Embed Size (px)
Citation preview
Solutés de remplissage :
questions / réponses
Benoit TavernierPôle d'anesthésie réanimation
Hôpital Roger SalengroCHU de Lille
Conflits d'intérêt : Fresenius-Kabi, B-Braun, LFB, Masimo
“Colloids vs. crystalloids:
a long lasting controversy”
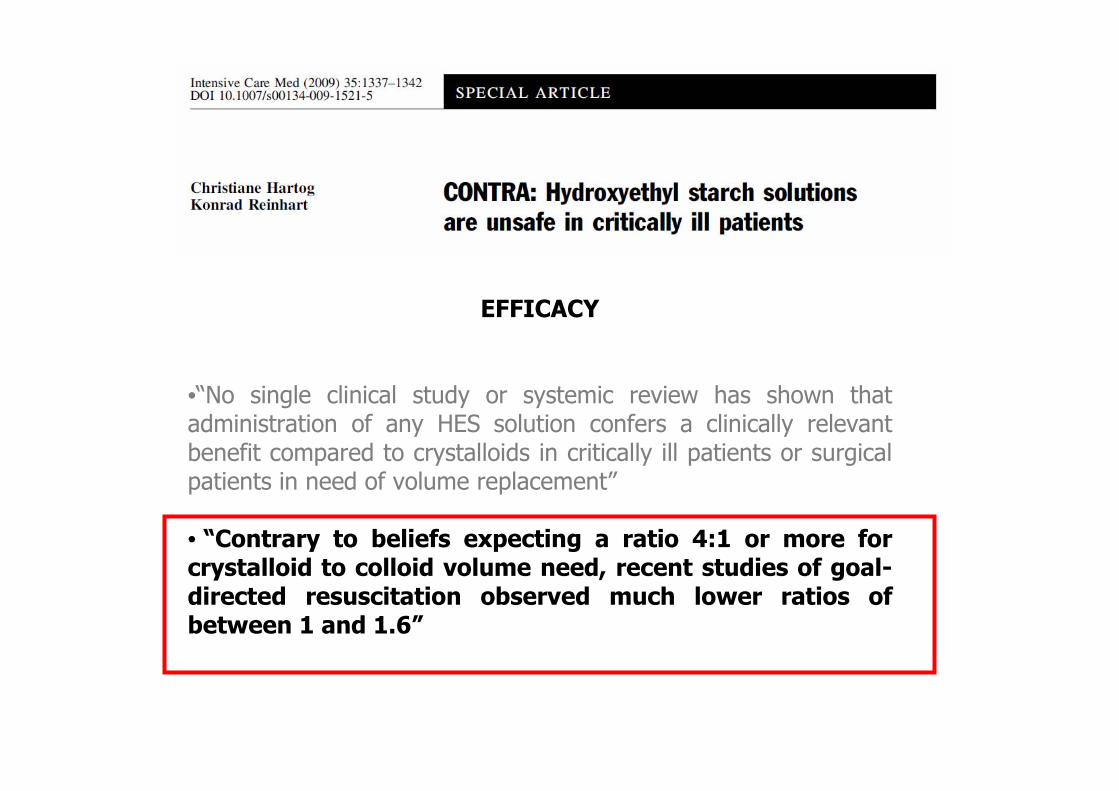
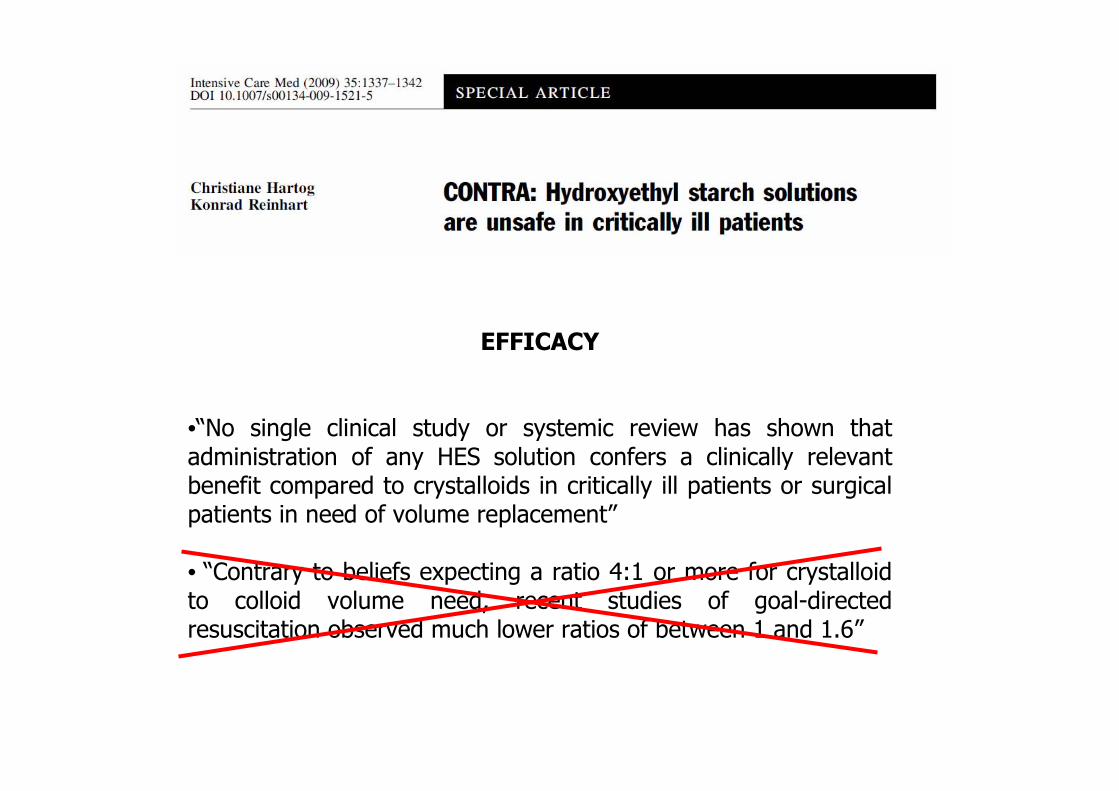
EFFICACY
•“No single clinical study or systemic review has shown that administration of any HES solution confers a clinically relevantbenefit compared to crystalloids in critically ill patients or surgical patients in need of volume replacement”
• “Contrary to beliefs expecting a ratio 4:1 or more for crystalloid to colloid volume need, recent studies of goal-directed resuscitation observed much lower ratios of between 1 and 1.6”
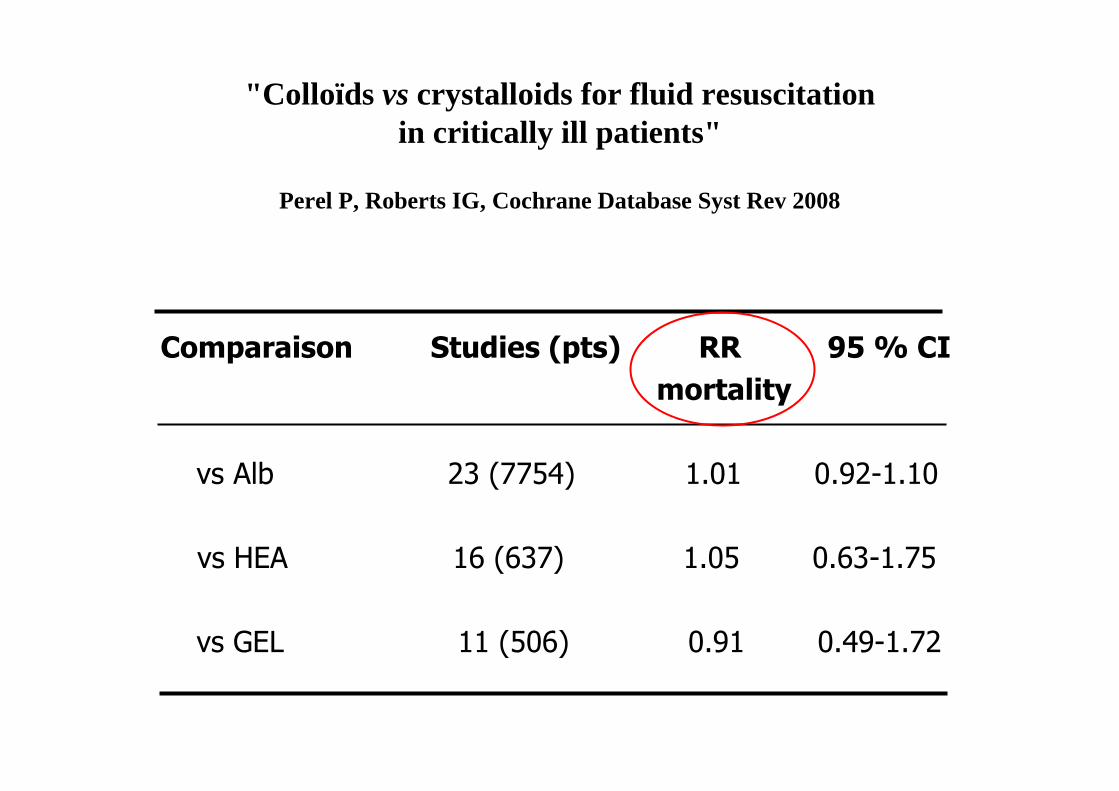
"Colloïds vs crystalloids for fluid resuscitationin critically ill patients"
Perel P, Roberts IG, Cochrane Database Syst Rev 2008
Comparaison Studies (pts) RR 95 % CI
mortality
vs Alb 23 (7754) 1.01 0.92-1.10
vs HEA 16 (637) 1.05 0.63-1.75
vs GEL 11 (506) 0.91 0.49-1.72
EFFICACY
•“No single clinical study or systemic review has shown that administration of any HES solution confers a clinically relevantbenefit compared to crystalloids in critically ill patients or surgical patients in need of volume replacement”
• “Contrary to beliefs expecting a ratio 4:1 or more for crystalloid to colloid volume need, recent studies of goal-directed resuscitation observed much lower ratios of between 1 and 1.6”

SAFETY
“HES administration is associated with dose-related side effects, suchas coagulopathy, nephrotoxicity, and protracted severe pruritus”
QUESTIONS
