Embed Size (px)
Citation preview
Progress of newborn screening for spinal muscular atrophy
Sara Shu-Chuan Chiang, Nancy Yin-Hsiu Chien, Paul Wuh-Liang Hwu
Department of Medical Genetics & Pediatrics, National Taiwan University Hospital, Taipei, Taiwan
This project is supported by Biogen. The authors denied any other conflict of interest.
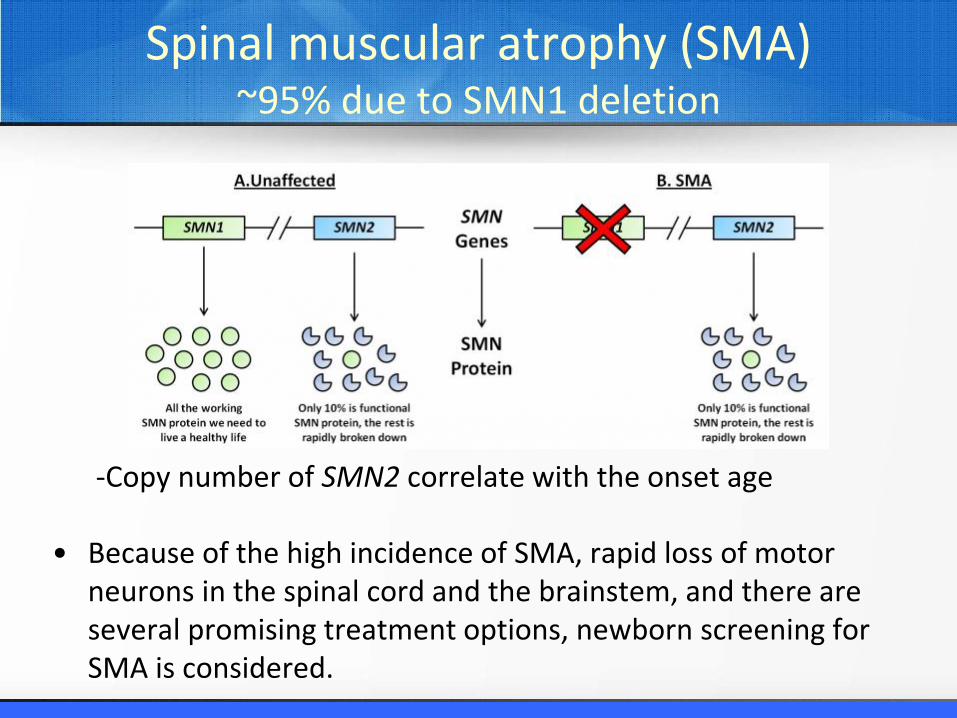
Spinal muscular atrophy (SMA)~95% due to SMN1 deletion
-Copy number of SMN2 correlate with the onset age
