Embed Size (px)
Citation preview

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Solutions for Nasal DefectsMarcelo Coelho Goiato, DDS, MD, PhD,*yDaniela Micheline dos Santos, DDS, MD, PhD,*yRenato Salviato Fajardo, DDS, MD, PhD,yStefan Fiuza de Carvalho Dekon, DDS, MD, PhDy
Abstract: Many studies on defects caused by trauma, infection, can-cer, or congenital are reported in the literature; in nasal reconstruc-tions, contradictions and distinct techniques exist that can be argued.Using the literature, we observe these distinct techniques that can besurgery or in surgery to reestablish and to integrate the patient withsatisfaction in the society.
Key Words: Rhinoplasty, nasal reconstruction, island flap, nasalprosthesis
Surgical excision of tumors from the face may create a defect thatis difficult to restore. Skin grafts can only cover superficial
defects and have a natural tendency to contract and may not takeproperly. In addition, because of color mismatch, it is not cosmet-ically identical to the face.1
A considerable number of people each year acquire facial defectsas a result of malignant disease, trauma, and congenital deformity.Malignancies of the nasal vestibule are rare and account for only 9%of all cancers of the nasal cavity.2
Nasal defects commonly seen by plastic surgeons result fromtrauma, burn injury, or tumor resection. Although nasal reconstruc-tion is one of the oldest plastic surgery endeavors, techniques con-tinue to evolve and be modified.3
Full-thickness nasal defects involving the alar rim require therestoration of the skin, the cartilage, and the nasal mucosa. The nasalskeleton is the supporting structure of the nose, and its integrity mustbe either maintained or restored for successful reconstruction. Nu-merous flaps were proposed in full-thickness defects. This reliableflap represents an alternative technique of composed grafts, dif-ferent nasolabial flaps, forehead flap, and so on.1,3Y7
Reconstruction of extensive nasal defects including the nasalbone, the septum, and the aesthetically defined units of the nosealways presents with certain difficulties. Forehead and free flaps canbe used for reconstruction of extensive nasal defects.5,8,9
The septal nasal perforation is an important problem for thelaryngologists and plastic surgeons. The reasons of septal nasalperforations are injuries, neoplasm, self-mutilation, chronic rhinitis,allergy, Wegener granuloma, sarcoidosis, tuberculosis, toxic metals(arsenic and chrome), some drugs (steroids), narcotizing agents(cocaine), and complications after endoscopic and septal nasaloperations.10
The main reasons that urge the patients to seek help are plasticcosmetic and functional impairments such as nasal obstruction.Surgical removal of the hyperplastic tumor mass is the treatment ofchoice for rhinophyma.11
Prosthetic rehabilitation is a surgical alternative in functional-aesthetic facial reconstruction when conventional reconstructivesurgery cannot be applied because of either the psychophysical con-ditions of the patient or an excessive substance loss.12,13 Prostheticsupply has been developed into a functional and aesthetic alternativeto plastic and reconstructive surgeries.14Y16
The purpose of this study was realized in a review of the indexedEnglish-language literature with the intention of coming up withsolutions for reconstructive surgery and no surgery of nose defects.
DISCUSSIONSolutions for Reconstructive Surgery and NoSurgery of the Nose Defects
Nasal defects are the most challenging of these facial defects. Nasalreconstruction requires reconstruction of 3 tissue layers: the innermucosal lining, the supporting structures (the cartilage or the bone),and the outer cutaneous lining. The new inner lining should consistof a well-vascularized thin tissue to prevent rejection of the cartilageor the bone in the supporting layer. For example, septal mucosa orskin can be used in various ways to reconstruct the inner lining. Thenew supporting structures, consisting of transplanted cartilage orbone, should be strong enough to prevent contraction of the softtissues’ inner and outer linings during wound healing. The outerlining is reconstructed per subunit of the nose, for example, thenostril, the ala nose, or the ridge of the nose. Usually, a paramedianforehead flap is used for the reconstruction of the outer lining.8,9
Surgical treatment, especially in cases of large septal perforation,is often difficult because of atrophy of the nasal mucosa and lack ofsuitable material for reconstruction. In surgical treatment, manymethods and reconstructive materials have been used. The followingautogenous tissues were used in the reconstruction of septalperforation: alloderm, temporal fascia, septal and auricle cartilage,cranial periosteum, perichondrium, ethmoidal, and hip bone. Thedefect of such materials is progressive resorption. For many years,the suitable synthetic material for septal nasal reconstruction hasbeen searched for. Among the biomaterials, the following have beenused without success: Dacron, porous polyethylene, dolomite, andbioglass. The rejection of the synthetic material was the reason of thefailure. In the implantation of the resorbable copolymer of glycolideand l-lactide, very good macroscopic and histological results wereachieved in vitro.10
To improve the function of the external airways, the patientunderwent surgery to reconstruct the nasal septum. Although car-tilage grafts are the state of the art to reconstruct the nasal septum,a bone graft from the iliac crest is used because the autoimmunepolychondritis precludes cartilage grafting because of expectedcartilage destruction. The use of bone grafts is a promising methodto restore and improve ventilation disorders caused by a saddle nosedeformity in relapsing polychondritis. The septum is reconstructedby insertion of a bone graft taken from the iliac crest. This methodhas been used and described in orofacial surgery before. However, ithas been proven to result to bone resorption. Here, cartilage graft-ing is not advisable, and bone grafting is the method of choice.17
Although autologous tissue is known as the best material, porouspolyethylene (Medpor) can be used safely regarding its low com-plication rate because of its porotic architecture and low morbidityin donors. Medpor implant provides functional improvement by itsstrength body. Its smooth surface helps to correct the asymmetry
BRIEF CLINICAL NOTES
2238 The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
From the *Buccal Oncology Center, and yDepartment of Dentistry Materialsand Prosthesis, Faculty of Dentistry of Ara0atuba, University of the State ofSao Paulo, Sao Paulo, Brazil.Received April 21, 2009.Accepted for publication May 30, 2009.Address correspondence and reprint requests to Dr Marcelo Coelho Goiato,
Departamento de Materiais Odontologicos e Protese, Faculdade deOdontologia de Ara0atubaVUNESP, Jose Bonifacio, 1193 VilaMendon0a, CEP 16015-050, Ara0atuba, Sao Paulo, Brazil;E-mail: [email protected]
Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181bf858c

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
by filling the defects. Using a saddle shape enabled us to treatdifferent components of the postrhinoplasty deformity with a singleimplant.18
Medial canthal and dorsal nasal defects after surgery have been achallenging problem for surgeons and patients to reduce scarring atthe donor area by planning a forehead island flap in an ellipticalfashion at the frontal hairline. There are no more incisions than theelliptical incision over the hairline. Primary closure of skin flaps atthe donor ensures a final scar that is hidden at the frontal hairlineborder. Forehead hairline island flap is an important flap for smalland medium defects as an alternative to the conventional paramedianforehead flap.9,19
Forehead flaps may be elevated as median or paramedianforehead flaps. Forehead flaps have certain advantages such as beinga local flap choice, accurate color and texture match, reliable flapchoice, and easy flap elevation technique. This technique also hascertain disadvantages such as scarring in the forehead area andrequiring a 2-step technique. We manage to primarily close foreheaddefects of 4 to 7 cm; however, in larger defects, full- and split-thickness skin grafts are used. The arterial supply of the foreheadflaps tends to become thinner when approaching the distal part of theflap, and this allows the surgeon to easily shape the flap and requiresless revision procedures.5
Grafts and local flaps are used in smaller defects. These defectsalso require replacement of all lost tissues to provide nasal lining,skeletal support, and skin coverage. Careful analysis of the defectand reliance on these general guidelines will allow for less obviousnasal reconstruction and a more natural appearance and function.3,4
On the other hand, some patients were defined as nonsatisfactory,with the deformity caused by scar retraction of the tip and ab-normalities in color and thickness of the skin grafted. With a fewexceptions, the patients had a good postoperative recovery withoutevents worthy of note. On the basis of the results obtained, we canrecommend an advancement flap for lateral nasal defects and trans-position of a nasolabial flap for the reconstruction of the nasal alar.Nasolabial flaps with a subcutaneous pedicle are effective for cor-recting injuries or defects involving the lateral surface of the nose.6
Although objective functional and aesthetic outcomes after nasalreconstruction sometimes show impairment compared with thenormal situation, they give high subjective patient satisfaction withfunction and aesthetics when reconstruction with a flap is used.20
The L-shaped split calvarial bone graft for nasal dorsal re-construction of septal saddle nose deformities provides the followingbenefits: dorsal support, increased tip projection, improved nasalairflow, and natural feel and appearance to the nose. The procedurecan be performed using the open rhinoplasty approach without theneed for radix incisions for rigid fixation or intranasal incisions. Inaddition, graft donor site morbidity is kept to a minimum. Theseadvantages make the split calvarial bone L-shaped strut techniqueexcellent for nasal reconstruction in patients with substantial septalsaddle nose deformities. Patients with chronic inflammatory condi-tions such as the Wegener disease are often excluded as acceptablesurgical candidates because of concerns about graft resorption andsurgical failure. We hope that the findings of this clinical series sug-gest otherwise.21
Reconstruction of total nasal defects remains one of the mostdifficult problems in plastic surgery because the nose combinesaesthetics and function. Standard techniques using either forehead ornasolabial flaps do not have a place in the case of extensive scarringon the face or areas with high risk of cancer recurrence on the face.In these cases, microsurgical free tissue transfer for soft tissuereconstruction in combination with bone grafts or implants for thenasal skeleton is ideal. Tsiliboti et al22 report the use of prelaminatedradial forearm flap with porous polyethylene implants for total nasalreconstruction.
The functional and the aesthetic outcomes were satisfactory inmost patients in whom a helical rim flap was used. The free vascu-larized preauricular and the helical rim flaps are a reliable method ofreconstructing nasal defects and have wide clinical applications.11
For Kalbermatten et al,23 the perichondrial cutaneous graft tech-nique provides a reliable composite graft routinely harvested fromthe anterior conchal bowl. This established perichondrial cutaneousgraft was simplified by using the less conspicuous posterior auriculardonor site, which can be closed without the need of cartilage resec-tion for reconstruction with a postauricular interpolated skin island.23
The surgical conduct for these cases is very complex because ofthe aesthetic consequences that result from the facial skeleton bonystructure resections and the contiguous vital organs proximity, as inthe orbit and the brain.24 The most common malignant tumors in thisarea are chondrosarcoma and osteogenic sarcoma.24Y26 Because ofthe bone limits of the paranasal sinus and the proximity of the vitalstructures, many times, the surgical reconstruction is not indicated,with a nasal rehabilitation with prosthesis being necessary (Figs. 1Y5).
Facial reconstruction with free microvascular flaps only hasrarely produced an aesthetic result. Menick stated that distant skinalways appears as a mismatched patch within a residual normalfacial skin. In addition, earlier techniques using a single large nasallining flap or bilateral nasal lining vaults incurred a high incidenceof airway obstruction. The authors used microvascular free flaps andhave proved them to be highly reliable and efficacious for restora-tion of missing elements of the nasal lining and adjacent facial softtissue defects in total and subtotal nasal reconstructions. Combinedwith a forehead flap, this aesthetic approach allows for reconstruc-tion of the center of the face layer by layer and facial unit by facialunit. Specific attention is paid to the artistic creation of normal nasaldimensions, proportion, and form using carved and assembled car-tilage grafts and by secondary subcutaneous contouring. In addition,this technique produces a patent airway.9,27
Rhinophyma, the end stage in the development of acne rosa-cea, is characterized by sebaceous hyperplasia, fibrosis, follicularplugging, and telangiectasia.28 It is assumed to be the end stage ofchronic acne rosacea.11
Although it is commonly considered a cosmetic problem, it canresult in gross distortion of soft tissue and airway obstruction. Basalcell carcinoma is a rare finding in patients with rhinophyma. Thepatient experienced chronic drainage and recurrent infections thatfailed conservative treatment with oral and topical antibiotics. Thepatient decided to proceed with surgical intervention and underwenttangential excision and dermabrasion in the operating room.28
Absence of half of the nose is an extremely rare congenital mal-formation, which has a devastating impact on the patient and thefamily. Pathogenesis is not clear, and the reported cases have
FIGURE 1. Nasal defect.
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2239

