Embed Size (px)
Citation preview

State of the ART: Integrase Inhibitors (clinical overview)
Mauro Schechter, MD PhDPrincipal Investigator, Projeto Praça Onze
Professor, Infectious DiseasesUniversidade Federal do Rio de Janeiro
Rio de Janeiro, Brasil
Global HIV Clinical Forum 2018Amsterdam
July 21, 2018

Honoraria for ad boards and lectures: Abbvie, Gilead, GSK/ViiV,
Janssen, Merck,
Disclosures

“There is no now. There are only immediate
memories of an extremely recente past”
(Anonymous and numerous)
Disclosures

BENCHMRK: Viral Suppression (NC=F)
and CD4 Cell Count (OF)
BENCHMRK = Blocking Integrase in Treatment Experienced Patients with a Novel Compound against HIV, Merck; F = failure; NC = noncompleter; OBT = optimized background therapy; OF = observed failure; OLRAL = open-label raltegravir; PBO = placebo; RAL = raltegravir.1. Eron JJ et al. Lancet Infect Dis. 2013;13(7):587-96. 2. Steigbigel RT et al. N Engl J Med. 2008;359(4):339-54.
100
Pa
tie
nts
With
HIV
RN
A
<5
0 c
op
ies/m
L, %
Weeks
80
0
20
024 9648
40
60
156 192 240
Double-Blind Open-Label OLRAL
33%
62%
26%
57%
22%
51%
16%
45%
16%
42%
Raltegravir group
Placebo group
100
Pa
tie
nts
With
HIV
RN
A
<4
00
co
pie
s/m
L, %
Weeks
80
0
20
024 9648
40
60
156 192 240
Double-Blind Open-Label OLRAL
37%
72%
28%
62%
23%
54%
18%
49%
17%
45%41%
78%
250
Ch
an
ge
fro
m B
ase
line
CD
4 C
ell
Co
un
t, c
ells
/mm
3
Weeks
200
0
50
0
24 9648
100
150
156 192 240
Double-Blind Open-Label OLRAL
45
109
49
125
68
164
56
165
61
183

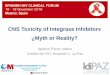
BIC
RAL EVG
Metal-Chelating Core: Oxygen atoms chelate a pair of Mg2+ ions and bind the integrase catalytic active site
1. Lazerwith SE, et al. ASM 2016. Poster #414. 2. Gallant J, et al. ASM 2016. Poster #415. 3. Tsiang M, et al. ASM 2016. Poster #416. 4.Tsiang M, et al., AAC 2016;60:7086.
Metal-Chelating Core Halogenated Phenyl Ring Side Chain
DTG
Halogenated Phenyl: Interacts with the integrase pocket that is normally occupied by the terminal 3’ base of viral DNA
Integrase Inhibitors

GUIDELINES
Nukes Non-nukes Instis PIs
TDF ou
TAF/
FTC/3TC
ABC/
3TC
AZT/
3TCEFV NVP RPV DTG EVG RAL BIC ATV DRV LPV
IAS-USA (2016)6
DHHS (2018)7
EACS (2017)8
WHO (2016)9
*
Brazil (2017)4
Preferential
Alternative
Not recommended, only special situationss
Not available *400 mg
4. BRASIL. Ministério da Saúde. Protocolo Clínico e Diretrizes Terapêuticas para Manejo da Infecção pelo HIV em Adultos. 2017. Disponível em: <http://www.aids.gov.br/system/tdf/pub/2013/64484/pcdt_adulto_270917.pdf?file=1&type=node&id=64484&force=1> . Acesso em: 24 abr. 2018.; 6. GÜNTHARD, HF. JAMA; 316(2):191-210, 2016.; 7. DHHS. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents Living with HIV. 2018. Disponível em: <https://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf>. Acesso em: 24 abr 2018.; 8. EACS. Guidelines. Version 9.0. Disponível em: <http://www.eacsociety.org/files/guidelines_9.0-english.pdf>. Acesso em: 24 abr. 2018.; 9. WHO. Consolidated Guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: Recommendations for a public health approach. 2016. Disponível em: <http://apps.who.int/iris/bitstream/handle/10665/208825/9789241549684_eng.pdf?sequence=1> . Acesso em: 24 abr. 2018.;
First Line Therapy (May, 2018)

BIC
RAL EVG
Metal-Chelating Core: Oxygen atoms chelate a pair of Mg2+ ions and bind the integrase catalytic active site
1. Lazerwith SE, et al. ASM 2016. Poster #414. 2. Gallant J, et al. ASM 2016. Poster #415. 3. Tsiang M, et al. ASM 2016. Poster #416. 4.Tsiang M, et al., AAC 2016;60:7086.
Metal-Chelating Core Halogenated Phenyl Ring Side Chain
DTG
Halogenated Phenyl: Interacts with the integrase pocket that is normally occupied by the terminal 3’ base of viral DNA
Integrase Inhibitors

• Study overview
– International, multicenter, double-blind, double-dummy, randomized (1:1), active-controlled,
noninferiority, phase 3 study
• Endpoints
– The primary endpoint was noninferiority with respect to the percentage of patients with HIV-1
RNA <50 copies/mL at Week 48, with a secondary time point at 96 weeks
– A prespecified exploratory analysis examined results at Weeks 156, 192, and 240
STARTMRK: RAL vs EFV Plus TDF/FTC in Treatment-Naive Adult HIV-1 Patients—Study Design
BID = twice daily; EFV = efavirenz; FTC = emtricitabine; QHS = every night; RAL = raltegravir; TDF = tenofovir.1. Rockstroh JK et al. J Acquir Immune Defic Syndr. 2013;63(1):77–85.
RAL 400 mg BID + TDF/FTC
(n=281)
EFV 600 mgQHS + TDF/FTC
(n=282)
1:1
Screening baseline HIV-1 RNA: >50,000 copies/mL vs ≤50,000 copies/mL Viral hepatitis coinfection status: positive for hepatitis B, hepatitis C, or both vs negative for both
Eligibility criteria:• ≥18 years old
•Treatment naïve
• HIV-1 infected• Viral load >5000
copies/mL• Without genotypic
resistance to EFV, TDF, or FTC
• Patients with stable, chronic hepatitis could be enrolled if serum aminotransferase was ≤5-fold the ULN range
71 Patients (25.2%)
Discontinued6 – Lack of efficacy
14 – Adverse events
210 Patients (74.5%) Completed
Entire 5-Year Study
281 Patients Treated With
RAL-Based Regimen
184 Patients (64.8%) Completed
Entire 5-Year Study
98 Patients (34.5%)
Discontinued10 – Lack of efficacy
28 – Adverse events
282 Patients Treated With
EFV-Based Regimen
563 Enrolled Patients
Randomized 1:1 to RAL/EFV Arms

