Embed Size (px)
Citation preview

CASE REPORT
Sonography of multifocal hydatidosis involving lung and liverin a female child
Abhishek Jha • Ekram Ullah • Prakhar Gupta •
Gagan Gupta • Mohd. Saud
Received: 17 December 2012 / Accepted: 27 February 2013 / Published online: 11 April 2013
� The Japan Society of Ultrasonics in Medicine 2013
Abstract Hydatid disease, caused by Echinococcus
granulosus, is a zoonotic infection encountered worldwide.
Though involvement of the liver and lungs is quite com-
mon, pelvic involvement is rarely reported, with the inci-
dence being 0.2–2.2 %. Ovarian and broad ligament
hydatids are rare entities and are usually seen after rupture
of a hepatic hydatid cyst. These cysts are usually asymp-
tomatic, and a high index of clinical suspicion coupled with
unequivocal imaging findings is required to make an
accurate and timely diagnosis. We present a case of mul-
tifocal hydatid disease in a female child involving the lungs
and liver and provide an account of the quintessential
radiological findings.
Keywords Hydatidosis � Lung hydatid � Hepatic hydatid �Double wall � Ultrasound
Introduction
Hydatid disease is a parasitic zoonosis caused by the larval
stage of Echinococcus granulosus and, uncommonly,
Echinococcus multilocularis. Canines are the definite hosts
of Echinococcus, and human beings and cattle are inter-
mediate hosts. Epidemiologically, it is found everywhere in
the world, and is especially common in Asian and African
countries. The most common organ to be involved in
hydatid disease is the liver (60–70 %), followed by the
lungs (10–25 %), while ovarian and parametrial involve-
ment is extremely uncommon [1]. Multiorgan involvement
is exceedingly rare and occurs in less than 2 % of the cases.
Diagnosis is usually established by serological tests and
radiological imaging. The optimal treatment of such cases
includes albendazole followed by surgical excision.
Case report
An 8-year-old female child from a rural background pre-
sented to the pediatric outpatient department with com-
plaints of difficulty in breathing and recurrent abdominal
pain. The patient had no history of any other chronic ill-
ness. On examination, vital signs of the patient were stable.
General examination revealed pallor. On respiratory
examination, there was reduced air entry bilaterally, and
fine crepitations were auscultated in bilateral lung bases.
Abdominal examination revealed tender hepatomegaly.
The rest of the examination was within normal limits.
Preliminary routine investigations revealed raised
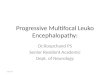
eosinophil count (17 %). Chest radiograph of the patient
revealed large, well-defined, spherical radio-opaque shad-
ows, with no air–fluid levels or apparent calcification, in
bilateral mid lung zones (Fig. 1). The medial border of the
right-sided lesion was indistinct from the right cardiac
border. There was no evidence of effusion. The patient was
then subjected to abdominal ultrasound examination, which
revealed hepatomegaly, with multiple multilocular cystic
lesions with multiple internal septations, and no
A. Jha � E. Ullah � G. Gupta � Mohd. Saud
Department of Radiodiagnosis, Jawaharlal Nehru Medical
College, Aligarh Muslim University, Aligarh, India
A. Jha (&)
Defender Locks and Hardware, Achal Tank,
Aligarh 202001, India
e-mail: [email protected]
P. Gupta
Department of General Surgery, Jawaharlal Nehru Medical
College, Aligarh Muslim University, Aligarh, India
123
J Med Ultrasonics (2013) 40:471–474
DOI 10.1007/s10396-013-0444-5

calcifications, distributed in both lobes of the liver (Figs. 2,
3). No free fluid was detected. A provisional diagnosis of
multifocal hydatid disease was made.
Thereafter, the patient underwent computed tomography
(CT) scanning of the thorax and the abdomen to confirm
the diagnosis, ascertain the extent of the lesion, and rule out
other possibilities. Contrast-enhanced CT scan of the tho-
rax revealed well-defined, unilocular, spherical, fluid
attenuation, cystic lesions with minimally enhancing walls
in the right middle lobe and left lower lobe (Fig. 4). There
was no evidence of calcifications within the lesions. No
definite mediastinal lymphadenopathy was noted, and no
apparent communication with bronchi was seen. CT scan
of the abdomen revealed multiple multilocular cystic
lesions, with thick internal septations producing a honey-
comb or cartwheel appearance. These lesions were present
in both hepatic lobes (Fig. 5).
ELISA for echinococcal immunoglobulin E was
49.7 Ku/L. The clinical picture combined with the radio-
pathological appearance strongly favored the diagnosis of
multifocal hydatidosis. The patient was started on alben-
dazole, and after 2 weeks she was taken up for surgery.