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
sporadically occurred. Many aspects must be considered whenreconstructing a congenital half-nose, such as the timing of surgery,the type of tissue to be used, and the need to reconstruct thenasal airway. Nasal reconstruction was performed at the age of 5 to 7years to minimize psychologic trauma. Forehead skin demonstratedto be an excellent donor site to resurface the nose. For the innerlining, a contralateral cutaneous nasal flap was our preference.Concerning the nasal framework reconstruction, alar contour wasrestored using a cartilage graft from the lower portion of the eartragus and the concha.29
Nasolabial flaps are very useful and versatile local flaps, withrobust vascularity that can be readily elevated without a delay. Theflap can be superiorly based to reconstruct defects on the cheek,the side wall or the dorsum of the nose, the alae, the collumula, andthe lower eye lid.1
The orbicularis oris myomucosal island flap is based solely onpart of the orbicularis oris muscle as a new flap for nasal lining. Theflap is designed horizontally on the oral mucosa of the upper lipalong the gingivolabial sulcus. The upper margin of the flap is de-signed just below the buccal sulcus. The pedicle location is selectedbased on the location of the nasal lining defects. The medial musclepedicle is chosen when the defect is located behind the columellaand the soft triangle, the lateral muscle pedicle is chosen when thedefect is located around the lateral two thirds of the ala, and thebilateral or unilateral muscle pedicle is chosen when the defect islocated around the nasal floor.7
For immediate nasal reconstruction with superficial temporalfascia, open rhinoplasty was used for absolute removal of the ab-sorbed foreign body from beneath the skin of the nasal dorsum
by the use of a rasp or curette. Any remnant foreign body then wasirrigated by an isotonic sodium chloride solution. It was incisedand dissected in the temporal area at 3 cm to check the superficialtemporal fascia. Fascia was harvested (7 � 3 cm) from the temporalarea. The fascia was used to wrap the thin silicon implant, afterwhich the fascia and implant were sutured using an absorbable su-ture material. The silicon implant wrapping with superficial tempo-ral fascia was inserted into the depressed nasal dorsum to correctthe nasal deformity.30
Efficient prosthetic supply in the exposed facial area requires awell scheduled and close cooperation between the surgeon and theanaplastologist. Preoperative diagnostic evaluation and operativefilling of the magnetic fixation in cooperation with the anaplastol-ogist provide satisfying functional and cosmetic prosthetic outcomesfor the patient. Advantages of this procedure combine early cosmeticrehabilitation with the option to directly investigate the tumor siteafter resection. Novel magnet systems provide a high degree offlexibility combined with confident fixation. Prosthetic rehabilita-tion should be offered and discussed with patients ahead of can-cer surgery in the head and neck area. This procedure should beconsidered in particular in patients who reject or are not feasible formultistep reconstructive surgery.13,14
The association of dental implants and prostheses promotes aes-thetic and function in the patient with nasal defects.15,16
No patient experienced severe inflammation requiring adminis-tration of systemic antibiotics or surgical revision. Implant successwas 100% in both the irradiated and the nonirradiated patients. Thedental implants result in a high rate of success in retaining mid-face prostheses and offer good stability and aesthetic.15
FIGURE 3. Patient’s face with nasal carcinoma. FIGURE 5. Nasal prosthesis.
FIGURE 4. Patient’s face with defect after total rhinectomy.FIGURE 2. Free flap transfer to the nose.
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2240 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
The titanium implants placed failed to support a nasal epithesisin a patient with hepatitis C virus, with an important parodontaldisease, who experienced a postinfective necrosis of the nose after aliver transplantation; it was necessary to place an adhesive pros-thesis. An implant failure was also observed in diabetic patientswith extensive midfacial defects due to a mycotic infection, but it didnot compromise the retention of the prosthesis. According to ourexperience, the indication to epithesis is when the conventional re-constructive interventions are inapplicable.12
The functional and aesthetic satisfaction of the patient after anasal reconstruction surgery or with prosthesis is a great challengeof the studies in literature.
REFERENCES
1. El-Marakby HH. The versatile naso-labial flaps in facial reconstruction.J Egypt Natl Canc Inst 2005;17:245Y250
2. Fradis M, Podoshin L, Gertner R, et al. Squamous cell carcinoma of thenasal septum mucosa. Ear Nose Throat J 1993;72:217Y221
3. Stewart D, Mentzer RM Jr. Nasal reconstruction. J Ky Med Assoc2003;101:280Y287
4. Delbaere-Delbecque M, Delaporte T, Toussoun G, et al. Modified Texiermediodorsal transposition island skin flap of the nose. Report of fourcases of ala nasi reconstruction. Ann Chir Plast Esthet 2007;52:130Y139
5. Ayhan M, Gorgu M, Aytug Z, et al. Comparison of aestheticoutcomes and morbidity of nasal reconstruction with forehead flapsand free flaps. Microsurgery 2007;27:411Y414
6. Cervelli V, Bottini DJ, Gentile P. Reconstruction of the nasal tip.J Craniofac Surg 2007;18:1380Y1384
7. Kashiwa K, Kobayashi S, Honda T, et al. Orbicularis oris myomucosalisland flap transfer to the nose. J Plast Reconstr Aesthet Surg 2009;62:e341Ye344
8. Hofer SO, Mureau MA. Surgical reconstruction of large defects of thenose. Ned Tijdschr Geneeskd 2008;152:1657Y1664
9. Boyd MC, Baker SH, Fader DJ, et al. The forehead flap for nasalreconstruction. Arch Dermatol 2000;136:1365Y1370
10. Scierski W, Polok A, Namysaowski G, et al. Study of selectedbiomaterials for reconstruction of septal nasal perforation. OtolaryngolPol 2007;61:842Y846
11. Sadick H, Goepel B, Bersch C, et al. Rhinophyma: diagnosis andtreatment options for a disfiguring tumor of the nose. Ann Plast Surg2008;61:114Y120
12. Leonardi A, Buonaccorsi S, Pellacchia V, et al. Maxillofacial prostheticrehabilitation using extraoral implants. J Craniofac Surg 2008;19:398Y405
13. Rodrigues S, Shenoy VK, Shenoy K. Prosthetic rehabilitation of apatient after partial rhinectomy: a clinical report. J Prosthet Dent2005;93:125Y128
14. Volkenstein S, Dazert S, Jahnke K, et al. Prosthetic supply of tissuedefects in head and neck surgery [in German]. Laryngorhinootologie2007;86:854Y860
15. Scolozzi P, Jaques B. Treatment of midfacial defects using prosthesessupported by ITI dental implants. Plast Reconstr Surg 2004;114:1395Y1404
16. Boudard P. Analysis of the possibilities for reconstruction of partialnasal tissue loss. Rev Laryngol Otol Rhinol (Bord) 2007;128:243Y248
17. Haug MD, Witt P, Kalbermatten FD, et al. Severe respiratorydysfunction in a patient with relapsing polychondritis: should we treatthe saddle nose deformity? J Plast Reconstr Aesthet Surg 2009;62:e7Ye10
18. Turegun M, Acarturk TO, Ozturk S, et al. Aesthetic and functionalrestoration using dorsal saddle shaped Medpor implant in secondaryrhinoplasty. Ann Plast Surg 2008;60:600Y603
19. Karzda? S, Sacak B, Bayraktaroglu S, et al. A novel approach for thereconstruction of medial canthal and nasal dorsal defects: frontal hairlineisland flap. J Craniofac Surg 2008;19:1653Y6517
20. Mureau MA, Moolenburgh SE, Levendag PC, et al. Aesthetic and
functional outcome following nasal reconstruction. Plast Reconstr Surg2007;120:1217Y1227. Discussion 1228Y1230
21. Shipchandler TZ, Chung BJ, Alam DS. Saddle nose deformityreconstruction with a split calvarial bone L-shaped strut. Arch FacialPlast Surg 2008;10:305Y3011
22. Tsiliboti D, Antonopoulos D, Spyropoulos K, et al. Total nasalreconstruction using a prelaminated free radial forearm flap and porouspolyethylene implants. J Reconstr Microsurg 2008;24:449Y542
23. Kalbermatten DF, Haug M, Wettstein R, et al. New posterior auricularperichondrial cutaneous graft for stable reconstruction of nasaldefects. Aesth Plast Surg 2005;29:489Y495
24. Goiato MC, Fernandes AUR, Santos DM, et al. Positioning magnets ona multiple/sectional maxillofacial prosthesis. J Contemp Dent Pract2007;8:101Y107
25. Glover AT, Grove AS. Orbital invasion by malignant eyelid tumours.Ophthal Plast Reconstr Surg 1989;5:1Y12
26. Howard GR, Nerad JA, Carter KD, et al. Clinical characteristicsassociated with orbital invasion of cutaneous basal cell and squamouscell tumours of the eyelid. Am J Ophthalmol 1992;113:123Y133
27. Burget GC, Walton RL. Optimal use of microvascular free flaps,cartilage grafts, and a paramedian forehead flap for aestheticreconstruction of the nose and adjacent facial units. Plast ReconstrSurg 2007;120:1171Y1207. Discussion 1208Y1216
28. Leyngold M, Leyngold I, Letourneau PR, et al. Basal cell carcinomaand rhinophyma. Ann Plast Surg 2008;61:410Y412
29. da Silva Freitas R, Alonso N, de Freitas Azzolini T, et al. The surgicalrepair of half-nose. J Plast Reconstr Aesthet Surg 2008;29E-pub ahead of print
30. Lee KC, Ha SU, Park JM, et al. Foreign body removal and immediatenasal reconstruction with superficial temporal fascia. Aesth PlastSurg 2006;30:351Y355
Excision and Grafting ofPalmoplantar Keratoderma
Aron G. Nusbaum, BS,* Erick G. Martell, MD,*Susan Bard, MD,y Elizabeth Alvarez Connelly, MD,ySeth R. Thaller, MD, DMD*
Abstract: Palmoplantar keratodermas may present to the clinicianwith an extremely broad series of clinical findings. Management hasalso taken on a wide variety of medical and surgical modalities. Theliterature seems to provide evidence that optimum managementconsists of surgical excision with skin grafting. It is believed that thiswill eliminate all of the underlying tissue and associated skin ap-pendages, which are believed to be the source of this abnormal skinentity. We present a case of a patient in which tangential excisionwith delayed split-thickness skin grafting was performed after initialapplication of an acellular dermal matrix (Integra). Unfortunately,
From the *Division of Plastic and Reconstructive Surgery, and yDepartment ofDermatology and Cutaneous Surgery, Miller School of Medicine, University ofMiami, Miami, Florida.Received May 18, 2009.Accepted for publication May 30, 2009.Address correspondence and reprint requests to Seth R. Thaller, MD, DMD,
Division of Plastic and Reconstructive Surgery, Miller School ofMedicine, University of Miami, 1611 NW12th Ave ET3019, Miami,Florida 33101; E-mail: [email protected]
Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181bf85a6
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2241

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.9
there was nearly immediate recurrence of this disease, and we,therefore, suggest a more aggressive approach to the initial excision.
Key Words: Palmoplantar keratodermas (PPK), split-thicknessgrafting
CLINICAL REPORT
A 5-year-old African-American girl presented to the plastic surgeryclinic with a history of progressive skin thickening on the volaraspects of the hands and the plantar aspects of the feet since birth. Atage 1 year, these areas became increasingly symptomatic with in-creasing pain on ambulation, writing, and with the use of utensils.There is no associated family history of similar skin changes.
Physical examination revealed areas of focal hyperkeratosis,consisting of yellow-brown plaques involving the pressure points ofthe plantar areas and smaller hyperkeratotic plaques on the volaraspect of the fingertips (Fig. 1). Flexion contractures were noted onthe interphalangeal joint of the thumbs and the distal interphalangealjoints of the index fingers (Fig. 2). Narrowing of the fingertips wasnoted on the thumb and index fingers bilaterally. Prominent lunulaeof the fingernails were noted. Medial displacement of the right greattoenail was also present and coincided with the thickest area ofplantar keratoderma. The most prominent area of palmar kerato-derma was present on the right thumb, which also exhibited the mostsevere distal tapering.
Complete blood cell count and metabolic and lipid panel valueswere all within normal limits. Medical treatment was initiated with10-mg etretinate daily with minimal improvement. The patient wasreferred to plastic surgery service for evaluation and treatment of theplantar keratoderma.
To facilitate postoperative ambulation, the initial procedure wasconfined to the right foot. Tangential excision of 2 hyperkeratoticplaques was performed to the depth of the deep dermis (Fig. 3). Theplaque on the metatarsal/instep area measured 8 � 10 cm, andthe plaque on the calcaneal area measured 3 � 4 cm. A dermalregeneration template consisting of cross-linked bovine cartilage andglycosaminoglycan matrix (Integra Life Sciences, Plainsboro, NJ)was applied to the wound and subsequently grafted with a thick split-thickness skin graft (Fig. 4) and vacuum-assisted closure.
Histopathologic examination revealed acanthotic and markedlyhyperkeratotic squamous epithelium consistent with keratoderma.
Postoperatively, it was observed that there was no graft take.Sporadic areas of recurrence were noted in the periphery and centerof the grafted areas at 3 weeks.
DISCUSSION
Palmoplantar keratodermas (PPKs) exhibit a broad range of clinicalcharacteristics possessing marked overlap between a variety ofclinical entities. Itin and Fistarol1 presented a scheme for classifyingthese disorders based on genetic transmission and described a dif-fuse versus circumscribed pattern. However, they reported that theclinical spectrum of PPK may be interindividually variable. Morerecently, these disorders have been separated by elucidating theirmolecular and genetic defects.2
We report a 5-year-old African-American girl with severe focalPPK present since birth with no associated family history of thedisease. Presence of flexion contractures, prominent lunulae,tapering, and constrictions of the digits in association with PPKare suggestive of the diagnosis of Huriez syndrome, an autosomaldominant syndrome characterized by diffuse scleroatrophy of thehands with sclerodactyly, PPK, and nail changes.3 Reports of Huriezsyndrome typically describe a mild diffuse and smooth PPK withatrophy of the fingertips and toes.3,4 Additional features such asflexion contracture, tapering of the digits, and hypoplastic nails withridging and prominent lunulae have also been described.5,6
Histologic findings in Huriez are nonspecific. They are character-ized by hyperkeratosis and acanthosis.4,7 Immunohistologic andultrastructural studies performed on 2 patients revealed almostcomplete absence of Langerhans cells.3,7
Autosomal dominant genetic transmission has been reportedin all cases of Huriez syndrome.3 Lack of family history and the
FIGURE 1. Yellow-brown hyperkeratotic plaques on thepressure points of the plantar areas and on the volar aspectsof the fingertips.
FIGURE 2. Digital constrictions, distal hyperkeratoticplaques, and flexion contracture of left fifth digit.
FIGURE 3. Right foot status post-tangential excision ofhyperkeratosis to the depth of the deep dermis.
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2242 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
possibility that this may be the first African American describedwith this syndrome indicate that our case may be considered unique.In addition, severity of the focal, thick hyperkeratotic plaques inour patient markedly contrasts with the diffuse/mild keratodermadescribed in previously reported cases.
Treatment of PPKs consists of topical keratolytics, systemicretinoids, and, in severe cases, tangential or full excision with skingrafting. Owing to the overwhelming thickness of the plantarhyperkeratosis that resulted in pain upon ambulation, our patientunderwent excision with split-thickness skin grafting after failingtreatment with etretinate.
There are 9 previously reported cases of plantar keratodermastreated by surgical excision with skin grafting. Although Lucker andSteijlen8 reported a case of full-thickness excision, no follow-upinformation was given. Wynn-Williams9 and Dencer10 each report1 patient with a successful outcome and describe their procedures asfull-thickness excision and complete excision, respectively.
Three patients underwent initial excision to the dermal levelwith subsequent grafting and experienced recurrence of the le-sions.11Y13 Two of these 3 patients underwent a second procedurein which the excision was carried down to the plantar aponeurosiswith no recurrence reported upon 6-month and 5-year follow-up.11,12 Another report of total excision of the sole to the level ofthe plantar aponeurosis was also reported to result in a successfuloutcome.14
Bedard et al15 reported 2 patients who experienced recurrencesin the grafted areas or at the periphery of the grafts. Excision wascarried to the level of the deep subcutaneous fat. Results were nev-ertheless viewed as successful with functional improvement despitethe need to treat focal recurrences with shave excision and etretinate.
In our patient, we chose to excise the lesions down to the dermalbed. Immediate recurrence and lack of graft viability were possiblydue to insufficient depth of excision. Friction may have played arole in failure of graft take.
CONCLUSIONS
We present a case of PPK treated with excision and grafting. Pre-vious case reports suggest that to prevent recurrence, excision ofplantar keratoderma must be carried to the level of the aponeurosis,removing all skin appendages.11 However, caution is advised whentreating children, as one must take into account the risk of growthrestriction if a graft is placed directly on the plantar aponeurosis.15
Lack of response to medical therapy in addition to these consid-erations would lead clinicians to continue to seek effective treatmentmodalities.
REFERENCES
1. Itin P, Fistarol S. Palmoplantar keratodermas. Clin Dermatol 2005;23:15Y22
2. Kimyai-Asai A, Kotcher L, Jih M, et al. The molecular basis ofhereditary palmoplantar keratodermas. J Am Acad Dermatol 2002;47:327Y343
3. Hamm H, Traupe H, Brocker B, et al. The scleroatrophic syndrome ofHuriez: a cancer prone genodermatosis.Br J Dermatol 1996;134:512Y518
4. Delaporte E, N’Guyen C, Janin A, et al. Keratoderma with scleroatrophyof the extremities or sclerotylosis (Huriez syndrome): a reappraisal.Br J Dermatol 1995;133:409Y416
5. Kavanagh G, Jardine P, Peachey R, et al. The scleroatrophic syndromeof Huriez. Br J Dermatol 1997;137:114Y118
6. De Berker D, Kavanagh G. Distinctive nail changes in scleroatrophyof Huriez (abstract). Br J Dermatol 1993;129:46
7. Guerriero C, Albaneski C, Girolomoni G, et al. Huriez syndrome: casereport with detailed analysis of skin dendritic cells. Br J Dermatol2000;143:1091Y1096
8. Lucker GP, Steijlen PM. The Olmstead syndrome: a mutilatingpalmoplantar and periorificial keratoderma. J Am Acad Dermatol1994;31:508Y509
9. Wynn-Williams D. Plantar keratodermia treated by split-skin grafts.Br J Plast Surg 1953;6:123Y129
10. Dencer D. Tylosis. Br J Plast Surg 1953;6:130Y14011. Keir M. Keratodermia palmaris et plantaris. Br J Dermatol 1967;79:
419Y42112. Chaouat M, Levan P, Mimoun M. Palmoplantar keratoderma: usefulness
of a surgical procedure. Ann Plast Surg 2001;46:664Y66513. Larregue M, Callot V, Kanitakis J, et al. Olmstead syndrome: report of
two new cases and literature review. J Dermatol 2000;27:557Y56814. Salamon T, Bogdaniv B, Sucur D. The surgical treatment of
palmo-plantar keratoderma. Br J Dermatol 1969;81:363Y36615. Bedard M, Powell J, Laberge L, et al. Palmoplantar keratoderma and
skin grafting: postsurgical long-term follow-up of two cases withOlmsted syndrome. Pediatr Dermatol 2008;25:223Y229
Supraorbital Nerve NeuromaCaused by Blind Curettage ofan Infected Epidermal Cyst
Hyoseob Lim, MD, Il Jae Lee, MD, Nam Suk Pae, MD,Myong Chul Park, MD, PhD
Abstract: A 38-year-old woman presented with a tender mass withmild erythematous change above the left eyebrow area. She had re-ceived curettage in another clinic after a diagnosis of infected epider-mal cyst 5 years previously. On examination, a round, irregular scarand a mass of 1-cm diameter associated with mild erythematous re-gion were observed above the right eyebrow.
From the Department of Plastic and Reconstructive Surgery, Ajou UniversityHospital, Suwon, South Korea.Received May 25, 2009.Accepted for publication May 30, 2009.Address correspondence and reprint requests to Dr Myong Chul Park,
Department of Plastic and Reconstructive Surgery, AjouUniversity School of Medicine, Wonchun-Dong, Yongtong-Gu,Suwon, 443-721, Gyeonggi-Do, South Korea;E-mail: [email protected]
None of the authors have a financial interest in any of the products,devices, or drugs mentioned in this paper.
Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181bf85bc
FIGURE 4. Wound coverage achieved with split-thicknessgrafts taken from the right thigh.
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2243

