Embed Size (px)
Citation preview

4�
aspect of the right forearm and another firm swelling (2x2 cm) over the dorsal aspect of distal radius.
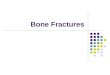
Radiographic examination of the right forearm (figure 1: a, b) showed irregular well defined osteolytic areas surrounded by sclerosis at the distal radius. Irregular bone formations at the
Soft-tissue Recurrence of Giant Cell tumor of Bone Associated with Pulmonary Metastases.
M. M. Abdel- Motaal 1, A. S. othman 1, M. K. C. Katchy 2, A. K. Jassar 3
1 Al-Razi orthopaedic Hospital, Kuwait, 2 Pathology Dept., Sabah Hospital, Kuwait, 3 Cytology laboratory, Hussein Makki Juma Centre for Specialized Surgery, Kuwait
Correspondance: Magdy M. Abdel-Mota’al.Specialist Orthopaedic Surgery. Al-Razi Orthopaedic Hospital,Kuwait. E-mail: [email protected]. Tel.: +�65-�5����1 / +�65-5�24185
Abstract
A soft tissue recurrence associated with pulmonary metastases developed in a 46 year old lady one year after intra-lesional excision and autogenous bone graft of giant cell tumor of bone of the distal end of the right radius. The different imaging modalities and procedures used for staging as well as the management were
discussed. Brief review of relevant literatures addressed different factors that influence recurrence, treatment options of primary and recurrent GCT of distal radius, and metaplastic bone formation in such lesions.
Key words
Giant cell, bone tumor, soft tissue recurrence, pulmonary metastases.
Introduction
Giant cell tumor (GCT) of bone is a benign but locally aggressive tumor that usually involves the ends of long bones (1). Despite its typical benign histologic features, multiple skeletal (2) and lung metastases were reported (�). GCT is characterized by a proliferation of mononuclear stromal cells and the presence of many multinucleated giant cells with homogenous distribution (1) .The stromal cells interact with hematopoietic cells in an autocrine manner to produce tumoral osteoclastogenesis and bone resorption (4). Soft tissue recurrence is a rare complication of GCT (5).
A case study
A 46 year old lady with a past history of surgical excision of a giant cell tumour of the distal end of the right radius in February 2004 in the form of intra-lesional excision and autogenous bone graft was referred to the Musculoskeletal Oncology Unit of Al-Razi Orthopaedic Hospital, Kuwait, in December 2007 with a painful swelling of the right forearm of 2 years duration.
Clinical examination revealed a diffuse hard swelling involving the distal half of the volar
Fig. 1a: Lateral view X-ray. Fig. 1b: AP view X-ray showing osteolytic lesion at distal radius with soft tissue ossification in forearm.
Fig. 1a Fig. 1b

50
Soft-tissue Recurrence of Giant Cell Tumor, M. M. Abdel- Motaal et al
radial styloid and early degenerative changes at the wrist were observed. There was soft tissue ossification at the distal half of the forearm, which was visualized in the CT (figure 1 c) as a thin shell of bone surrounding soft tissue mass anterior to the radius and ulna.
cystic changes. This bony lesion was associated with a large soft tissue mass lesion, involving the anterior compartment of the forearm, with a small extension of this soft tissue to the posterior compartment ( figure 2).
CT of the lung reported multiple bilateral variable size pulmonary nodules ( five in the right and one in the left basal segments). The largest nodule was one seen subpleurally at the lateral segment of the right middle lobe. CT guided fine needle aspiration was undertaken from the right lung nodule. Cytology examination reported benign features and showed a mixture of multinucleated and mononucleated cells with similar oval nuclei with, fine to granular chromatin, small nucleoli and variable mitosis which was consistent with metastatic benign GCT of bone (Fig �a, b).
Bone scan excluded multicentric GCT.
Fig. 2: T-1 sagittal cut MRI showing the intraosseous lesion, volar soft tissue mass and dorsal nodule
MRI imaging reported a large ill-defined bony lesion at the meta-diaphysis of the lower right radius, eliciting low T1 signal, mixed high T2 signal, as there were areas of fluid intensity like
Fig. 3a: A 22 gauge needle was inserted into the 2.0 cm right lung nodule to obtain cells for cytologic examination.
Fig. 1c: Axial CT showing shell of bone surrounding soft tissue lesion anterior to radius and ulna.
Fig.3b: Osteoclast type giant cells are characteristically evenly distributed in a background of mononuclear stromal cells.
Fig. 1c

