Embed Size (px)
Citation preview
SLOWING PROGRESSION Mark SLOWING PROGRESSION OF KIDNEY DISEASE
Mark Rosenberg MD
University of MinnesotaOF KIDNEY DISEASE Minnesota

OUTLINEOUTLINE
1. Epidemiology of progression
2. Therapy to slow progressionBl d P t la. Blood Pressure control
b. Renin-angiotensin-aldosterone blockade
c. Dietary protein restriction
d. Bicarbonate
e. Delivery of care
f Future therapiesf. Future therapiesI. Endothelin receptor antagonism
II. Therapy directed at inflammation/oxidant stress
III Anti fibrotic therapyIII. Anti-fibrotic therapy
3. Conclusions

EPIDEMIOLOGY OF PROGRESSIONEPIDEMIOLOGY OF PROGRESSION


WHY IDENTIFY PATIENTS WITH EARLY CKD ?
Manage complications
AnemiaAnemia
Mineral and bone disorders
Hypertension
C di l **Cardiovascular **
Slow progressionp g
Plan for renal replacement therapy


PATHOPHYSIOLOGY OF PROGRESSIONPATHOPHYSIOLOGY OF PROGRESSION
Hyperfiltration
R i i i ldRenin-angiotensin-aldosterone
Inflammation/oxidant stressInflammation/oxidant stress
Genetic susceptibility