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Exploration disclosed a 1-cm neuroma with mild adhesion to abranch of the supraorbital nerve. The neuroma was completely re-moved. However, although partial transection of the supraorbitalnerve was performed during surgery, the nerve was not repaired. Theopen wound was repaired securely. A histopathologic examinationof the resected specimen resulted in a diagnosis of traumatic neu-roma. The patient had no forehead numbness before or after surgery.
Key Words: Supraorbital nerve, neuroma, curettage
Traumatic neuroma may result from partial laceration, completetransection, or external compression by acute nerve injury or
chronic nerve entrapment. Furthermore, axonal injury initiates a re-parative response, whereby the distal portion of the damaged axonis gradually absorbed in a process called Wallerian degenerationand the proximal portion retains a potential for regeneration. If dis-placement has occurred between the nerve endings, sprouting axonsmay be unable to reach the distal endoneural tubes and will insteadcontinue to elongate and proliferate at the site of the injury to form aneuroma. In this paper, the authors document a case of supraorbitalnerve neuroma caused by simple and blind curettage of infectedepidermal cyst above an eyebrow.
CLINICAL REPORTA 38-year-old woman noticed a tender mass with mild erythematouschange above the left eyebrow. She had undergone curettage in thisregion at another clinic for an infected epidermal cyst 5 years pre-viously. She had visited our hospital because the lesion had recurredat the original site. On examination, a round 1-cm-diameter sub-cutaneous mass was found at the original irregular scar with anassociated 1-cm-diameter mild erythematous mass above the lefteyebrow (Fig. 1). She complained of mild tenderness and cosmesis,but she had no numbness of the forehead or tingling sensation. Ourpreoperative impression was that the mass was a recurrence of theprevious epidermal cyst.
The subcutaneous mass was identified under a loupe as a 1-cm-diameter neuroma during operation, which mildly adhered to abranch of the supraorbital nerve. The neuroma was completelyremoved, and although partial transection of the supraorbital nervewas performed during surgery, no repair was conducted. The openwound was repaired securely. The subsequent examination of theresected mass revealed it to be round, irregular, and 1 cm in diameter(Fig. 2). Disordered nerve fiber bundles intermixed with connectivetissue. The small bundles of axons were surrounded by organizedlayers containing Schwann cells, fibroblasts, and perineurial cells(Fig. 3). Accordingly, a diagnosis of traumatic neuroma was made.The patient had no numbness of the forehead before or after surgery.During 1-year follow-up, the operative scar was acceptable and nocomplications were found, such as hypoesthesia and recurrence.
DISCUSSION
Traumatic neuroma can be caused by partial laceration, completetransection, or external compression due to acute nerve injury orchronic nerve entrapment. 1Y3 Axonal injury initiates a reparativeresponse, whereby the distal portion of the damaged axons isgradually absorbed in a process called Wallerian degeneration toform empty endoneural tubes. On the other hand, the proximalportions of the axons maintain the potential for regeneration.However, if nerve endings become displaced, sprouting axons maybe unable to reach the distal endoneural tubes and continue toelongate and proliferate in a disorganized manner at injury sites toform a neuroma.3,4
The supraorbital nerve is a branch of the frontal nerve, whichoriginates from the ophthalmic branch of the trigeminal nerve.3,4
This nerve runs through the supraorbital foramen or notch, ascendsthe forehead with the supraorbital artery, and then divides intoa smaller medial and lateral branch, which supply the skin of thescalp almost as far back as the lambdoid suture.5 The supraorbitalnerve typically exits the frontal bone via a palpable notch or fo-ramen along the medial third of the supraorbital rim.5 However, inrare instances, this exit may be located anywhere along or aboveor even lateral to the supraorbital rim.2,6 Immediately after the su-praorbital nerve exits its foramen, the nerve trunk forms superficial(medial) and deep (lateral) divisions.2,5 The superficial (medial)division passes over the frontalis muscle and provides sensory sup-ply to the forehead skin and the anterior margin of the scalp.5 On theother hand, the deep (lateral) division runs cephalad across thelateral forehead between the galea aponeurotica and the pericrani-um and provides sensory innervation to the frontoparietal scalp.5,6
When blind curettage is performed around the supraorbital fo-ramen, injury of this superficial division may cause a neuroma to
FIGURE 1. A 38-year-old woman noticed a 1-cm tendermass with mild erythematous change above the lefteyebrow area (arrow).
FIGURE 2. The mass was irregular, firm, and 1 cm indiameter.
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2244 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
form. Those conditions are able to show symptoms, such as pain,tingling sensation, and hypoesthesia. Those symptoms can makea diagnosis of nerve injury or neuroma formation. However, in thepresent case, numbness or hypoesthesia of the scalp and the fore-head did not occur because of dual innervation by the superficialand deep divisions; this situation can lead to missed diagnoses ofsupraorbital nerve injury.5
Many reports have been issued on supraorbital neuromas causedby endoscopic forehead lifts, motor vehicle collisions, shrapnel in-juries, orbital enucleation, halo fixation, frontal bone fracture, swimgoggle use, and even insect bites.1,2,7 However, to our knowledge,this is the first case of a supraorbital nerve neuroma caused by blindcurettage.
Epidermal cysts are the most common cyst type encountered andoccur primarily on the face, back or base of the ears, chest, or back.8
Although excision of the entire epidermal lining is usually bestdeferred until the inflammation and infection have subsided, simpleand blind curettage of infected epidermal cysts is a recognizedmeans of controlling infection.8 Many physicians consider this pro-cedure simple and straightforward. However, in the described case,simple curettage of an infected epidermal cyst near the supra-orbital nerve caused neuroma formation. Furthermore, the encoun-tered mass could easily have been misdiagnosed as a recurrentepidermal cyst, and thus, we advise that care be taken when con-fronted by a recurrent mass near the supraorbital nerve and foramen.
Summarizing, we describe a case of supraorbital nerve neuromacaused by blind curettage of an infected epidermal cyst. Many pre-vious reports have cautioned that treatment of infected epidermalcysts may cause neuroma formation. However, to our knowledge,this is the first case of supraorbital nerve neuroma caused by blindcurettage. The treatment of neuroma involves complete removalwithout minimal nerve injury to prevent recurrence and numbness.Furthermore, if a neuroma, as a result of misdiagnosis, is treated asa recurred epidermal cyst, serious problems could ensue, such as,prolonged pain and recurrence. Accordingly, care is required duringboth diagnosis and treatment of recurrent mass after blind curettageof epidermal cyst.
REFERENCES
1. Benvenuti D. Endoscopic brow lifts with injury to the supraorbital nerveand neuroma formation. Plast Reconstr Surg 1999;104:297Y298
2. Ducic I, Larson EE. Posttraumatic headache: surgical management ofsupraorbital neuralgia. Plast Reconstr Surg 2008;121:1943Y1948
3. Kakinoki B, Ikeguchi R, Atiyya AN, et al. Treatment of posttraumaticpainful neuromas at the digit tip using neurovascular island flaps.J Hand Surg Am 2008;33:348Y352
4. Tashiro A, Imafuku S, Furue M. Traumatic neuroma of the lower lipwith intraepithelial nerve fibers. J Cutan Pathol 2008;35:320Y323
5. Beer GM, Putz R, Mager K, et al. Variations of the frontal exit ofthe supraorbital nerve: an anatomic study. Plast Reconstr Surg1998;102:334Y341
6. Knize DM. A study of the supraorbital nerve. Plast Reconstr Surg1995;96:564Y569
7. Jacobson RI. More Bgoggle headache[: supraorbital neuralgia.N Engl J Med 1983;308:1363
8. Leon P. Benign tumors of the skin. In: Mathes SJ, Hentz VR. eds.Plastic Surgery, 2nd ed/V. Philadelphia: Saunders, 2006:256Y257
Recurrent and Refractory GiantCell Tumor of the Jaw
Millicent O. Rovelo, BS, Regina Kim, MD,Leo Mascarenhas, MD, Jeffrey Hammoudeh, MD, DDS,Mark M. Urata, MD, DDS
Abstract: Recurrent giant cell tumors refractory to various treatmentmodalities are challenging dilemmas for the most experienced prac-titioner. We report a case of a multiply recurrent aggressive giant celltumor diagnosed at 10 months of age with extensive involvementof the maxillae and mandibles unresponsive to multiple therapeuticmodalities. The various treatments attempted in this patient includingconventional therapies as well as the original use of bevacizumab(Avastin) are described.
FIGURE 3. Histopathologic section showing disordered nerve fiber bundles intermixed with connective tissue (left: hematoxylinand eosin, original magnification �40; right: hematoxylin and eosin, original magnification �200).
From the Children’s Hospital Los Angeles and Keck School of Medicine ofthe University of Southern California, Los Angeles, California.Received May 10, 2009.Accepted for publication June 21, 2009.Address correspondence and reprint requests to Mark M. Urata, MD, DDS,
Children’s Hospital Los Angeles, 4650 W Sunset Blvd, MS #96,Los Angeles, CA 90027; E-mail: [email protected]
Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181bf866e
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2245