STARTMRK: Viral Suppression and CD4 Cell Counts at Week 240
BID = twice daily; EFV = efavirenz; F = failure; FTC = emtricitabine; NC = noncompleter; OF = observed failure; QHS = every bedtime; RAL = raltegravir; TDF = tenofovir.1. Lennox JL et al. Lancet. 2009;374(9692):796-806. 2. Lennox JL et al. J Acquir Immune Defic Syndr. 2010;55(1):39-48. 3. Rockstroh JK et al. Clin Infect Dis. 2011;53(8):807-16. 4. DeJesus E et al. HIC ClinTrials. 2012;13(4):228-32. 5. Rockstroh JK et al. J Acquir Immune Defic Syndr. 2013;63(1):77-85.
Viral Suppression (NC=F Analysis)
80
Pa
tien
ts w
ith
HIV
RN
A
Leve
ls <
50
co
pie
s/m
L, %
Weeks
60
40
0 48 144 216
100
20
024 72 19296 120 168 240
Number of Contributing Patients
RAL 400 mg BID
EFV 600 mg QHS
281 280 280 277279 281 281281 279277 281
282 281 281 282282 282 282282 281 282 279
12
278
282
82
86
79
81
61%
71%
67
76
69
75
Exploratory
analysis
Secondary
endpoint
Primary
endpoint
• Difference (95% Cl) = 9.5 (1.7,17.3)
• P<0.001
• Superiority concluded
300
Change fro
m B
aselin
e
CD
4 C
ell
Count, c
ells
/mm
3
Weeks
250
200
0 48 144 216
350
150
100
50
0
24 72 19296 120 168 240
400
12
RALEFV
189
163
240
225
374
312
361
301295
331

• Study overview: Phase 3, prospective, randomized, open label trial• Hypothesis: FTC/TDF QD with ATV/r QD, RAL BID, or DRV/r QD will be
equivalent in terms of virologic efficacy and tolerability over 96 weeks• Co-primary End Points
– Virologic Failure: time to HIV-1 RNA >1,000 c/mL at or after Week 16 to before Week 24, or >200 c/mL at or after Week 24
– Tolerability Failure: time to DTC of randomized component for toxicity • Secondary Endpoint: the earlier occurrence of either virologic failure or
tolerability failure• Substudies:
– Mean change from baseline in fasting lipid profile over time– Percentage bone mineral density change at total hip,
lumbar spine, and total body
ACTG 5257: Ritonavir-Boosted DRV or ATV versus RAL:
Study Design
ART = antiretroviral; ATV/r = atazanavir/ritonavir; BID = twice daily; DRV/r = darunavir/ritonavir ; DTC – discontinuation; FTC = emtricitabine; QD = once daily; RAL = raltegravir; TDF = tenofovir disoproxil fumarate.1. Lennox JL et al. Ann Intern Med. 2014;161(7):461-71. 2. Ofotokun I et al. Clin Infect Dis. 2015;60(12):1842-51. 3. Brown TT et al. J Infect Dis. 2015;212(8):1241-9.
ATV/r 300/100 mg QD + FTC/TDF 200/300 mg QD
(n=605)
RAL 400 mg BID + FTC/TDF 200/300 mg QD
(n=603)
1:1:1
Stratified by screening baseline HIV-1 RNA: ≥100,000 copies/mL vs <100,000 copies/mL with balancing by institution. Stratified by metabolic substudy participation and Framingham 10-yr risk of MI or coronary death (<6% vs ≥6%)
Eligibility criteria:• ≥18 years old• ART naïve• HIV-1 infected• Plasma HIV-1 RNA
>1000 copies/mL DRV/r 800/100 mg QD + FTC/TDF 200/300 mg QD
(n=601)
1814 patients randomized 1:1:1 to
ATV/r:RAL:DRV/r 5 patients excluded 1 acute illness, 1 prior ART, and 3 prior ART
and resistance
1809 patients included in all analyses
605 patients ATV/r5 never started ART
603 patients RAL4 never started ART
601 patients DRV/r4 never started ART
89 patients (14.7%)
discontinued10 death29 lost to follow up
28 unable to travel to clinic
22 nonadherentor other
72 patients (11.9%)
discontinued6 death
23 lost to follow up
35 unable to travel to clinic8 nonadherent
or other
101 patients (16.8%)
discontinued13 death34 lost to follow up
30 unable to travel to clinic
24 nonadherentor other
556 patients (91.9%) completed
96 weeks
560 patients (92.9%) completed
96 weeks
546 patients (90.8%) completed
96 weeks

ACTG 5257
Primary endpoint analyses at Week 96
Lennox JL et al. Ann Intern Med 2014;161:461–471. .
▪ Significantly greater incidence of
treatment failure with ATV/r vs
RAL or DRV/r
– in part due to a high proportion of
patients with hyperbilirubinemia
Tolerability failure
▪ RAL superior to
either boosted PI
▪ DRV/r superior to
ATV/r
Composite endpoint
Difference in 96-week cumulative incidence (97.5% CI)
0–10 10 20
ATV/r vs RAL3.4% (–0.7 to 7.4)
DRV/r vs RAL5.6% (1.3 to 9.9)
ATV/r vs DRV/r–2.2% (–6.7 to 2.3)
0–10 10 20
ATV/r vs RAL15% (10to 20)
Favours RAL
ATV/r vs DRV/r7.5% (2.3 to 13.0)
Favours DRV/r
DRV/r vs RAL7.5% (3.2 to 12.0)
Favours RAL
0–10 10 20
DRV/r vs RAL3.6% (1.4 to 5.8)
ATV/r vs RAL13% (9.4 to 16.0)
Favours RAL
ATV/r vs DRV/r9.2% (5.5 to 13.0)
Favours DRV/r
VF
▪ Regimens equivalent
in time to VF

