds in 4 Appalachian States)
MMWR, May 2015

Reported Cases of Acute HCV in Tennessee
2011 2012 2013 2014 2015
US case rate 0.4 0.6 0.7 0.7 0.8
cases 1,229 1,778 2,138 2,194 2,436
TN case rate 1.3 2.0 1.5 1.9 2.6
cases 83 129 98 123 173
rank 4th 4th 6th 5th 4th
http://www.cdc.gov/hepatitis/statistics/2015surveillance/pdfs/2015hepsurveillancerpt.pdf* per 100,000 population
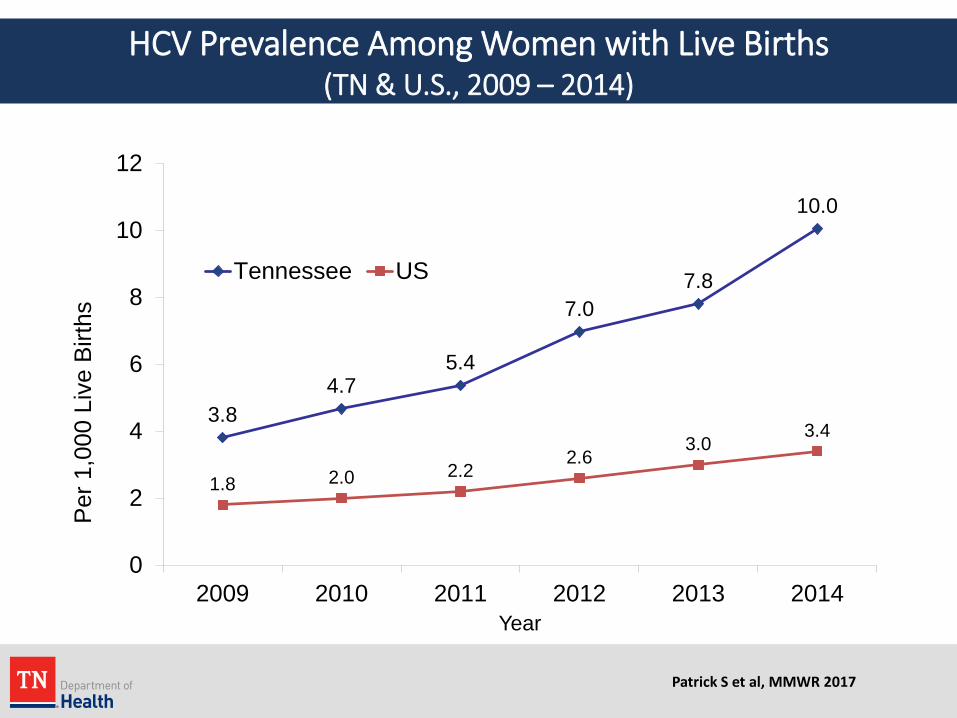
HCV Prevalence Among Women with Live Births(TN & U.S., 2009 – 2014)
3.84.7
5.4
7.07.8
10.0
1.8 2.0 2.22.6
3.03.4
0
2
4
6
8
10
12
2009 2010 2011 2012 2013 2014
Per 1
,000
Liv
e Bi
rths
Year
Tennessee US
Patrick S et al, MMWR 2017

HCV Prevalence Among Women with Live Births (2014, TN by county, unpublished data)
Patrick S et al, MMWR 2017

Intersection of Epidemics
Opioid Abuse
Hepatitis C HIV

HIV and HCV Coinfection
• According to the CDC, about 25% of HIV-infected persons in the US are also infected with HCV
• Among IDUs, the co-infection rate is estimated to be anywhere from 50-90%
• HIV/HCV co-infection causes liver damage to progress more rapidly in infected persons
http://www.cdc.gov/hepatitis/populations/hiv.htm

