Embed Size (px)
DESCRIPTION
medicina
Citation preview

Neurological disorders with sleep alterations
Cristina Panea, MD, PhDElias Emergency University
Hospital Bucharest
Why the neurologists should be interested
by sleep study ?
The brain is their domain
Because they know
The brain Structural, pathophysiologic,
neurochemical support Generation of sleep: pons, midbrain,
hypothalamus, thalamus REM state: cholinergic and aminergic nuclei
– tegmentum of the pons and midbrain non-REM state: serotoninergic nuclei of the
upper brain stem tegmentum and anterior hypothalamus, reticular nucleus of the thalamus (sleep spindles)

Any abnormality
Alter sleep Generate
symptoms and signs complications prognosis
Why the neurologists should be interested
by sleep study ?
Because they can
Sleep study – based on electrophysiological examinations
PSG
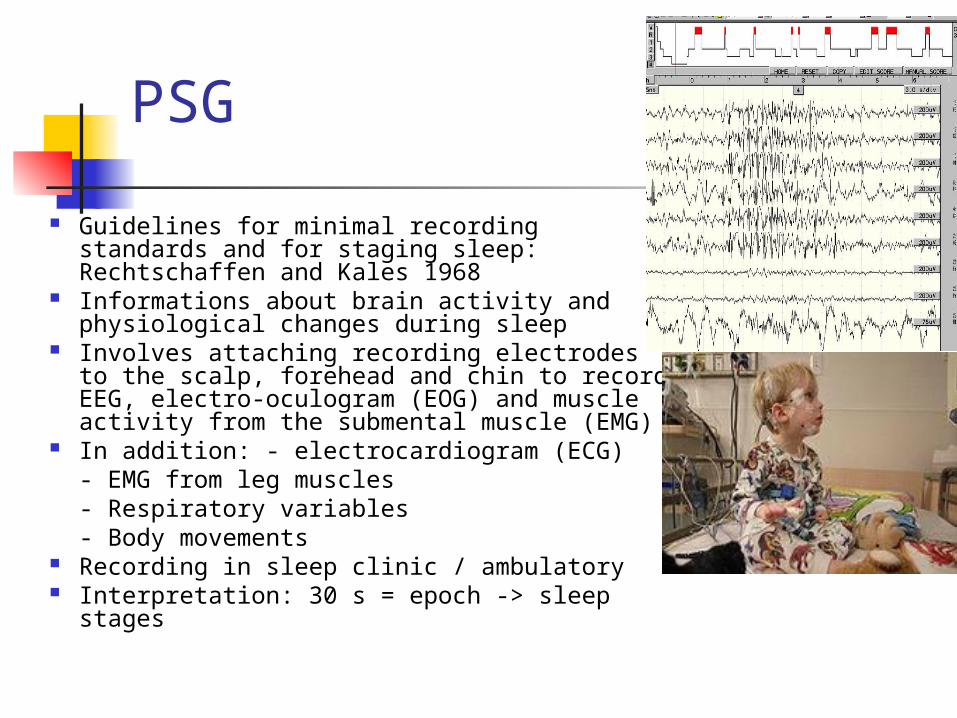
Guidelines for minimal recording standards and for staging sleep: Rechtschaffen and Kales 1968
Informations about brain activity and physiological changes during sleep
Involves attaching recording electrodes to the scalp, forehead and chin to record EEG, electro-oculogram (EOG) and muscle activity from the submental muscle (EMG)
In addition: - electrocardiogram (ECG)- EMG from leg muscles- Respiratory variables- Body movements
Recording in sleep clinic / ambulatory Interpretation: 30 s = epoch -> sleep stages

PSG reports
Time in bed (TIB) Sleep onset Sleep onset latency Sleep period Total sleep time Nb of awakenings Sleep efficiency Wake after sleep
onset REM onset latency Time in each sleep
stage Sleep stages (%)
Apnoea – hypopnea index Desaturation index PLMS index (index of number of
leg movements per hour
Multiple sleep latency (MSLT)
Objectively assessing a person`s propensity to sleep in the daytime Excessive daytime sleepiness Narcolepsy Detection sedative /
awakening effects of drugs Several times (4 x 20 min)
per day, after an overnight sleep recording
EEG, EMG -> sleep onset, REM latency, sleep stages