▪ Design
▪ Objective– Non inferiority of RAL QD: % HIV RNA < 40 c/mL by ITT, NC=F
(lower margin of the 2-sided 95% CI for the difference = - 10%, 90% power)
RAL 1200 mg ** QD + RAL 400 mg BID placebo
TDF/FTC fdc QD
RAL 400 mg BID + RAL 1200 mg ** QD placebo
TDF/FTC fdc QD
> 18 years
ARV-naïveHIV RNA > 1000 c/mL
*Randomisation was stratified by baseline HIV RNA (< or > 100 000 c/mL) and viral hepatitis co-infection status** Reformulated RAL 600 mg tablet
ONCEMRK Study: raltegravir 1200 mg QD
vs 400 mg BID, with TDF/FTC
Randomisation*2 : 1
Double-blind
N = 266
N = 531
W96W48
Cahn P. AIDS 2016, Durban, Abs. FRAB0103LB

ONCEMRK Study: raltegravir 1200 mg QD
vs 400 mg BID, with TDF/FTC
53.5
78.283.5
87.4 88.7 88.9
51.9
76.382.1
86.5 87.2 88.3
0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36 40 44 48
Week
Difference QD vs BID = 0.5% (- 4.2 ; 5.2)
Patients with baseline HIV RNA > 100 000 c/mL: % HIV RNA < 40 c/mL
(observed failure):
QD = 86.7% vs BID = 83.8% ; difference = 2.9% (- 6.5 ; 14.1)
%
Cahn P. AIDS 2016, Durban, Abs. FRAB0103LB
▪ CD4/mm3 increase at W48 (observed failure): QD = + 232 vs BID = + 234 ; ∆ -2 (- 31 ; 27)
HIV RNA < 40 c/mL (NC = F ; snapshot), % (95% CI)
RAL 1200 mg QD + TDF/FTC
RAL 400 mg BID + TDF/FTC

ONCEMRK: Adverse Events by Race/Ethnicity
• ‡ Determined by the investigator to be related to study drug.• § Study medication withdrawn.• AE = adverse event; BID = twice daily; DR = drug-related; QD = once daily; RAL = raltegravir.• 1. Cahn P et al. Oral presentation at HIV Glasgow 2016. Glasgow, UK. Abstract # 3514101.
% Subjects With
White Black
RAL 1200 mg
QD (N=301)
RAL 400 mg
BID (N=172)
RAL 1200 mg
QD (N=98)
RAL 400 mg
BID (N=36)Any adverse event (AE) 82.7 86.0 90.8 94.4Drug-related‡ (DR) AE 25.9 22.7 27.6 36.1Serious AE 5.0 9.9 11.2 8.3Serious & DR AE 0.3 0.6 0.0 2.8Discontinued§ owing toAE 0.3 1.2 1.0 5.6
% Subjects With
Asian Hispanic/Latino
RAL 1200 mg
QD (N=83)
RAL 400 mg
BID (N=40)
RAL 1200 mg
QD (N=126)
RAL 400 mg
BID (N=52)Any adverse event (AE) 69.9 85.0 88.1 84.6Drug-related‡ (DR) AE 15.7 25.0 30.2 19.2Serious AE 4.8 12.5 1.6 7.7Serious & DR AE 0.0 0.0 0.0 0.0Discontinued§ owing toAE 0.0 2.5 1.6 1.9

BIC
RAL EVG
Metal-Chelating Core: Oxygen atoms chelate a pair of Mg2+ ions and bind the integrase catalytic active site
1. Lazerwith SE, et al. ASM 2016. Poster #414. 2. Gallant J, et al. ASM 2016. Poster #415. 3. Tsiang M, et al. ASM 2016. Poster #416. 4.Tsiang M, et al., AAC 2016;60:7086.
Metal-Chelating Core Halogenated Phenyl Ring Side Chain
DTG
Halogenated Phenyl: Interacts with the integrase pocket that is normally occupied by the terminal 3’ base of viral DNA
Integrase Inhibitors

The QUAD Pill: Study Design
Treatment- naive
Any CD4 count
Quad QD
EFV/FTC/TDF QHS
Placebo
EFV/FTC/TDF QHS
Quad Placebo QD
n=350
n=350
Week 48 Week 192
• Elvitegravir 150 mg
• Cobicistat 150 mg
• Emtricitabine 200 mg
• Tenofovir disoproxil fumarate 300 mg

88%84%
7% 6% 5%9%
84% 82%
7% 8% 9% 11%
0
20
40
60
80
100
W48 W96 W48 W96 W48 W96
Virologic Success Virologic Failure No data at W48 (or 96)
Per
cen
tag
e o
f su
bje
cts
(%)
QUAD (STBD) EFV/FTC/TDF (ATR)
Quad Vs Efavirenz: 48 and 96 weeks results

Median Change from Baseline in Serum Creatinine
BL 2 4 8 12 16 24 32 40 48
0.35
0.30
0.25
0.20
0.15
0.10
0.05
0.00
-0.05
-0.10
Ch
ange
fro
m B
L in
Ser
um
Cre
atin
ine
(mg
/dL)
(IQ
R)
Week

Two Phase 3, International, randomized, double-blind,
active-controlled studies comparing TDF vs TAF
19
Primary Endpoint HIV-1 RNA <50 copies/mL* at Week 48 by FDA Snapshot analysis (12% Non-inferiority margin of E/C/F/TAF to E/C/F/TDF)†
Secondary EndpointsEfficacy, safety** and tolerability observed through Week 96, Week 144
ClinicalTrials.gov Identifier: NCT01780506 and NCT01797445
Treatment Naïve PatientsStudy 102 and 103
Secondary Endpoints
Tx-Naïve Adults
HIV-1 RNA ≥ 1000 c/mL
eGFR ≥ 50 mL/min
Primary Endpoint
Week 48 Week 96
Stratification by • HIV-1 RNA ≤ />100,000 c/mL• CD4 cell count• Geographic region
1:1
Week 144
E/C/F/TAF QD
E/C/F/TAF Placebo QD
E/C/F/TDF Placebo QD
E/C/F/TDF QD (STB)
N =866
N =867
*Taqman 2.0 assay†Combined efficacy analysis was pre-specified. **SCr, proteinuria, hip and spine BMD were pre-specified week 48 safety endpoints.Study 104 (North America, EU, Asia) and Study 111 (North America, EU, Latin America)
E/C/F/TAF: elvitegravir 150 mg / cobicistat 150 mg / emtricitabine 200 mg / tenofovir alafenamide 10 mgSTB: Stribild; elvitegravir 150 mg / cobicistat 150 mg / emtricitabine 200 mg / tenofovir DF 300 mg
1. Wohl D, et al. JAIDS 2016 3. Ward, D., HIV and Aging 2016, Poster #33.2. Sax P, et al. Lancet 2015 4. Arribas J, et al. CROI 2017. Seattle, WA. Poster #453