• Colloïdes vs cristalloïdes :aspects quantitatifs
• HEA : effets secondaires
• Solutions « balancées »
A - 4 / 1
B - 3 / 1
C - 2 / 1
D - 1 / 1
Efficacité hémodynamique :
le « ratio » cristalloïde / colloïde est
EFFICACY
•“No single clinical study or systemic review has shown that administration of any HES solution confers a clinically relevantbenefit compared to crystalloids in critically ill patients or surgical patients in need of volume replacement”
• “Contrary to beliefs expecting a ratio 4:1 or more for crystalloid to colloid volume need, recent studies of goal-directed resuscitation observed much lower ratios of between 1 and 1.6”

A - 4 / 1
B - 3 / 1
C - 2 / 1
D - 1 / 1
Efficacité hémodynamique :
le « ratio » cristalloïde / colloïde théoriqueest
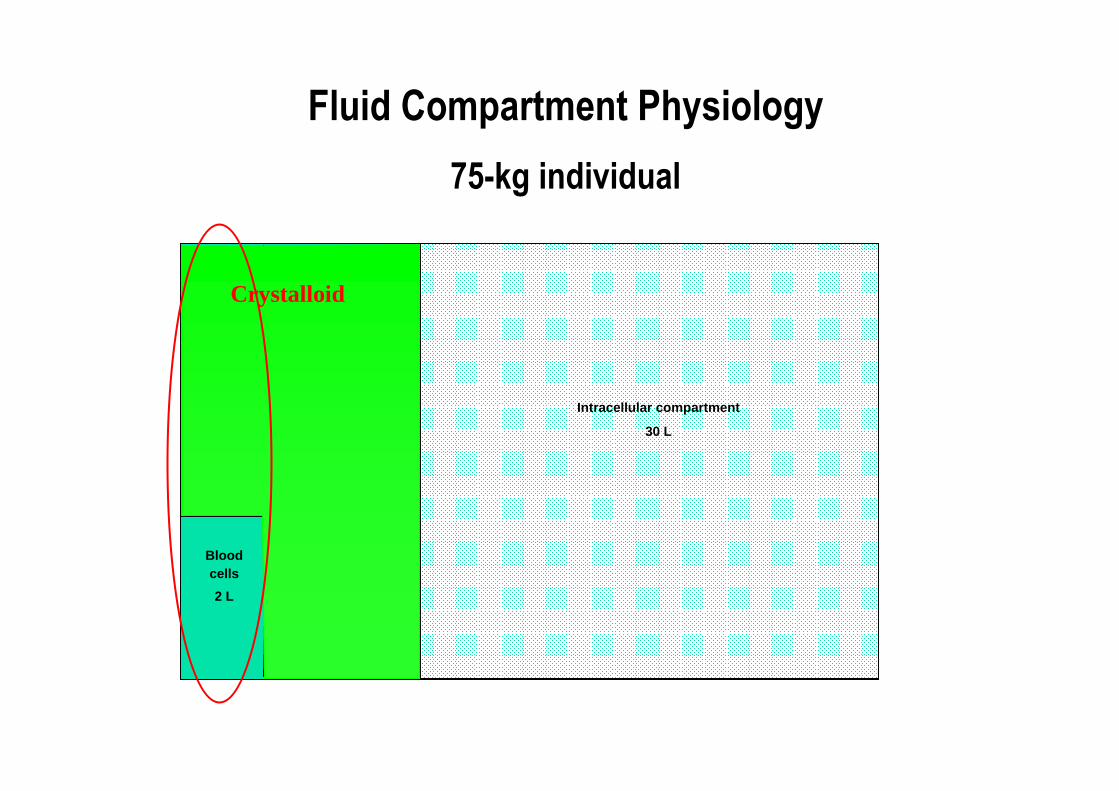
Fluid Compartment Physiology
75-kg individual
Intracellular compartment
30 L
Interstitial
compartment
10 L
Bloodcells
2 L
Plasma
3 L
Crystalloid
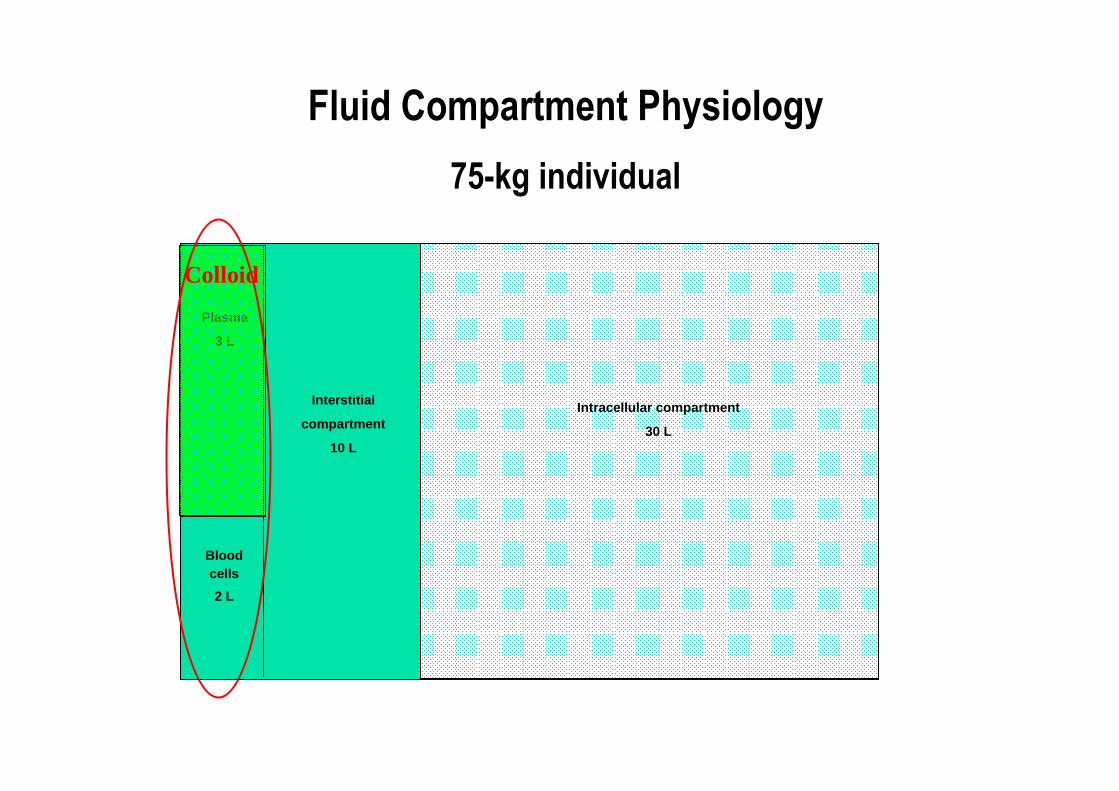
Fluid Compartment Physiology
75-kg individual
Intracellular compartment
30 L
Interstitial
compartment
10 L
Bloodcells
2 L
Plasma
3 L
Colloid
A - 4 / 1
B - 3 / 1
C - 2 / 1
D - 1 / 1
Efficacité hémodynamique :
le « ratio » cristalloïde / colloïde expérimental est
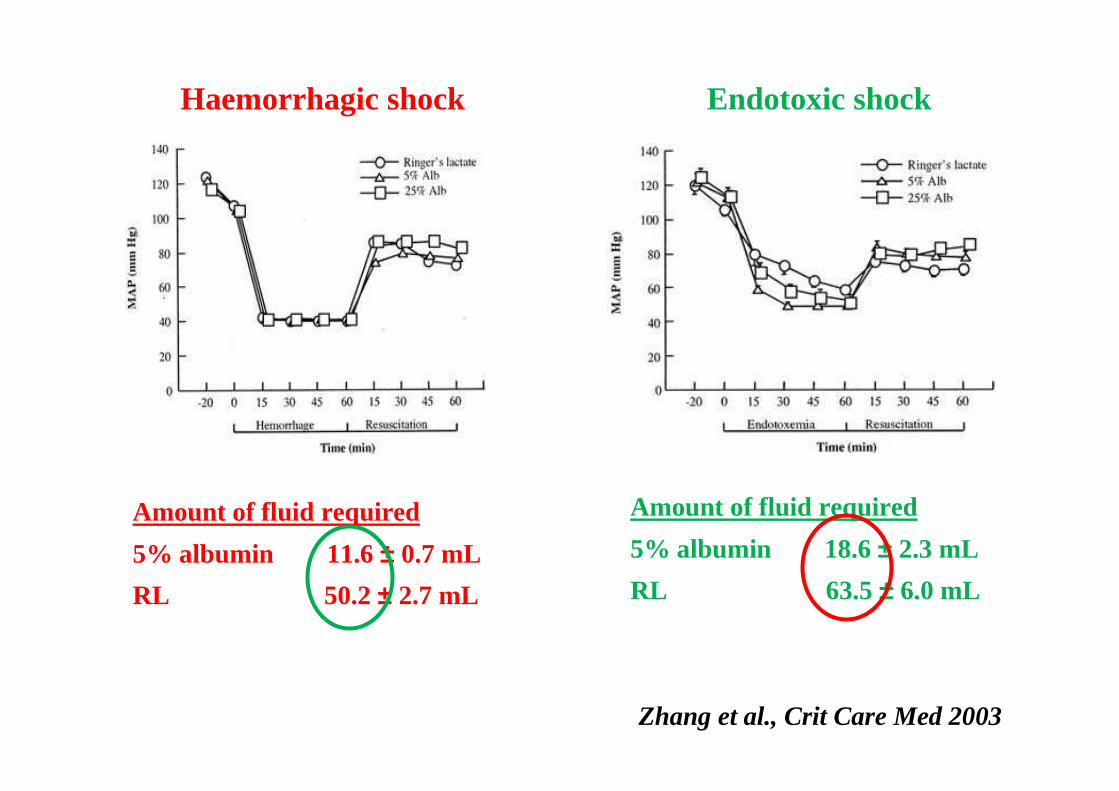
Amount of fluid required
5% albumin 11.6 ± 0.7 mL
RL 50.2 ± 2.7 mL
Haemorrhagic shock
Amount of fluid required
5% albumin 18.6 ± 2.3 mL
RL 63.5 ± 6.0 mL
Endotoxic shock
Zhang et al., Crit Care Med 2003
A - 4 / 1
B - 3 / 1
C - 2 / 1
D - 1 / 1
Efficacité hémodynamique :
le « ratio » cristalloïde / colloïde
en clinique est
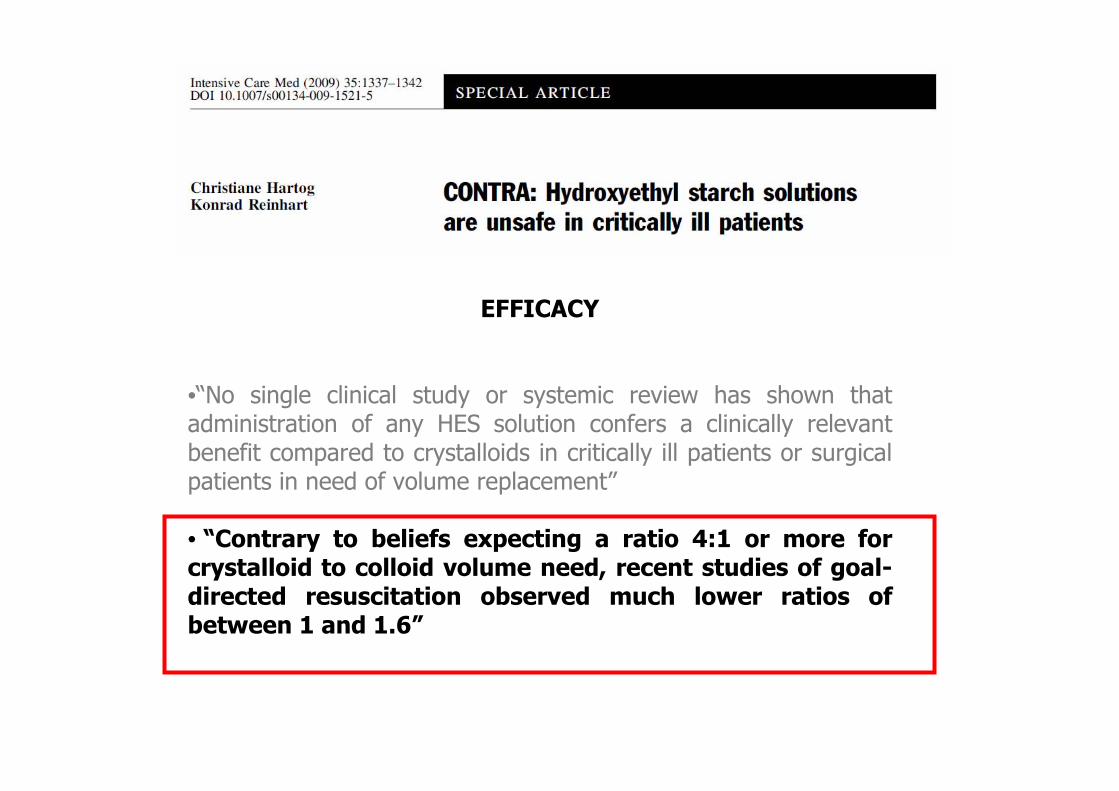
EFFICACY