• Because of the high incidence of SMA, rapid loss of motor neurons in the spinal cord and the brainstem, and there are several promising treatment options, newborn screening for SMA is considered.
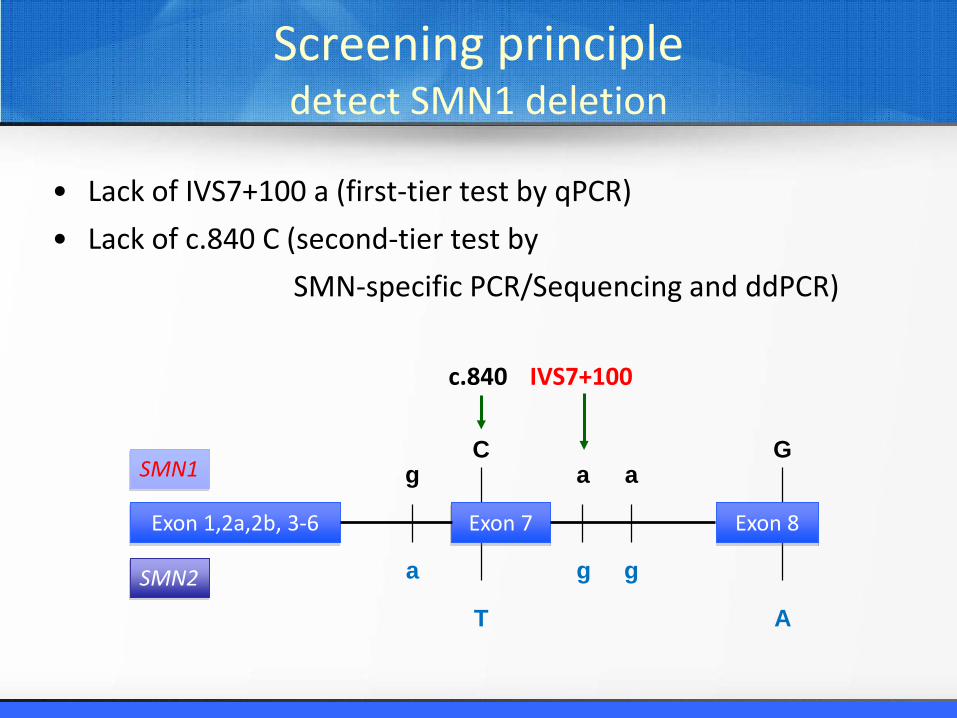
Screening principledetect SMN1 deletion
• Lack of IVS7+100 a (first-tier test by qPCR)• Lack of c.840 C (second-tier test by
SMN-specific PCR/Sequencing and ddPCR)
IVS7+100
SMN1
SMN2
Exon 1,2a,2b, 3-6 Exon 7 Exon 8
a
g
C
T
c.840
a
g
g
a
G
A
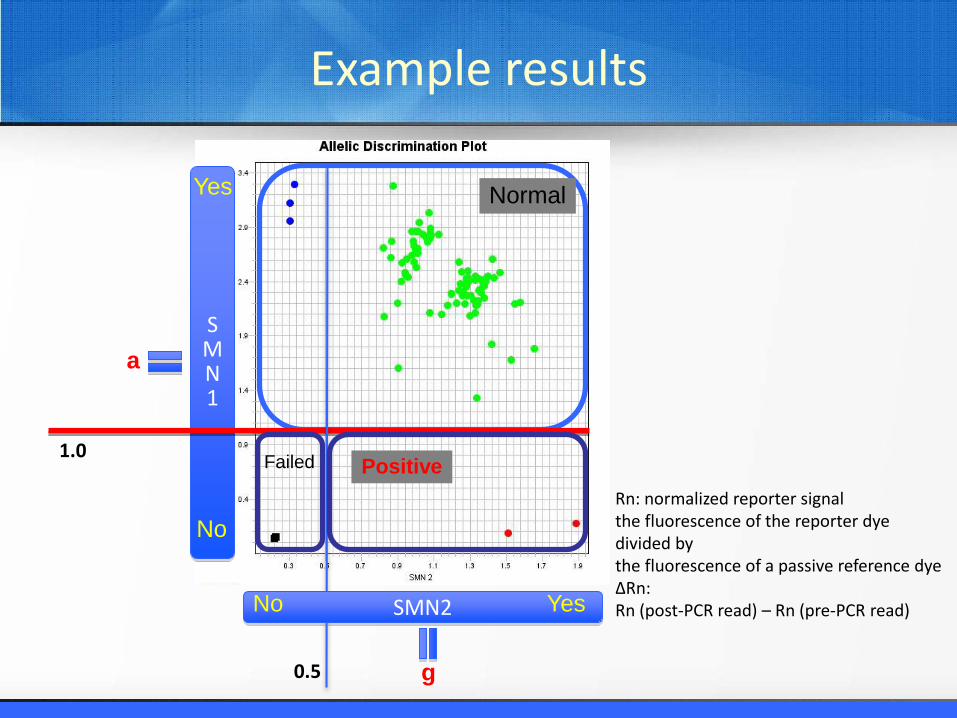
Rn: normalized reporter signalthe fluorescence of the reporter dye divided by the fluorescence of a passive reference dye∆Rn:Rn (post-PCR read) – Rn (pre-PCR read)