% (n/n) of Participants Difference (95% CI)
E/C/F/TDFn=867
E/C/F/TAFn=866
Age
<50 yrs80
(602/753)83
(647/777)
≥50 yrs*81
(92/114)92
(82/89)
Sex
Male82
(603/740)84
(616/733)
Female*72
(91/127)85
(113/133)
Race
Black71
(152/213)75
(168/223)
Nonblack*83
(542/654)87
(561/643)
Region
US*80
(423/532)84
(447/532)
Non-US81
(271/335)84
(282/334)
Treatment Difference in Virologic Outcomes at Week 144
by Pre-specified Subgroups
20
-1 8 -1 2 -6 0 6 1 2 1 8 2 4-2 4
E/C/F/TAFE/C/F/TDF
* Statistically significant.
Arribas J, et al. CROI 2017. Seattle, WA. Poster #453

Me
dia
n (
IQR
) %
Ch
an
ge
Fro
m B
L
21
* p-values calculated using 2-sided Wilcoxon rank-sum test to compare treatment groupsBL, baseline; β2M, β2 microglobulin; IQR, interquartile range; RBP, retinol binding protein; UPCR, urine protein:Cr ratio.
E/C/F/TDFE/C/F/TAF
23 3454
-32 -32 -26
-100
-50
0
50
100
150
200
250
300
350
0 48 96 144Week
β2M:Cr
BL, µg/g100.6103.1
848 803 722
848 789 681
761
737
5174
111
10 14 35
-100
-50
0
50
100
150
200
250
300
350
0 48 96 144
Week
RBP:Cr
BL, µg/g63.967.1
855 812 769 728
855 800 746 687
20 16 25
-4 -9 -11
-100
-50
0
50
100
150
0 48 96 144
Week
866 819 768 740
866 801 751 699
UPCR
BL, mg/g43.943.8
n=
n=
p <0.001* for all
Renal Parameters through Week 144
Arribas J, et al. CROI 2017. Seattle, WA. Poster #453
• At Week 144, median decrease from baseline in eGFRCG was significantly smaller with E/C/F/TAF vs E/C/F/TDF (-1.6 vs -7.7 mL/min; p<0.001)

• Through Week 144, significantly greater losses in spine and hip BMD in TDF group
• No D/C due to bone AEs in TAF arm vs 6 in TDF arm
• Initiated meds during the study to increase BMD: 16% TAF vs. 21% TDF; p=0.018
Spine
Week
Hip
-0,45-0,76 -0,90 -0,93
-1,56
-3,00-3,57 -3,53
-6
-4
-2
0
2
0 24 48 96 144
E/C/F/TAF: (n=)
E/C/F/TDF: (n=)
795
790
845
850
797
816
744
745
702
686
791
784
836
848
789
815
735
742
690
683
Me
dia
n C
ha
ng
e (
Q1
,Q3
)
E/C/F/TAF E/C/F/TDF
‡
P <0.001
for all
Week
Arribas J, et al. JAIDS 2017. E-pub. DOI: 10.1097/QAI.0000000000001350
P <0.001
for all
*p-value calculated using analysis of variance model including treatment as a fixed effect.
-1,22 -1,20 -0,97 -0,89
-2,72 -2,76 -2,82 -2,87
-6
-4
-2
0
2
0 24 48 96 144
Median Change in Spine and Hip BMD
through Week 144

BIC
RAL EVG
Metal-Chelating Core: Oxygen atoms chelate a pair of Mg2+ ions and bind the integrase catalytic active site
1. Lazerwith SE, et al. ASM 2016. Poster #414. 2. Gallant J, et al. ASM 2016. Poster #415. 3. Tsiang M, et al. ASM 2016. Poster #416. 4.Tsiang M, et al., AAC 2016;60:7086.
Metal-Chelating Core Halogenated Phenyl Ring Side Chain
DTG
Halogenated Phenyl: Interacts with the integrase pocket that is normally occupied by the terminal 3’ base of viral DNA
Integrase Inhibitors

Spring-2: A double-dummy, multicentre study comparing Dolutegravir to Raltegravir in Treatment Naïve Patients
Primary endpoint: proportion of subjects with HIV-1 RNA <50 c/mL at Week 48 (FDA Snapshot), with a -10% non-inferiority margin
DTG (50 mg QD) plus RAL placebo (BID) + 2 NRTIs*
(n=411)
RAL (400 mg BID) plus DTG placebo (QD) + 2 NRTIs*
(n=411)
• Treatment-naïve, HIV-1-infected adults
• HIV-1 RNA ≥1000 c/mL• Stratified by NRTI and
viral load
DTG (50 mg QD) + 2 NRTIs
Screening period Randomised phase Open-label phase
Randomisation (Day 1) Analysis Week 48 Analysis Week 96 Screening Visit (Day -14)
*Investigator’s selection ABC/3TC or TDF/FTCFDA, Food and Drug Administration

TreatmentNumber of responders/
total assessed, n (%)Difference in
proportion (95% CI) (DTG - RAL)Adjusted difference in
proportion (95% CI) (DTG - RAL)
DTG 50 mg QD 332/411 (81) 4.4% (–1.2%, 10.0%) 4.5% (–1.1%, 10.0%)
RAL 400 mg BID 314/411 (76)
Error bars indicate 95% CI Adaptado a partir das referências 3, 4, 6
DTG and RAL were associated with similar increases in CD4+ cell count from baseline over time.
Spring-2: A double-dummy, multicentre study comparing Dolutegravir to Raltegravir in Treatment Naïve Patients