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Key Words: Giant cell tumor, mandible, maxilla, Avastin,bevacizumab, antiangiogenic therapy, osteoglophonic dwarfism
A lthough a number of tumor types may demonstrate largenumbers of giant cells, 3 distinct entities are found in the head
and neckVbrown tumor of hyperparathyroidism, giant cell repar-ative granuloma, and true giant cell tumor. In 1986, giant cell tumorswere classified into 2 subgroupsVnonaggressive and aggressivebased on a clinicopathology study of tumors arising in the maxil-lofacial skeleton.1 Nonaggressive tumors included brown tumor andgiant cell granuloma and were defined by slow growth, minimalsymptoms, and a low rate of recurrence. Aggressive tumors, theBtrue[ giant cell tumors of the jaw, were defined as greater than5 cm, rapidly growing, recurring, or resulting in tooth displacement,root resorption, or cortical perforation. Given the virtually identicalhistological appearance of giant cell lesions, this stratificationallowed for treatment based on clinical presentation.
Our patient was classified as having an aggressive giant celltumor of the jaw based on her initial presentation. As we will discussbelow, she had persistence of her giant cell tumors despite a tem-porary response and disease stabilization with various treatmentmodalities that included surgery, embolization, antiangiogenic ther-apy, chemotherapy, hormonal therapy, and bisphosphonates.
CLINICAL REPORT
An 8-month-old female infant presented in June 2003 with a5-month history of gingival hyperplasia and bleeding gums. Med-ical history was significant for a neonatal intensive care unit staysecondary to chronic lung disease and failure to thrive. She also hada history of osteoglophonic dwarfism, cranial vault remodeling,tracheostomy, and gastrostomy-tube placement.
A facial computed tomographic (CT) scan was obtained thatdemonstrated a soft tissue mass involving the maxilla and mandible.Intralesional biopsy confirmed giant cell tumor pathology. Sheunderwent 2 resections by the age of 1 year, the first of whichincluded administration of intralesional steroids and the extractionof 2 teeth. Because of the rapid tumor growth, she was given inter-feron >2b therapy in March 2004. After a period of slower growth,the tumor rapidly began to increase in size (Fig. 1). In addition, her
interferon therapy was associated with intractable vomiting andmarked electrolyte abnormalities. Interferon therapy was thereforediscontinued after only 3 months. Two additional attempts at tumordebulking resulted in significant blood loss and infection. A sub-sequent CT scan demonstrated impending invasion of the cranialbase. Chemotherapy with doxorubicin and cyclophosphamide wastherefore initiated in an attempt to decrease the tumor size and todivert it away from vital cranial base structures. The patient received6 courses of chemotherapy with the same agents between July 2004and December 2004 and achieved a partial response. Therapy withpegylated interferon >2b was initiated on a weekly basis during thelast 3 months, with the hope that it would contribute to her continuedresponse and have fewer adverse effects than previously. Chemo-therapy was discontinued because of the fear of cardiotoxicityassociated with cumulative anthracycline dose. Shortly after this, thetumors progressed, prompting another embolization and an addi-tional 2 resections. Despite these resections, the tumors recurredand continued to increase in size. Bisphosphonate therapy withintravenous pamidronate therapy was initiated, together with theongoing interferon therapy. During this period, progressive tumorgrowth resulted in an additional embolization and 2 further de-bulking procedures. In March 2006, the interferon therapy wasdiscontinued secondary to ineffectiveness and continued tumorgrowth, but pamidronate therapy was continued to improve the poorbone health associated with osteoglophonic dwarfism. The patientwas then administered a low-dose vincristine intravenously andcyclophosphamide enterally as antiangiogenic therapy. This, too,was stopped 5 months later secondary to ineffectiveness and tumor-associated bleeding.
In August 2006, an interdisciplinary conference was held withthe patient’s family regarding further treatment options. A trial ofcalcitonin administered subcutaneously was offered. Continuedgrowth of these tumors prompted 3 more embolizations and debulk-ing procedures and discontinuation of the calcitonin. Computedtomographic scans continued to demonstrate enlarging tumor. Be-cause of the recalcitrant nature of the tumor, the patient was given atrial of bevacizumab (Avastin [Genetech, Inc, South San Francisco,
FIGURE 1. Clinical photograph of the patient after 2resections and 3 months of interferon therapy (June 2004).
FIGURE 2. Coronal three-dimensional CT reconstruction(December 2008).
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2246 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
CA]) immunotherapy. Beginning in September 2007, the patientreceived 12 doses of bevacizumab at a dose of 10 mg/kg every2 weeks over a 6-month period. Given the lack of safety informationand the patient’s complicated medical issues, bevacizumab wasgiven as monotherapy, rather than in combination with chemo-therapy. After an initial stabilization of tumor growth and a minorsubjective response, the tumors continued to progress, and beva-cizumab, too, was discontinued in March 2008. The patient con-tinues to have enlarging giant cell tumors of her maxillae andmandibles (Figs. 2 and 3), while continuing on intravenously admin-istered pamidronate that is now being administered on a quarterlybasis. At this time, the patient is alive and receiving symptomaticmanagement. She will continue to be offered surgical debulking asneeded for palliative care or offered experimental therapy should asuitable agent be available.
DISCUSSION
We present the case of a 6-year-old girl with osteoglophonicdwarfism and refractory giant cell tumors of the jaws. Classified ashaving an aggressive giant cell tumor, the patient was expectedto have demonstrated a response to enucleation and adjuvant ther-apy with interferon. Her resistance to all treatment modalities hastherefore become a complex medical issue and is of intense biologicinterest.
Nonaggressive giant cell lesions can often be successfully treatedwith enucleation and curettage, whereas aggressive lesions typicallyrequire multiple treatment modalities. In the past, the standardtreatment was en bloc resection for these aggressive tumors; how-ever, because of the resulting disfigurement and the need for sub-sequent reconstruction, current treatment involves enucleation incombination with adjuvant therapy. Adjuvant therapies include em-bolization, intralesional steroids, calcitonin, radiation, and chemo-therapy. Radiation therapy was not attempted in this patient becauseof her age and the location of the tumors, as it would certainlyresult in unacceptable morbidity. However, this remains a treatmentmodality that will be considered later once the patient is older.
Giant cell tumors are highly vascular lesions. As such, they tra-ditionally respond to antiangiogenic therapy. Recently, much data
have been published describing the effectiveness of interferon > inthe treatment of recalcitrant giant cell tumors.2Y4
One of the newer antiangiogenic therapies is bevacizumab(Avastin), a monoclonal antibody that targets vascular endothe-lial growth factor A. Bevacizumab currently has Food and DrugAdministration approval for use in metastatic renal cell cancer, colonand rectal cancer, nonYsmall cell lung cancer, and HER2-negativebreast cancer. Bevacizumab is most effective when used in com-bination with chemotherapy. It is believed to stabilize the tumorvasculature, thereby resulting in decreased tumor shedding andmetastasis, as well as improved delivery of therapeutic agents.5,6 Ourpatient had a rapid growth of her giant cell tumor, despite treatmentwith various modalities, including antiangiogenic therapies withinterferon and low-dose chemotherapy. Therefore, therapy withbevacizumab was attempted.
There is one other reported case of a patient with osteoglophonicdwarfism who developed intractable mandibular swelling resem-bling giant cell granulomata. The tumor was unresponsive to vinblas-tine and methotrexate but eventually was suppressed by intravenouslyadministered bisphosphonate.7 This similar resistance to therapy ismost likely directly related to the comorbidity of osteoglophonicdwarfism. Osteoglophonic dwarfism is caused by activatingmutationsin FGFR1, a receptor for fibroblast growth factors (FGFs) that ispresumably involved in the modulation of bone elongation.7 This isthought to contribute to the characteristic features of the disease, thatis, craniosynostosis, midface hypoplasia, frontal bossing, mandibularprognathism, rhizomelic dwarfing of the limbs, and characteristiccystic lesions of the long bones, mandible, and maxilla. The FGFR1mutation was also detected in our patient and has been reported.8
Given the underlying disorder of bone formation and regulation, itis not unexpected that our patient should have such an aggressiveform of bone tumor.
What is very disturbing about this case is the patient’s level ofunresponsiveness to antiangiogenic therapies. Resistance to antian-giogenic therapy in cancer is postulated to be the result of several fac-tors. Some tumor cells demonstrate an intrinsic resistance toantiangiogenic-induced hypoxia, perhaps due to a mutant p53 gene,and are therefore less affected by hypoxia-inducing therapies.9 An-other mechanism of resistance is the use of existing blood vessels(cooption) by tumors growing in vasculature-rich areas. More im-portantly, VEGF and its regulators seem to have a maximum effect inearly angiogenesis and tumor development. Later angiogenesis isunder the control of additional factors, including basic FGF andplatelet-derived growth factor (PDGF).10 Therefore, a late-stage tumormight escape anti-VEGF therapy by upregulating these additionalfactors in response to antiangiogenic-induced hypoxia. The role of allthese factors in giant cell tumors of bone is still unclear.
Recently, it has been found that monoclonal inhibition of thePDGF receptor results in decreased vascularity and tumor growth ofend-stage tumors.11,12 Newer angiogenetic inhibitors (ie, sorafenib,sunitinib) that target both VEGF and PDGF receptors are associatedwith loss of a previously stable vascular bed. Given their ability totarget angiogenic receptors at various stages of vessel growth, so-rafenib and sunitinib have recently been approved as monotherapyfor renal cancer, and sunitinib has been approved for use in gastro-intestinal stromal tumors. Unfortunately, these agents are availableonly in an oral preparation, precluding their use in our gastrostomy-dependent patient.
For our patient, other antiangiogenic therapies such as thalido-mide might be beneficial. Thalidomide is a powerful teratogen, andin utero limb deformities are now considered to be the result ofthalidomide’s ability to decrease secretion of both VEGF and basicFGF, thereby inhibiting angiogenesis.13 Thalidomide and one of itsnewer structural analogs, lenalidomide, have recently been approvedfor the treatment of multiple myeloma. Thalidomide and especially
FIGURE 3. Sagittal three-dimensional CT reconstruction(December 2008).
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2247

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
lenalidomide have also proved efficacious in the treatment ofmyelodysplastic syndrome. Their use is currently under investiga-tion in the treatment of other solid tumors, including Kaposi sarcomaand malignant melanoma. Therapeutic use of thalidomide and itsderivatives is restricted and requires enrollment in safety programsdesigned to prevent possible teratogenic outcomes. Similar to sora-fenib and sunitinib, thalidomide is available only as an oral pre-paration. Administration of thalidomide to our patient would beparticularly difficult, as thalidomide would have to be crushed forgastrostomy-tube administration, thereby potentially exposingcaregivers of childbearing age to its teratogenic effects.
Giant cell tumors of bone are also rich in RANKL (receptoractivator of nuclear factor JB ligand), which plays a key role in bonedestruction in several diseases that affect bone. Recently, denosu-mab, a fully monoclonal antibody against RANKL, was reported tohave caused responses in 87% of adult patients with unresectableor refractory giant cell tumors.14 Unfortunately, this agent is notavailable to patients in the pediatric age group at this time even on acompassionate basis.
This patient represents the first reported case of a giant cell tumorof the jaw that has not responded to any available treatments. Con-tinued treatment of this patient remains challenging and unprec-edented. Further research needs to be conducted to elucidate themechanisms of giant cell tumor formation in osteoglophonic dwarf-ism that may provide insight for potential therapeutic approaches. Inaddition, understanding current antiangiogenic therapies and theirrole in giant cell tumors will remain critical to the treatment of thiscondition.
REFERENCES
1. Chuong R, Kaban LB, Kozakewich H, et al. Central giant cell lesionsof the jaws: a clinico-pathologic study. J Oral Maxillofac Surg 1986;44:708Y713
2. Kaban LB, Mulliken R, Ezekowitz A, et al. Antiangiogenic therapy ofa recurrent giant cell tumor of the mandible with interferon alfa-2a.Pediatrics 1999;103:1145Y1149
3. Kaban LB, Troulis MJ, Ebb D, et al. Antiangiogenic therapy withinterferon alpha for giant cell lesions of the jaws. J Oral Maxillofac Surg2002;60:1103Y1111
4. Kaban LB, Troulis MJ, Wilkinson MJ, et al. Adjuvant antiangiogenictherapy for giant cell tumors of the jaws. J Oral Maxillofac Surg2007;65:2018Y2023
5. Willett CG, Boucher Y, di Tomaso E, et al. Direct evidence that theVEGF-specific antibody bevacizumab has antivascular effects in humanrectal cancer. Nat Med 2004;10:145Y147
6. Jain RK. Normalization of tumor vasculature: an emerging concept inantiangiogenic therapy. Science 2005;307:58Y62
7. White KE, Cabral JM, Siobhan I, et al. Mutations that causeosteoglophonic dysplasia define novel roles for FGFR1 in boneelongation. Am J Hum Genet 2005;76:361Y367
8. Farrow EG, Davis SI, Mooney SD, et al. Extended mutational analysesof FGFR1 in osteoglophonic dysplasia. Am J Med Genet 2006;140A:537Y539
9. Yu JL, Rak JW, Coomber BL, et al. Effect of p53 status on tumorresponse to antiangiogenic therapy. Science 2002;295:1526Y1528
10. Bergers G, Javaherian K, Lo K, et al. Matrix metalloproteinase-9triggers the angiogenic switch during carcinogenesis. Nat Cell Biol2000;2:737Y744
11. Bergers G, Song S, Meyer-Morse N, et al. Benefits of targeting bothpericytes and endothelial cells in the tumor vasculature with kinaseinhibitors. J Clin Invest 2003;111:1287Y1295
12. Motzer RJ, Michaelson MD, Redman BG, et al. Activity of SU11248, amultitargeted inhibitor of vascular endothelial growth factor receptorand platelet derived growth factor receptor, in patients with metastaticrenal cell carcinoma. J Clin Oncol 2006;24:16Y24
13. D’Amato RJ, Loughnan MS, Flynn E, et al. Thalidomide is an inhibitorof angiogenesis. Proc Natl Acad Sci U S A 1994;91:4082Y4085
14. Thomas D, Chawla SP, Skubitz K, et al. Denosumab treatment of giantcell tumor of bone: interim analysis of an open-label phase II study.J Clin Oncol 2008;26. Abstract 10500
Use of Wide BipedicledPericranial Flap in AnteriorScalp Reconstruction
Semra Karsidag, MD, Arzu Ozcan, MD, Ozay Ozkaya, MD,Kemal Ugurlu, MD, Lutfu Bas, MD
Abstract: Pericranial flap is a composite flap involving the peri-osteum of the skull with its overlying loose areolar tissue termedsubgaleal fascia. The multiple blood supply of the pericranial tissueenables this versatility, with a rich, anastomosing arterial supplyfrom the supraorbital, supratrochlear, superficial temporal, posteriorauricular, and occipital vessels. Thus, the shape, size, and locationof the pericranial flap could be altered as long as a sufficient pedi-cle width could be fashioned to maintain a blood supply. In ourstudy, we have performed wide bipedicled pericranial flap in scalpreconstruction in 2 cases. After tumor excision was completed, apericranial flap was planned on the caudal side of the defect. Abipedicle-based pericranial flap was outlined with the use of asharp dissection; this flap was elevated in a submusculoaponeuroticplane. The bipedicled pericranial flap, whose arterial supply wasfrom the superficial and posterior auricular arteries, was transposedto the frontal defect.
We preferred a bipedicled flap, whose arterial supply is from thesuperficial temporal and posterior auricular arteries to augmentvascular supply. If a large, long pericranial flap is required, makingthe flap pedicled ensures stable blood supply.
KeyWords:Bipedicled pericranial flap, wide defects, stable vascularity
Pericranial flap is a composite flap involving the periosteum of theskull with its overlying loose areolar tissue termed subgaleal
fascia.1 The anatomy of the pericranial flap has been reported byPotparic et al,1 who described subgaleal fascia as several thin con-nective tissue layers that are loosely adherent and glide over oneanother. The multiple blood supply of the pericranial tissue enablesthis versatility, with a rich, anastomosing arterial supply from thesupraorbital, supratrochlear, superficial temporal, posterior auricu-lar, and occipital vessels. Perforating vessels from the supraorbital,supratrochlear, occipital, posterior auricular, and superficial tem-poral arteries have been designed based on 2 different axial patternblood supplies: anteriorly and laterally. The anteriorly based flap issupplied by deep perforating branches of the supraorbital and su-pratrochlear arteries, whereas a laterally based flap is supplied bythe branches of the superficial temporal artery. Thus, the shape,
From the Plastic, Reconstructive and Aesthetic Surgery Clinic, Sisli EtfalTraining and Research Hospital, Istanbul, Turkey.Received June 1, 2009.Accepted for publication June 18, 2009.Address correspondence and reprint requests to Arzu Ozcan, MD, Plastic,
Reconstructive and Esthetic Surgery Department, Sisli Etfal Education andResearch Hospital, Istanbul, Turkey; E-mail: [email protected]
Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181bf871b
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2248 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
size, and location of the pericranial flap can be altered as long as asufficient pedicle width can be fashioned to maintain a bloodsupply.2,3 Takagi et al4 harvested bipedicled pericranial flap, whosearterial supply was based on superficial temporal and occipitalarteries, for dura mater and cranial bone reconstruction. We did notfind in the literature bipedicled pericranial flap designs whose ar-terial supply is based on superficial temporal and posterior auric-ular arteries. In our study, we have performed wide bipedicledpericranial flap in scalp reconstruction in 2 cases. We preferredbipedicled flap whose arterial supply is from the superficial tem-poral and posterior auricular arteries to augment vascular supply.If a large, long pericranial flap is required, making the flap pedicledensures stable blood supply.
MATERIALS AND METHODS
After tumor excision was completed, a pericranial flap was plannedon the caudal side of the defect. A bipedicle-based pericranial flapwas outlined with the use of a sharp dissection; this flap was elevatedin a submusculoaponeurotic plane. The tissues are dissected down tothe pericranium and dissected to expose the desired width and lengthof the pericranial flap while the skin edges are retracted. The desireddimensions of the flap are outlined, and then the flap is cut from the
caudal and cranial sides. The bipedicled pericranial flap, whose ar-terial supply was from the superficial and posterior auricular arteries,was transposed to the frontal defect.
It is important that the pericranial flap does not bear tension;because of this, it is then carefully sutured in place with interruptedsutures.
Patient 1
A 49-year-old male patient has squamous cell carcinoma since 2years on the frontal region, and the lesion has invaded the frontalbone (Fig. 1A). The anterior table of the frontal sinus that has tumorinvasion was outlined and removed using a 2-mm burr. At this point,the sinus mucosa was exenterated. After tumor excision wascompleted, a pericranial flap was planned on the caudal side of thedefect; with the use of a sharp dissection, this flap was elevated in asubmusculoaponeurotic plane. Flap size was 20 � 10 cm (Fig. 1B).The pericranial flap was used to cover the bony defect of the frontalsinus and exposed part of the frontal bone. So that the pericranialflap does not bear tension, it is carefully sutured in place withinterrupted sutures, and then, split-thickness skin graft was adopted(Fig. 1C). Our follow-up period was 10 months, and in this period,we observed that graft intake was complete and frontal depressionwas minimal (Fig. 1D). We did not see wound dehiscence or partialor total flap necrosis.
FIGURE 1. A 49-year-old male patient has squamous cell carcinoma since 2 years on the frontal region (A). After tumor excisionwas completed, a pericranial flap was planned on the caudal side of the defect; with the use of a sharp dissection, this flapwas elevated in a submusculoaponeurotic plane (B). So that the pericranial flap does not bear tension, it is carefully sutured inplace with interrupted sutures, and then, split-thickness skin graft was adopted (C). Graft intake was complete, and frontaldepression was minimal (D).
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2249