HIV disease by status and year of diagnosis (TN, 2005-2015)
954 939972
996
712753
923
784
865861 852
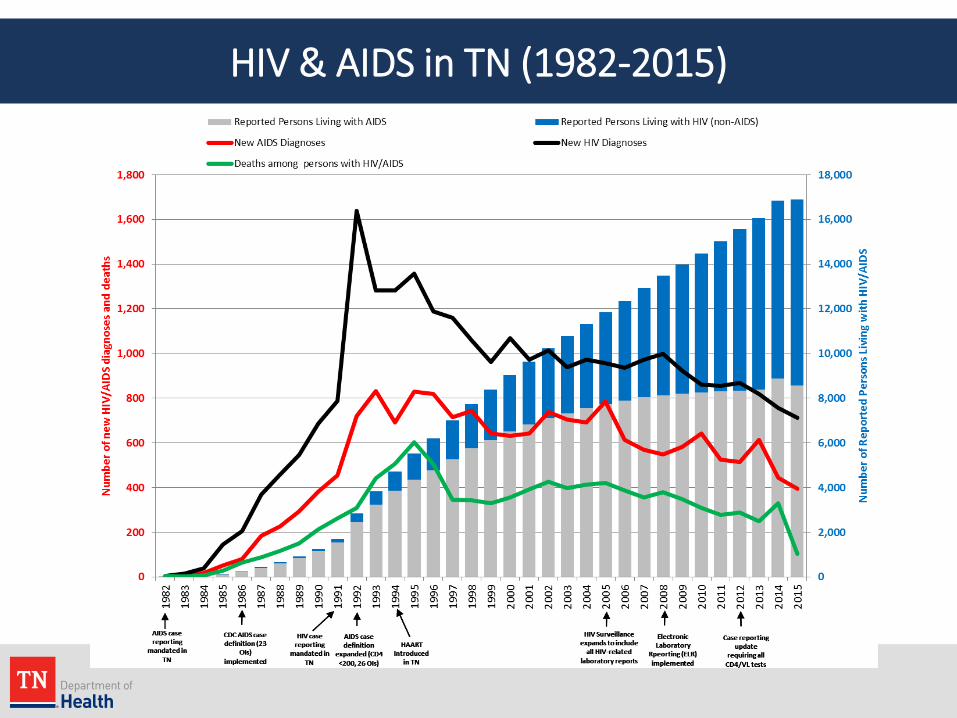
HIV & AIDS in TN (1982-2015)

Scott County, IndianaHIV/HCV Outbreak (NEJM, 2016)
Outbreak Detection & Response1/16/15: 6 HIV cases in 6 days 1/22 – 2/10/15: AIDS Dir & State Epi informed2/11/15: Emergency meeting3/23/15: Epi AID team arrives3/26/15: Exec Order, PH Emergency Declared (Governor)4/4/15: SEP startedEstablishment of Care Coordination Centers
Results (11/18/14 – 11/1/15))181 HIV +
92% co-infected HCV88% IDU536 contacts
94% Care Coordination74% Insurance69% Engaged in Care↓Wait time for inpatient detox (12 d)

Scott County: Lessons Learned
• The affected population demonstrated:– High levels of unemployment, poverty, IDU, and,– Low levels of education and medical insurance coverage
• Per CDC, the three approaches that turned around the HIV/HCV epidemic in Scott County were increased access to:– HIV and HCV testing,– HIV and HCV treatment, and – Syringe service programs

HIV Risk Vulnerability Assessment Webinar (CDC, September 2, 2015)

HIV Risk Vulnerability Assessment, Tennessee Profile, County Level

Distribution of New Cases in TN: HCV and HIV (2015)
Acute HCV Cases
Newly Diagnosed HIV Cases
Tennessee NBS, accessed February 10, 2017Note: County Data Unavailable for n=19 HCV Cases
Tennessee eHARS, internal sourceNatural Breaks/Manual, 5 Classes

Continuum of Cure

Surveillance & Education
Testing
Navigation
Case Management
Prevention
Prevention
Strengthening Prevention & Treatment Along the Spectrum of TN’s HCV Continuum of “Cure”

Health Department Responsibilities / Opportunities Prevention
o Community & Provider Educationo Hepatitis B Vaccination Programo Syringe Exchange, Opioid Substitution Therapy, PrEP
TDH Laboratory Capacityo HCV Ab with reflex to HCV RNA o GHOST surveillance (Global Hepatitis Outbreak Surveillance Technology)
Surveillance / Outbreak Investigationo Streamline VH case investigation / Develop NBS User’s Guide o Augment HCV lab consumption centrallyo Develop & Pilot HIV Outbreak Response Plano Develop VH Epi Profile o Establish chronic HCV (2017) and HIV genotyping (2018) as lab reportable
Partnershipso Local HD’s, MHSA, Corrections, Community, Academic Partners, SE AETC

Health Department Responsibilities & Opportunities
Treatmento Provider Trainings (SE AETC)o Provider Tool Kits (“HCV Treatment” and “HCV Medication Access”)o Navigation to treatment (HIV, HCV, MHSA) o RFA: Establish 6 Transient Elastography hubs
Pilotso HCV Testing / GHOST in Health Departments (2016)o Perinatal HCV Surveillance – central office (2017)o HIV/HBV/HCV Testing in Methadone Clinics (2017)
Futureo Establish HBV testing in state labo Support scale-up SSPso Integrate traditional and molecular surveillance o Pilot one-stop shops (PrEP, PEP, HIV Test-and-Treat)o ?? Establish chronic HBV and perinatal HCV as reportable