AEs, n (%)DTG 50 mg QD
(n=411)RAL 400 mg BID
(n=411)
WEEK 48
Any event 339 (82) 340 (83)
Nausea 59 (14) 53 (13)
Headache 51 (12) 48 (12)
Nasopharyngitis 46 (11) 48 (12)
Diarrhoea 47 (11) 47 (11)
WEEK 96
Any event 349 (85) 349 (85)
Nausea 60 (15) 56 (14)Nasopharyngitis 55 (13) 58 (14)Diarrhoea 57 (14) 55 (13)Headache 56 (14) 55 (13)
SPRING-2: Adverse Events
Discontinuations due to AEs were 2% for DTG vs 2% for RAL at Week 96

Change in serum CR, Mean (+/- SD)2,3
25
20
15
10
5
0
-5Mea
n ch
ange
from
bas
elin
e
of C
R (μm
ol/L
)
2 4 8 12 16 24 32 40 48
Week
+12.3*
+4.7*
Baseline (µmol/L): DTG: 74.7 versus RAL: 75.2
Adaptado a partir das referências 3, 4, 5, 7, 8
*Mean change in serum CR (mg/dL): DTG, +0.14mg/dL, RAL, +0.05 mg/dL; based on conversion rate 0.011mg/dL = 1 µmol/LCR, creatinine
0.3
0
0.2
0.1
mg/dL
SPRING-2: Effect of Dolutegravir on Creatinine Serum Levels
A small initial increase in creatinine was observed with DTG, due to the blockade of creatininesecretion. There was no further increase in mean serum CR from Week 48 to Week 96 (Week 0 to
96: DTG +14.6 mmol/L; RAL +8.2 mmol/L)5
Creatinine clearance byCockcroft-Gault, mean (SD)
DTG 50 mg QD + NRTIs*
RAL 400 mg BID + NRTIs*
n mL/min n mL/min
Baseline 411 125 (25.8) 411 127.8 (31.2)
Week 24 389 -17.5 (13.4) 384 -6.4 (13.8)
Week 48 369 -16.5 (14.2) 353 -5.4 (13.9)
These changes are not considered to be clinically
relevant as the glomerular filtration rate is unchanged

Unexpectedly High Rate of Intolerance for Dolutegravir in Real Life Setting
• Guido van den Berk, Josephine Oryszczyn, Willem Blok, Narda van der Meche, Rosa Regez, Daoud Ait Moha, Kees Brinkman
• dept internal medicin OLVG, Amsterdam, The Netherlands
abstract
948
background
methods
conclusion
results
- Integrase inhibitors (INSTI)are now preferred antiretrovirals in first line cART.
- Dolutegravir (DTG) is possibly considered as one of the most efficacious, convenient and tolerated INSTI, with hardly any chance for drug-drug interactions.
- Since we encountered many patients who stopped DTG because of intolerance, we analyzed the experience with DGV in our whole patient population since licensing in the Netherlands (aug 2014)
- OLVG cohort: ±3000 patients, (97,4% on cART)
- retrospective analysis of all patients who started DTG, either as initial therapy or after switching from other antiretrovirals for any reason.
- Baseline characteristics at the moment of DTG start were recorded.
- We calculated the proportion of patients who stopped DTG, analyzed the reason for interruption and evaluated potential risk factors.
- Chi-squared test and Z-score to check for significant differences between groups and proportions.
In a real life setting a substantial proportion of patients unexpectedly interrupted DTG treatment for reasons of intolerance, in particular sleeping, gastrointestinal and psychiatric problems.
This was much higher than reported in clinical trials.
DTG treatment was stopped in 62/387 (16,0%) patients. There were no virological failures. Main reason for DGV interruption was intolerance in 56/62 (90,3%) patients: 19/56 (31,3%) sleeping problems, 18/56 (29,5%) gastrointestinal problems, 12/56 (19,7%) psychiatric problems, 8/56(12,9%) headache, 9/56 (14,6%) fatigue and 6/55 (10,9%). Some patients reported more than one toxicity.
Psychiatric reason to stop (n=12) varied from anxiety, depression and agitation to psychosis (n=2)
results
total (N=387) naives(N=65) non-naives (N=322)
median age (IQR) 48 46 (22) 48 (13) ns
female 44 11,4% 8 12,3% 36 11,2% ns
dutch origin 136 35,1% 28 43,1% 108 33,5% ns
median CD4/mm3 (IQR) 650 530 (395) 655 (345) ns
median DTG days (IQR) 220 196 (147) 221 (148) ns
DTG separate.. 156 15 141
DTG in STR.. 231 50 181
DTG stopped 62 16,0% 13 20,0% 49 15,2% ns
median DTG days (IQR) 78 81 (71) 75 (99) ns
female 5 11,4% 3 37,5% 2 5,6% p=0.01
DTG separate 24 15,4% 1 6,7% 23 16,3% ns
DTG in STR 38 16,6% 12 24,0% 26 14,4% ns
reason for interruption
other than toxicity* 6 9,7% 1 7,7% 5 10,2%
toxicity 56 90,3% 12 92,3% 44 89,8% ns
sleeping.. 19 31,3% 5 38,5% 14 28,6% ns
gastro-intestinal.. 18 29,5% 4 30,8% 14 28,6% ns
neuro-psychiatric.. 12 19,7% 3 23,1% 9 18,4% ns
paresthesia.. 6 9,7% 0 0,0% 6 12,2% ns
headache.. 8 12,9% 0 0,0% 8 16,3% ns
fatigue.. 9 14,6% 1 7,7% 8 16,3% ns
allergy.. 1 1,7% 1 7,7% 0 0,0% ns
other.. 5 8,2% 1 7,7% 4 8,2% ns*LTFU, HBV protection, insurance, induction, patient request, interaction

BIC
RAL EVG
Metal-Chelating Core: Oxygen atoms chelate a pair of Mg2+ ions and bind the integrase catalytic active site
1. Lazerwith SE, et al. ASM 2016. Poster #414. 2. Gallant J, et al. ASM 2016. Poster #415. 3. Tsiang M, et al. ASM 2016. Poster #416. 4.Tsiang M, et al., AAC 2016;60:7086.
Metal-Chelating Core Halogenated Phenyl Ring Side Chain
DTG
Halogenated Phenyl: Interacts with the integrase pocket that is normally occupied by the terminal 3’ base of viral DNA
Integrase Inhibitors