BP CONTROLBP CONTROL

INVEST (136 mmHg)
Trial SBP achieved
CONVINCE (137 mmHg)ALLHAT (138 mmHg)IDNT (138 mmHg)IDNT (138 mmHg)RENAAL (141 mmHg)UKPDS (144 mmHg)ABCD (132 mmHg)MDRD (132 mmHg)HOT (138 mmHg)HOT (138 mmHg)AASK (128 mmHg)
Number of BP Meds1 2 3 4
Bakris GL. Am J Kidney Dis. 2000;36(3):646-616
Number of BP Meds
Bakris
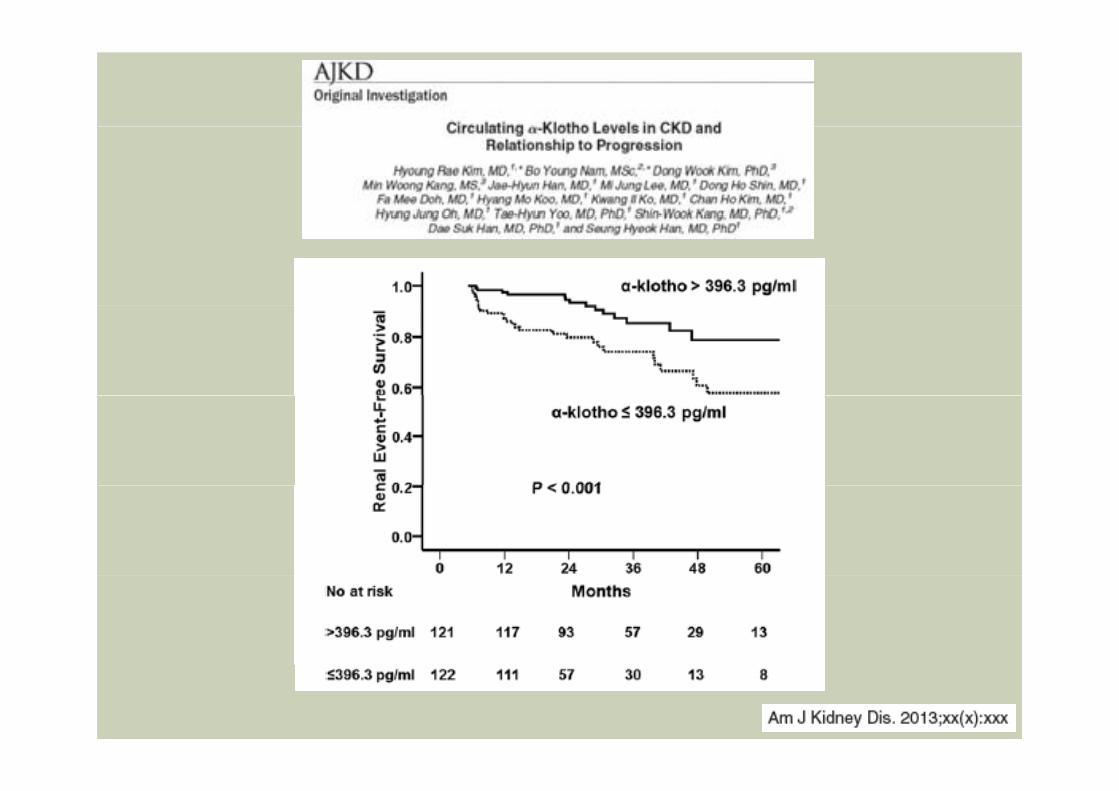
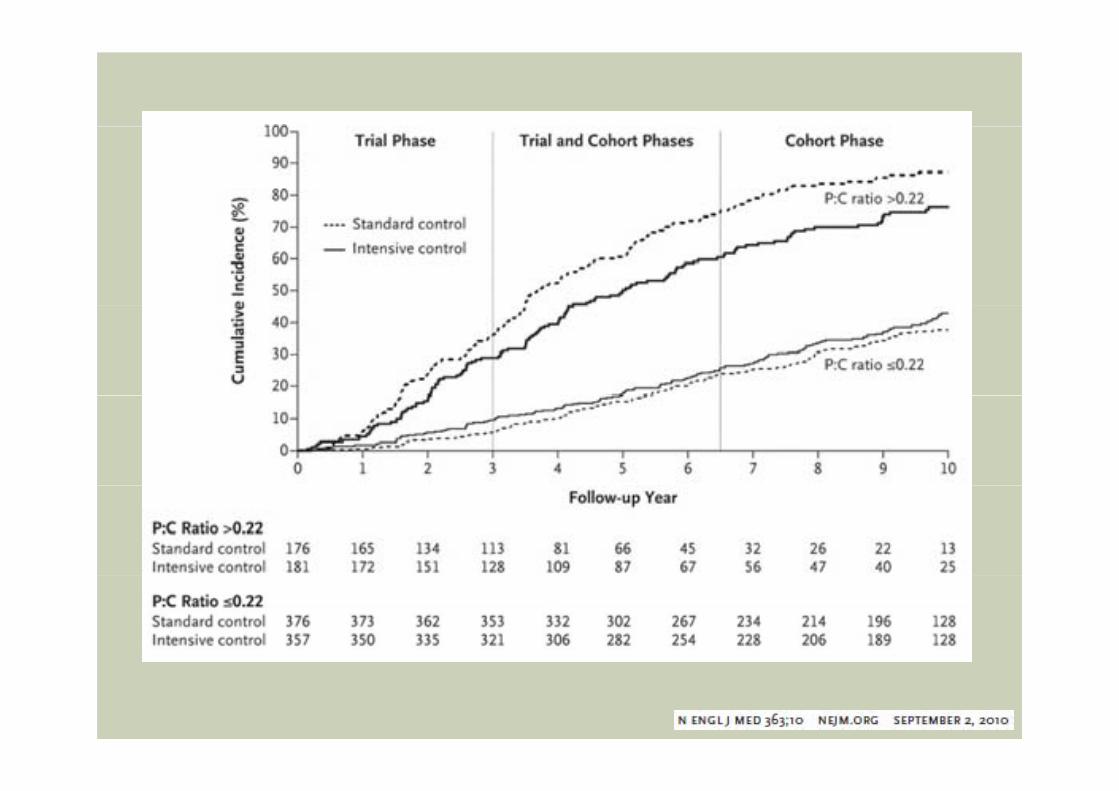
• 2272 subjects, non-diabetic kidney disease, trials comparing 2 different BP levels• MDRD• AASK• AASK• REIN-2
• BP target 125/75-130/80 not better than <140/90BP target 125/75 130/80 not better than <140/90• Low target may be beneficial in subgroups with
proteinuria >300-1000 mg/dproteinuria >300 1000 mg/d• Low BP needed more medications and had more
adverse eventsadverse events• SPRINT Study underway