G. J. O. Issue 5, 2009
51
Incisional biopsy from the volar soft tissue was done on �.12. 2007. Histological examination revealed giant cell tumor of bone.
Under brachial plexus block and pneumatic tourniquet, the intra and extra-osseous. Soft tissue recurrence was excised on 24.12.2007. The volar lesion was approached through an anterior midline incision. There was complete thin shell of bone surrounding reddish brown soft tissue (fig 4).
After marginal excision of the lesion, there was cortical defect in the volar aspect of the distal radius while the ulna was intact.
The intra-osseous part of the tumor was excised using curettes of different sizes and high-speed power burr. The cavity was filled with cement (polymethylmetharcrylate) .
Through a separated dorsal incision over the distal radius, a subcutaneous soft tissue nodule was removed.
The histopathology laboratory received two specimens: one from the incision biopsy and the other from the definitive marginal excision. The first, from the bone lesion comprised multiple pieces of tan soft tissue measuring �.5 x 2.5 x 0.5cm. The second was from the excised bone curettage and the excised soft tissue component. This comprised multiple pieces of bone and friable yellowish soft tissue measuring 11 x � x �cm. Both showed features of a giant cell tumor of bone composed of many giant cells set in a background of mononuclear stromal cells (figure 5a). In the second specimen, the lesion extended into the soft tissue and had a shell of bone at its periphery (figure 5b).
Fig. 4 : Intra-operative photography showing complete shell of bone surrounding reddish brown soft tissue.
The case was discussed during the multi disciplinary joint meeting at Hussein Makki Al-Juma Centre for Specialized Surgery, Kuwait (HMJCSS). Based on the multiplicity of the pulmonary metastases, the chest surgeon decided to observe her with regular radiological evaluation and CT. The patient was scheduled for regular follow-up by clinical assessment, X-ray and MRI, if necessary, for early detection of local recurrence.
Discussion
Approximately 10% of giant cell tumors involve the distal part of the radius, which is the third most common site after the distal end of the
Fig. 5a : Giant cell tumor of bone composed of multi-nucleated giant cells and round to oval mononuclear stromal cells (H & E x 200)
Fig. 5b : Giant cell tumor (GCT) infiltrating the soft tissue. Shell of bone is seen at its advancing margin on the right (H & E x 100)

52
Soft-tissue Recurrence of Giant Cell Tumor, M. M. Abdel- Motaal et al
femur and proximal end of the tibia (6,7). Local recurrence and a primary lesion at the distal radius are associated with an increase risk of lung metastases (�).
The rate of recurrence varies according to surgical techniques site and grade of GCT, and ranging from 8.�% (8) to 50% (�). Campanacci reported rate of local recurrence of 27% after intra-lesion excision, only 8% after marginal excision and zero % after wide or radical excision. O’Donnell (�) correlated the rate of recurrence to tumor sites, the highest rate was in the distal radius 5/10 cases, followed by the proximal tibia 7/25 cases (28%) and distal femur �/2� cases (25%). A recent study on 186 cases of GCT reported overall recurrence rate of 17%- 18% after curettage, and 16% after resection. For recurrent lesion treated by curettage, the recurrence rate was �5%(10).
Phenol (6, �) was used as adjuvant agents to destroy tumor cells remaining after curettage. Bone cement (polymethylmethacrylate) was applied as a local adjuvant to fill the resultant cavity left after curettage to provide mechanical stability (1,6,�). Chang (4) suggested topical or systemic use of bisphosphonates pamidronate or zoledronate as adjuvant therapy for GCT.
Treatment of benign aggressive tumors of the distal radius consisted of either curettage followed by packing the cavity with bone graft or cement, or resection of the lesion followed by some sort of reconstruction (11). Whenever possible, joint preservation is preferable regarding better extremity function but weaker grip, higher local tumor relapse, and late arthritis remains of concern (12). Wide resection is limited to patients with sever Campanacci Grade III (6) tumors, displaced pathological fracture with poor bone stack not allowing for internal fixation even with cement, or in patients with joint destruction (10). Puloski treated 14 cases out of 25 Campanacci Grade III (6) benign locally aggressive lesions (21 were giant cell tumors) involving the distal radius with aggressive curettage and high-speed
burring. The skeletal defect was reconstructed with cement in 8 patients, auto graft in � and allograft in 3. Recurrence was observed in five (12) patients, two of them had their joint salvaged.
Vult von Steyern (7) reported local recurrences of GCT in long bones following treatment with curettage and cementation in 1�7 patients. A total of 1� patients (14%) were recorded, and 1� of them were successfully treated by further curettage and cementation. McGough (16) reported 45 cases with recurrent GCT, 10 of them were located at distal radius. Repeated curettage was carried in 4 out of these 10 cases. He concluded that bone recurrences in the metaphyseal region were more amenable to re-curettage and joint sparing surgery than were subchondral recurrences (16).
A rare complication of GCT, observed in only 17 of 1,100 cases of GCT reported from the Mayo Clinic, is recurrence within the adjacent soft tissue .Often, the soft tissue implants show a radiographically detectable rim of metaplastic bone formation (5). Production of osteoinductive growth factors by GCT may have a paracrine effect on mesenchymal progenitor cells, thereby stimulating the osteoblastic differentiation and metaplastic bone formation (14).
Although it may be odd to link lung meta-stases, a behavior usually associated with malignancy, to histologically benign GCT, it has been observed by many investigators (6,�,15). The estimated incidence of this phenomenon is �% (15). On histology, the lung metastases are identical to benign GCT of bone (6). It is difficult to predict the behavior of this metastatic benign lesion to the lung. Spontaneous regression and disappearance has been reported (15). Surgical resection, including the excision of nodules, wedge or segmental resection and/or lobectomy, is the preferred treatment in such metastases (6,15). In cases in which lung lesions are unresectable or multiple, radiotherapy (6,16) or chemotherapy could be an option, but their usefulness remains to be confirmed (17).