TDH Highlights
Surveillanceo Chronic HCV reporting, Outbreak Planning & Response
Preventiono HBV Vaccination Program in Jails
Pilotso HCV Testing in Health Departments
Treatmento Provider Trainings / Tool Kits

HBV Vaccination
TDH’s HBV Vaccination Program in Jails
Originally funded through PPHF (2012)o 2 FTEs (RN, admin)
Implementationo Targeting the right settings Risk, geography
o Logistics Nursing protocols & trainings
o Case management Updating immunization registries Vaccine completion

Targeting the Right Setting: Geography

TDH’s HBV Vaccination Program in Jails: Results
Sept 2012 – May 2016o 15,493 doses administered
56%, 1st dose 27%, 2nd dose 17%, 3rd dose
o Recipients 71%, male 86%, > 25 years old 90%, non-Hispanic White
From 2012 – 2015, rates of acute HBV rose more slowly in participating regions (7%) than rest of the state (29%)
Program maintained with state fundingo $300,000 / year (3 FTEs & ~8,000 doses HBV vaccine / year)

Surveillance

Increasing HCV Surveillance
• Simplify and streamline existing efforts
• Continue field investigations of all suspected acute HCV by regional staff
• Establish reporting for chronic HCV labs by Central Office– Associate “orphan” laboratory reports (ELR) with cases in NBS– Data entry of paper laboratory reports
• Notify regional staff of any cases suspected of acute HCV

Surveillance for Chronic HCV in Tennessee
*Central office chronic HCV surveillance efforts augmented beginning 7/1/15
Case Classification
2013 2014 2015* 2016
Confirmed 1,782 (44%)
3,385 (50%)
7,394 (59%)
10,442(50%)
Probable 2,234 3,421 5,244 10,496
Total (C + P) 4,016 6,806 12,628 20,938

Confirmed & Probable Cases of Chronic HCV in TN (2016) (n = 20,938)

Outbreak Planning, Detection, and Response
• Shift our thinking to outbreak detection
• Plan, prepare, and have early detection since we are vulnerable
• Increase surveillance and testing activities (including groups with currently low rates of HIV)

Outbreak Planning – Tools
• Outbreak Response Plan
• Questionnaire
• Just in Time Training
• Research Electronic Data Capture (REDCap Database)

HCV Testing

HCV Testing
• Rapid testing (antibody only, finger stick, 20 minutes)– Community-based organizations – Coupled with HIV testing
• Blood-based (antibody reflex to RNA, venipuncture, 1-2 weeks)– Health Department Pilot (June-October 2016)
• Health Department Roll-Out (April 1, 2017)– Statewide– Record Risk Factor(s) – PTBMIS supplemental screen– Clinics – Primary Care, STD, FP, others…
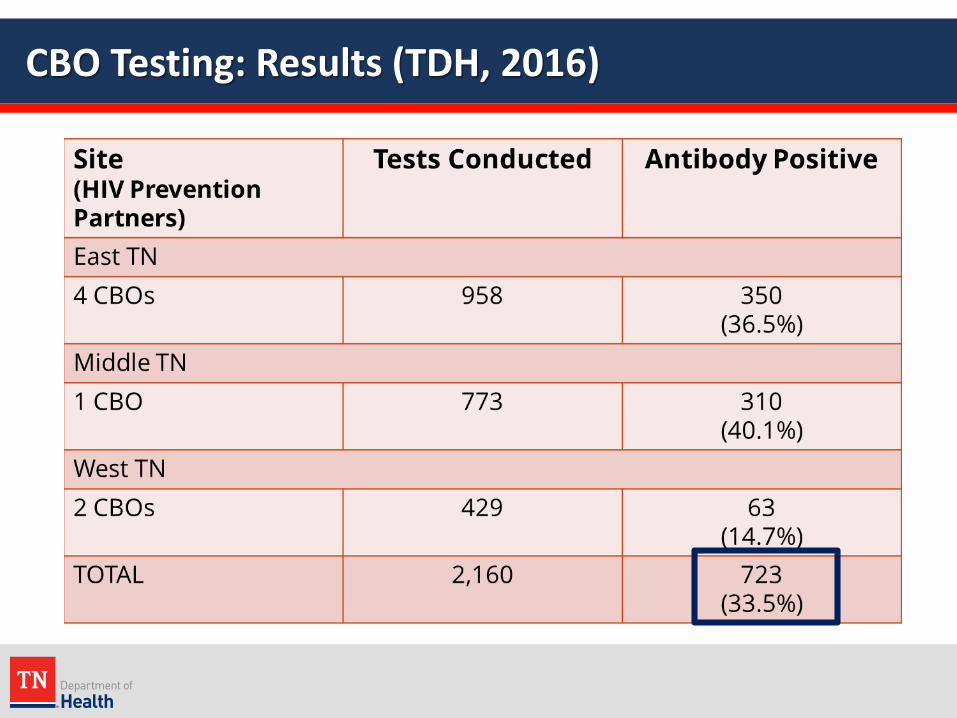
CBO Testing: Results (TDH, 2016)

