Embed Size (px)
Citation preview

Poster Design & Printing by Genigraphics® - 800.790.4001
A Unique Alternative in Reconstruction of Nasal Cavity DefectsScott A. Asher, MD1; Nathan S. Alexander, MD1; J. Scott Magnuson, MD1; Artemus J. Cox III, MD1
1From the Department of Surgery, Division of Otolaryngology – Head and Neck Surgery, School of Medicine at the University of Alabama at Birmingham, Birmingham, Alabama
OBJECTIVE
RESULTS
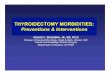
Figure 1. Preoperative images (A) and postoperative images (B) after resection and reconstruction.
ABSTRACTOBJECTIVE:There is a paucity of literature reporting nasal reconstruction after extirpation of nasal cavity/paranasal sinus malignancies. Here we describe a novel method for reconstruction of a unique nasal cavity defect with a variation of the commonly used paramedian forehead flap in conjunction with a calvarial bone graft. METHODS:One patient underwent open surgical excision of a stage IV squamous cell carcinoma of the nasal cavity/paranasal sinuses via lateral rhinotomy. The resultant defect required reconstruction of the upper two-thirds of the nasal framework, the entire nasal lining, yet none of the external skin. Near total septectomy and turbinectomy limited possible donor sites. The defect was reconstructed with a paramedian forehead flap to line the nasal cavity and provide coverage for a cantilevered calvarial bone graft. RESULTS:The described technique resulted in an excellent functional and aesthetic nasal reconstruction. It avoided the morbidity of a free flap, provided robust coverage that maintained viability throughout postoperative radiation therapy, preserved frontal sinus outflow tract patency, and allows for endoscopic oncologic surveillance. The patient has been very pleased with his postoperative appearance and reports excellent nasal airflow. CONCLUSIONS:Excision of advanced nasal cavity/paranasal sinus malignancies can yield unique and challenging nasal defects. The use of familiar techniques such as the paramedian forehead flap and calvarial bone grafting as presented here can result in a novel, functional, and aesthetic reconstruction.
METHODS
CONCLUSIONS
REFERENCES
Scott A. Asher, MDUAB PGY-4 Otolaryngology ResidentEmail: [email protected];
[email protected]: 205-218-3331
CONTACT
SPECIAL THANKS• To Daniel R. Englert for his expertise in medical illustration. All drawings are his original work.• To this particularly grateful patient for his consent to allow us to display his photographs and tell his story.
A
B
A B C
Malignancy of the nasal cavity/paranasal sinuses has an annual incidence of less than 1 per 100,000.1 There is a plethora of literature describing nasal reconstruction after cutaneous malignancy,2-9 but most research regarding reconstruction associated with nasal cavity/paranasal sinus malignancy has focused on the importance of recreating a barrier between intracranial contents and sinonasal compartments in cases of advanced disease.10-12 This disease process can result in defects somewhat dissimilar to those typically reconstructed by the facial plastic surgeon. It is rare to encounter a defect of the nasal lining and framework with the nasal skin intact. Typical teaching in nasal reconstruction suggests first identifying all deficiencies in the nasal external and internal lining as well as the framework in order to properly repair the defect. Next, all options on the reconstructive ladder must be considered before deciding the best strategy for each patient based on their individual defects, medical co-morbidities, and patient preferences.3, 9 The paramedian forehead flap and the calvarial bone graft are both commonly used tools for nasal reconstruction after excision of cutaneous malignancies.3, 9, 13-18 Here, we describe a novel method for reconstruction of a unique nasal cavity defect by applying these concepts and utilizing a variation of these commonly used tools.
The described technique resulted in an excellent functional and aesthetic nasal reconstruction (Figure 1B). He received postoperative radiation, and is doing well. Almost six months have passed and the patient has been very pleased thus far with his appearance and has deferred pedicle division, scar revision, or revision rhinoplasty. He has had no postoperative issues with sinusitis. Our technique has allowed for routine endoscopic oncologic surveillance that, to date, has shown no evidence of recurrent disease on physical exam or via radiologic survey (Figure 1). The patient has consistently reported excellent nasal airflow.
Here we describe a novel method for reconstruction of a unique nasal cavity defect with a variation of the commonly used paramedian forehead flap in conjunction with a calvarial bone graft. Lack of reconstruction certainly would have resulted in significant contraction with an obvious and extreme cosmetic saddle nose deformity, likely nasal airway obstruction, and the potential for frontal sinus mucocele formation. The nasal lining defect could have been addressed differently with a fasciocutaneous free flap (i.e. radial forearm), or a pericranial flap.19, 20 We felt like if we could spare the patient the morbidity of a free flap and still provide a robust enough coverage to avoid extrusion of the nasal framework, the paramedian forehead flap was the best option. The need for postoperative radiation therapy was a significant factor in our decision, and we felt inferior turbinate grafts would not provide adequate lining. As there is a significant recurrence rate with this type malignancy, we also kept in mind the need for potential donor sites in the future should the patient’s cancer recur.1 An osseocutaneous radial forearm free flap was one additional option for reconstruction considered that would have fulfilled both the nasal lining and framework requirements. The other options we considered for nasal framework were a costal cartilage or bone graft, homologous graft, or an alloplast. Utilizing this type flap and graft for nasal reconstruction is not novel. However, to our knowledge, reconstruction of this type defect has not previously been described. By reporting this case we hope to add to the indications for the use of these workhorse techniques, and strengthen the armamentarium of the facial plastic and reconstructive surgeon.