Actigraphy
Method of monitoring movements over days or weeks in real-life situations Small wrist- worn monitor containing an accelerometer -
> electrical impulses in response to movements, stored in a digital memory
Records both intensity and duration of movements Non-compliants patients: infants, dementia
Limits: wakefulness is associated with moving, sleep is associated with being still Accompanied by daily diary Followed by PSG
Parkinson`s diseaseInteractions between movement disorder, damage to brain area
controlling sleep, dopaminergic medication- spindle activity reduced – enhanced with L-Dopa
Excessive daytime sleepiness 20-50% pts: higher disease severity, higher doses of L-Dopa,
dopamine agonists Sleepness narcolepsy-like (sleep onset REM periods)
Insomnia Nocturia, nighttime incontinence, pain, restless leg syndrome,
periodic limb movements REM sleep behaviour disorder
> 30% Even daytime Hallucinations Phasic muscle activity (~ specific for synucleinopathies)
Arnulf 2000, 2006; Onofrj 2002; Bilwise DL, 2004

Shy-Drager syndromeNocturnal hypotension, lesions in pontine tegmentum,
reticular formation, nucleus ambiguus, anterior horn of C and T spinal cord
REM sleep behaviour disorder and REM without atonia – can precede the onset of typical neurologic deficits by 2-3 years
Sleep apnea, dysrythmic patterns of respiration, respiratory arrest – DEATH
Laryngeal stridorCastaine P, 1977Briskin JG, 1978Chokroverty S, 1988Bannister R, 1981

Indeterminate sleep
= Electrographic features of wakefulness in association with behavioral sleep, poor definition of sleep stages
Sleep generators in pontine tegmental structures
Progressive Supranuclear Palsy Sleeplesness, reduction sleep time, poor development of
sleep spindles Olivopontocerebellar degeneration
Sleep apnea syndromes, REM without atonia Spinocerebellar degeneration
Sleep time reduced (absence REM), breathing irregularities – DEATH
Aldrich MS, 1989
Chokroverty S, 1984Osorio I,
1980
Huntigton`s Chorea Global brain atrophy, caudate nc and putamen
Insomnia – even before neurologic manifestation
Reduced SWS, REM Sleep fragmentation
Increased density and amplitude of sleep spindle – high level of cerebral dopamine ?
Puca FM, 1973

Dementia Sleep-wake alterationExcessive sleep fragmentationInsomnia – worsening of executive attention and working
memory (preF cortex more susceptible to sleep deprivation) Alzheimer`s Disease
Disturbance of the central cholinergic system centered in the nucleus basalis of Meynert ->generation REM => REM sleep latency prolonged + REM percentage decreased
Respiratory disturbaces, increased periodic limb movements Vascular dementia
Sleep apneas and hypopneas – related to worsening dementia (hemodynamic and cardiac changes)
REM sleep disorders: lacunar infarction of pontine tegmentum, leucoaraiosis / ischemic subcortical leukoencephalopathy (supratentorial system modulate REM atonia and stereotypic behaviours)
Vitiello MV, 1984Culebras A, 1992; Zee PC,
2005; Durmer JS, 2005

Stroke Short sleep duration associated with increased
incident of CVD due to a prothrombotic state
Acute phase Inversion of sleep-wake rhythm – recovery in 6 months Sleep apnea (obstructive / central)
Chronic phase Large infarct (right): increase amounts of SWS, loss of
sleep spindles – poor prognosis for survivalCulebras A,
1983Hachinski V,
1977Stiles S, 2007Barclay L, 2008Moul DE, 2009
Headache
Secondary: brain tumors, depression, systemic hypertension, sleep apneas, seizures, bruxism
Primary: Cluster headache
75% attacks occur in sleep 50% REM related
Paroxysmal hemicrania REM related: “REM sleep-locked headache”
Migraine Provoked or attenuated by sleep Sleep hygiene Interactions between migrain medication and serotoninergic
system -> sleepDexter JD, 1986Culebras, 1996
Epilepsy
25% seizures predominantly in sleep: Juvenile myoclonic epilepsy, rolandic epilepsy, generalized tonic-clonic seizures on awakening, epilepsy with continuous spikes and wawes during SWS
Sleep deprivation lowers seizure threshold -> recurent seizures
Transitions to wakefulness, light non-REM sleep Non-REM facilitates <-> REM inhibits ictal
activity
Sleep fragmentation
Conclusions
GenerateBrain damage sleep
disordersAggravate
Neurologists have the knowledges to recognize and treat neurological (even
primary) sleep disorders