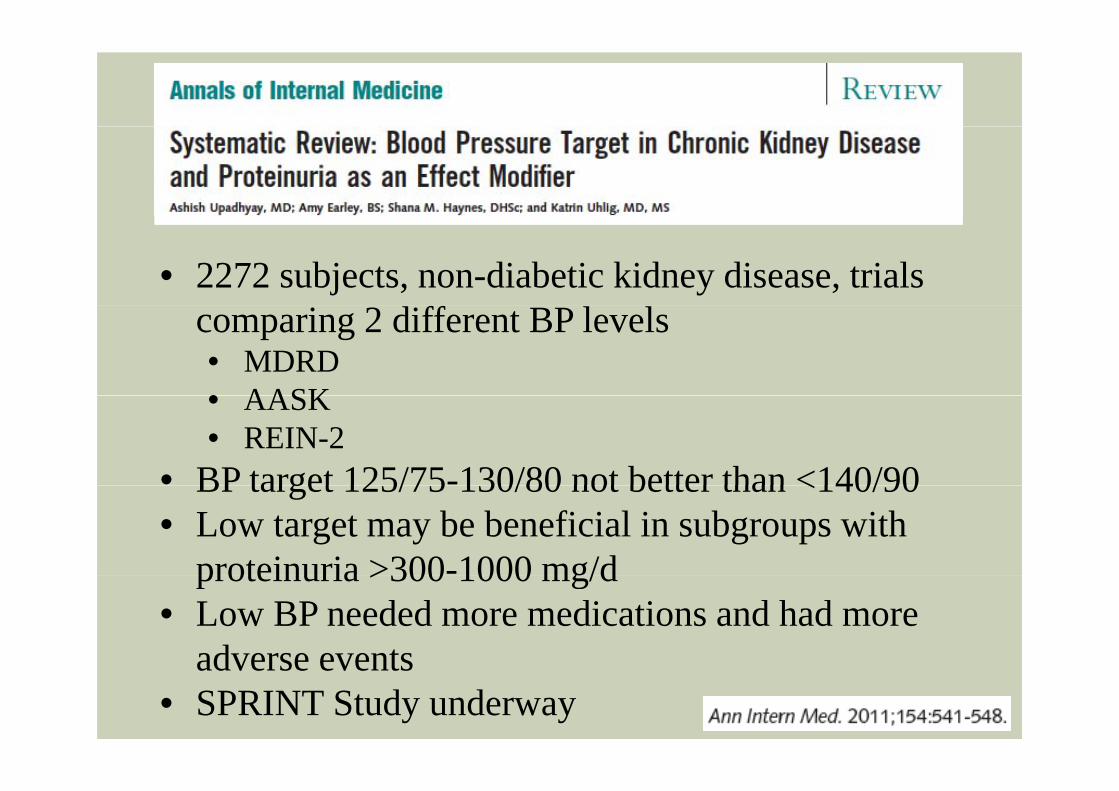
MDRD STUDY(MAP 107 VS 92 MMHG)
d GFR 13-24GFR 25-55
n = 32n = 63n = 136n = 54n = 104n = 420

Usual 140/90 (mean 102 107)JAMA. 2002;288(19):2421-2431. doi:10.1001/jama.288.19.2421
Usual 140/90 (mean 102-107)Lower 125/75 (mean 92)


ADVERSE EFFECTS OF ANGIOTENSIN II
Efferent arteriole glomerular capillary hypertension
proteinuria
Loss of podocytes
⇑ mesangial matrix⇑ mesangial matrix and proliferation
Afferent arteriole
Pro-fibrotic
proinflammatory

The renin-angiotensin-aldosterone system
Angiotensinogen Slide from Parving
Angiotensin I
Renin Renin Inhibitor
Angiotensin I
ACE-IACE
Angiotensin II
Angiotensin II receptor
ARB
Aldosterone antagonistAngiotensin II receptor Aldosterone antagonist
Aldosterone Aldosterone receptor

BENEFICIAL EFFECT OF RAS INHIBITION
Diabetic patientsNormoalbuminuric normotensive Microalbuminuric normotensiveDiabetic nephropathyDiabetic nephropathy
Non-diabetic kidney disease
Angiotensin II receptor blockade = Angiotensin converting enzyme inhibition
20% risk reduction

Group 1: Cr 1.5-3.0Group 2: Cr 3.1-5.0P i iPrimary outcome: time to doubling of Cr, ESRD, death
Hyperkalemia not a problem


EXPERIMENTAL MODELS IMPLICATINGALDOSTERONE AS A PATHOGENIC FACTOR
Remnant kidneyDOCA saltDOCA saltRadiation nephritisCyclosporine toxicityDi b tDiabetesObstructionOther models of hypertension