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Patient 2
A 52-year-old male patient was admitted to our clinic because ofrecurrent basal cell carcinoma on the frontal region without boneinvasion (Fig. 2A). Once tumor excision was initiated, periostealinvolvement of the tumor was realized, but there was no boneinvasion. After measurement of the defect size was completed,bipedicled pericranial flap was planned from the caudal side of thedefect to cover the exposed bone. Flap size was 5� 10 cm (Fig. 2B).It is carefully sutured in place with interrupted sutures, and then,split-thickness skin graft was adopted (Fig. 2C). Our follow-upperiod was 1 year, and in this period, we observed that graft intakewas complete and frontal depression was minimal (Fig. 2D). We didnot see wound dehiscence or partial or total flap necrosis.
RESULTS
We have performed bipedicled pericranial flap on 2 patients whounderwent tumor surgery. Our mean follow-up time was 11 months.Complete flap failure and full-thickness skin-graft necrosis did notoccur; also, we did not see any wound infection or dehiscence.
Both patients stated complete satisfaction with the results. Nei-ther patient reported tumor recurrence, and both were pleased withthe aesthetic results and the frontal contour.
DISCUSSION
The term pericranium has been used to refer to the skull peri-osteum5,6 or to the composite of the periosteum and overlying
subgaleal fascia. In our study, the periosteum and subgaleal fasciawere included, making the flap more robust and easier to harvestthan a pure subgaleal fascial flap. Pericranial flaps are used by allsurgical specialties that might involve the head and neck. The rangeof applications for which pericranial flaps have been used is asvaried as the specialties that make use of it. Wolfe7 reported the useof a pericranial flap to support rib grafts in cranial reconstruction.Common uses include the reconstruction of skull-base defects,8,9
frontal sinus obliteration,10 and the closure of abnormal commu-nications between the orbit, sinuses, and nasal cavity.11,12
We have used it mainly as a vascularized base for full-thicknessskin grafting where bone has been exposed by excision of tumorsextending to the periosteum. By including both periosteum andsome subgaleal fascia in the flap, it also has some bulk, helping tofill out depressions that may otherwise make the repaired defectdistinct and unsightly compared with the surrounding normaltissues, as would be the case if split-thickness skin grafts were used.This well-vascularized versatile flap is easy to harvest and avoidssecond donor site and its associated morbidity. Also, secondary graftcontracture was minimal because of the rich vascular supply of thebipedicled pericranial flap.
In literature, anteriorly or laterally based pericranial flaps couldbe harvested. In our cases, supraorbital and supratrochlear arterycirculations were broken down with tumor excision. However, thevascular supply of our bipedicled pericranial flap depends on thesuperficial temporal and posterior auricular arteries. Takagi et al4
harvested bipedicled pericranial flap for dura mater reconstruction,but the vascular supply of their flap was based on the branches of thesuperficial temporal and occipital arteries. Our bipedicled flap,whose arterial supply was from superficial temporal and posteriorauricular arteries, differs from their flap by vascular supply.
FIGURE 2. A 52-year-old male patient who has recurrent basal cell carcinoma on the frontal region (A). After measurementof the defect size was completed, bipedicled pericranial flap was planned from the caudal side of the defect to cover theexposed bone (B). It is carefully sutured in place with interrupted sutures, and then, split-thickness skin graft was adopted (C).Follow-up period was 1 year, graft intake was complete, and frontal depression was minimal (D).
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2250 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Furthermore, even in cases such as our cases in which a large, longpericranial flap is required, making the flap bipedicled ensures stableblood supply. In our cases, there was absolutely no problem withblood supply, and the graft took completely. Our experience withthe pericranial flap shows that it is a versatile, robust flap that isrelatively easy to harvest. However, the pericranial flap does not bearthe tension; because of this, it should then be carefully manipulated.This technique could provide good cosmetic results with minimalfrontal depression and nice frontal contour.
REFERENCES
1. Potparic Z, Fukuta K, Colen LB,et al. Galeo-pericranial flaps in theforehead: a study of blood supply and volumes. Br J Plast Surg 1996;49:519Y528
2. Ducic Y, Stone TL. Frontal sinus obliteration using a laterally basedpedicled pericranial flap. Laryngoscope 1999;109:541Y545
3. Thaller SR, Donald P. The use of pericranial flap in frontal sinusfractures. Ann Plast Surg 1994;32:284Y287
4. Takagi M, Kiyokawa K, Sakamoto A,et al. Two-stage reconstructivesurgery of a patient with head trauma resulting in extensive cranial boneand dura mater loss caused by postoperative infection: usefulness ofa pericranial flap for dura mater reconstruction. J Craniofac Surg 2004;17:584Y590
5. Tolhurst DE, Carstens MH, Greco RJ,et al. The surgical anatomy of thescalp. Plast Reconstr Surg 1991;87:603Y612
6. Williams PL, Warwick R, eds. Gray’s anatomy. 36th ed. Edinburgh:Churchill Livingstone, 1980:530
7. Wolfe SA. The utility of pericranial flaps. Ann Plast Surg 1978;1:147Y1538. Argenta LC, Friedman RJ, Dingman RO,et al. The versatility of
pericranial flaps. Plast Reconstr Surg 1985;76:695Y7029. Smith JE, Ducic Y. The versatile extended pericranial flap for closure of
skull base defects. Otolaryngol Head Neck Surg 2004;130:704Y71110. Parhiscar A, Har-El G. Frontal sinus obliteration with the pericranial
flap. Otolaryngol Head Neck Surg 2001;124:304Y30711. Newman J, Constantino P, Moche J. The use of unilateral pericranial
flaps for the closure of difficult medial orbital and upper lateral nasaldefects. Skull Base 2003;13:205Y209
12. Tse DT, Goodwin WJ, Johnson T,et al. Use of galeal or pericranial flapsfor reconstruction of orbital and eyelid defects. Arch Ophthalmol1997;115:932Y937
Nasopharyngeal Encephalocele:Report of Transcranial andTranspalatal Repair With a25-Year Follow-Up
Malcolm A. Lesavoy, MD, Dat T. Nguyen, MD,Gerald Yospur, MD, Brian P. Dickinson, MD
Background: Encephaloceles are an extension or protrusion of anyintracranial matter through a cranial bone defect. The sphenoeth-moidal encephalocele is often fatal. For those who survive long
enough, expeditious repair is critical. We report a case that was re-paired successfully via a combined transcranial and transpalatalapproach, and because of successful repair, the patient underwentmultiple secondary reconstructions resulting in a 25-year follow-up.Clinical Report: A 3960-g, term male infant from a normal ges-tation was delivered via cesarean delivery for breech position. Initialexamination revealed a 2 � 3-cm gray intraoral nasopharyngealmass with smooth mucosal covering extruding through a midlinepalatal cleft. At 4 weeks of life, extradural and intradural explorationof the encephalocele was performed via a bifrontal craniotomy. At15 months of age, the patient underwent median cleft lip repair. At6 years of age, hypertelorism was corrected by wedge resection ofthe frontal and nasal bones and medial mobilization of the orbits.Follow-up was continued until 25 years of age, which revealed ex-cellent maintenance of correction.Conclusion: Sphenoethmoidal encephalocele is a rare sporadiccongenital cranial floor defect associated with typical facial andcerebral anomalies. Encephaloceles extending into the nasopharynxmay cause airway obstruction and feeding difficulty and present apotential pathway for central nervous system infection. Repair of theencephalocele should then be performed as soon as possible. Care ofpatients with nasopharyngeal encephaloceles requires a lifetime ofreconstructive surgery. Care of these patients can be rewarding toboth families and surgeons.
Key Words: Nasopharyngeal encephalocele, transcranial repair,transpalatal repair
Encephaloceles are an extension or protrusion of any intracranialmatter through a cranial bone defect. The defect is usually located
along a cranial suture or at the junction of several bones. Mostcommon locations of the defect are in occipital, orbital, or frontalareas.1,2 They reportedly occur in 1 to 3 of 10,000 live births.3 Theetiology remains unknown, although occasionally they have beenobserved to occur in families whose members have developmentalanomalies of the central nervous system (CNS).3
Encephaloceles are divided into 2 groups according to the loca-tion of involvement: those involving the convexity of the skull andthose involving the base of the skull. The latter represents only 10%to 15% of all encephaloceles.4 The sphenoethmoidal encephaloceleis of the basal group. It has been described as protruding into thenasal cavity through a defect in the sphenoid and ethmoid bones andextending farther into the nasopharynx via a palatal cleft.4 Such anasopharyngeal encephalocele may cause airway obstruction andalso represents a potential pathway for infection of the CNS. Inaddition, vital brain structures may be damaged if not reduced intothe cranium. For those who survive long enough, expeditious repairis critical. Of the few cases reported, repair has been described via atranscranial or combined transoral/transpalatal approach. Becausethe transcranial repair has been reported with a low success rate andmortality rate of 50%, some surgeons have advocated the latterapproach.5 We report a case that was repaired successfully via acombined transcranial and transpalatal approach. Furthermore,because of his successful repair, the patient underwent multiplesecondary reconstructions resulting in a 25-year follow-up.
CLINICAL REPORT
A 3960-g, term male infant, from a normal gestation, was deliveredvia cesarean delivery for breech position. Initial examination re-vealed a 2 � 3-cm gray intraoral nasopharyngeal mass with smooth
From the Division of Plastic & Reconstructive Surgery, UCLA School ofMedicine, Los Angeles, California.Received June 2, 2009.Accepted for publication June 19, 2009.Address correspondence and reprint requests to Malcolm A. Lesavoy, MD,
Plastic and Reconstructive Surgery, UCLA School of Medicine,16311 Ventura Blvd, Suite 550, Encino CA 91426-4314;E-mail: [email protected]
Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181bfc3a7
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2251