Normal
SMN1
Yes
a
PositiveFailed
SMN2No Yes
No
g
1.0
0.5
Example results
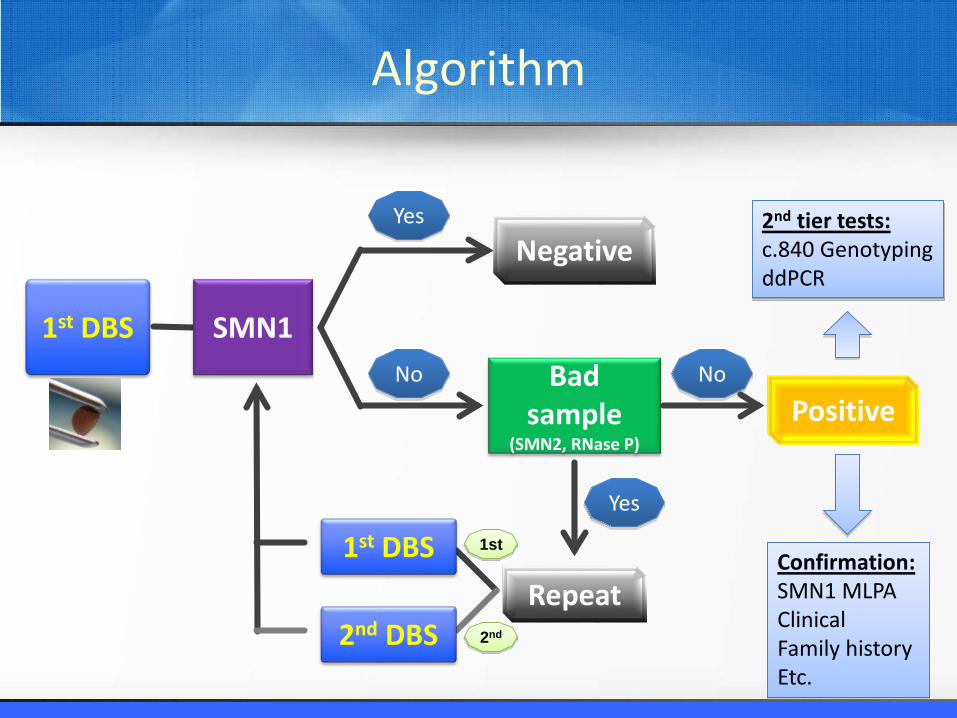
Repeat
Positive
Negative
1st DBS
1st DBSYes
No
Yes
Bad sample
(SMN2, RNase P)
No
2nd DBS
1st
2nd
SMN1
Confirmation:SMN1 MLPAClinicalFamily historyEtc.
2nd tier tests:c.840 GenotypingddPCR
Algorithm
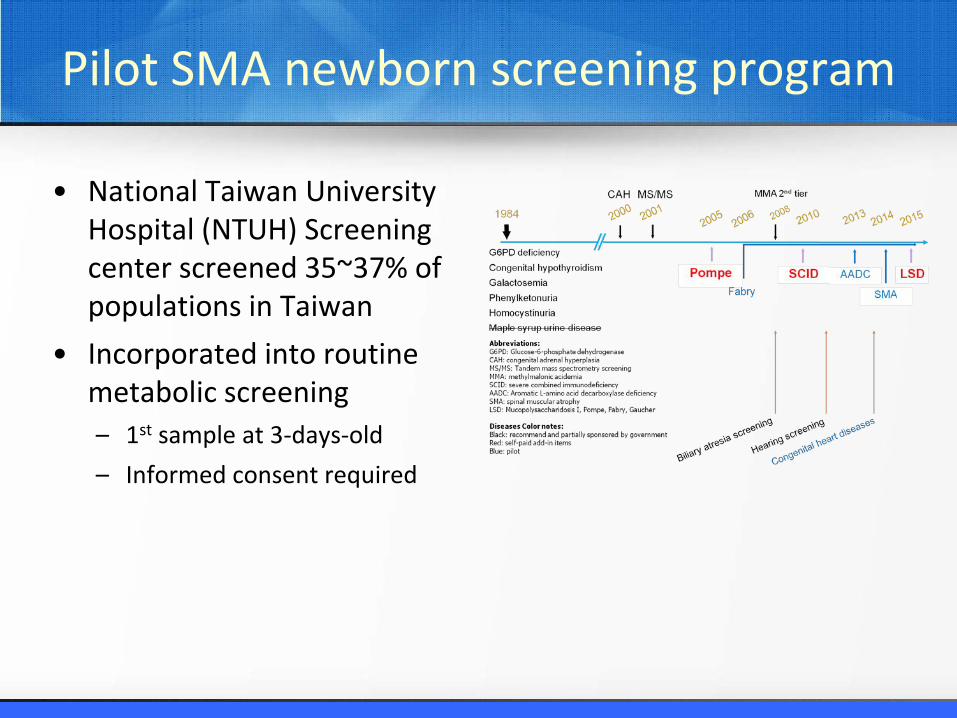
Pilot SMA newborn screening program
• National Taiwan University Hospital (NTUH) Screening center screened 35~37% of populations in Taiwan