1. White K, et al., European Workshop HIV & Hep 2016. Rome, Italy. Poster O-01. 2. Tsiang M, et al., AAC 2016;60:7086-7097.
92%89%
04%2% 4%6% 2%
0
10
20
30
40
50
60
70
80
90
100
EVG RAL
% o
f Is
ola
tes b
y F
C C
ate
go
rie
s
17%
17%
17%
49%
DTG
2%13%
15%
70%
BIC
Mean fold changes: BIC 2.8 (ref) ; DTG 5.8, p=0.042; RAL >100, p<0.001; EVG >106, p<0.001
Each of 47 patient-derived clinical isolates (from Monogram Biosciences) had ≥ 1 primary and/or other INSTI mutations with phenotypic resistance to INSTIs and comprised all available INSTI resistant variants in the Monogram library).
Stratification of 47 HIV-1 Clinical Isolates Based on Fold Change in Resistance
< 2.5 ≥ 102.5 to < 5 5 to < 10
EC50 Fold Change (FC) vs Reference Wild Type
EC50=effective concentration of half maximal response; FC=fold change; IN=Integrase; T1/2=half-life.
Phenotypic Analysis of Clinical Isolates

ART-naive Adults▪ HIV-1 RNA ≥ 500 c/mL ▪ eGFRCG ≥ 30 mL/min
n=320
n=325
1:1
Week 0
DTG + FTC/TAF Placebo QD
B/F/TAF QD
B/F/TAF Placebo QDDTG + FTC/TAF QD
48 14496
Study 14903,4 *
B/F/TAF Vs DTG in Treatment-Naïve
ART-naive Adults▪ HIV-1 RNA ≥ 500 c/mL ▪ eGFRCG ≥ 50 mL/min▪ HLA B*5701 negative
n=314
n=315
1:1
Week 0
ABC/3TC/DTG Placebo QD
B/F/TAF QD
B/F/TAF Placebo QDABC/3TC/DTG QD
48 14496
Study 14891,2 *
Ran
do
miz
edD
ou
ble
-Blin
dR
and
om
ized
Do
ub
le-B
lind
Gallant J, et al. IAS 2017. Paris, France. Oral #MOAB0105LB; Gallant J, et al. Lancet 2017;390:2063-72; Sax P, et al. IAS 2017. Paris, France. Poster Discussion #TUPDB0201LB; Sax P, et al. Lancet 2017;390:2073-82;

White K, et al . CROI 2018. Boston, MA. Poster 532; Gallant J, et al. Lancet 2017;390:2063-72;. Sax P, et al. Lancet 2017;390:2073-82.
32
B/F/TAF displayed rapid viral suppression (M=E)1
and non-inferior efficacy2,3* vs. DTG-based regimens at Week 48
Par
tici
pan
ts(%
)
* Based on Snapshot analysis
Virologic Efficacy:
HIV-1 RNA <50 copies/mL, Missing=Excluded AnalysisPooled ART-naïve Studies 1489 and 1490

Drug-Related Adverse Events (AEs) through Week 48
Study 14891
All grade
(≥ 2% in either arm)
B/F/TAF
n=314
DTG/ABC/3TC
n=315
Any Drug-related AEs 26%* 40%
Diarrhea 6% 4%
Nausea 5%† 17%
Headache 5% 5%
Fatigue 3% 3%
Abnormal dreams 3% 3%
Dizziness 2% 3%
Insomnia 2% 3%
Study 18442
All grade (≥ 1% in either arm)
B/F/TAFn=282
DTG/ABC/3TCn=281
Any Drug-related AEs 8%** 16%
Headache 3% 3%
Abnormal dreams <1% 2%
Diarrhea <1% 1%
Fatigue <1% 1%
Flatulence 0% 2%
Nausea 0% 2%
Insomnia 0% 1%
B/F/TAF was well tolerated with significantly fewer drug-related AEsthan DTG/ABC/3TC in ART-naïve and suppressed patients,
largely due to GI and CNS AEs
Difference between treatment arms: * p<0.0013, † p<0.0001, and ** p=0.01
White K, et al . CROI 2018. Boston, MA. Poster 532; Gallant J, et al. Lancet 2017;390:2063-72;. Sax P, et al. Lancet 2017;390:2073-82.

RALTEGRAVIR ELVITEGRAVIR DOLUTEGRAVIR BICTEGRAVIR
Clinical dose 400 mg BID* OR 1200
mg QD
150 mg QD with cobi and
FTDF or FTAF
50 mg QD
50 mg BID (INI-resistant)
50 mg QD with FTAF
Metabolism UGT1A1 CYP3A (major), UGT1A1/3
(minor)
UGT1A1 (major), CYP3A
(minor)
UGT1A1 and CYP3A
(equal)
DDI Potential Least Highest Slightly greater
than RAL
Slightly greater
than DTG
1. Tivicay SmPC updated October 2015. 2. Min S, et al. Antimicrob Agents Chemother 2010;54:254–8. 3. Min S, et al. AIDS 2011;25:1737–45
4. Isentress SmPC July 2015; 5. Stribild SmPC updated June 2015); 6. Ramanathan S, et al. Clin Pharmacokinet 2011;50:229–44.
Integrase Inhibitors: Clinical
Pharmacology Profile

Legend primarily applies to drug therapy
www.hiv-druginteractions.org

Selected DDI for Boosted Regimens
(PI/r; PI/c; EVG/c)
Smith JM et al. AIDS 2017, Burgess MJ et al. HIV AIDS 2015; Nachega JB et al. AIDS 2012, www.hiv-druginteractions.org
Drug class Comment
Corticosteroids Risk of Cushing syndrome. Avoid PI/r, PI/c, EVG/c. Risk not just oral but inhaled, eye
drops, injection, topical. Triamcinolone, budesonide, fluticasone, mometasone contra-
indicated.
Antidepressants Avoid tricyclics - can cause anticholinergic effects, sedation, orthostatic hypotension.
Benzodiazepines Caution - increased sensitivity in elderly with risk of cognitive impairment, falls etc. AEs
increased by inhibition of CYP metabolism. Use lowest dose for short duration. Midazolam,
triazolam contraindicated.
Chemotherapy drugs Many chemotherapy drugs metabolised by CYP. Increased risk of chemo related
toxicities.
Anticoagulants;
Vit K antagonists
Monitor INR and adjust dose accordingly. Dose adjustment may be required if
switching from ritonavir to cobicistat.
Direct acting
anticoagulant (DOAC)
Significant effect expected (limited data). Effect not routinely measured. Recommended -
avoid with boosted regimens
Calcium channel blockers Increased exposure and potential hypotensive effect. Start with lowest dose and titrate
based on response
Statins Increased exposure of some statins. Simva-, lovastatin contraindicated. Pitavastatin can
be used. Others – start with low dose and titrate.