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
mucosal covering extruding through a midline palatal cleft. Thismass was compressible and easily reducible into the cleft. Markedhypertelorism, a bifid nose, and a midline BO[ cleft lip were alsopresent. The rest of the physical examination was unremarkable.
Skull radiographs showed a midline defect of the ethmoid andsphenoid bones with absence of the cribriform plate, medial portionof anterior fossa floor, planum, and tuberculum. The sphenoid, sellaturcica, and anterior and posterior clinoids were present. In addition,the computed tomography (CT) scan showed a soft tissue densitymass in the nasopharynx, absence of the corpus callosum, and dila-tion of the posterior horns of the lateral ventricles (Fig. 1). Theelectroencephalogram and results of laboratory tests did not showabnormalities.
Hospital Course and Subsequent Treatments
Initially, the infant’s feeding was impaired because of the mass andpalatal defect, and a feeding tube was placed. On the 14th day, theinfant was found to have evidence of diabetes insipidus and adecreased level of serum adrenocorticotropic hormone. The patientwas treated with vasopressin (Pitressin) and dextrose 5% in water.Twenty-four days after his birth, the patient developed respiratorydistress secondary to airway obstruction by the nasopharyngealmass. Emergent tracheostomy was performed.
At 4 weeks, extradural and intradural exploration of the encepha-locele was performed via a bifrontal craniotomy. Intraoperatively, theencephalocele was found to be composed of a cystic cavity withcopious, glistening, tough dysplastic tissue. Ninety percent of this
tissue was removed. The inferior aspect of the encephalocele sac waslacking a dura mater and was thus essentially composed of arachnoidmembrane and nasopharyngeal mucosa. The medial anterior cranialfloor defect, extending from the ethmoidal to an area of anterior toposterior clinoid processes, was repaired with a bone graft from thebifrontal craniotomy. A dural graft was also required. Postopera-tively, a cerebrospinal fluid leak was noted with subsequentdevelopment of Pseudomonas meningitis. Antibiotics were intrave-nously administered. At 6 weeks, a progressive nasopharyngealswelling at the site of the repaired encephalocele was noted. Thepatient was found to have hydrocephalus by CT scan, and a ven-triculoperitoneal shunt was placed. A follow-up CT scan showeddiffuse air in the ventricular system with an air track between thenasopharynx and the apex of the frontal horn. At 10 weeks, it wasnoted that the repair had ruptured secondary to the developmentof hydrocephalus, and extradural and intradural exploration of therepaired anterior cranial floor was undertaken. A fistulous defectwas found in the floor, which was repaired with cranial bone graft
FIGURE 2. Patient at 15 months of age with median cleft lip.
FIGURE 3. Intraoperative markings for median cleft lip repairat 15 months of age.
FIGURE 4. Postoperative photograph at 4 years after mediancleft lip repair.
FIGURE 1. CT scan of the head showing midline defect.
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2252 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
sandwiched between 2 sheets of lyophilized dura mater (Lyodura,Braun Melsungen AG, Marburg, Germany). In addition, transposi-tion of a palatal mucosal flap (a right Millard island flap) was used tocover the inferior surface of the floor defect from the mouth. The hy-drocephalus, pneumocephalus, and meningitis subsequently resolved,and the patient was discharged home at 13 weeks on DDAVP (1-deamino-5-d-arginine vasopressin) and hydrocortisone.
On subsequent follow-up, the patient was found to havedeficiencies of growth hormone and thyroid function and thereforewas administered growth hormone and levothyroxine (Synthroid). Afrontal epidural abscess that communicated with the nasopharynxwas drained and treated with intravenously administered antibiotics.The fistula spontaneously closed with the resolution of abscess.
At 10 months of age, the patient had stabilized from his priorsurgeries and began to gain weight appropriately but remained with
his unrepaired median cleft lip and palate (Fig. 2). At 15 monthsof age, the patient underwent median cleft lip repair by makingcorresponding markings from each oral commissure to the highpoints of the Cupid’s bow. An inverted BV[ design was traced onthe lip from the apex of the cleft that lies at the base of the columellato 2 corresponding points 3 mm medial to the high points of theCupid’s bow. A 90-degree angle in the marking for excision wasmade approximately 3 mm above the mucocutaneous white roll oneach side of the cleft, to give vertical length to the repaired lip andprovide fullness of the vermillion in the midline tubercle (Fig. 3).
The patient was followed up at 4 years of age, which revealedan excellent result of the median cleft lip repair. The patienthad persistent hypertelorism (Fig. 4) and nasomaxillary hypoplasia(Fig. 5). At 6 years of age, the hypertelorism was corrected by wedgeresection of the frontal and nasal bones and medial mobilization ofthe orbits. A preoperative photograph depicts the severity of thehypertelorism that progressed at age 6 years (Fig. 6). Intra-operatively, the medial interorbital distance measured 38 mm aswell as a large nasal defect at the site of the repaired encephalocele(Figs. 7 and 8). Rib grafts were obtained, and the remaining nasalbones were used as a composite cantilever graft to reconstruct thenose after 12 mm was resected from the frontal and nasal bones
FIGURE 6. Intraoperative on table photograph showing thesevere hypertelorism.
FIGURE 7. With the periorbita retracted, the nasal defect canbe seen from the prior nasopharyngeal encephalocele.
FIGURE 8. Intraoperative photograph after coronal incisionand release of the periorbita showing an interorbital distanceof 38 mm.
FIGURE 5. Lateral photograph at 4 years of age showing thesevere nasomaxillary hypoplasia secondary to the wide cleftpalate and nasopharyngeal encephalocele.
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2253

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
(Figs. 9 and 10). The frontal cranial defect was also reconstructedwith multiple split rib grafts (Figs. 11 and 12). The hard and softpalates were not repaired but were obdurated by a prosthesis.Photographs obtained at 4 months postoperatively revealed excellentcorrection of the orbital hypertelorism as well as an augmented nasalradix and dorsum (Fig. 13). Hospitalization occurred at 12.5 yearsfor hydrocephalus secondary to malfunction of the ventriculoper-itoneal shunt. The shunt was revised, and the patient was dischargedhome without further complication.
Growth and Development
At 4 months of age, the patient was noted to have a problemwith his vision and hearing and was developmentally delayed. Hisweight and height were both below the fifth percentile. Laboratorydata indicated hypopituitarism. At the age of 3 years, his weightand height continued to be below the fifth percentile. Examinationof the eyes showed slight amblyopia in the left eye with a constantnystagmus and a disconjugate gaze. Audiometry showed a responseat 80 dB. Sound field responses were similar to those of a youngerchild with low-normal responses through speech range. At 8 yearsof age, his weight and height were only at 50% of children 4.5 yearsof age. Despite the continuation of growth stunting, his mental
development was comparable to that of children at his age. By12 years of age, he attended seventh grade and was reported to bea good student. Follow-up at 13 years old revealed maintenance ofthe nasal dorsum correction, with the beginning of recurrence ofthe orbital hypertelorism associated with a growth spurt (Fig. 14);however, he remained relatively underdeveloped secondary to thehypopituitarism. At 25 years of age, the patient returned for follow-up visit (Figs. 15 and 16). Photographs were obtained and revealedmaintenance of the nasal dorsum and correction of the hypertel-orism. There were a moderate orbital dystopia and persistent naso-maxillary hypoplasia likely secondary to the prior encephaloceleand use of the Millard rotational flap to close the intracranial defect.The patient and his mother were extremely satisfied with thereconstruction.
DISCUSSION
As illustrated in our case, these rare patients with a sphenoethmoi-dal encephalocele are associated with the following facial andcerebral deformities: hypertelorism, bifid nose, cleft lip, cleft palate,and partial or complete agenesis of the corpus callosum. Depend-ing on whether the pituitary was involved, the patient may presentwith evidence of hypopituitarism. The patient may also have visual
FIGURE 10. The resected nasal bones are removed andthen used in conjunction with the cantilever bone graft toaugment the nasal radix.
FIGURE 11. Rib graft was harvested and used to reconstructthe calvaria as well as augment the radix as a cantileverbone graft.
FIGURE 12. Intraoperative photograph showing thecantilever nasal bone graft and slit rib grafts to reconstructthe calvaria.
FIGURE 9. The amount of nasal bones to be resected ismarked in ink (12 mm).
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2254 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
problems due to optic nerve atrophy.3Y6 Therefore, in addition tophysical examination, patients should have a complete radiologicalstudy of the head (skull film and head CT), an evaluation ofendocrine function, and an ophthalmologic evaluation.
Patients frequently present with feeding difficulties and evidenceof airway obstruction due to the presence of the encephalocele in thenasopharynx. In addition, its presence also creates a potential path-way for CNS infection. For these reasons, reduction of the en-cephalocele and repair of the cranial floor should be undertaken assoon as possible.
Mortality due to bacterial meningitis is relatively high, especiallyfor neonates (between 25% and 50%).7 Because of this fact, trans-cranial repair of a nasopharyngeal encephalocele has been the rec-ommended approach. However, transoral and transpalatal repairunder an antibiotic umbrella has been advocated because it allowsfor easy manipulation and reduction of the encephalocele withoutdisrupting vital structures within the encephalocele.5 As seen in our
case, the bases of the encephalocele were found to be without dura.No dura can be detached from the nasal mucosa for the reduction ofthe encephalocele. Intradural and subdural structures would havebeen contaminated with naso-oral flora, and the risk of infectionwould have been increased if a transpalatal approach was used. Inaddition, to repair the cranial floor and dural defects in thesepatients, either an autologous or alloplastic graft would be required.By introducing the graft via a naso-oral route, the risk for con-tamination would increase the risk of postoperative infection.
Transpalatal repair has been reported to be associated with lessincidence of hypopituitarism because it avoids resection of cerebralstructures within the encephalocele.5 However, often these patientswith nasopharyngeal encephalocele already have panhypopituita-rism and risking infection for a transpalatal approach would not beprudent in these patients.
Because anterior cerebral arteries have been found to deflectinferiorly into the encephalocele,4 prior study of intracephalocelecontent is wise to prevent vascular injury and subsequent brainischemia. These patients with nasopharyngeal encephaloceles haveimmediate life-threatening medical and surgical emergencies asso-ciated with airway compromise and endocrine dysfunction. However,
FIGURE 14. Patient at 13 years of age at onset of growthspurt. Note the overall lack of signs of pubertal developmentsecondary to the hypopituitarism. At 13 years of age, the radixgraft persisted, but there began to be an increase in theintraorbital distance.
FIGURE 15. Patient at 25 years of age. Anteroposterior view.
FIGURE 16. Patient at 25 years of age. Profile view.
FIGURE 13. Patient at 6 years of age 4months postoperativelyat a bird s-eye view showing augmentation of the nasaldorsum and correction of the orbital hypertelorism.
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2255