• Incorporated into routine metabolic screening– 1st sample at 3-days-old – Informed consent required
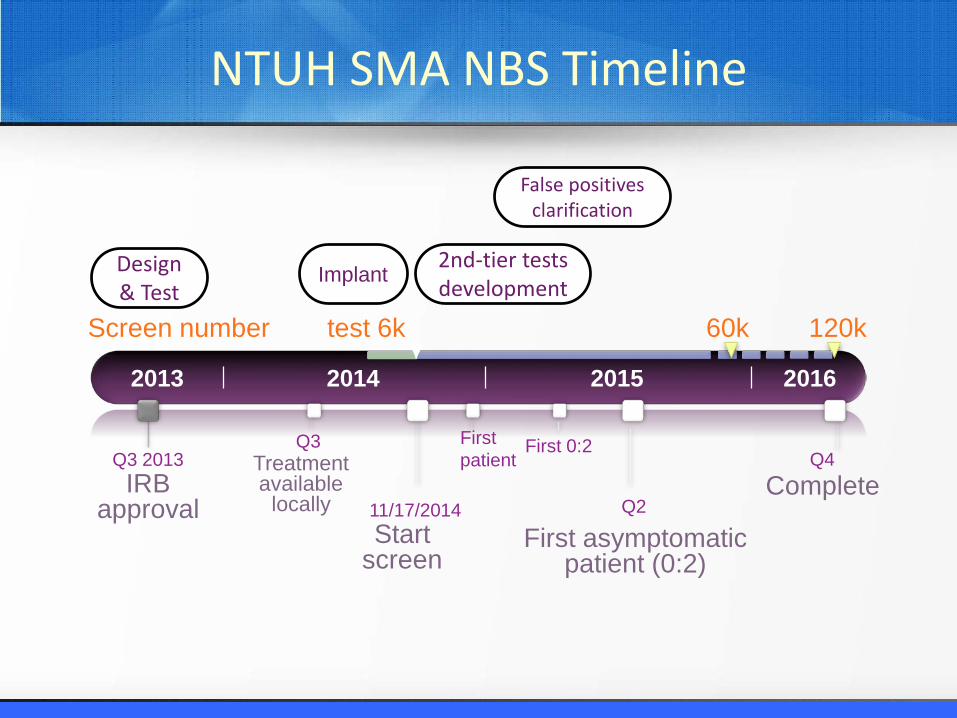
False positives clarification
2nd-tier tests developmentImplantDesign
& Test
2013 2014 2015 2016
60k
CompleteQ4
First asymptomatic patient (0:2)
First patient
Start screen
11/17/2014
Treatment available
locally
Q3
IRB approval
Q3 2013
Q2
First 0:2
test 6k Screen number 120k
NTUH SMA NBS Timeline
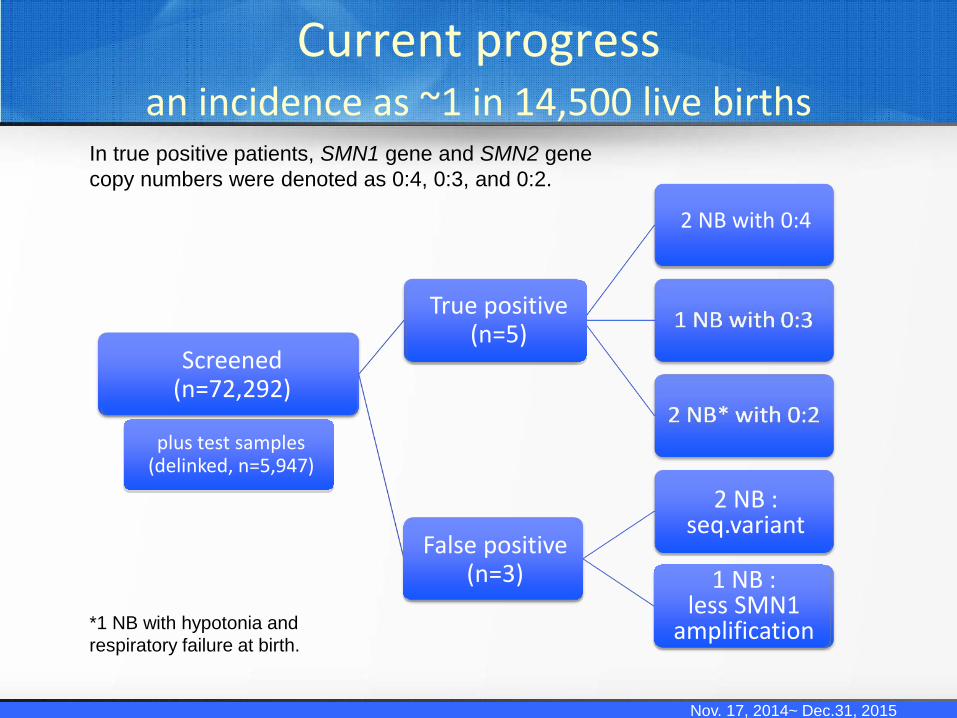
Current progress an incidence as ~1 in 14,500 live births
Nov. 17, 2014~ Dec.31, 2015
*1 NB with hypotonia and respiratory failure at birth.