Integrase Inhibitors and Cation Containing
Medications: Recommendations
Coadministered
Drug
Raltegravir Dolutegravir Elvitegravir/c Bictegravir
Mg/Al containing
antacid
Not
recommended
(NR) bd & qd
Separate well (6h
before/2h after
Separate by
least 4h
Take BIC under
fasting 2h before
Calcium
supplements
No dose
adjustment (bd)
NR - qd
Separate well (6h
before/2h after
Not stated BIC and
supplement can
be taken with
food
Multivitamins Not stated Separate well (6h
before/2h after
Separate by
least 4h
Not stated
Iron supplements Not stated Separate well (6h
before/2h after
Not stated BIC and
supplement can
be taken with
food
Genvoya SmPC 03/18; Tivicay SmPc 03/18.; Isentress SmPC 02/18; Bictarvy PI 02/18

Selected DDI for Integrase Inhibitors
(RAL; DTG; EVG/c; BIC)
Smith JM et al. AIDS 2017, Burgess MJ et al. HIV AIDS 2015; Nachega JB et al. AIDS 2012, www.hiv-druginteractions.org
Drug Class Comment
Antacids
Calcium, Mineral
supplements
Integrase inhibitors form complex with divalent cations in the g.i.tract which limits
absorption. Potential risk of treatment failure.
Metformin DTG increases metformin exposure (inhibits OCT2 in kidney).
EVG/c probably increases metformin exposure.
RAL has no effect.
BIC increases metformin exposure - but less than DTG.
Note: No DDIs with most other antidiabetic drugs.
Rifampicin DTG – Rifampicin decreases DTG exposure.
RAL – Rifampicin decreases RAL exposure
EVG/c – Rifampicin decreases EVG exposure
BIC – Rifampicin decreases BIC exposure
Rifabutin DTG and RAL – no clinically significant change in exposure
EVG/c – Rifabutin decreases EVG exposure
BIC – Rifabutin decreases BIC exposure

REFLATE Trial
(Missing = Failure, Study drug discontinuation = Failure)

INSPIRING: Phase IIb, randomized, multicenter, open-label, non-
comparative, active-control parallel-group study
• ART, antiretroviral therapy; DTG, dolutegravir; EFV, efavirenz; HR, isoniazid, rifampin; HRZE, isoniazid, rifampin, pyrazinamide, ethambutol; NRTI, nucleoside reverse transcriptase inhibitor; RIF, rifampin; TB, tuberculosis.aDuration of continuation phase of TB treatment according to local guidelines (continuation phase up to 7 months in some countries).ClinTrials.gov NCT02178592
HR (4 months)a
Day 1 52 weeks
End of randomized phase24 weeks
DTG (50 mg QD) + 2 NRTIs
Interim analysis: % <50 c/mL
(Snapshot) Primary endpoint at Week 48: % <50 c/mL
(Snapshot)
DTG (50 mg BID) + 2 NRTIs (n = 69)
EFV (600 mg QD) + 2 NRTIs (n = 44)
TB therapy
HIV/TB coinfected
ART-naive adults
Inclusion criteria
• HIV-1 RNA ≥1000 copies/mL and CD4+ ≥50 cells/mm3
• Pulmonary, pleural, or lymph node tuberculosis with RIF-sensitive MTB confirmed by culture or GeneXpert
• RIF-containing TB treatment started up to a maximum of 8 weeks before randomization and no later than the screening date
DTG:EFV 3:2 randomization stratified by
• Screening plasma HIV-1 RNA 100,000 or >100,000
copies/mL
• Screening CD4+ 100 cells/mm3 or >100 cells/mm3
DTG dose switch2 weeks post-completion of TB treatment
Screening
−28 to −14 days
HRZE (2 months)
1. DOOLEY, KE. et al. INSPIRING: Safety and efficacy of dolutegravir-based ART in TB/HIV coinfected adults at week 24. In: CROI, 2018. Disponível em: <http://www.natap.org/2018/CROI/croi_07.htm>. Acesso em: 28 mar. 2018.
Adapted from reference 1

Virologic and Immunologic Results in the
ITT-E Population Through Week 24
-20
0
20
40
60
80
100
-4 0 4 8 12 16 20 24 28
Per
cen
tage
, %
Week
Proportion of Participants With HIV-1 RNA <50 copies/mL, % (95% CI)
DTG (n=69)
EFV (n=44)
81 (72, 90)
89 (79, 98)
Modified FDA snapshot analysis (ITT-E) Pre-dose concentration: DTG 50 mg BID with RIF
Time n DTG Conc (ng/mL)Geomean (90%CI) %CV
Wk 8 41 852 (208-2340) 118
Wk 24 22 942 (19-3380) 276
Pre-dose concentration: DTG 50 mg QD without RIF (post-TB treatment phase)
Time n DTG Conc (ng/mL)Geomean (90%CI) %CV
Wk 36 16 1143 (80-4370) 151
Wk 48 12 591 (19-3310) 359
INSPIRING Pharmacokinetic Data
INSPIRING DTG Ctau when administered twice daily with
RIF were similar to DTG 50 mg once daily without RIF and
to previously reported data for DTG 50 mg once daily in
Phase 2/3 HIV trials.
• Median change from Baseline CD4+ cell count (Q1, Q3) at Week 24: DTG, 146 cells/mm3 (71,
214); EFV 93 cells/mm3 (47, 178)
1. DOOLEY, KE. et al. INSPIRING: Safety and efficacy of dolutegravir-based ART in TB/HIV coinfected adults at week 24. In: CROI, 2018. Disponível em: <http://www.natap.org/2018/CROI/croi_07.htm>. Acesso em: 28 mar. 2018.
Adapted from reference 1