•“No single clinical study or systemic review has shown that administration of any HES solution confers a clinically relevantbenefit compared to crystalloids in critically ill patients or surgical patients in need of volume replacement”
• “Contrary to beliefs expecting a ratio 4:1 or more for crystalloid to colloid volume need, recent studies of goal-directed resuscitation observed much lower ratios of between 1 and 1.6”
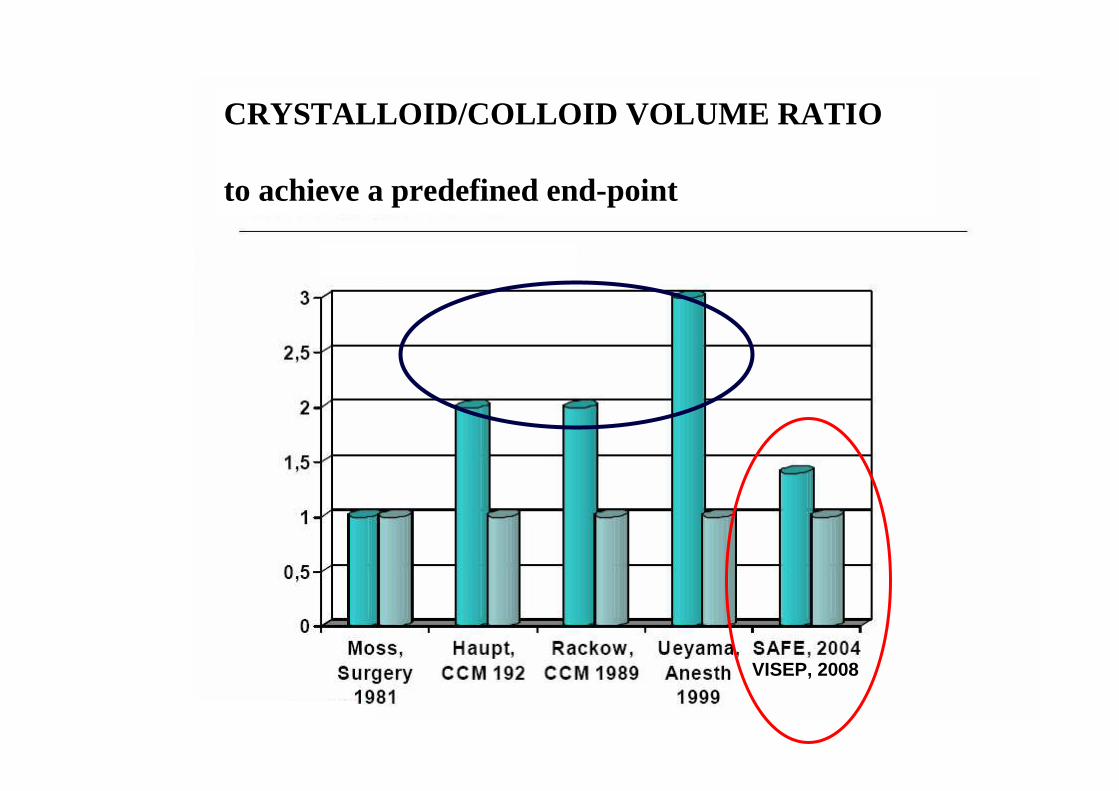
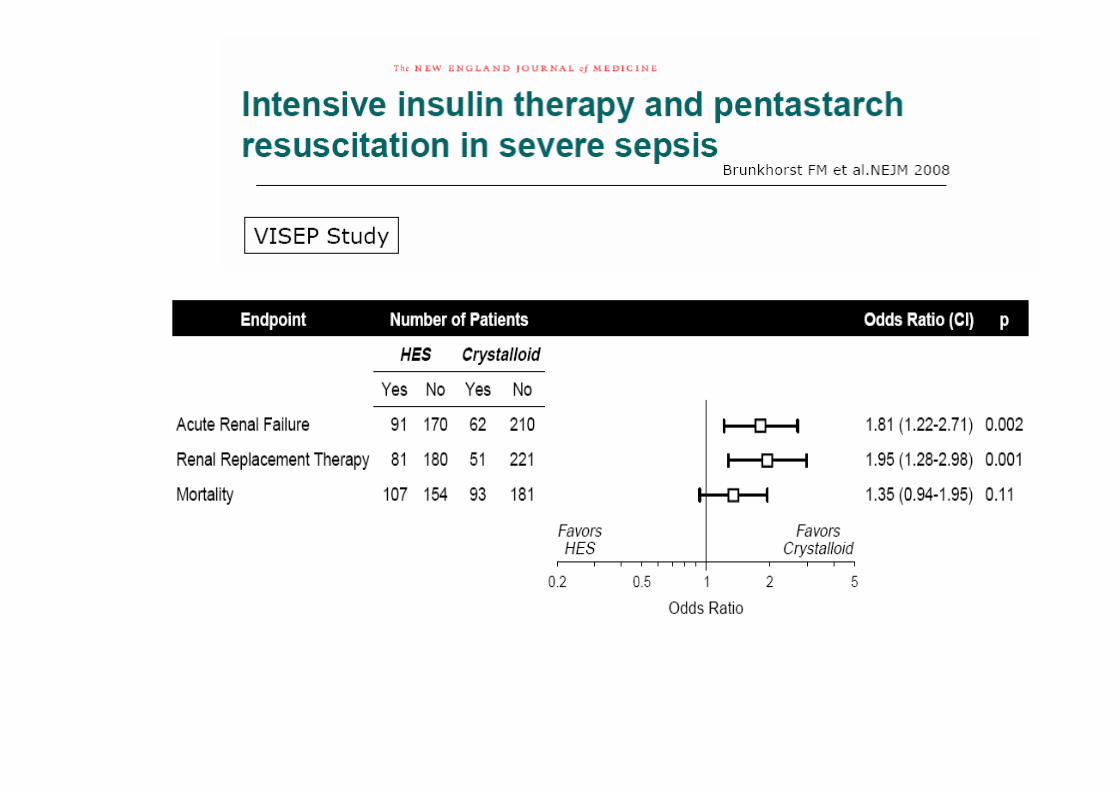
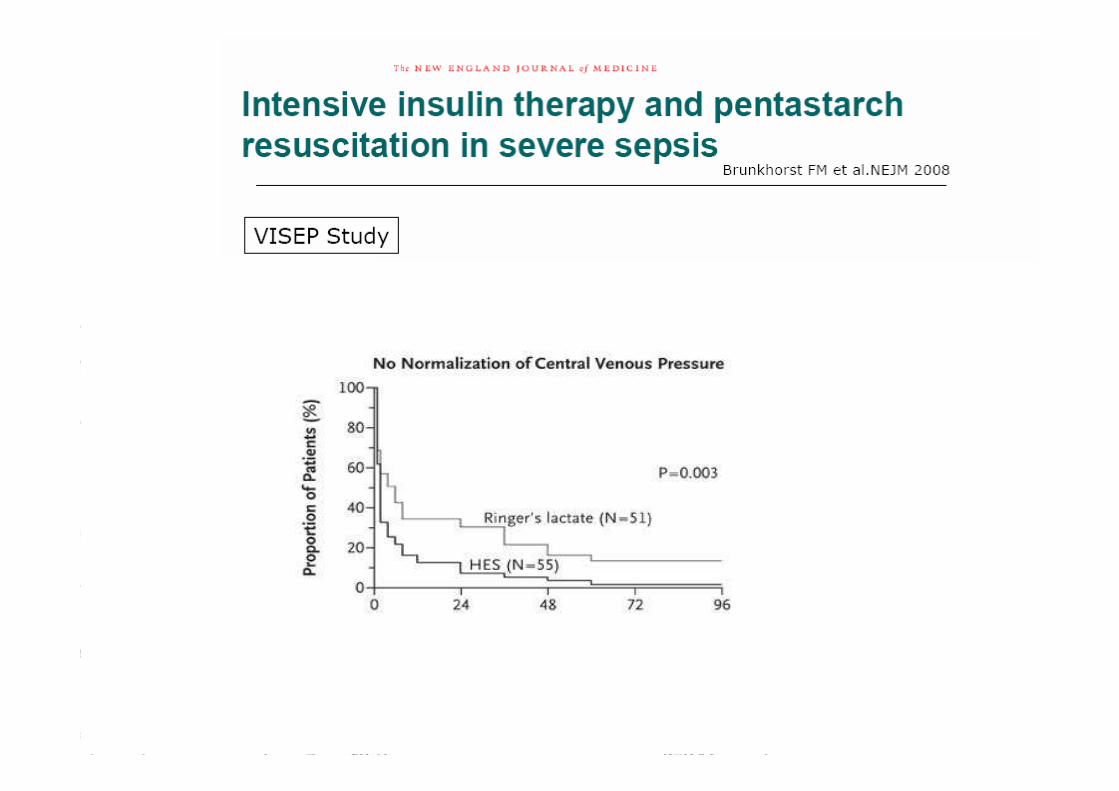
VISEP, 2008
CRYSTALLOID/COLLOID VOLUME RATIO
to achieve a predefined end-point



Soluté de remplissage vasculaire
• Pouvoir d'expansion volémique "instantané"
• Persistance de l'effet
• Critère d'efficacité ("end-point") :
pertinence et « satisfaction »
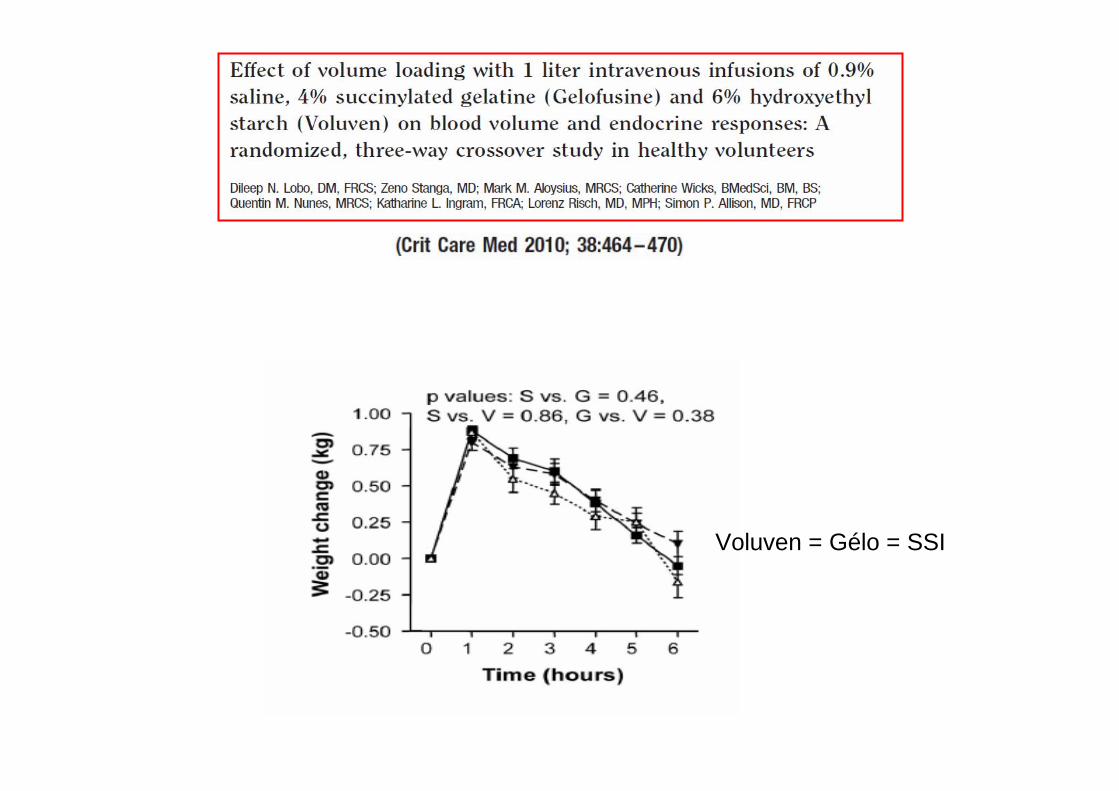
Voluven = Gélo = SSI

SSI
SSICOLLOIDE
COLLOIDE
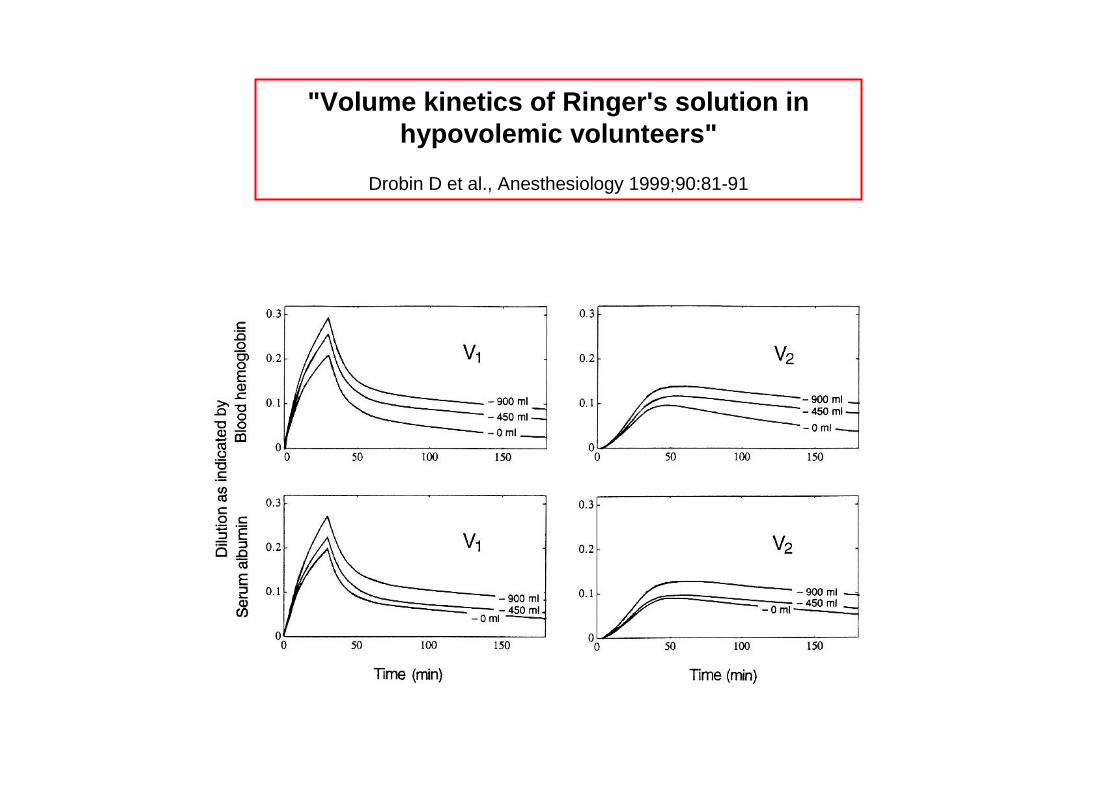
"Volume kinetics of Ringer's solution in hypovolemic volunteers"
Drobin D et al., Anesthesiology 1999;90:81-91

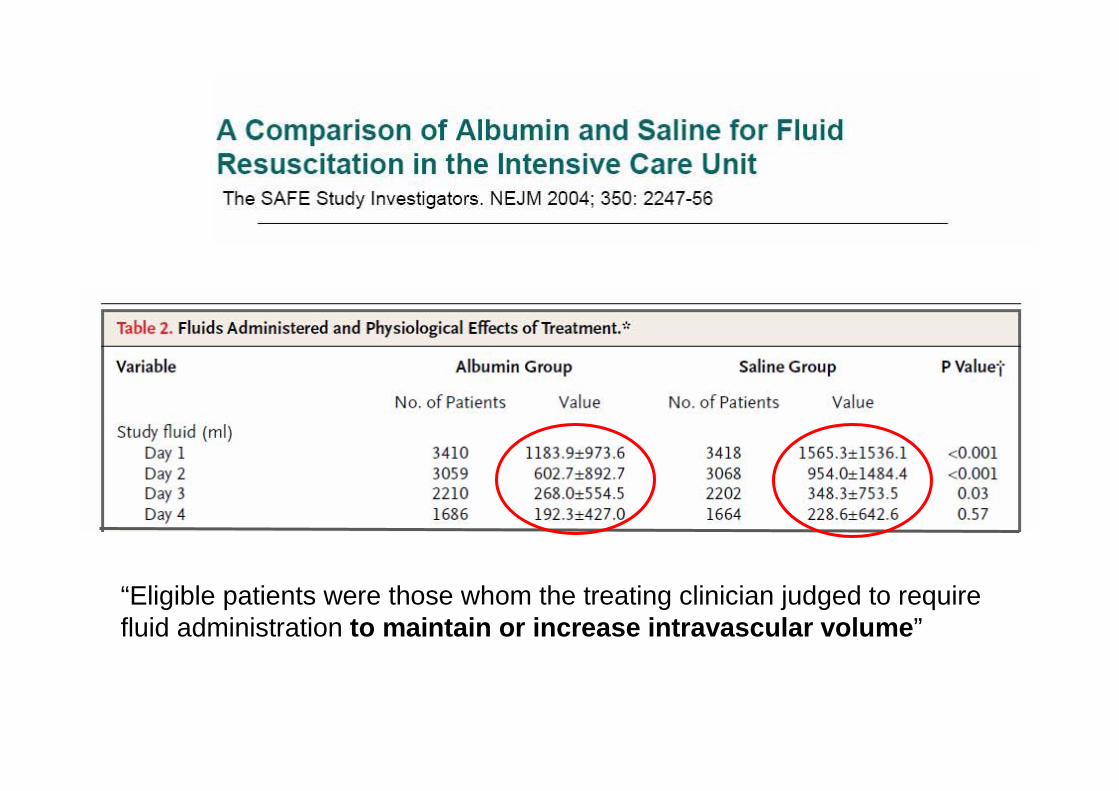
“Eligible patients were those whom the treating clinician judged to require fluid administration to maintain or increase intravascular volume ”
HEAfusine 10%
• 537 patients (severe sepsis / septic shock)
• Ringer lactate vs HES 200/0.5 10%
• Goal: CVP ≥ 8 mm Hg, MAP ≥ 70 mm Hg, ScvO2 ≥ 70 %

HEAfusine 10%
• 537 patients (sepsis sévère / choc septique)
• Ringer lactate vs HEAfusine 10%
• Objectif PVC ≥ 8 mm Hg, PAM ≥ 70 mmHg, ScvO2 ≥ 70 %
• Ratio RL / HEA = 1,3 pour volume total HEA (médian) : 70 ml/kg
OUI, mais ….
• J1 : ratio RL / HEA = 1,6
•H-12 à H0 : 2000 (1000-3500) ml de RL + 850 (500-1000) ml d'HEA
• H0 : objectif hémodynamique (PVC) déjà atteint chez 80% des pts dans les deux groupes