Health Department (HD) HCV Testing Pilot
• During June 1–October 31, 2016:
4,753Patients were tested
for HCV

HCV Testing: HD Pilot Results 4,753 persons tested for HCV
o 8.4% Ab positive 74.1% RNA positive
Populationo ~70% STI clinics, ~30% FP clinics
Risk Factors among population testedo ~10% injection drug useo ~20% intranasal drug useo ~25% incarceration
Females 11-50 yo represented 58% of persons testedo 6.3% Ab (+)
5 were pregnant at the time of testing

HCV Testing: HD Pilot Results (cont’d)
Risk Factor Totaln (%)
N=4753
HCV Ab (+)n (%)
N=397
HCV Ab (-)n (%)
N=4356
P Value
Injection drug use 425 (8.9) 276 (64.9) 149 (35.1) <0.0001
Intranasal drug use 967 (20.3) 295 (30.5) 672 (69.5) <0.0001
Tattoo / piercing 1092 (23.0) 188 (17.2) 904 (82.8) <0.0001
Incarceration 1309 (27.5) 303 (23.1) 1006 (76.9) <0.0001
Transfusion 62 (1.3) 13 (21.0) 49 (79.0) 0.0003
No risk factors 2598 (54.7) 39 (1.5) 2559 (98.5) <0.0001
4,753 persons testedo 8.4% Ab positive
74.1% RNA positive

HCV Testing: TDH Recommendations
One time test for all patients that are:• Born from 1945 to 1965• Identified as high risk• Seeking evaluation and/or treatment for STIs• Requesting HCV testing or counseling
Persons with ongoing risk for HCV infection may have repeat screening at intervals of > 12 months, including:• Injection drug use (even once)• Illicit intranasal drug use (even once)• History of incarceration over 24 hours• Receipt of an unregulated tattoo • High-risk sexual behaviors (multiple sex partners, unprotected sex or sex with
an HCV-infected person or an injection drug user)

HCV Treatment

Impact of HCV in the U.S. --Acute, Chronic, Cirrhosis (U.S., 1950 - 2030)
Estimates range from 3.2-5.2 million cases in the USA
Davis GL et al. Gastroenterology 2010. // Armstrong GL et al. Ann Int Med 2006.Slide Credit: Dr. Cody Chastain

Impact of HCV in U.S. -- Death Rates: HIV, HCV, HBV (U.S., 1999 – 2007)
Ly KN et al. Ann Int Med 2012. Rein DB et al. Dig Liver Dis 2011. Zalesak M et al. PLoS ONE 2013.