A midline incision was made and the surgical field
involving the peritoneal cavity was packed with sponges
dipped in 0.5 % silver nitrate. The largest of the hepatic
cysts was then aspirated through a suction device and
daughter cysts were evacuated. The residual pericystic
cavity was then filled with normal saline and closed by
purse-string sutures. Three more similar cysts were excised
in this fashion. The cyst wall was sent for histopathological
examination, which confirmed the diagnosis of hydatid
cyst. No postoperative complications were seen. No defi-
nite surgical procedure was planned for pulmonary hydatid
cysts, which showed marked regression in size following
medical therapy.
Discussion
Hydatid disease is worldwide in distribution and is espe-
cially common in countries where animal husbandry is
largely practiced. The most common organs to be involved
include the liver and lungs. Many authors report pulmonary
involvement to be the commonest in the pediatric popu-
lation [2, 3]. It is hypothesized that increased compliance
of lung tissue as compared to the liver favors expansion
and growth of these cysts. Pelvic hydatid cysts are rarely
primary and are most commonly seen secondary to inoc-
ulation from rupture of a hepatic hydatid [4–6].
Clinically, these cysts are usually asymptomatic when
small. With growth in size, symptoms secondary to a mass
effect of these cysts arise. Large hepatic hydatid cysts may
cause abdominal pain and obstructive jaundice. Cough and
chest pain are the most common features of pulmonary
hydatids. Symptoms may also arise due to complications
like rupture of cyst, secondary infection, and formation of
cystobiliary fistulas, which may include anaphylaxis, urti-
caria, or cholangitis.
Pathologically, hydatid cysts consist of three layers. The
outermost layer is fibrous and is called pericyst. It is
formed due to inflammatory changes secondary to activa-
tion of the immune system of the host. Pericyst is absent in
hydatid cysts located in brain and lungs. The middle layer
is acellular and is called the laminar membrane or the
ectocyst, and the inner layer is the germinal layer, which is
the vital layer and harbors the parasites, also known as
endocyst [7, 8]. The fluid within the cyst is alkaline and is
highly antigenic. Peritoneal spillage of this fluid can result
in severe anaphylactic reaction.
Imaging plays a pivotal role in the diagnosis of these
lesions. The most common imaging modalities include
ultrasonography, CT scan, and magnetic resonance imaging
Fig. 1 Chest X-ray
posteroanterior and lateral
views showing large, well-
defined, spherical, radio-opaque
shadows, with no air–fluid
levels or apparent calcification,
in bilateral mid lung zones
472 J Med Ultrasonics (2013) 40:471–474
123

(MRI). Plain chest radiograph is a valuable tool in the initial
diagnosis of pulmonary hydatid. Several radiographic signs
of pulmonary hydatid cysts have been described in the lit-
erature, including notch sign, water-lily sign, meniscus sign,
annular solar eclipse, and the migratory sign.
Ultrasonography is an essential tool in the diagnosis of
hydatid cysts. Several sonographic signs have been
described in relation to hydatid cysts. On ultrasonography,
the cyst wall is seen as two echogenic lines separated by
linear hypoechogenicity [9], the so-called ‘‘double wall’’
sign. The motion of fine echogenic debris with change in
the patient’s posture can be well appreciated, and is also
referred to as the ‘‘snow storm’’ sign [9]. Detachment of the
endocyst from the pericyst can result from trauma,
degeneration or host tissue reaction. In such cases, visible
‘‘floating membranes’’ can be appreciated within the cyst.
In some cases, a focal rent in the wall can also be noticed.
When the detachment is complete, the sonographic ‘‘water-
lily sign’’ can be seen, which is so named because of the
resemblance of pulmonary hydatids to waterlily. With
disease progression, the physical properties of the hydatid
fluid also undergo transition from watery to more viscid
fluid, resulting in the folds of the germinal layer becoming
immobile and being seen as serpentine structures entrapped
within an echogenic matrix. This appearance is called the
‘‘congealed water-lily’’ sign. Daughter cysts are visualized
as multiple cysts separated from each other by well-defined
walls and may give rise to a multilocular or honeycomb
appearance of these lesions. In conditions where the cyst
cavity is completely obliterated by the matrix, the cyst may
appear as a solid mass [10]. Calcification, both within the
wall as well as within the matrix, can also be well depicted
by ultrasound. Ultrasound stands out as the most sensitive
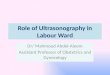
Fig. 3 Transabdominal ultrasonography with a 3.75-MHz curvilinear
probe showing multiple small anechoic cysts within a larger cyst,
referred to as ‘‘daughter’’ cysts
Fig. 4 Contrast-enhanced CT scan of the patient shows cystic lesions
with well-defined spherical fluid intensity and high attenuation wall in
the right middle lobe in the paracardiac location and the left lower
lobe, with no evidence of calcification, air–fluid level, or daughter
cysts
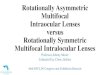
Fig. 2 a Transabdominal ultrasonography with a 3.75-MHz curvi-
linear probe showing well-defined multilocular cystic lesions in the
right hepatic lobe giving rise to a honeycomb appearance and b the
same lesion with a linear 7.5-MHz probe showing the ‘‘double wall’’
of these cystic lesions. Note the outer wall (straight white arrow)
representing the pericyst and the inner layer (curved white arrow)
representing the ectocyst. No definite evidence of calcifications is
seen
J Med Ultrasonics (2013) 40:471–474 473
123

imaging modality in detection of septa, membranes, and
hydatid sand [9].