G. J. O. Issue 5, 2009
5�
References
1. Turcotte R E .Giant cell tumor of bone. Orthop Clin N Am 2006; �7:�5-51.
2. Leichtle CI, Leichtle UG, Gartner V et al. Multiple skeletal metastases from a giant cell tumor of the distal fibula with fatal outcome. JBJS 2006; 88-B (�): ��8-��.
�. Siebenrock KA, Unni KK,Rock MG.Giant cell tumor of bone metastasising to the lung: A long-term follow-up. JBJS 1���; 80-B: 4�-7.
4. Chang SS, Suratwala SJ, Jung KM, et al. Bisphoshonates may reduce recurrence in giant cell tumor by inducing apoptosis. Clin Orthop 2004; 426:10�-10�.
5. Cooper KL,Beabout JW and Dahlin DC. Giant cell tumor: ossification in soft tissue implants. Radiology 1�84; 15�:5�7-602.
6. Campanacci M, Baldini N, Boriani S, et al. Giant cell tumor of bone. JBJS 1�87; 6�-A: 106-14.
7. Vult von Steyern F, Bauer HCF, Trovik C et al. Treatment of local recurrence of giant cell tumor in long bone after curettage and cementation: a Scandinavian Sarcoma Group study. JBJS 2006; 88-B (4):5�1-5.
8. Lewis VO, Wei A, Mendoza T, et al. Argon beam coagulation as an adjuvant for local control of giant cell tumor. Clin Orthop 2007; 454:1�2-7.
9. O’Donnell RJ,Sprigfield DS,Motwani HK, et al .Recurrence of giant cell tumor after curettage and packing with cement.JBJS 1��4 ;76-A(12):1827-��.
10. Turcotte RE, Wunder JS, Isler MH et al. Giant cell tumor of long bone. A Canadian Sarcoma Group Study. Clinc Orthop 2002; ��7:248-58.
11. Vander G, Robert A, Funderburk CH. The treatment of giant cell tumor of the distal part of the radius. JBJS 1���; 75-A (6):88�-�08.
12. Puloski SKT, Griffin A, Ferguson PC et al. Functional outcome after treatment of aggressive tumors in the distal radius. Clin Orthop 2007; 45�: 154-60.
1�. McGough RL,Rutledge J, Lewis VO. et al. Impact severity of local recurrence in giant cell tumor of bone. Clin Orthop 2005; 4�8:116-22.
14. Teot L A, O’Keefe R J, Rosier R N, et al. Extraosseous primary and recurrent giant cell tumor: transforming growth factor-b1 and –b2 expression may explain metaplastic bone formation. Human Pathology 1��6; 27 (7): 626-�2.
15. Tubbs WS, Brown LR, Beabout JW,et al. Benign giant cell tumor of bone with pulmonary metastases: clinical finding and radiologic appearance of metastases in 13 cases. AJR 1��2; 158:��1-4.
16. Feigenberg SJ, Marcus RB, Zlotecki RA, et al .Whole lung radiotherapy for giant cell tumors of bone with lung metastases. Clin Orthop 2002; 401: 202-8.
17. Bertoni F, Present D, Enneking WF. Giant-cell tumor of bone with pulmonary metastases. JBJS 1�85; 67-A (6): 8�0-�00.