Impact of HCV in U.S. – Death Rates: HCV vs. all other notifiable infect. conditions (U.S., 2003 - 2013)
Ly KN et al. CID 2016.
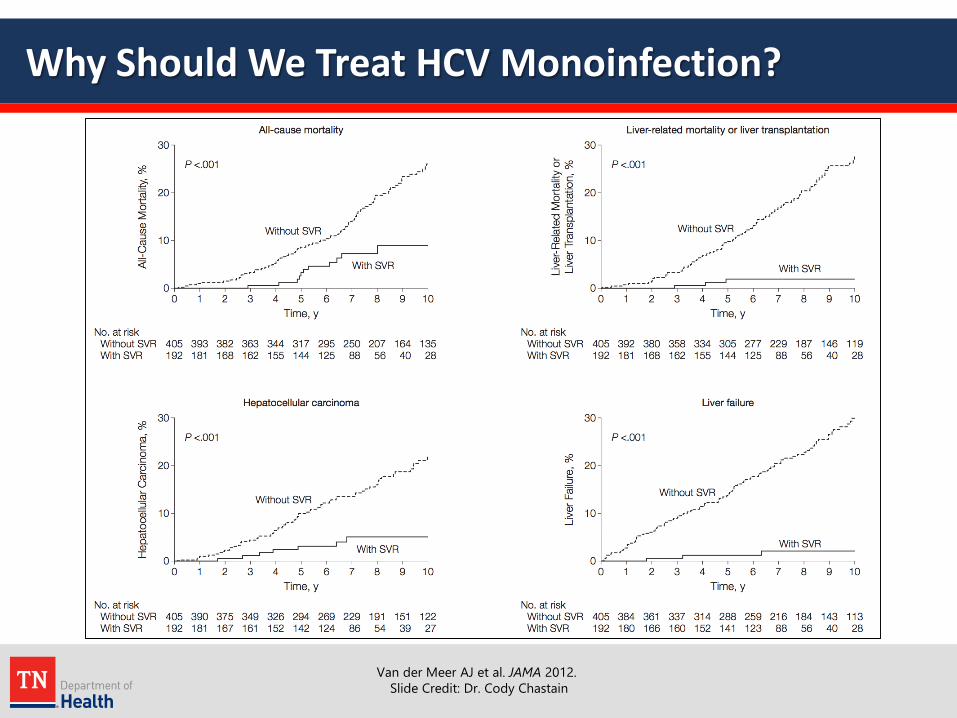
Why Should We Treat HCV Monoinfection?
Van der Meer AJ et al. JAMA 2012.Slide Credit: Dr. Cody Chastain

Impact: HCV Testing, Care, & Curative Treatment
Test• Persons born 1945 – 1965• Persons who inject drugs
Care and Treatment• ~90% + cure with 8-12 week
oral only treatment
Benefits• 73% reduction in liver cancer• 93% reduction in liver-related
mortality
Impact• Prevent 321,000 HCV deaths• Decrease HCV transmission
van der Meer, JAMA 2012; Morgan Ann Int Med 2012; Rein, CID 2015; Martin, CID 2013

HCV Treatment: Efficacy
Highly efficacious (>90%), oral-only, short-course (8-12 wks)
Pan-genotypic regimens -- highly effective across GTs and stages of liver disease (sofosbuvir / velpatasvir)
99 98 99 100 100 97 100
41/41
34/35
116/116
104/104
117/118
206/210
618/624
100
80
60
40
20
0n/N =
SVR
12 (%
)
All Pts 1a 1b 2 4 5 6
HCV Genotype
Feld JJ, et al. N Engl J Med. 2015; Foster GR, et al. N Engl J Med. 2015

HCV Treatment Provider Education in TN
Identify Safety Net Providerso HIV Centers of Excellenceo Primary Care Providers (FQHCs & Health Departments)
SE AETC / Vanderbilto 5 regional full-day provider trainings since 9/2016o Webinars, biweekly case conference (with SC’s AETC)o IAS-USA full-day HCV treaters’ workshop
Provider “Tool Kits”o HCV Treatment (visit-by-visit)o Medication Access
HD-specific protocolso Triage algorithmo Provider treatment guidelineso EHR visit-specific templates

Summary
• HCV is a widespread, serious, curable communicable disease
• 70% of acute infections are associated with IDU
• Rates of acute HCV are on the rise, predominately among young (<30 years of age), white, men and women living in rural areas
• Tennessee has 41 counties at high risk for an HIV/HCV outbreak
• HCV testing is indicated for baby boomers and anyone with risk factors
• Highly effective HCV treatment is available (most regimens are oral only 12-week regimens with minimal side effects)
• HCV treatment is prohibitively expensive
• Pan-genotypic HCV treatment regimens have been available since June 2016 (with more coming down the pipeline)

Acknowledgements/Resources
• TDH Viral Hepatitis Team
• TDH HIV Surveillance
• Vanderbilt SE-AETC
• http://www.hcvonline.org
• http://www.clinicaloptions.com
• http://hcvguidelines.org

Thank You!

Viral Hepatitis: Central Office Contacts
Programmatic• Carolyn Wester
– [email protected], 615-532-8516• Lindsey Sizemore
– [email protected], 615-770-6928
Prevention• Cathy Goff
– [email protected], 865-549-5384
Clinical Services• Kim Gill
– [email protected], 615-253-7304
Surveillance• Jennifer Black
– [email protected], 615-253-4782• Travis Sondergath
– [email protected], 615-253-4462• Shannon DePont
– [email protected], 615-532-8518
Perinatal Hep B• Janice Johnson
– [email protected], 615-253-1359
Hepatitis A• Robb Garman
– [email protected], 615-532-8507