1. Dulguerov P, Jacobsen MS, Allal AS, Lehmann W, Calcaterra T. Nasal and paranasal sinus carcinoma: are we making progress? A series of 220 patients & a systematic review.Cancer.Dec 15 2001;92(12):3012-29.2. Ge NN, McGuire JF, Dyson S, Chark D. Nonmelanoma skin cancer of the head and neck II: surgical treatment and reconstruction. Am J Otolaryngol. May-Jun 2009;30(3):181-192.3. Baker SR. Local Flaps in Facial Reconstruction. 2nd ed. Philadelphia, PA: Elsevier; 2007.4. Burget GC, Walton RL. Optimal use of microvascular free flaps, cartilage grafts, and a paramedian forehead flap for aesthetic reconstruction of the nose and adjacent facial units. Plast Reconstr Surg. Oct
2007;120(5):1171-1207; discussion 1208-1116.5. Soliman S, Hatef DA, Hollier LH, Jr., Thornton JF. The rationale for direct linear closure of facial Mohs' defects. Plast Reconstr Surg. Jan;127(1):142-149.6. Shaye DA, Sykes JM, Kim JE. Advances in nasal reconstruction. Curr Opin Otolaryngol Head Neck Surg. Aug;19(4):251-256.7. Salgarelli AC, Bellini P, Multinu A, et al. Reconstruction of nasal skin cancer defects with local flaps. J Skin Cancer.2011:181093.8. Rohrich RJ, Griffin JR, Ansari M, Beran SJ, Potter JK. Nasal reconstruction--beyond aesthetic subunits: a 15-year review of 1334 cases. Plast Reconstr Surg. Nov 2004;114(6):1405-1416; discussion 1417-1409.9. Papel ID. Facial Plastic and Reconstructive Surgery. New York, NY: Thieme Medical Publishers, Incoporated; 2002.10. Zanation AM, Thorp BD, Parmar P, Harvey RJ. Reconstructive options for endoscopic skull base surgery. Otolaryngol Clin North Am. Oct;44(5):1201-1222.11. Harvey RJ, Parmar P, Sacks R, Zanation AM. Endoscopic skull base reconstruction of large dural defects: a systematic review of published evidence. Laryngoscope. Feb;122(2):452-459.12. Patel MR, Stadler ME, Snyderman CH, et al. How to choose? Endoscopic skull base reconstructive options and limitations. Skull Base. Nov;20(6):397-404.13. Boyd CM, Baker SR, Fader DJ, Wang TS, Johnson TM. The forehead flap for nasal reconstruction. Arch Dermatol. Nov 2000;136(11):1365-1370.14. Menick FJ. A 10-year experience in nasal reconstruction with the three-stage forehead flap. Plast Reconstr Surg. May 2002;109(6):1839-1855; discussion 1856-1861.15. Sajjadian A, Naghshineh N, Rubinstein R. Current status of grafts and implants in rhinoplasty: Part II. Homologous grafts and allogenic implants. Plast Reconstr Surg. Mar;125(3):99e-109e.16. Sajjadian A, Rubinstein R, Naghshineh N. Current status of grafts and implants in rhinoplasty: part I. Autologous grafts. Plast Reconstr Surg. Feb;125(2):40e-49e.17. Quetz J, Ambrosch P. Total nasal reconstruction: a 6-year experience with the three-stage forehead flap combined with the septal pivot flap. Facial Plast Surg. Jun;27(3):266-275.18. Alagoz MS, Isken T, Sen C, Onyedi M, Izmirli H, Yucel E. Three-dimensional nasal reconstruction using a prefabricated forehead flap: case report. Aesthetic Plast Surg. Jan 2008;32(1):166-171.19. Cannady SB, Cook TA, Wax MK. The total nasal defect and reconstruction. Facial Plast Surg Clin North Am. May 2009;17(2):189-201.20. Wax MK, Burkey BB, Bascom D, Rosenthal EL. The role of free tissue transfer in the reconstruction of massive neglected skin cancers of the head and neck. Arch Facial Plast Surg. Nov-Dec 2003;5(6):479-482.
This patient is a 61 year old male who presented with widening of the nasal dorsum (Figure 1A), nasal airway obstruction, and pain. He consented to open surgical excision of a stage IV squamous cell carcinoma of the nasal cavity/paranasal sinuses via left lateral rhinotomy. This resection included 80-90 percent of his nasal septum, both middle turbinates, bilateral upper lateral cartilages, bilateral nasal bones, a significant portion of the anterior table of the frontal sinus, anterior ethmoids, and almost the entire lining of the nose. The external skin of the nose and the lower lateral cartilages were able to be spared. There was no violation of the skull base or orbits.The resultant defect required reconstruction of the upper two-thirds of the nasal framework, and associated nasal lining. The prior left lateral rhinotomy incision was reopened (Figure 2). A left paramedian forehead flap was then raised in the standard fashion after measurement of the nasal lining defect. Rather than rotating or twisting the flap, it was flipped down into the nasal cavity and secured. The calvarial bone graft was then harvested and secured to the remaining frontal bone in a cantilevered fashion. The three layers of the nose were coapted and the lateral rhinotomy was closed. A small corner of the vascular pedicle that remained exposed was covered with a full-thickness skin graft. A nasal trumpet was temporarily placed in the left nasal cavity to serve as an inferior bolster and allow for airway patency. The right nasal cavity was left open for postoperative access to endoscopically monitor and ensure flap viability.
• Review of outcomes in our head and neck reconstruction patients has been given Institutional Review Board Approval at the University of Alabama at Birmingham.
Figure 2. Photos and artist’s depiction of nasal reconstruction. (A/D) The lateral rhinotomy was reopened revealing the defect. (B/E) Paramedian forehead flap is raised and shown how it will be used as the nasal lining after the framework is reconstructed. (C/F) The nasal skin is still held open revealing the calvarial bone graft secured and forehead flap flipped down to provide nasal lining.
D FE