Efficacy of Eplerenone in Type 2 diabetic Patients with Albuminuria treated with Enalapril 20 mg dailyAlbuminuria treated with Enalapril 20 mg daily
Antiproteinuric effects after 12 weeks treatmentPlacebo Eplerenone Eplerenone
50 mg 100 mg
Antiproteinuric effects after 12 weeks treatment
10
0
g g(n=80) (n=83) (n=77)
e (%
)
7-20
-10
hang
e - 7
-40
-30
CR
Ch
60
-50
UA
C - 41*- 44 *
*p<0 01 vs placebo-60
Epstein M et al., Clin J Am Soc Nephrol 1: 940-951, 2006
p<0.01 vs. placebo


The renin-angiotensin-aldosterone system
Angiotensinogen Slide from Parving
Angiotensin I
Renin Renin Inhibitor
Angiotensin I
ACE-IACE
Angiotensin II
Angiotensin II receptor
ARB
Aldosterone antagonistAngiotensin II receptor Aldosterone antagonist
Aldosterone Aldosterone receptor

RAS blockade Dual blockade RAS blockade
1993 2003 2008 2012 2013
Randomized controlled trialR i il 10 t l i t 80 b thRamipril 10mg, telmisartan 80 mg or both25,620 subjects, age 55 with established ASCVD or diabetes with end organ damageFU 56 months
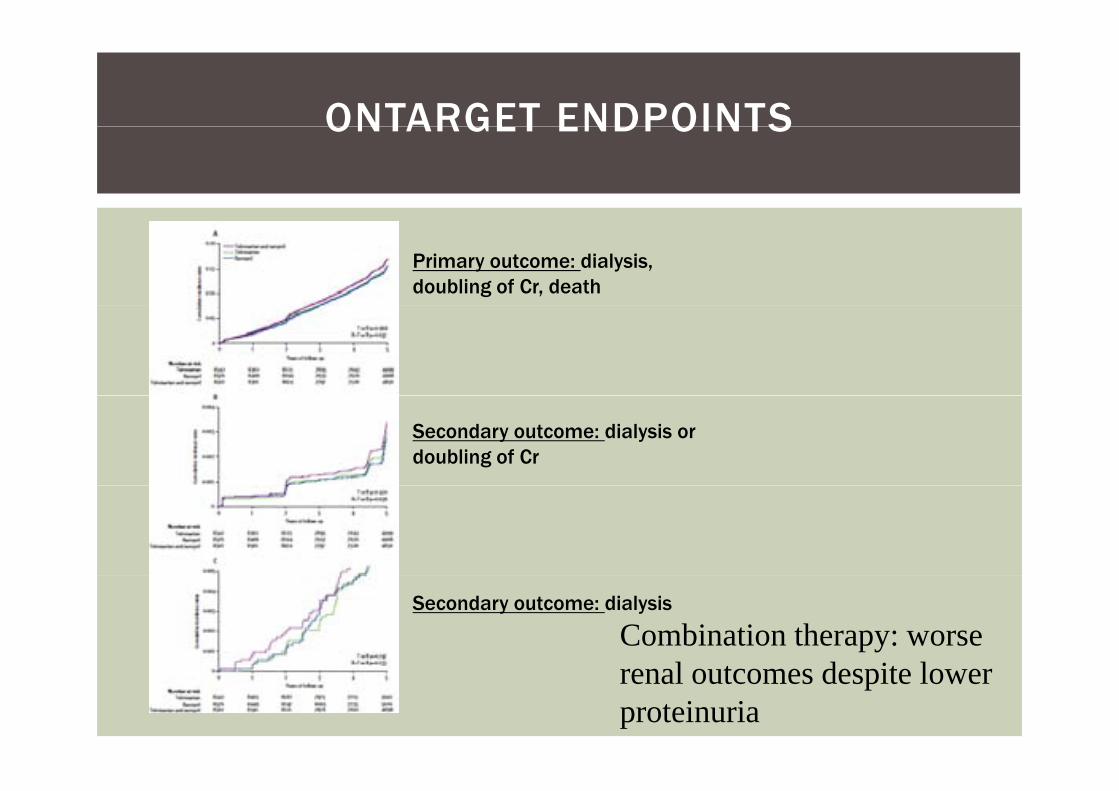
ONTARGET ENDPOINTSONTARGET ENDPOINTS
Primary outcome: dialysis, doubling of Cr, death
Secondary outcome: dialysis or doubling of Cr
Secondary outcome: dialysis
Combination therapy: worse l t d it lrenal outcomes despite lower
proteinuria