HEAfusine 10%
EFFICACY
•“No single clinical study or systemic review has shown that administration of any HES solution confers a clinically relevantbenefit compared to crystalloids in critically ill patients or surgical patients in need of volume replacement”
• “Contrary to beliefs expecting a ratio 4:1 or more for crystalloid to colloid volume need, recent studies of goal-directed resuscitation observed much lower ratios of between 1 and 1.6”
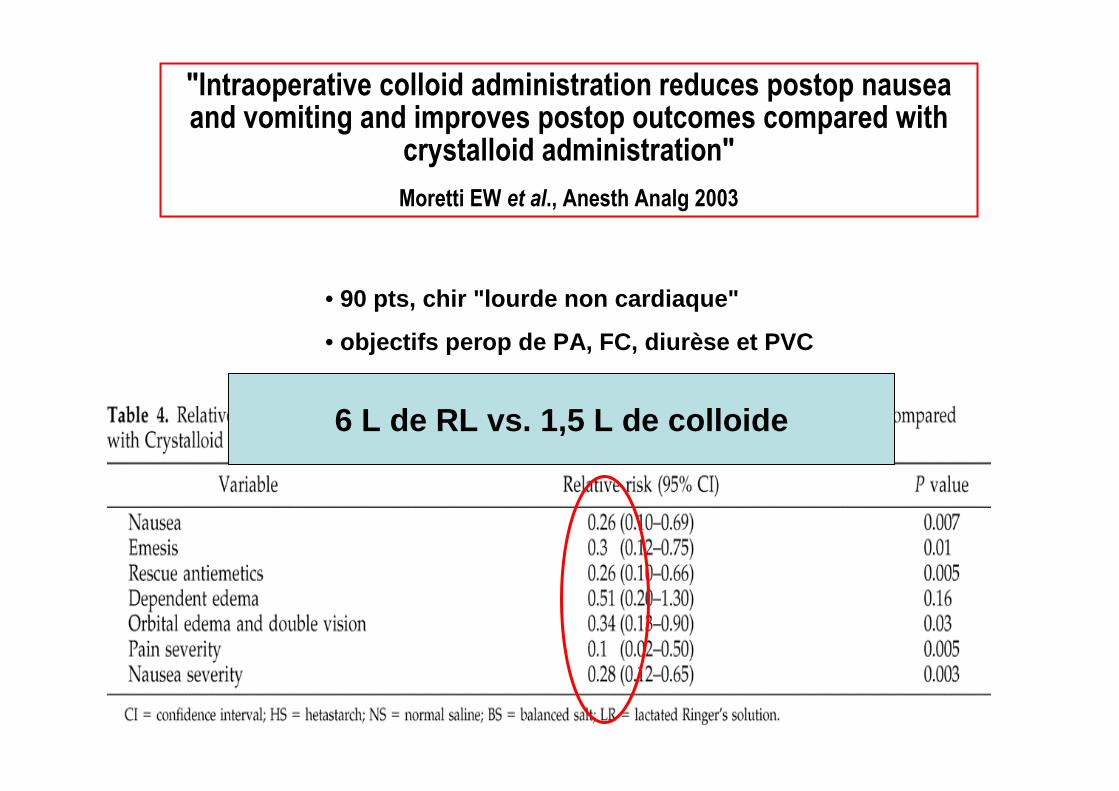
"Intraoperative colloid administration reduces postop nausea and vomiting and improves postop outcomes compared with
crystalloid administration"
Moretti EW et al., Anesth Analg 2003
• 90 pts, chir "lourde non cardiaque"
• objectifs perop de PA, FC, diurèse et PVC
6 L de RL vs. 1,5 L de colloide

Synthèse
• RV : d'abord les cristalloïdes ("evidence-based"; tous consensus et recommandations)
• Limites– Délai d'obtention des objectifs hémodynamiques– Durée d'obtention de ces objectifs
• Colloïdes= objectifs atteints plus vite et maintenus avec moindre (2 à 3 x
moins) volume

Cas cliniqueCas clinique
Mme M, 73 ans, est opMme M, 73 ans, est opéérréée de d’’une perforation diastatique du caecum. une perforation diastatique du caecum.
LL’’intervention rintervention rééalisaliséée sous AG a dure sous AG a duréé 6 heures.6 heures.
En prEn préé-- et peropet peropéératoire, la patiente a reratoire, la patiente a reççu 3500 ml de SSI, 1000 ml de u 3500 ml de SSI, 1000 ml de
collocolloïïde (dans SSI) et 2 CGUA.de (dans SSI) et 2 CGUA.
A la sortie du BO, lA la sortie du BO, l’’hhéémodynamique est stable, la patiente est encore modynamique est stable, la patiente est encore
sous VC.sous VC.