CT scan clearly depicts most of the findings that are
seen on sonography. On contrast-enhanced CT scan, these
cysts show a high attenuation wall. Calcifications, detached
membranes, and daughter cysts can be easily seen on CT
scan. CT scan is also the investigation of choice in detec-
tion of cyst infection. On MRI, these cysts contain a hyp-
ointense peripheral rim on T2W sequences, which is
represented by pericyst, which is rich in collagen [11]. The
daughter cysts are hypointense on T1W sequences and
hyperintense on T2W sequences in comparison with cyst
fluid. Ovarian and broad ligament hydatids are extremely
rare, and in a review of 532 cases by Bickers et al. [12],
only two cases of broad ligament hydatids were identified.
Most of the ovarian hydatid cysts are seen in elderly and
middle-aged females. The treatment of hydatid disease is
chiefly surgical, and albendazole is given preoperatively to
reduce their size. The overall prognosis of these cysts is
good with reported recurrence of 7–14 % [13]. Recurrence
is chiefly attributed to rupture of the cyst. In cases of
ovarian hydatids, cystectomy is the treatment of choice,
while complete cyst excision with preservation of maxi-
mum possible pulmonary tissue is advocated for lung
hydatids.
Conflict of interest The authors report no conflict of interest.
References
1. Tsaroucha AK, Polychronidis AC, Lyrantzopoulos N, et al.
Hydatid disease of the abdomen and other locations. World J
Surg. 2005;29:1161–5.
2. King CH. Cestodes (tapeworms). In: Mandell GL, Bennet JE,
Dolin R, editors. Principles and practice of infectious disease. 6th
ed. New York: Churchill Livingstone; 2005. p. 3290–2.
3. Karaoglanoglu N, Kurkcuoglu IC, Gorguner M, et al. Giant
hydatid lung cysts. Eur J Cardiothorac Surg. 2001;19(6):914–7.
4. Gueddana F, Chemmen Lebbene L, Lebi I, et al. Intrauterine
hydatidosis: a case report. J Obstet Gynecol Reprod Biol (Paris).
1990;19:725–7.
5. Komongui DG, Diouf A, Dao B, et al. Hydatid cyst of the uterus
(apropos of a case seen at the gynecologic and obstetrical clinic
of the C.H.U. of Dakar). Dakar Med. 1990;35:162–7.
6. Tarcoveanu E, Dimofte G, Bradea C, et al. Multiple peritoneal
hydatid disease after rupture of a multivesicular hepatic hydatid
cyst: case report. J Gastrointestin Liver Dis. 2006;15:301–5.
7. Pumarola A, Rodriguez-Torres A, Garcıa-Rodriguez JA, et al.
Microbiologıa y parasitologıamedica. 2nd ed. Spain: Salvat;
1990.
8. King CH. Cestodes (tapeworms). In: Mandell GL, Bennett JE,
Dolin R, editors. Principles and practice of infectious diseases.
4th ed. New York: Churchill Livingstone; 1995. p. 2544–53.
9. Moguillanski SJ, Gimenez CR, Villavicencio RL. Radiologıa de
la hidatidosis abdominal. In: Stoopen ME, Kimura K, Ros PR,
editors. Radiologıa e imagendiagnostica y terapeutica: abdomen,
vol. 2. Philadelphia: Lippincott Williams & Wilkins; 1999.
p. 47–72.
10. Gharbi HA, Hassine W, Brauner MW, et al. Ultrasound exami-
nation of the hydatid liver. Radiology. 1981;139:459–63.
11. Davolio SA, Canossi GC, Nicoli FA, et al. Hydatid disease: MR
imaging study. Radiology. 1990;175:701–6.
12. Bickers WM. Hydatid disease of the female pelvis. Am J Obstet
Gynaecol. 1970;107:477–83.
13. Xu MQ. Hydatid disease of the lung. Am J Surg. 1985;150(5):
568–73.
Fig. 5 Contrast-enhanced CT
scan of the abdomen showing a
multilocular cystic lesion with a
‘‘cart-wheel’’ appearance in the
right hepatic lobe (white arrow)
and another lesion with
daughter cysts (black arrow)
474 J Med Ultrasonics (2013) 40:471–474
123