Participants With TB and Non–TB-Associated IRIS
n (%)DTG
(n=69)EFV
(n=44)
Participants with events sent to adjudication committee for TB-associated IRISMet criteria for TB-associated IRISPossibly met criteria for TB-associated IRIS
9 (13)4a (6)
0
12 (27)4b (9)
0
Participants with events sent to adjudication committee for non–TB-associated IRISMet criteria for non-TB-associated IRISPossibly met criteria for non-TB-associated IRIS
2 (3)1c (1)1d (1)
3 (7)00
No participant in either arm permanently discontinued treatment due to IRIS
a1 x Grade 1, 2 x Grade 2 and 1 x Grade 3.b3 x Grade 2 and 1 x Grade 4.cGrade 2 (IRIS and strongyloidiasis; also experienced TB-associated IRIS).dGrade 1 (Herpes zoster).
1. DOOLEY, KE. et al. INSPIRING: Safety and efficacy of dolutegravir-based ART in TB/HIV coinfected adults at week 24. In: CROI, 2018. Disponível em: <http://www.natap.org/2018/CROI/croi_07.htm>. Acesso em: 28 mar. 2018.
Adapted from reference 1

REALITY: RAL Intensification in First-line ART
• Randomized, open-label phase III trial in Uganda, Kenya, Zimbabwe, and Malawi
– Primary endpoint: 24-wk mortality; endpoints assessed via “blinded” adjudication
Gibb DM, et al. CROI 2018. Abstract O23.
▪ Baseline characteristics well balanced between arms
ART-naive adults,
adolescents, and children
with HIV infection;
≥ 5 yrs with CD4+ count
< 100 cells/mm3
(N = 1805)
Follow-up to Wk 48
RAL intensified:
2 NRTI + NNRTI +
additional RAL
(n = 902)
Standard ART:
2 NRTI + NNRTI
(n = 903)
Standard ART:
2 NRTI + NNRTI
Wk 12 Wk 24

RAL Intensification of First-line ART:
HIV-1 RNA and All-Cause Mortality
• 24-wk mortality rate
– RAL intensified: 10.9%
– Standard ART: 10.2%
– HR: 1.10 (95% CI: 0.82-1.46; P = .53)
• 48-wk mortality rate– RAL intensified: 12.4%
– Standard ART: 13.0%
– HR: 0.98 (95% CI: 0.76-1.28; P = .91)
Gibb DM, et al. CROI 2018. Abstract O23. Reproduced with permission.
RAL Intensified
Standard ART
Overall P < .0001
Wks Since Randomization (ART Initiation)
HIV
-1 R
NA
< 5
0 c
/mL,
% (
95%
CI)
P value: < .0001 < .0001 .36 .47
100
80
60
40
20
0
0 4 12 24 48
80.7%76.7%
71.9%
41.0%
13.4%
51.7%
74.7%79.2%
HIV-1 RNA < 50 copies/mL at Wk 48 (ITT)

RAL Intensification of First-line ART: IRIS-
Compatible Events and Prophylaxis Outcomes
• No impact of additional RAL on
IRIS-compatible eventsGibb DM, et al. CROI 2018. Abstract O23. Slide credit: clinicaloptions.com
IRIS-Compatible
Events,* n (%)
RAL
Intensified
Standard
ART
All fatal events
▪ TB-IRIS
▪ Cryptococcal-IRIS
▪ Other of known
etiology
▪ Unknown etiology
36 (4.0)
20 (2.2)
8 (0.9)
5 (0.6)
3 (0.3)
31 (3.4)
21 (2.3)
5 (0.6)
4 (0.4)
1 (0.1)
All fatal/nonfatal events
▪ TB-IRIS
▪ Cryptococcal-IRIS
▪ Other of known
etiology
▪ Unknown etiology
89 (9.9)
53 (5.9)
15 (1.7)
17 (1.9)
4 (0.4)
86 (9.5)
54 (6.0)
16 (1.8)
14 (1.6)
2 (0.2)
*P > .05 for all comparisons.
Independent Predictor of
Fatal/Nonfatal IRIS Events
sHR
(95% CI)
P
Value
RAL intensified vs standard ART1.08
(0.80-1.45).63
Enhanced vs standard
prophylaxis
0.60
(0.44-0.82).001
CD4+ count (per 10 cells/mm3
higher)
0.87
(0.82-0.93)< .001
Age at last birthday (per yr older) .03
▪ ≤ 29 yrs 1.07
(1.02-1.22).008
▪ ≥ 30 yrs 0.99
(0.97-1.01).44
Current TB disease at ART
initiation
1.62
(1.11-2.37).01

Differences in the DDI Profile of TDF & TAF
TDF TAF Potential Mechanism
Rifabutin NR Induction of P-gp
Rifampicin NR* Induction of P-gp
Rifapentine NR Induction of P-gp
Carbamazepine CA Induction of P-gp
Oxcarbazepine CA Induction of P-gp
Phenobarbitone CA Induction of P-gp
Phenytoin CA Induction of P-gp
St John’s Wort NR Induction of P-gp
Data from: www.hiv-druginteractions.org ; Descovy SmPC Oct 017; Custodio JM, EACS 2017.
NR = Not Recommended
CA = Consider Alternative
*TAF BD + RIF data presented at EACS 2017





• INSTIs are widely recommended as the preferred third drug in first line therapy
• All INSTIs are generally well tolerated*
• Occasional reports of insomnia, depression, and suicidal ideation, primarily in
patients with a history of psychiatric illnesses
• Treatment-emergent mutations that confer resistance are very uncommon in
patients receiving INSTIs as part of a three-drug regimen for initial therapy
• In addition to differences in resistance profile, INSTIs differ considerably in
potential drug-drug interactions that can have important clinical implications
• Drug-drug interactions, safety profile, and cost may affect the choice of the
backbone and of INSTI
*Except for DTG in some European cohorts, with up to 16% discontinuation rates due to AEs
Conclusions

• David Back
• Mark Boyd
• Kees Brinkman
• Carlos Brites
• Ricardo Diaz
• Valdez Madruga
• Anton Pozniak
• Jonathan Shapiro
Acknowledgements

OBRIGADO !!!!