Bio: pH 7,22, PaCOBio: pH 7,22, PaCO22 37 mmHg, HCO37 mmHg, HCO33 17 mmol/l, BE 17 mmol/l, BE --9 mmol/l, ur9 mmol/l, uréée e
0,45 g/l, cr0,45 g/l, crééat 8 mg/l, Naat 8 mg/l, Na++ 139 mmol/l, K139 mmol/l, K+ + 4,5 mmol/l, Ca4,5 mmol/l, Ca2+2+ 1,1 mmol/l, 1,1 mmol/l,
MgMg2+2+ 0,5 mmol/l, Cl0,5 mmol/l, Cl-- 108 mmol/l, phosphore 1,4 mmol/l 108 mmol/l, phosphore 1,4 mmol/l
«« …… encore une acidose par remplissage au SSI encore une acidose par remplissage au SSI …….. »»
A - SSI
B - Ringer
C - Gélofusine
D - Voluven
E - S Glu 5%
F - Polyionique
Sont susceptibles d’entraîner une acidose hyperchlorémique :

pH = pK1’ + logSID – Atot / (1 + 10pKa - pH)
S . PCO2
Constable PD, Anesth Analg 2003
SID = « Strong Ions Difference » [Acides faibles non volatils] : Alb-, Pi-
SID
Mécanisme : équations de Stewart

SID = [ Na+, K+, Ca2+, Mg2+] – [Cl -, lact, SO 42-, CC]
[Cl-]
et
[Na+]
et
[Autres cations forts] [Autres anions forts]
SID= 40 mEq/L
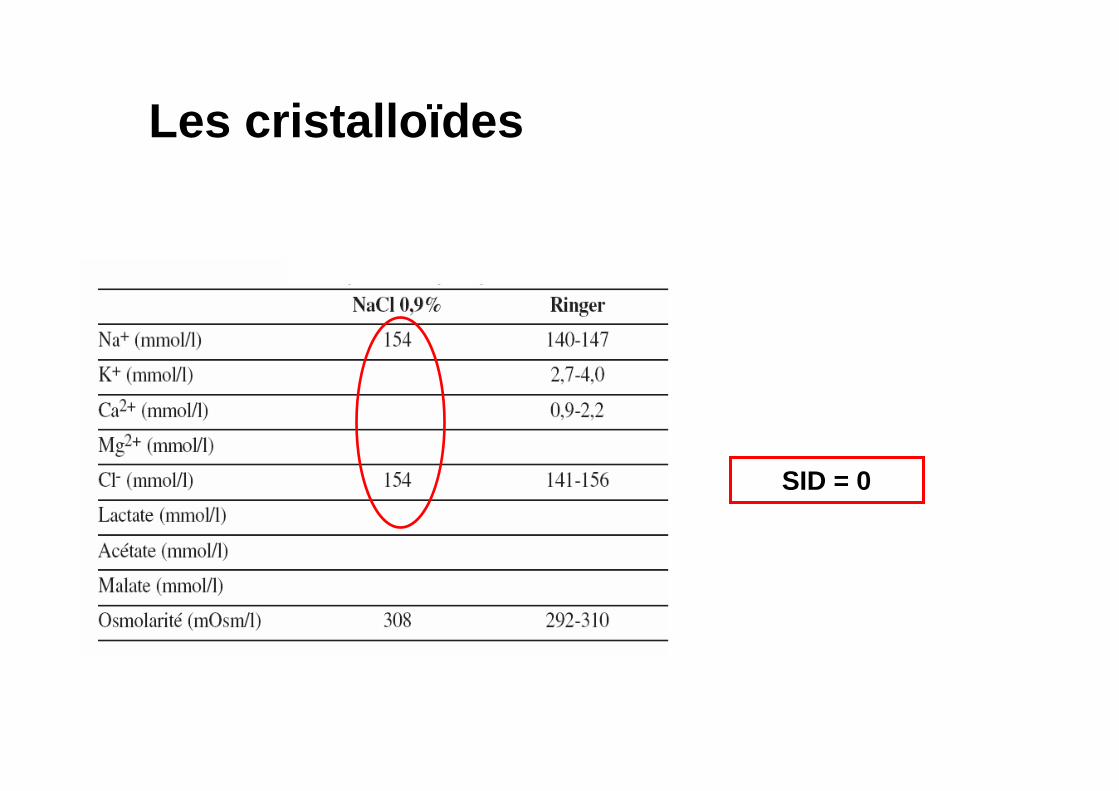
Les cristalloïdes
SID = 0

pH = pK1’ + logSID – Atot / (1 + 10pKa - pH)
S . PCO2
Constable PD, Anesth Analg 2003
SID = [ Na+, K+,…] – [Cl-, Lact-,…] [ Alb-, Pi- ]*
SID
Hyperchlorémie � ↓ SID � Acidose
Hypoalbuminémie � ↓ Atot � Alcalose
Mécanisme : équations de Stewart
Valeur "idéale" du SID d'un soluté ≈ 24-26 meq/l
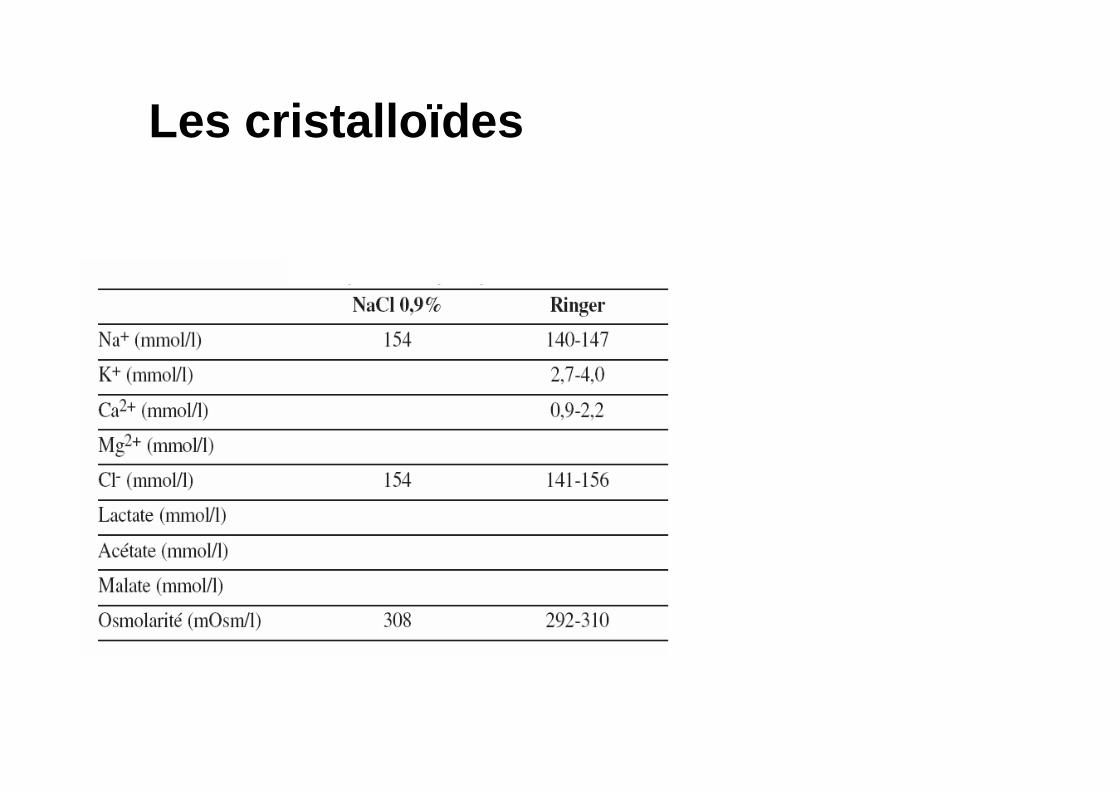
Les cristalloïdes
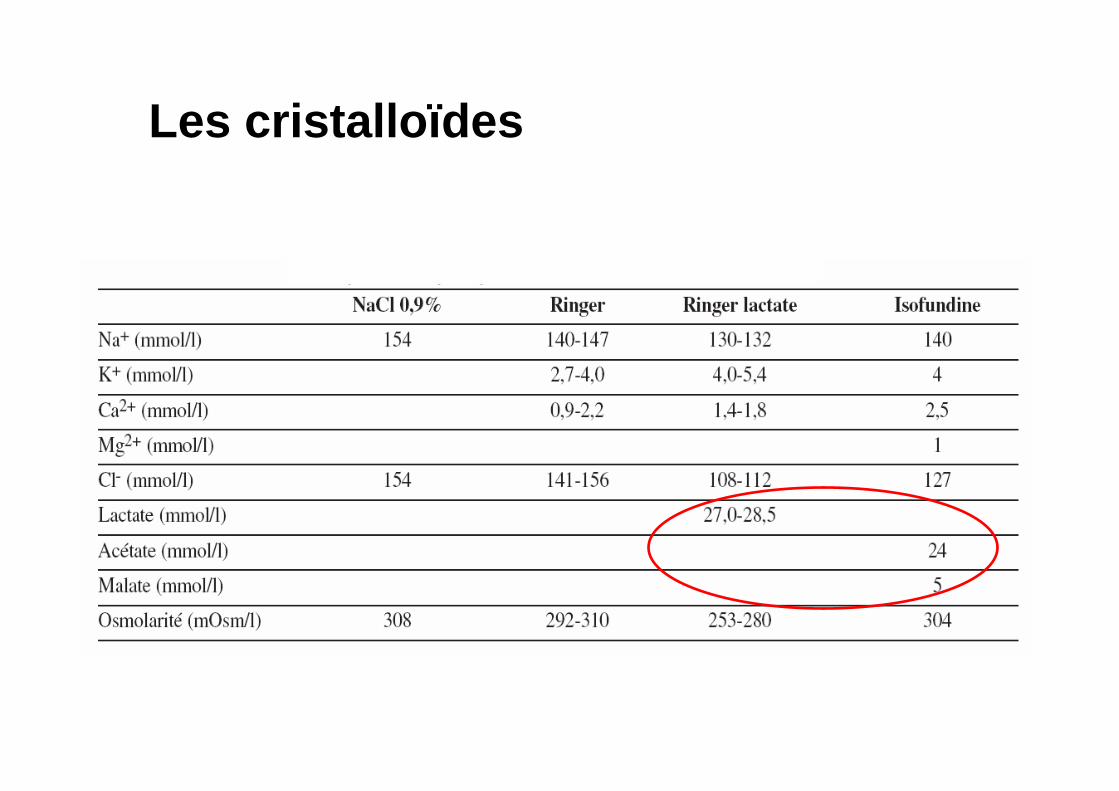
Les cristalloïdes
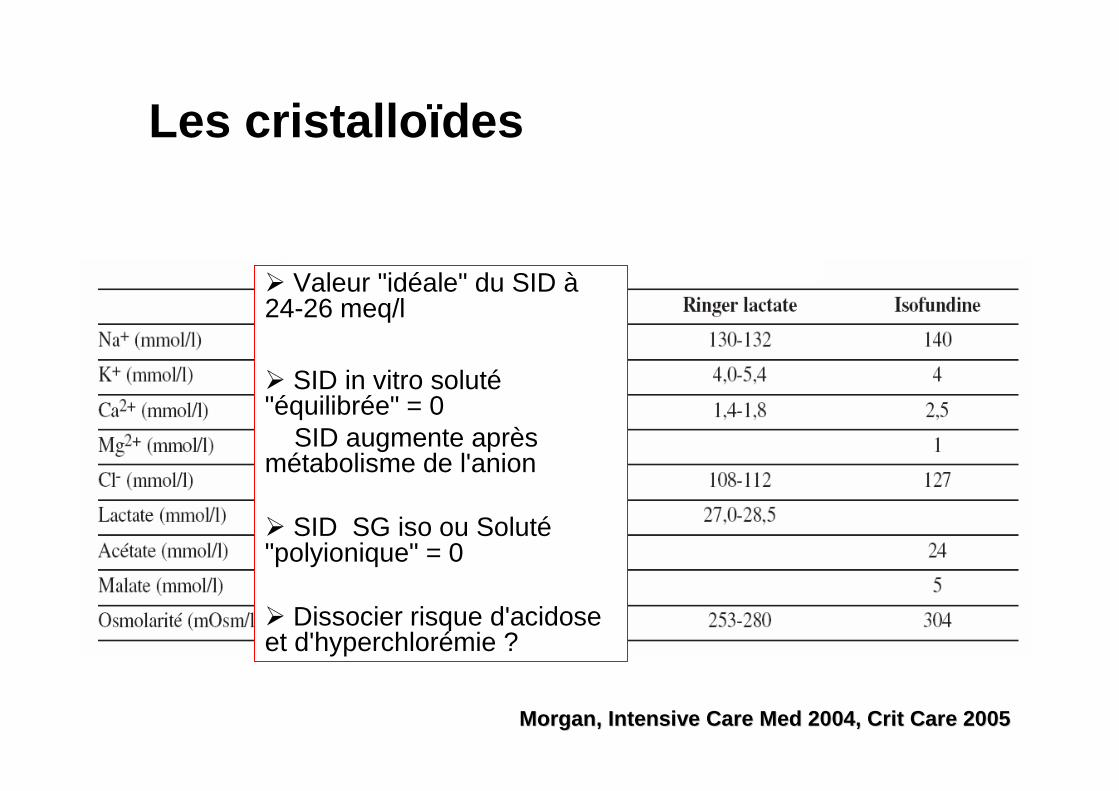
Les cristalloïdes
� Valeur "idéale" du SID à24-26 meq/l
� SID in vitro soluté"équilibrée" = 0
SID augmente après métabolisme de l'anion
� SID SG iso ou Soluté"polyionique" = 0
� Dissocier risque d'acidose et d'hyperchlorémie ?