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
once they have stabilized from these reconstructive procedures, theresulting craniofacial deformities secondary to the mass effect needto be corrected. These sequential procedures require correction oforbital hypertelorism, and the maxilla is hypoplastic resulting inAngle class III malocclusion. However, as in this case, a Millardpalatal island flap was used to prevent intracranial and nasal commu-nication, and no tissue was left to reconstruct the large palatal defect.
CONCLUSIONS
Sphenoethmoidal encephalocele is a rare sporadic congenital cranialfloor defect associated with typical facial and cerebral anomalies.Encephaloceles extending into the nasopharynx may cause airwayobstruction and feeding difficulty and present a potential pathwayfor CNS infection. Complete evaluation should include radiologicalstudies of the head and endocrine studies for determination of pitui-tary functions. Repair of the encephalocele should then be performedas soon as possible. Although transpalatal repair offers less risk ofdeveloping postoperative hypopituitarism, its approach puts patientsat higher risk for postoperative CNS infection. However, it seems thatthe pathological anatomy usually will dictate a combined approach.Care of patients with nasopharyngeal encephaloceles requires a life-time of reconstructive surgery. Care of these patients can be reward-ing to both families and surgeons.
REFERENCES
1. Matson DD. Neurosurgery in Infancy and Childhood. Springfield, IL:Charles C. Thomas, 1969:61Y75
2. Blumenfeld R, Shnolnik EM. Intranasal encephaloceles. ArchOtolaryngol 1965;82:527Y531
3. George TN. Cephalocele. Laryngoscope 1987;97:77Y844. Modesti LM, Glasaver FE, Terplan KL. Sphenoethmoidal
encephalocele. A case report with view of the literature. Childs Brain1977;3:140Y153
5. Lewin LM. Sphenoethmoidal cephalocele with cleft palate: trans-palatalversus transcranial repair. Report of two cases. J Neurosurg 1983;58:924Y931
6. Kenna MA. Transphenoidal encephalocele. X-ray study of the month.Ann Otol Rhinol Laryngol 1985;94:520Y522
7. Fortum HM. Epidemiology of bacterial meningitis. Arch Dis Child1993;68:763Y767
Desmoplastic AmeloblastomaBelir Atalay, DDS, PhD,* Merva Soluk, DDS, PhD,yAmila Brki(, DDS,* Yusuf Emes, DDS, PhD,*Ozge Cetin, DDS,* Vakur Olgac, DDS, PhDy
Abstract: Ameloblastoma is a rare benign odontogenic epithelialtumor characterized by abnormal cell growth, which easily infil-
trates and destroys surrounding bony tissues. Clinically, it is mostlyseen in the ascending ramus area, in men in their fourth and fifthdecades more frequently than in women. One of the 3 clinicalvariants of ameloblastoma is desmoplastic type, with involvement ofthe maxillary arch more often than the mandible. Its histopathologicvariant characterized by extensive squamous metaplasia, islandsof tumor cells, and sometimes keratin formation is known as des-moplastic acanthomatous ameloblastoma.
The aim of this report was to present an unusual case ofsymphysis located desmoplastic acanthomatous ameloblastoma ina 56-year-old female patient, who was experiencing laryngeal car-cinoma 2 years ago.
Key Words: Ameloblastoma, desmoplastic acanthomatousameloblastoma, symphysis mandible, radiolucency
Ameloblastoma represents 11% of all odontogenic tumors andoriginates from the epithelium, which is involved in the for-
mation of teeth.1 Potential epithelial sources include enamel organ,odontogenic rests, reduced enamel epithelium, and the epitheliallining of odontogenic, especially dentigerous cysts. The trigger orstimulus for neoplastic transformation of the previously mentionedepithelial sources is totally unknown.2 If the unicystic type is formedfrom the epithelial lining of a dentigerous cyst, it is called a muralameloblastoma.1 Ameloblastomas with a slight predilection occurin men and develop more often in black Africans.1 Localizations ofameloblastomas are mostly seen (80%) in the molar-ramus region ofthe mandible; however, they may develop in the symphyseal area.1,2
In the maxilla, the molar area is more commonly affected than theanterior or premolar area.2 Although the ameloblastoma is mostly anintraosseous tumor, there are cases of the so-called extraosseousperipheral ameloblastomas found in the gingiva or buccal or palatalmucosa.1Y5 These peripheral forms of ameloblastomas compriseapproximately 1% of all ameloblastomas.5 The ameloblastomaoccurs predominantly in the fourth and fifth decades (35Y45 y),1,2
although it may be found in young (age, 3 y) people and in indi-viduals older than 80 years.1 Recurrence rates are higher in olderpatients and in those with multilocular lesions. Local recurrence,whether detected radiographically or histologically, may have a moreaggressive character than the original tumor.1 There is a pronouncedtendency for ameloblastomas to cause extensive root resorptionand tooth displacement. The stroma of the ameloblastoma usuallyconsists of relatively acellular loose connective tissue. Sometimes,it is more collagenous and may be frankly desmoplastic with smallnests and strands of odontogenic epithelium. This has been de-scribed as desmoplastic ameloblastoma.6 Desmoplastic ameloblas-toma was first described by Eversole et al in 1984.7 Accordingto the World Health Organization’s histopathological typing ofodontogenic tumors, desmoplastic ameloblastoma is a benign andlocal invasive jaw tumor, which represents approximately 4% to13% of all ameloblastomas, with involvement of the maxillary archmore often than the mandible.6Y12 The term acanthomatous is usedwith cases where there is extensive squamous metaplasia, sometimeswith keratin formation, within the islands of tumor cells. The generalpattern of the tumor is that of the follicular type. This variety mustbe distinguished from the squamous odontogenic tumor, in whichthe peripheral cells are flat rather than columnar.6
CLINICAL REPORT
In December 2008, a 56-year-old female patient referred to theDepartment of Oral and Maxillofacial Surgery, Istanbul University,
From the *Department of Oral and Maxillofacial Surgery, and yInstitute ofOncology, Istanbul University Capa, Istanbul, Turkey.Received May 26, 2009.Accepted for publication July 2, 2009.Address correspondence and reprint requests to Belir Atalay, DDS, PhD,
Department of Oral and Maxillofacial Surgery, Faculty of Dentistry,Istanbul University, 34390 Capa, Istanbul, Turkey; E-mail: [email protected]
The third coauthor of this paper was a fellow of the TUBITAK(The Scientific and Technological Research Council of Turkey),during her PhD education in Istanbul University.
Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181bfc537
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2256 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
with a complaint of swelling in the region of anterior mandible,which was present for 2 years. Clinical intraoral examinations dis-closed a very bad oral hygiene with periodontal disease, remnantsof the teeth roots, and caries lesions of the most teeth. In the anteriorpart of the mandible from the vestibule side, a swelling was noticed,which was of soft consistency. The surface was smooth, and thecolor was similar with the adjacent mucosa. With appliance ofpressure, white exudate was flowed from the fistula. There were nosymptoms of pain or paresthesia. Teeth 41, 42, 43, 44, 45, 31, 32,33, 34, and 36 associated with the lesion were nonvital. Extraoralexaminations revealed a presence of asymmetry at the left side ofthe mandible, and the presence of lymphadenopathy at the leftsubmandibular region was noted too. A laryngostoma was present,and the patient could not speak.
The radiographic examinations have revealed a large well-circumscribed radiolucent lesion that was 8 cm in diameter, locatedbetween the first right premolar and second left molar teeth, whichwas radiologically suspicious to be a radicular cyst (Fig. 1). Thelower edge of the lesion was the inferior border of the mandible,whereas the upper edge in the left premolar region was in the levelof oral mucosa and cervix of the lower left canine and the first pre-molar teeth.
From the patient’s health history, it was learned that she hadexperienced laryngeal carcinoma. In the period between November2003 to May 2005, the patient had undergone 3 different surgicalprocedures, which resulted to complete laryngectomy and anteriorlymph node dissection. Having consulted the patient’s specialist ofoncology, it was found out that the patient had a squamous cellcarcinoma of the larynx, which was treated just operatively becauseradiotherapy and chemotherapy were refused by the patient herself.Four months after the first operation (March 2004), the second onewas performed, which resulted to complete laryngectomy and lymphnode dissection as the consequence of tumor metastasis. In May2005, a permanent laryngostoma was embedded. The patient wasunder follow-up for 4 years without any complaints and complica-tions. Taking to consideration the general health condition of thepatient, there were no contraindications to surgical interventionunder local anesthesia because the surgery under general anesthesiawas refused by the patient.
Before surgery, the patient underwent an endodontic treatment ofteeth 41, 42, 43, 44, 45, 31, 32, 33, 34, and 36, which were involvedin the cystic lesion. Under local anesthesia, a full mucoperiosteal,sulcular incision was made from the lower right first molar to the left
FIGURE 1. Panoramic radiographs revealed a largewell-circumscribed radiolucent formation suspicious to be aradicular cyst.
FIGURE 2. Pathologic specimen after fixation with10% formaldehyde.
FIGURE 3. Control panoramic radiograph taken6 months postoperatively.
FIGURE 4. Tumoral masses surrounded by ameloblasticcells are observed (thin black arrows). These cells are in aconnective tissue with dense collagen fibers (thick blackarrows). There is also squamous epithelial metaplasia seenat the middle of the quasi-stellar cells (white thick arrows;hematoxylin and eosin [H&E], original magnification �200).
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2257

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
second molar. The mucoperiosteal flap was reflected into the fornix.At the beginning of operation, apicotomy with cyst enucleation wasplanned. However, during the curettage of the pathologic mass, theapiectomy was abandoned because there was no bone around theroots of the teeth. Therefore, the 31, 32, 33, 34, 35, 36, 41, 42, 43,and 47 teeth were extracted. The pathologic specimen was submittedto the Department of Oncologic Cytology and Tumor Pathology,Istanbul University, as the infected radicular cyst (Fig. 2). The flapwas placed in its original position and sutured. After 8 days, thewound healed, and the sutures were removed. The patient reporteda sense of numbness in the region of the lower lip and chin fromthe left side, which started a day after the surgery. The patient isfollowed up for 6 months, and there was no sign of infection orrecidivation observed until now (Fig. 3).
According to histopathologic examinations, the lesion was di-agnosed as acanthomatous desmoplastic ameloblastoma (Figs. 4Y6).
DISCUSSION
Ameloblastoma is the second most common odontogenic tumor,which originates from the epithelial components of the tooth-forming apparatus. The stimulus for the neoplastic transformation ofthese tissues is not known yet.6,7,13
Eversole et al7 first described desmoplastic ameloblastoma in1984, and their studies were later reviewed byWaldron and el-Mofty10
in 1987. These reports indicated that this type of ameloblastomahas many features that are inconsistent with conventional amelo-blastoma. There is a dense fibrous connective tissue around the tumorisland, a comparatively unusual location from other ameloblastomas,and a radiographic appearance that is similar to a benign fibroos-seous lesion, which could be due to the infiltrative and osteoblasticbehaviors of this tumor.6,13 Clinically, patients with typical amelo-blastoma do not have significant initial complaints; however, in thecases of desmoplastic ameloblastoma, there are possibilities ofinitial pain.14
If the central portions of the tumor islands became squamoid orelongated, the terms acanthomatous and spindle are used to modifyameloblastomas. In our case, it was identified histopathologically:
tumoral masses between high density of collagen fibers at the con-nective tissue.
Gortzak et al15 indicate that with large ameloblastomas in whichthe cortical bone has enlarged expansively, the periosteal tissue isinvolved but not perforated by the tumor. Moreover, it is found thatno matter how enlarged the ameloblastoma is, the skin tissue isnot involved, owing to the skin’s superior regenerative capacitycompared with the ameloblastoma’s growth rate. In our case, anapparent swelling in the anterior region of the mandible was ob-served, with no inclusion of the cortical bone and the periostealtissue whatever.
The teeth that are adjacent to the ameloblastoma and that arewithin the safety parameters of the resection have the indication forextraction. Leaving such teeth conservatively is a risk factor of arecurrence.16 Although ameloblastomas are defined as benignneoplasms, they are locally destructive and have a high rate ofrecurrence if they are not entirely excised.17Y19 While planning thetreatment of ameloblastoma, besides patient age and complaints,factors such as tumor anatomic localization, size, and radiographicproperties should be taken into notice. Observed recurrences aremostly a result of insufficient or failed surgical operations.20
Reichart et al21 indicate that mean age at first diagnosis for am-eloblastoma is 35.9 years and the duration of the symptoms untilthe diagnosis is 2 to 3 years. Clinically, ameloblastomas are mostlyseen in the fourth and fifth decades. Because of its slow growingrate, their development is probably initiated in childhood.19 In ourpresented case, the patient was above these mean values. She was atthe age of 56 years when ameloblastoma was diagnosed.
According to recent reviews, in most desmoplastic ameloblas-tomas, there were no typical radiographic features of ameloblas-toma.22,23 In many cases, the ameloblastoma showed a mixedradiolucent/radiopaque appearance with ill-defined margins. Thecases in Kishino et al23 were difficult to diagnose correctly andlacked typical findings for ameloblastoma. The findings resembledodontogenic cysts, fibroosseous lesions and odontogenic mixo-mas. 22,23 Because we observed a lesion with well-defined margins,our preoperative diagnostics were toward a radicular cyst.
In the previous reports, desmoplastic ameloblastoma has a higherrate of occurrence in the anterior region of jaws.10,12,22 In our case,
FIGURE 5. Tumoral masses surrounded by ameloblasticcells are observed (thin black arrows). These cells are in aconnective tissue with dense collagen fibers (thick blackarrows). There is also squamous epithelial metaplasia was seenat the middle of the quasi stellar cells (white thick arrows;[H&E], original magnification �200).
FIGURE 6. Tumoral masses surrounded by ameloblasticcells are observed (thin black arrows). These cells are in aconnective tissue with dense collagen fibers (thick blackarrows). There is also squamous epithelial metaplasia wasseen at the middle of the quasi stellar cells (white thickarrows; H&E, original magnification �400).
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2258 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
desmoplastic acanthomatous ameloblastoma was also located in theanterior mandible. Our case also showed this predilection for theanterior jaw.
REFERENCES
1. White SC, Pharoah MJ, eds. Oral Radiology Principles andInterpretation. 6th edn. St Louis: Mosby Elsevier; chapter 22,part V, 2009:373
2. Regezi JA, Sciubba J, eds. Oral Pathology: Clinical-PathologicCorrelations. 2nd edn. Philadelphia: WB Saunders Company;chapter 11, 1993:363Y374
3. Vanoven BJ, Parker NP, Petruzzelli GJ. Peripheral ameloblastoma ofthe maxilla: a case report and literature review. Am J Otolaryngol2008;29:357Y360
4. Smullin SE, Faquin W, Susarla SM, et al. Peripheral desmoplasticameloblastoma: report of a case and literature review. Oral SurgOral Med Oral Pathol Oral Radiol Endod 2008;105:37Y40
5. Pekiner FN, Ozbayrak S, Sener BC, et al. Peripheral ameloblastoma:a case report. Dentomaxillofac Radiol. 2007;36:183Y186
6. Barnes L, Eveson JW, Reichart P, et al. World Health Organization,Classification of Tumours Pathology and Genetics of Headand Neck Tumours. Lyon: ARC Pres; 2005:296Y300
7. Eversole LR, Leider AS, Hansen LS. Ameloblastomas withpronounced desmoplasia. J Oral Maxillofac Surg 1984;42:735Y740
8. Kaffe I, Buchner A, Taicher S. Radiologic features desmoplasticvariant of ameloblastoma. Oral Surg Oral Med Oral Pathol1993;76:525Y529
9. Philipsen HP, Reichart PA, Nikai H, et al. Peripheral ameloblastoma:biological profile based on 160 cases from the literature. OralOncol 2001;37:17Y27
10. Waldron CA, el-Mofty SK. A histopathologic study of 116ameloblastomas with special reference to the desmoplasticvariant. Oral Surg Oral Med Oral Pathol 1987;63:441Y451
11. Kramer IR, Pindborg JJ, Shear M. The World Health Organizationhistological typing of odontogenic tumours. Introducing the secondedition. Eur J Cancer B Oral Oncol 1993;29B:169Y171
12. Philipsen HP, Reichart PA, Takata T. Desmoplastic ameloblastoma(including Bhybrid[ lesion of ameloblastoma). Biological profilebased on 100 cases from the literature and own files. OralOncol 2001;37:455Y460
13. Sakashita H, Miyata M, Okabe K, et al. Desmoplastic ameloblastomain the maxilla: a case report. J Oral Maxillofac Surg 1998;56:783Y786
14. Rapidis AD, Andressakis DD, Stavrianos SD, et al. Ameloblastomasof the jaws: clinicopathological review of 11 patients. Europ JSurg Oncol 2004;30:998Y1002
15. Gortzak RA, Latief BS, Lekkas C, et al. Growth characteristics oflarge mandibular ameloblastomas; report of 5 cases with implicationsfor the approach to surgery. Int J Oral Maxillofacial Surg 2006;35:691Y695
16. Torres-Lagares D, Infante-Cossio P, Hernandez-Guisado JM, et al.Mandibular ameloblastoma. A review of the literature andpresentation of six cases. Med Oral Patol Oral Cir Bucal2005;10:231Y238
17. Eversole LR, Wysocki GW, Sapp P, eds. Contemporary Oral andMaxillofacial Pathology. St Louis: Mosby; 2004:135Y143
18. Miyake T, Tanaka Y, Kato K, et al. Gene mutation analysis andimmunohistochemical study of B-catenin in odontogenic tumors.Pathol Int 2006;56:732Y737
19. Huang IY, Lai ST, Chen CH, et al. Surgical management ofameloblastoma in children. Oral Surg Oral Med Oral PatholOral Radiol Endod 2007;104:478Y485
20. Al-Khateeb T, Ababneh KT. Ameloblastoma in young Jordanians:a review of the clinicopathologic features and treatment of 10 cases.J Oral Maxillofac Surg 2003;61:13Y18
21. Reichart PA, Philipsen HP, Sonner S. Ameloblastoma: biologicalprofile of 3677 cases. Eur J Cancer B Oral Oncol 1995;31B:86Y99
22. Beckley ML, Farhood V, Helfend LK, et al. Desmoplastic
ameloblastomas of the mandible: a case report and review of literature.J Oral Maxillofac Surg 2002;60:194Y198
23. Kishino M, Murakami S, Fukuda Y, et al. Pathology of the desmoplasticameloblastoma. J Oral Pathol Med 2001;30:35Y40
Comparison of the Soft TissueThickness of the Midface inCraniosynostosis
Dong Won Lee, MD, Dong Kyun Rah, MD,Be-young Yun Park, MD, Yong Oock Kim, MD, PhD
Abstract: Craniosynostosis is classified according to the includedsutures as either symmetric, such as scaphocephaly and brachy-cephaly, or asymmetric, such as plagiocephaly. Asymmetric cra-niosynostosis has been known to exert asymmetric effects not onlyon the cranium but also on the facial skeleton. Nonetheless, thepresence of asymmetry in soft tissues is only speculative and isbased on the experience of plastic surgeons. In our study, aftermeasuring the surface coordinates of soft and bone tissues fromnumerous positions on three-dimensional computed tomography(CT), the distance between the coordinates was calculated andthe thickness of the soft tissues was obtained by objective mea-surements. The subjects included a control group of 8 symmetriccraniosynostosis patients, and the study group consisted of 7asymmetric craniosynostosis patients selected by computed tomo-graphic data. In each patient, the thickness of the midfacial areawas measured by dividing it into frontal and lateral views. Theresults show that in symmetric craniosynostosis, the thicknessesof the right and the left soft tissues were statistically identical.However, in asymmetric craniosynostosis, the thickness of soft tis-sues in the hypoplastic side was statistically significantly thin ac-cording to measurements taken at both the frontal and the lateralviews (P = 0.048 and P = 0.034, respectively). This suggests thatsurgeons should pay attention to the asymmetry of soft tissuesduring follow-up and when correcting facial asymmetry in asym-metric craniosynostosis.
Key Words: Craniosynostosis, soft tissue thickness, three-dimensionalcomputed tomography
C raniosynostosis has different appearances depending on thelocation or number of synostosed suture lines, and it affects
not only the cranium but also the midfacial area.1Y3 According to
From the Department of Plastic and Reconstructive Surgery, Yonsei Univer-sity Health System, Severance Hospital, Seoul, Republic of Korea.Received June 23, 2009.Accepted for publication July 12, 2009.Address correspondence and reprint requests to Dr Yong Oock Kim,
Department of Plastic and Reconstructive Surgery, Yonsei UniversityHealth System, Severance Hospital, 134 Shinchon-dong, Seodaemun-gu,120-752 Seoul, Republic of Korea; E-mail: [email protected]
This study was supported by a grant (No. A080432) from the KoreaHealth 21 R&D Project, Ministry of Health and Welfare, Republic ofKorea, and a faculty research grant of Yonsei University College ofMedicine for 6-2005-0046.
Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181bfc556
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2259