In true positive patients, SMN1 gene and SMN2 gene copy numbers were denoted as 0:4, 0:3, and 0:2.
True positive(n=5)
False positive(n=3)
Screened(n=72,292)
2 NB with 0:4
1 NB :less SMN1
amplification
2 NB : seq.variant
plus test samples (delinked, n=5,947)
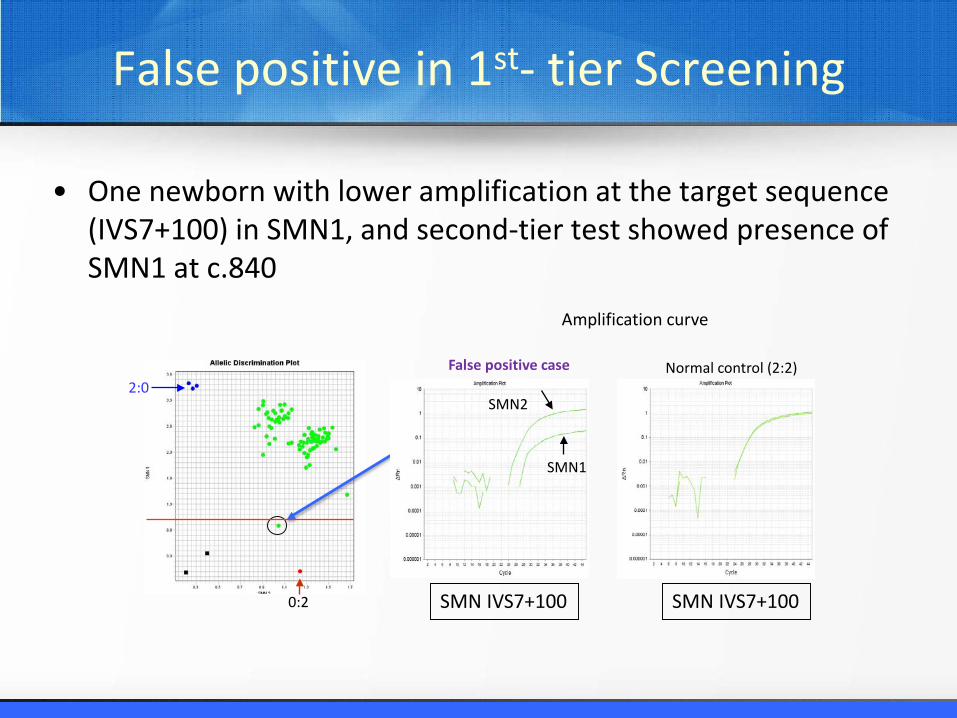
False positive in 1st- tier Screening
• One newborn with lower amplification at the target sequence (IVS7+100) in SMN1, and second-tier test showed presence of SMN1 at c.840
0:2
2:0Normal control (2:2)
SMN1
SMN2
SMN IVS7+100SMN IVS7+100
False positive case
Amplification curve
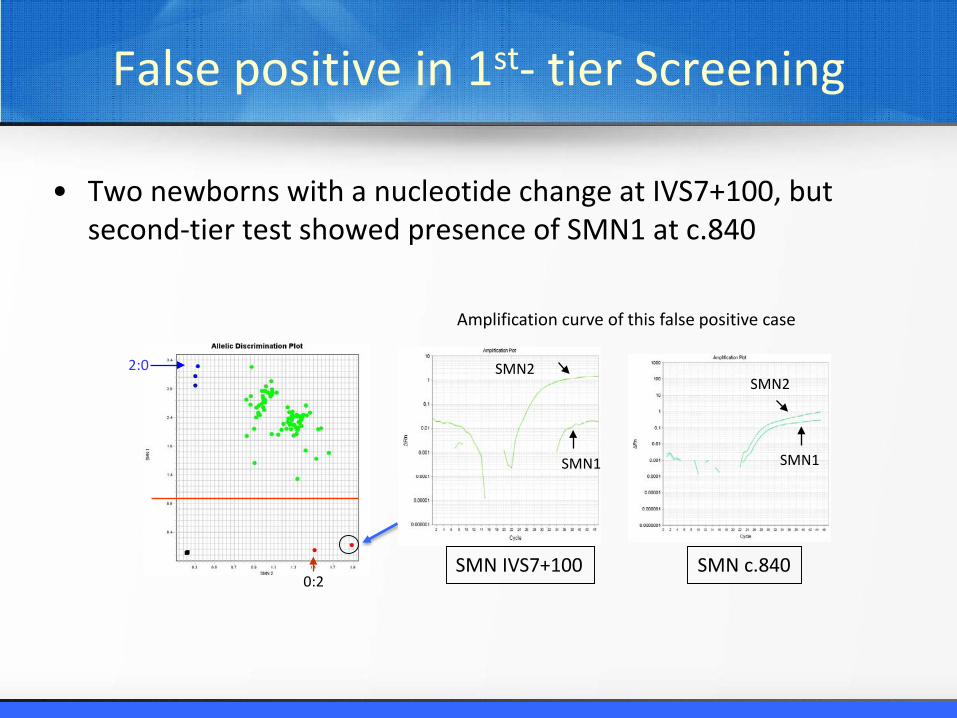
False positive in 1st- tier Screening
• Two newborns with a nucleotide change at IVS7+100, but second-tier test showed presence of SMN1 at c.840