Morgan, Intensive Care Med 2004, Crit Care 2005Morgan, Intensive Care Med 2004, Crit Care 2005
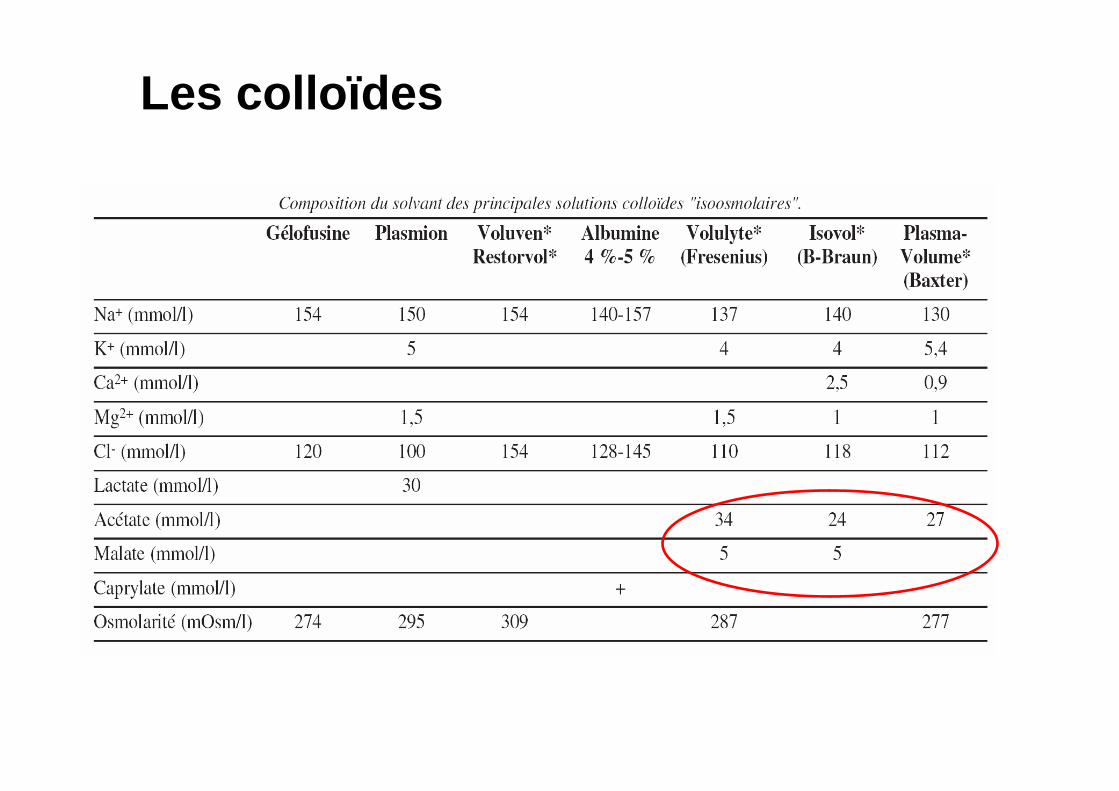
Les colloïdes
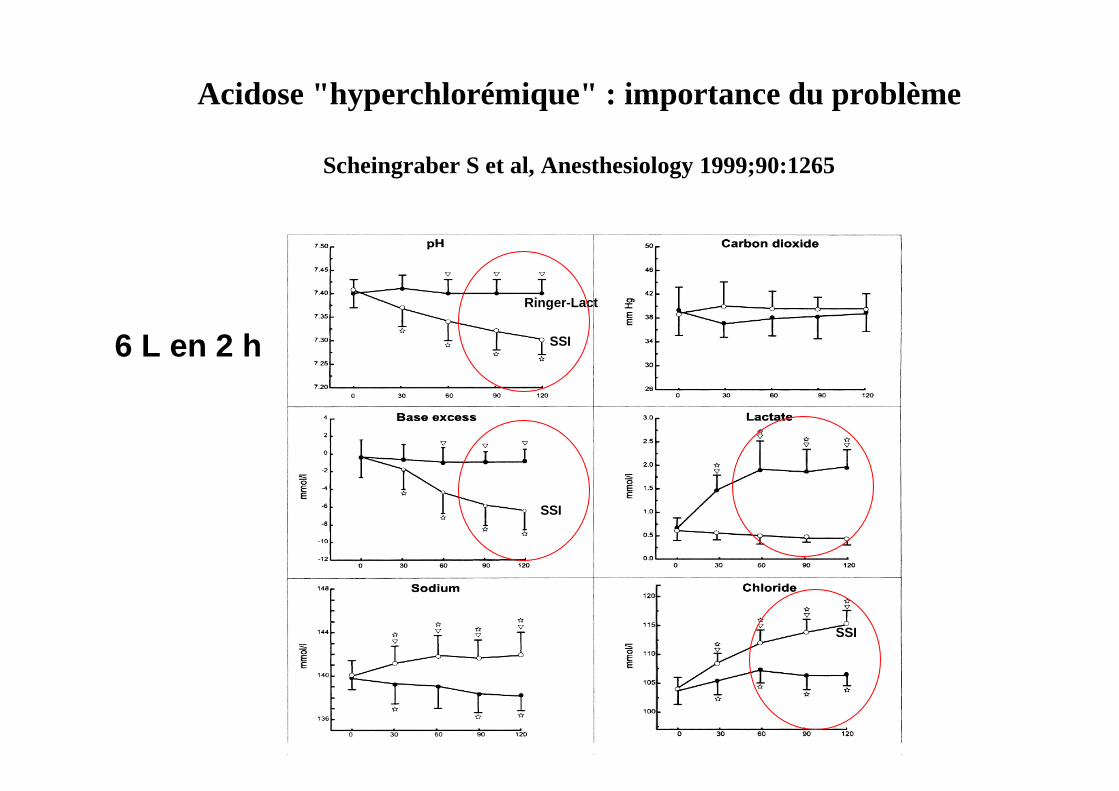
Acidose "hyperchlorémique" : importance du problème
Scheingraber S et al, Anesthesiology 1999;90:1265
Ringer-Lact
SSI6 L en 2 h
SSI
SSI

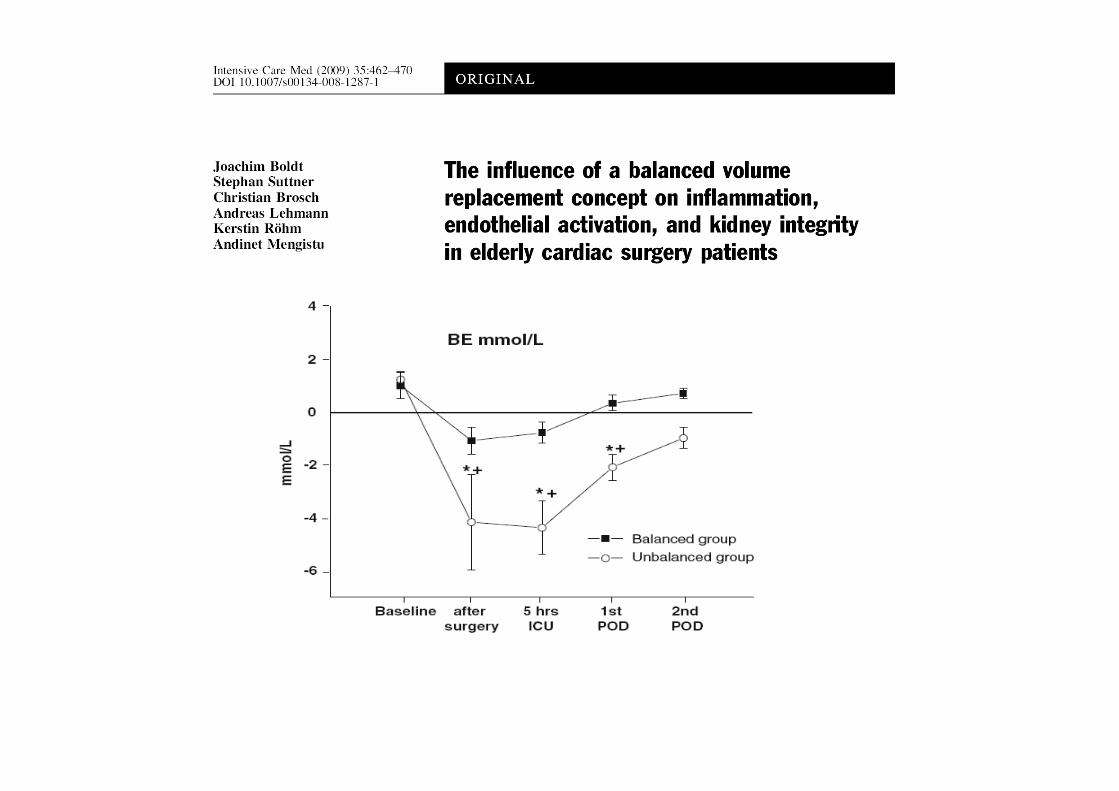
"balancé" (crist + coll)
vs.
"non balancé" (crist + coll)
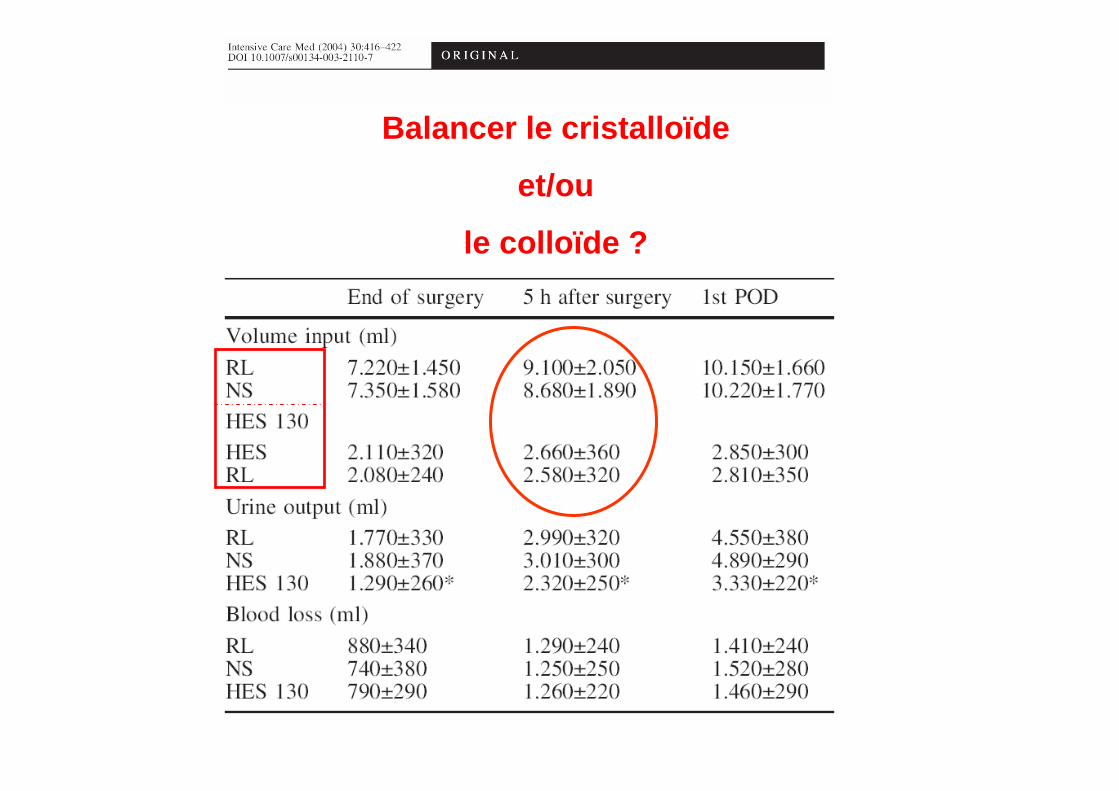
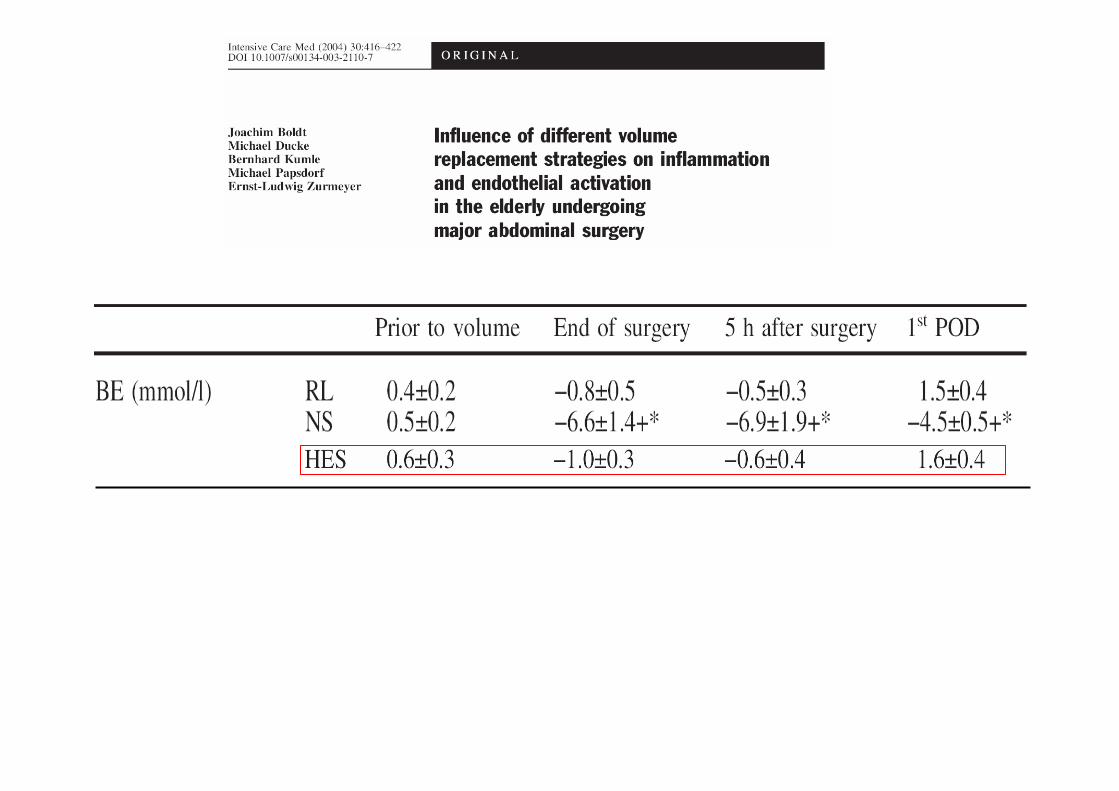
Balancer le cristalloïde
et/ou
le colloïde ?