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
the included sutures, morphologic changes are shown as symmet-ric or asymmetric craniofacial skeletons. Particularly, plagioceph-aly, which is caused by early closure of the unilambdoid or theunicoronal suture, induces asymmetry of not only the cranium butalso the facial area.4Y6 Such asymmetry represents all of the changesin the bone and the soft tissues. Nonetheless, asymmetry of the softtissues has not been reported as the causative factor of asymmetry ofthe facial area, but asymmetry of bone tissues has been reportedas such.4,5 This is considered to be due to the methods to mea-sure asymmetry of soft tissues that effectively do not exist. In our
study, the thickness of facial soft tissues was obtained by three-dimensionally reconstructing the images from computed tomog-raphic (CT) scans, by measuring the coordinates on the surface ofthe skin and the surface of the bone tissues of the facial area fromthe predetermined same points, and by calculating the distancebetween the 2 coordinates. In addition, by comparing the thicknesseson the right and the left sides, the role of the soft tissues in theasymmetry of the midface in plagiocephaly was examined.
MATERIALS AND METHODSMaterials
The craniofacial CT scans of 15 patients with a diagnosis of non-syndromic craniosynostosis were reconstructed as three-dimensionalCT images using the Analyze AVW 5.0 (AnalyzeDirect, OverlandPark, KS). The age range was 2 to 58 months, and 10 patients wereboys, and 5 were girls. Among 15 patients, 8 had symmetric cra-niosynostosis (4 with sagittal craniosynostosis, 3 with bicoronalcraniosynostosis, and 1 with metopic craniosynostosis) and 7 hadasymmetric craniosynostosis (6 with unicoronal craniosynostosisand 1 unilambdoid craniosynostosis). Measurements were obtainedfrom the symmetric craniosynostosis patients as the control groupfor comparison with those from the asymmetric craniosynostosispatients.
Methods
Axial and noncontiguous CT scans were obtained from the mentumto the vertex at 2-mm intervals. Three-dimensional reconstruction
FIGURE 1. Frontal view of the reconstructedthree-dimensional images. A, Bone tissue accentuatedimage. B, Soft tissue accentuated image.
FIGURE 2. Lateral view of the reconstructed three-dimensional images. Right (A) and left bone tissue accentuated images (B).Right (C) and left soft tissue accentuated images (D).
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2260 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
was performed using the Analyze AVW 5.0 software, and the pixelsize was 0.5 mm. The reconstructed three-dimensional CT scan wasrealigned while the horizontal plane passed through the nasion andboth porions, and the vertical plane formed a perpendicular anglewith the horizontal plane and passed through the nasion and thebasion.7 From the realigned three-dimensional CT scan, 2 types ofbone tissue and soft tissue images were prepared while the densitythreshold controls. Subsequently, in the frontal and both lateralviews of the soft tissue images, the x coordinates dividing the spacebetween the right and the left tangent line to 4 equal parts and they coordinates dividing the space between the highest and lowesttangent line to 9 equal parts were obtained. Based on the cross pointsof the x and y axes, x and y coordinates could be determined fromthe (x, y, z) coordinates. From the soft tissue images on the corre-sponding (x, y) coordinates, z coordinates were obtained, and sim-ilarly, the z coordinates of the bone tissue images were obtained;thus, the three-dimensional coordinates of the surface soft and thebone tissues of the same cross points were obtained. By calculat-ing the distance between the soft and the bone tissue coordinatesand applying the formula d = ¾(x1 j x2)
2 + (y1 j y2)2 + (z1 j z2)
2,the thickness of the soft tissues at each cross point was measuredthrough multiplication by the pixel size (0.5 mm). Among each crosspoint, on the frontal view, 6 coordinates of the midface, excludingthe coordinates in the midline, were acquired and termed ARn, ALn(n = 1È3; Fig. 1). On both lateral views, 12 coordinates of the 6right and 6 left cross points corresponding to the midface, excludingthe occipital, were selected and termed LLm, LRm (m = 1È6;Fig. 2). As a result, on the frontal view, the hypoplastic and thenonhypoplastic sides were compared according to the 3 pairs ofcross points ARn and ALn (n = 1È3), and the 6 pairs of the right andthe left cross points LLm and LRm (m = 1È6) in the lateral viewwere compared with each other statistically. For statistical analysis,t test (P G 0.05) was performed.
RESULTS
On the frontal view of the symmetric craniosynostosis group, theright and the left sides were measured (mean [SD]) at 29 (14) and28 (16) mm, respectively; and on the lateral view, at 17 (17) and 17
(14) mm, respectively. The thicknesses of the soft tissues on the leftand the right sides from the frontal and the lateral views were notstatistically different (P = 0.440 and P = 0.936, respectively). Onthe frontal view of the asymmetric craniosynostosis group, the hy-poplastic and the nonhypoplastic sides were measured (mean [SD])to be 29 (24) and 43 (24) mm, respectively; and on the lateral view,21 (18) and 23 (19) mm, respectively. The results of the statisticalanalysis shows that in the study group, the hypoplastic and non-hypoplastic sides showed a significant difference on both the frontaland the lateral views (P = 0.048 and P = 0.034, respectively; Fig. 3,Table 1).
DISCUSSION
In the nonsyndromic craniosynostosis patients, the primary defor-mity of the cranium may secondarily induce deformity of the facialbones, and asymmetric deformities such as unicoronal synostosisand unilambdoid synostosis are commonly associated with hypo-plasia of the bone tissues in the ipsilateral area.4,5 Recently, due tothe generalization of cosmetic surgery, the interest of patients,guardians, and surgeons regarding the necessity of correcting facialasymmetry in congenital deformities has been on the rise. Therefore,it is important to more accurately understand facial asymmetry thatmay be developed in asymmetric craniosynostosis. However, studyinto the causes of facial asymmetry in craniosynostotic plagioce-phaly patients has mostly been focused on the asymmetry of bonetissues, and there have been few studies that have examined theasymmetry of soft tissues.8,9
Measuring soft tissue thickness using three-dimensional CTscans in our study is a new method. By realigning three-dimensionalCT scans on the standard horizontal and vertical plane, the locationof deviation that may occur during CT was standardized, and thefrontal and the lateral views among patients could be made identical.In addition, the cross points were selected by dividing the vertex andthe mentum into 9 equal parts and the right and left sides into 4 equalparts. Therefore, the measurement points were determined under anidentical demographic principle, which allowed us to minimize dif-ferences that may occur among patients. The distance between thecoordinates on the surface of the skin and the bone from each crosspoint was defined as the soft tissue thickness. This method could not
Table 1. Comparison of Soft Tissue Thicknesses
Group
View
Frontal Lateral
Symmetric CRSNo. patients, n 24 48Right, mean (SD), mm 28.9 (13.7) 17.3 (17.2)Left, mean (SD), mm 27.6 (15.6) 17.2 (14.4)P 0.440 0.936
Asymmetric CRSNo. patients, n 21 42Hypoplastic, mean (SD), mm 29.4 (23.8) 20.7 (17.8)Nonhypoplastic, mean (SD), mm 42.6 (24.1) 23.1 (19.1)P 0.048* 0.034*
The thickness of the hypoplastic side is significantly thinner than that of the non-hypoplastic side in the asymmetric craniosynostosis group.*The value is statically significant (P G 0.05).CRS indicates craniosynostosis.
FIGURE 3. Comparison of soft tissue thicknesses betweenboth sides (hypoplastic and nonhypoplastic). The thicknessof the hypoplastic side is significantly thinner than that of thenonhypoplastic side in the asymmetric craniosynostosis group.
The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009 Brief Clinical Notes
* 2009 Mutaz B. Habal, MD 2261

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
be a tool to measure the absolute soft tissue thickness, but it couldallow for the best consistency and reliability compared with othermethods reported until now, and it is meaningful as a noninvasivemethod to measure in vivo data.10Y12
The results show that asymmetry of soft tissues in asymmetriccraniosynostosis is also statistically significant as deduced by sur-geons, which demonstrates that the asymmetry of soft tissues con-tribute partially to facial asymmetry in patients with asymmetriccraniosynostosis. This suggests that attention must be paid duringfollow-up evaluation and corrective surgery. Considering that theimportance and effectiveness of soft tissue reconstruction in thecorrection of hemifacial microsomia and other facial asymmetry hasbeen reported, it is believed that similar concerns are warranted forasymmetric cranisynostosis.13,14
However, there were only 3 pairs of cross points in the frontal viewin our study, which are considered to be insufficient. This is becauseour study subjects were pediatric patients; thus, the ratio of the mid-facial area, including the maxilla, was markedly smaller than that inadults. Therefore, it is assumed that such errors could be reduced bymeasuring more cross points through the subdivision of the area orthe selection of already known landmarks in future studies.
CONCLUSIONS
Facial asymmetry developed in asymmetric craniosynostosis isaccompanied not only by asymmetry of bone tissues but alsoasymmetry of soft tissues, which should be considered for the eval-uation and treatment of this disease.
REFERENCES
1. Arnaud E, Renier D, Marchac D. Unoperated craniosynostosis patients:correction in adulthood. Plast Reconstr Surg 2008;122:1827Y1838
2. Pusch CM, Spring A, Czarnetzki A, et al. Morphometric analysis ofuntreated adult skulls in syndromic and nonsyndromic craniosynostosis.Neurosurg Rev 2008;31:179Y188
3. Richtsmeier JT, Vanderkolk CA, Marsh JL, et al. Three-dimensionalmorphological analysis of isolated metopic synostosis. Anat Rec1999;256:177Y188
4. Kane AA, Kim YO, Eaton A, et al. Quantification of osseous facialdysmorphology in untreated unilateral coronal synostosis. PlastReconstr Surg 2000;106:251Y258
5. Marsh JL, Gado MH, Vannier MW, et al. Osseous anatomy of unilateralcoronal synostosis. Cleft Palate J 1986;23:87Y100
6. Mulliken JB, Deutsch CK, Rogers GF, et al. Facial asymmetry inunilateral coronal synostosis: long-term results after fronto-orbitaladvancement. Plastic Reconstr Surg 2008;121:545Y562
7. Lee H, Kim K, Jang YB, et al. Alignment of CT images of skulldysmorphology using anatomy-based perpendicular axes. Phys MedBiol 2003;48:2681Y2695
8. Vaandrager JM, Mulder PG, Mathijssen IM, et al. Long-term aestheticresults of frontoorbital correction for frontal plagiocephaly. J Neurosurg2006;105:21Y25
9. Vannier MW,Marsh JL, Hardesty RA. Unicoronal synostosis. A surgicalintervention. Neurosurg Clin N Am 1991;2:641Y653
10. Singh, Jit P, Singh I, et al. Facial soft tissue thickness in northwest Indianadults. Forensic Sci Int 2008;176:137Y146
11. Vannier MW, Dawson DV, Lee JB, et al. Accuracy of facial soft tissuethickness measurements in personal computer-based multiplanarreconstructed computed tomographic images. Forensic Sci Int2005;155:28Y34
12. Son DG, Park BG, Kim JH, et al. Cadaver dissection and dynamic CTfor vascular anatomy of rectus abdominis muscle. J Korean Soc PlastReconstr Surg 2008;35:663Y668
13. Siebert JW, Longaker MT. Microsurgical correction of facial contour incongenital craniofacial malformations: the marriage of hard and softtissue. Plast Reconstr Surg 1996;98:942Y950
14. Siebert JW, McCarthy JG, Reavey P, et al. Microsurgical correction offacial contour deformities in patients with craniofacial malformations: a15-year experience. Plast Reconstr Surg 2008;121:368eY378e
Brief Clinical Notes The Journal of Craniofacial Surgery & Volume 20, Number 6, November 2009
2262 * 2009 Mutaz B. Habal, MD




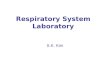










![Reconstruction of oral mucosal defects using the ...reconstruction was reported at the end of the nineteenth century [4,5]. Superiorly based nasolabial flaps can be used for reconstruction](https://img.dokumen.tips/doc/110x75/5f4833ce90a39d743618cf2a/reconstruction-of-oral-mucosal-defects-using-the-reconstruction-was-reported.jpg)