2:0
0:2
SMN1
SMN2
SMN IVS7+100 SMN c.840
SMN1
SMN2
Amplification curve of this false positive case
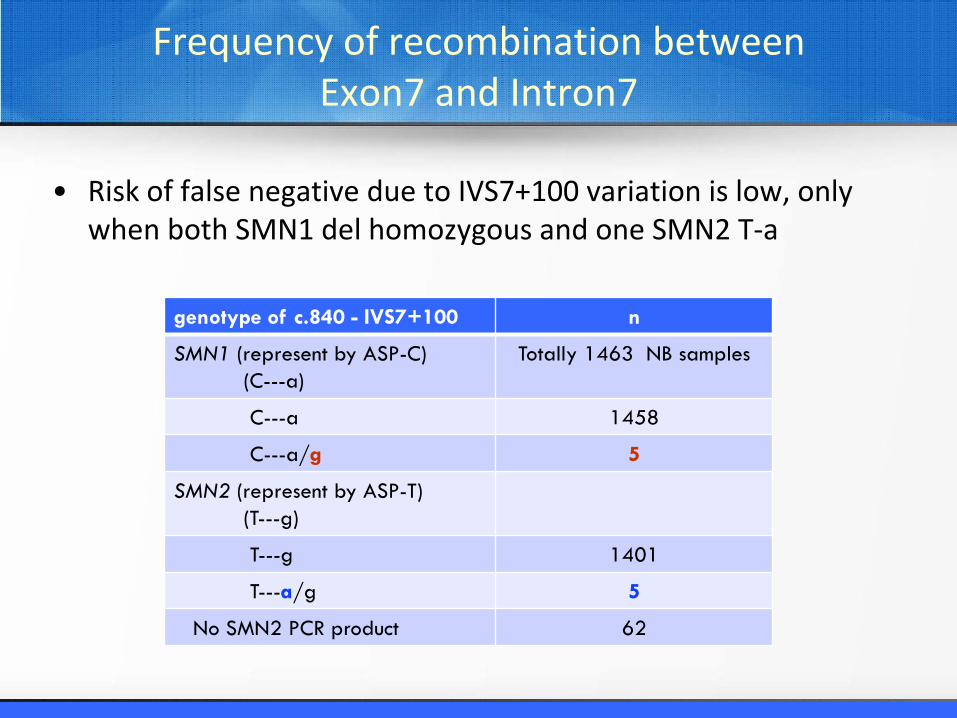
Frequency of recombination between Exon7 and Intron7
• Risk of false negative due to IVS7+100 variation is low, only when both SMN1 del homozygous and one SMN2 T-a
genotype of c.840 - IVS7+100 n
SMN1 (represent by ASP-C)(C---a)
Totally 1463 NB samples
C---a 1458
C---a/g 5
SMN2 (represent by ASP-T)(T---g)
T---g 1401
T---a/g 5
No SMN2 PCR product 62
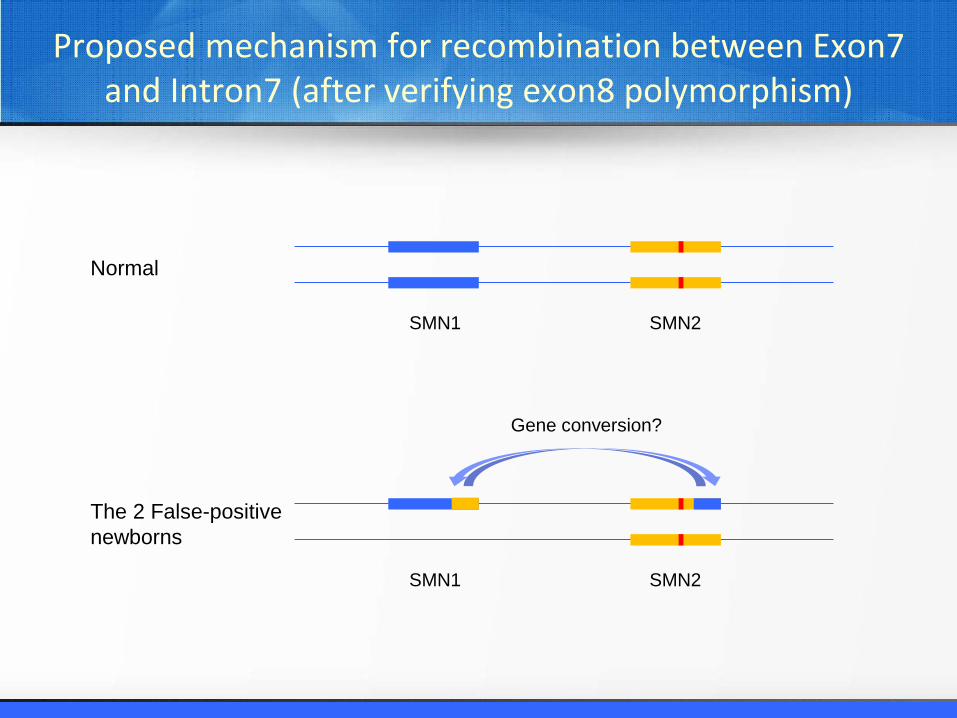
Proposed mechanism for recombination between Exon7 and Intron7 (after verifying exon8 polymorphism)
SMN1 SMN2
SMN1 SMN2
Gene conversion?
Normal
The 2 False-positive newborns
Conclusion
• The incidence of SMA in our newborn population is 1 in 14,500 (95% Confidence interval 1 in 6,176~33,849).
• Doing only 1st-tier has very low false positive, and the positive prediction rate is 62.5%. – Combining with 2nd-tier test, such as assay at c.840 either
by Genotyping assay or ddPCR, can largely improve the screening performance
– The theoretically false negative rate was 5% since we only detect SMN1 deletion homozygous patients.
Acknowledgement
• National Taiwan University Hospital– Department of Pediatrics
• Wang-Tso Lee• Wen-Chin Weng• Wu-Shiun Hsieh• Yuh-Jyh Jong
– Newborn Screening Center• Jin-Jer Lin• Li-Wen Hsu• An-Ju Lee
• CDC– Newborn Screening and Molecular Branch (NSMBB)
• Biogen





