Acidose "hyperchlorémique" : importance du problème
• BE diminue de 0,06 à 0,07 mmol/L par ml de SSI/kg de poids administré
• Adulte
• 2 L (30 ml/kg) SSI : BE : - 2 mmol/L
• 4 L (60 ml/kg) SSI : BE : - 4 mmol/L
• 6 L (90 ml/kg) SSI : BE : - 6 mmol/L
• A moduler selon vitesse d'administration et fonction rénale
• Problème si acidose pre-existante ou associée, si fonction rénale altérée ?
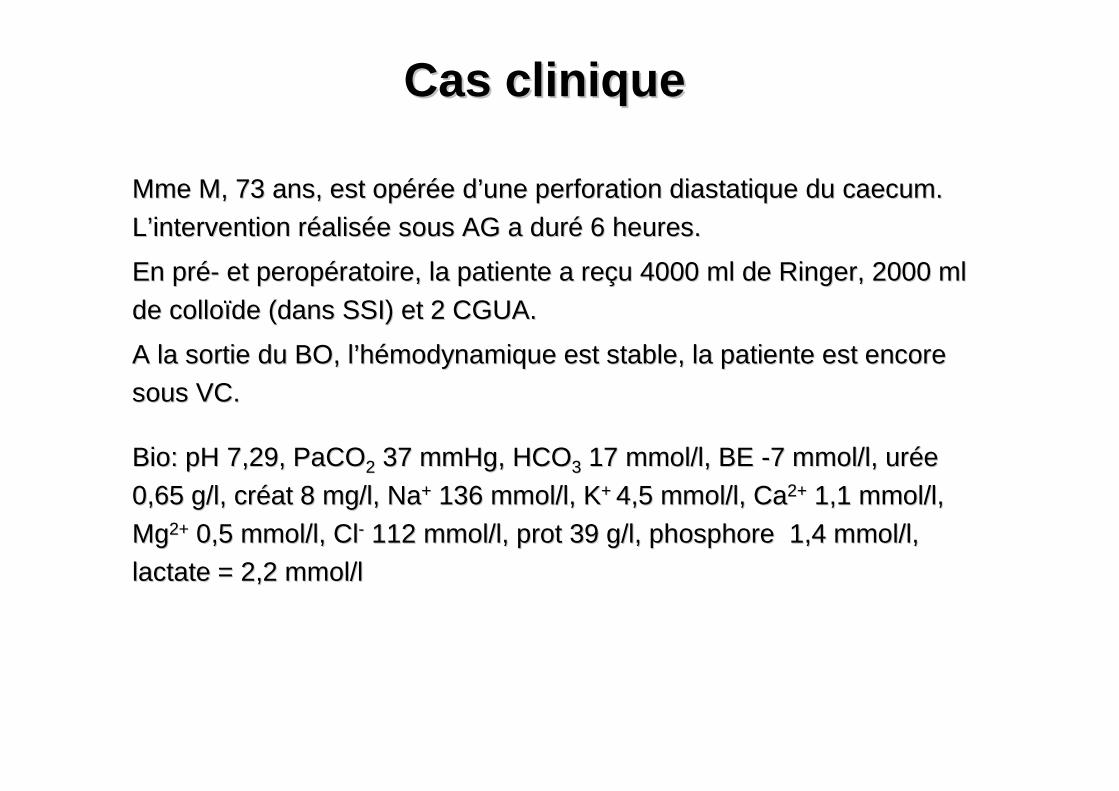
Cas cliniqueCas clinique
Mme M, 73 ans, est opMme M, 73 ans, est opéérréée de d’’une perforation diastatique du caecum. une perforation diastatique du caecum.
LL’’intervention rintervention rééalisaliséée sous AG a dure sous AG a duréé 6 heures.6 heures.
En prEn préé-- et peropet peropéératoire, la patiente a reratoire, la patiente a reççu 4000 ml de Ringer, 2000 ml u 4000 ml de Ringer, 2000 ml
de collode colloïïde (dans SSI) et 2 CGUA.de (dans SSI) et 2 CGUA.
A la sortie du BO, lA la sortie du BO, l’’hhéémodynamique est stable, la patiente est encore modynamique est stable, la patiente est encore
sous VC.sous VC.
Bio: pH 7,29, PaCOBio: pH 7,29, PaCO22 37 mmHg, HCO37 mmHg, HCO33 17 mmol/l, BE 17 mmol/l, BE --7 mmol/l, ur7 mmol/l, uréée e
0,65 g/l, cr0,65 g/l, crééat 8 mg/l, Naat 8 mg/l, Na++ 136 mmol/l, K136 mmol/l, K+ + 4,5 mmol/l, Ca4,5 mmol/l, Ca2+2+ 1,1 mmol/l, 1,1 mmol/l,
MgMg2+2+ 0,5 mmol/l, Cl0,5 mmol/l, Cl-- 112 mmol/l, prot 39 g/l, phosphore 1,4 mmol/l, 112 mmol/l, prot 39 g/l, phosphore 1,4 mmol/l,
lactate = 2,2 mmol/l lactate = 2,2 mmol/l
L’acidose hyperchlorémique du remplissage vasculaire
SSI, Ringer, colloïdes
=
Solutions
non physiologiques
Solutions "équilibrées"
=
"plasma-adapted"
balanced solutions

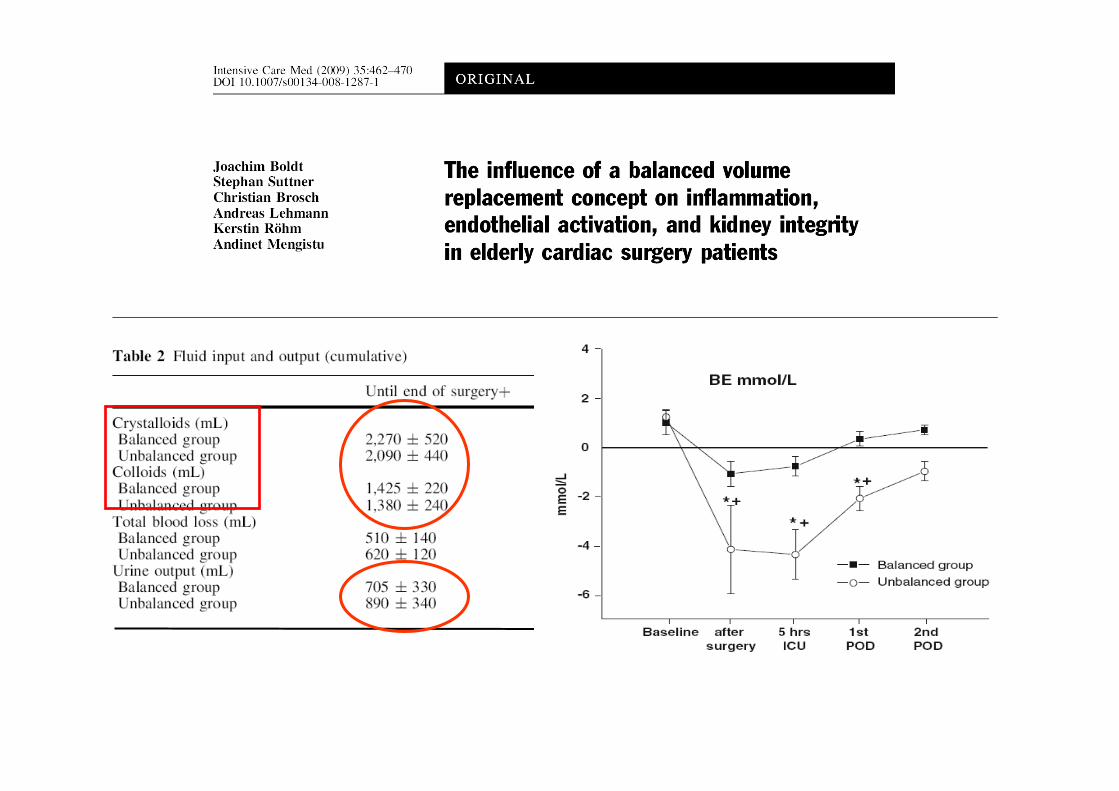
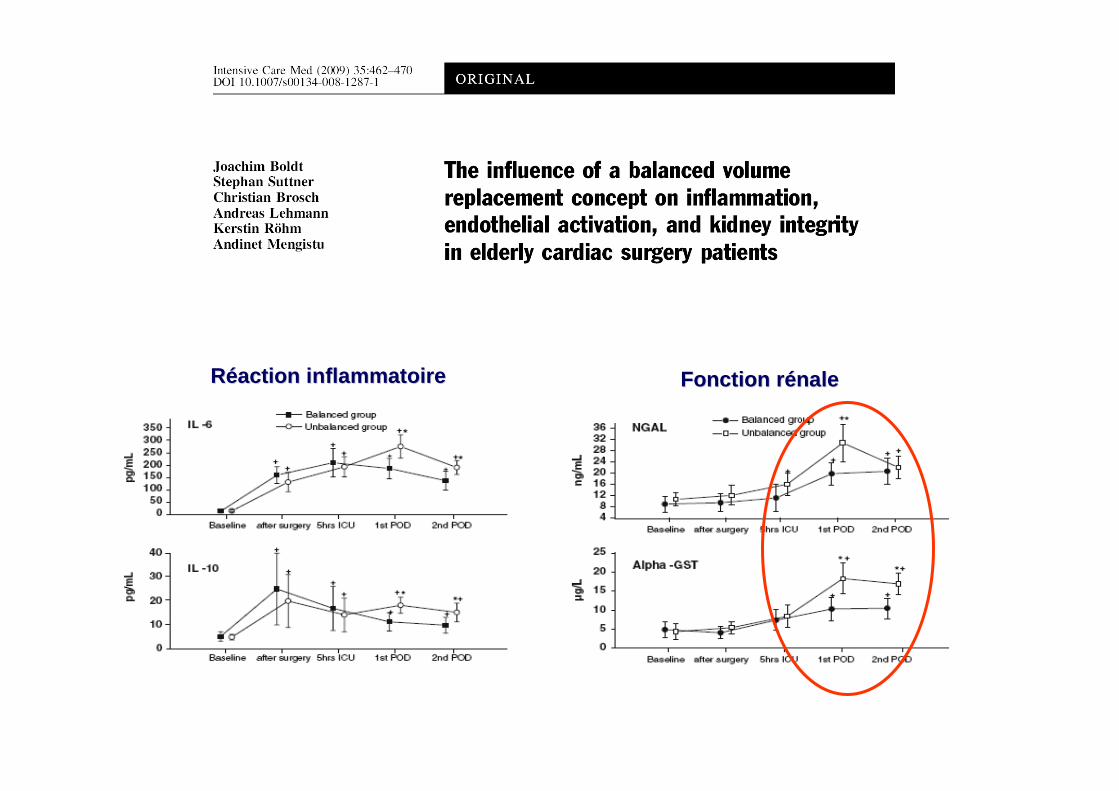
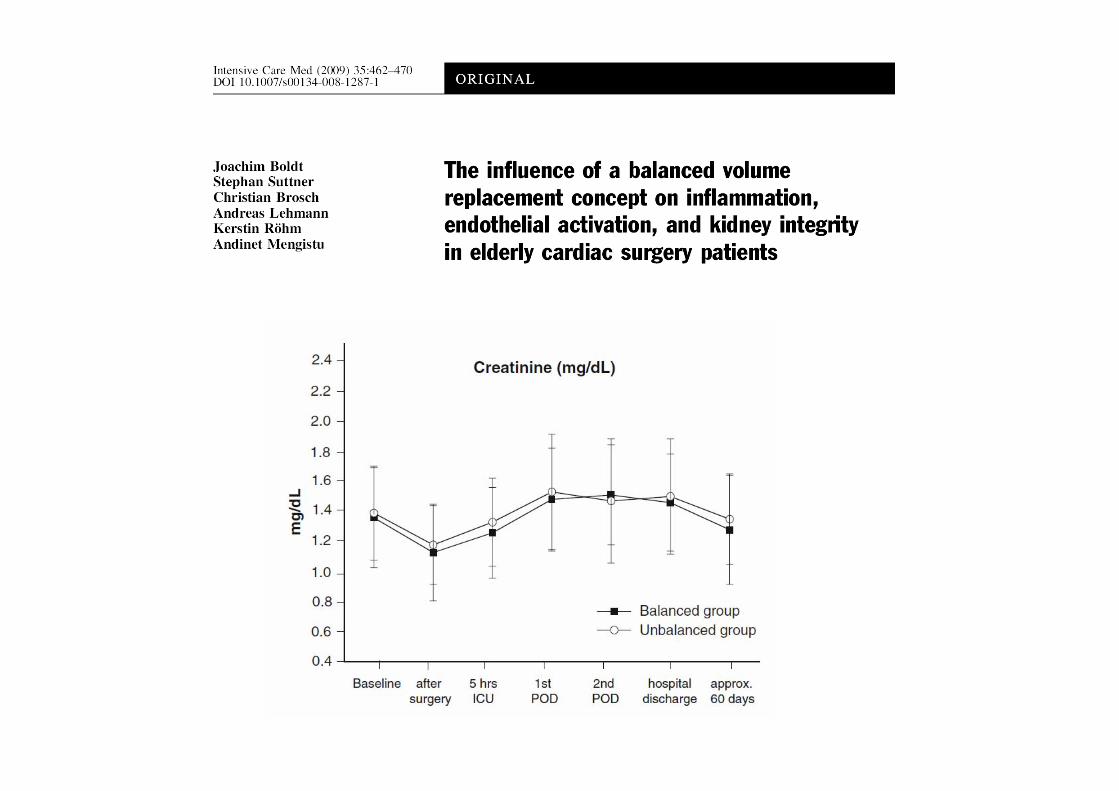
RRééaction inflammatoireaction inflammatoire Fonction rFonction r éénalenale

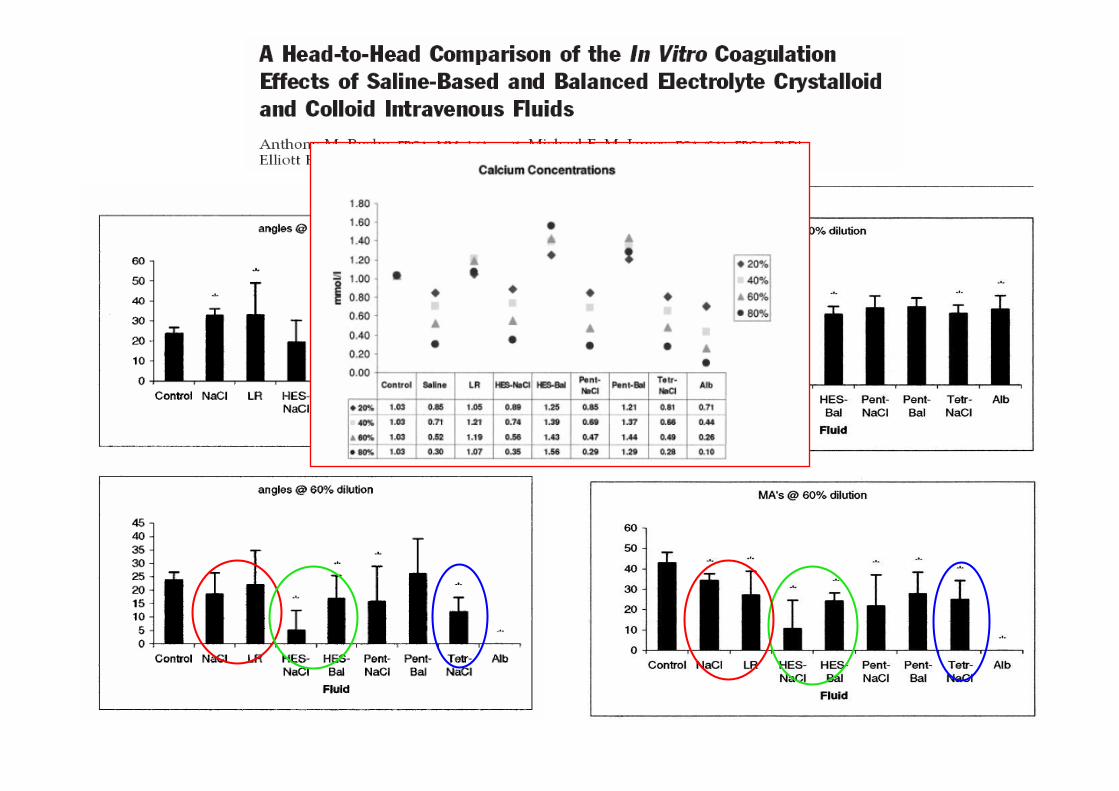
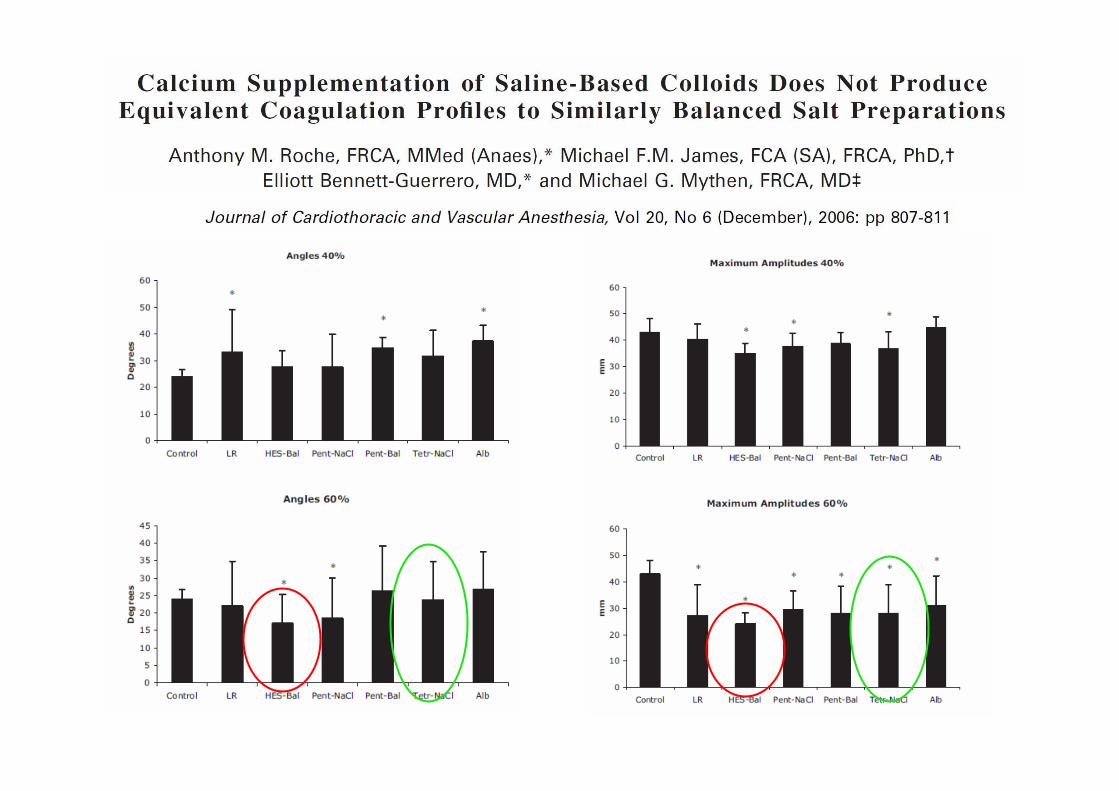
Etudes in vitro
• Différences peu marquées et inconstantes (sauf HEA haut PM)
• Dilutions importantes
• Rôle démontré du Ca2+
Les solutions "équilibrées"
• Quand ?– volumes importants, fonction rénale altérée, acidose et/ou
hyperchlorémie préexistante– intérêt des colloïdes pour diminuer les volumes, donc le
risque d'acidose– en 1ere … ou 2eme intention
• Cristalloïdes : Ringer Lactate ou Ringer Acetate ?– osmolalité– lactate vs. acétate– chlorémie
• Colloïdes : utilité ?
CONCLUSION
• Acidose hyperchlorémique avec solutions non "balancées" : avéré…et pas nouveau
• Volumes "limités" : aucun problème
• Surtout les cristalloïdes
• Seuil et conséquences cliniques ?
• Bénéfice solutions balancées sur pronostic reste àdémontrer
Cas cliniqueCas clinique
Mme M, 73 ans, est opMme M, 73 ans, est opéérréée de d’’une perforation diastatique du caecum. une perforation diastatique du caecum.
LL’’intervention rintervention rééalisaliséée sous AG a dure sous AG a duréé 6 heures.6 heures.
En prEn préé-- et peropet peropéératoire, la patiente a reratoire, la patiente a reççu 5000 ml de Ringer, 2000 ml u 5000 ml de Ringer, 2000 ml
de collode colloïïde (dans SSI) et 2 CGUA.de (dans SSI) et 2 CGUA.
A la sortie du BO, lA la sortie du BO, l’’hhéémodynamique est stable, la patiente est encore modynamique est stable, la patiente est encore
sous VC.sous VC.
Bio: pH 7,28, PaCOBio: pH 7,28, PaCO22 37 mmHg, HCO37 mmHg, HCO33 17 mmol/l, BE 17 mmol/l, BE --8 mmol/l, ur8 mmol/l, uréée e
0,65 g/l, cr0,65 g/l, crééat 8 mg/l, Naat 8 mg/l, Na++ 136 mmol/l, K136 mmol/l, K+ + 4,5 mmol/l, Ca4,5 mmol/l, Ca2+2+ 1,1 mmol/l, 1,1 mmol/l,
MgMg2+2+ 0,5 mmol/l, Cl0,5 mmol/l, Cl-- 112 mmol/l, prot 39 g/l, phosphore 1,4 mmol/l, 112 mmol/l, prot 39 g/l, phosphore 1,4 mmol/l,
lactate = 2,2 mmol/l lactate = 2,2 mmol/l
InterprInterpr éétation de ltation de l ’é’équilibre acidoquilibre acido --basique?basique?
![Le système excréteur contribue au maintien de lhoméostasie : Osmolarité sanguine : [Solutés totaux ] sang Concentrations de certains ions : Na +, K + ;](https://img.dokumen.tips/doc/110x75/551d9dba497959293b8dde41/le-systeme-excreteur-contribue-au-maintien-de-lhomeostasie-osmolarite-sanguine-solutes-totaux-sang-concentrations-de-certains-ions-na-k-.jpg)
![Quebecmsssa4.msss.gouv.qc.ca/intra/formres.nsf/c6dfb077f4130b4985256… · Collet cervical Planche dorsale Sonde urinaire Drain thoracique (d/g) [2 Matelas immobilisateur C] Solutés](https://img.dokumen.tips/doc/110x75/607fab0df07ad1469146dcc5/collet-cervical-planche-dorsale-sonde-urinaire-drain-thoracique-dg-2-matelas.jpg)