• 8561 with DM2 and CKD, CVD or both
• Aliskiren (300 mg/d) or placebo ( g ) padded to ARB
• Primary end point: time to CVD (cardiac arrest, MI, stroke, unplanned(cardiac arrest, MI, stroke, unplanned hospitalization for heart failure), ESRD, death to kidney failure, doubling of Cr need for RRTdoubling of Cr, need for RRT
• Study stopped: no difference in end point, more K>6 and hypotension
ith bi tiwith combination• >reduction in proteinuria with
aliskiren



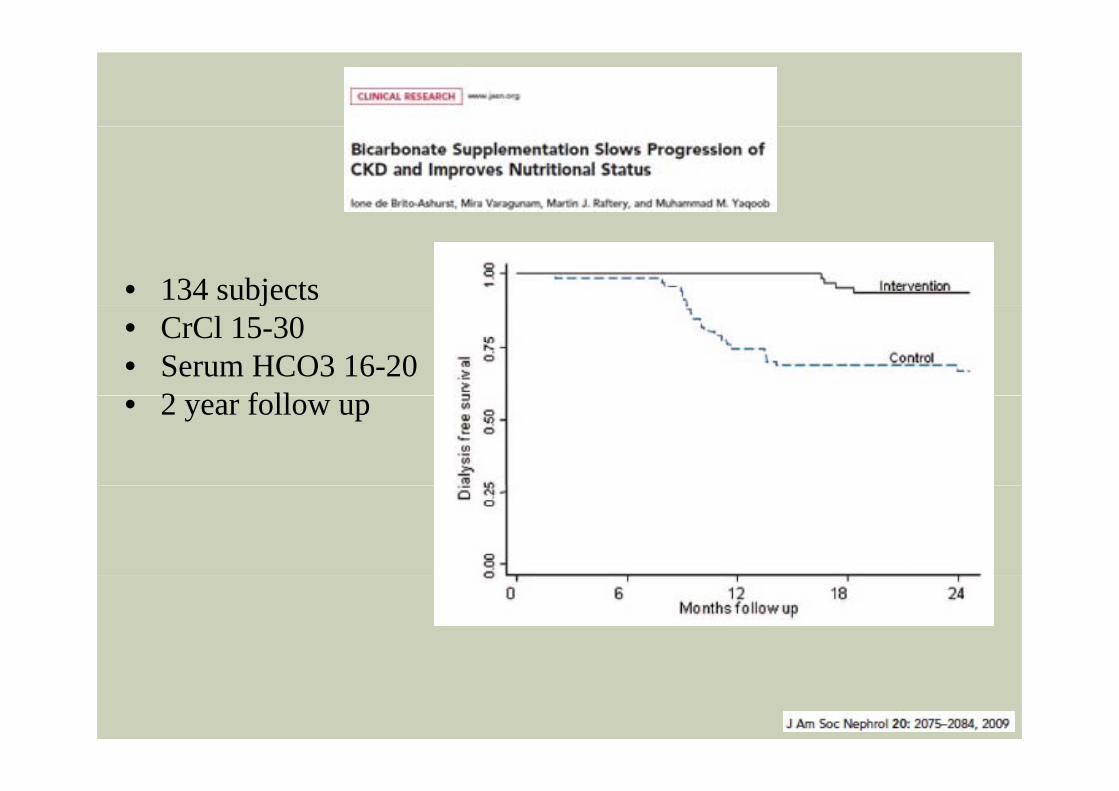
• 134 subjects j• CrCl 15-30• Serum HCO3 16-20
2 f ll• 2 year follow up

• 120 subjects• MacroalbuminuricMacroalbuminuric
hypertensive nephropathy
• GFR 60 90• GFR 60-90• 5 year follow up


No effect of renal disease progression: ESRD, death, or d bli f ti idoubling of creatinine

FUTURE THERAPIESFUTURE THERAPIES
Endothelin antagonists
Therapy directed at inflammation/oxidant stressinflammation/oxidant stress
Anti-fibrotic therapy
Cellular therapy
ENDOTHELIN 1ENDOTHELIN-1

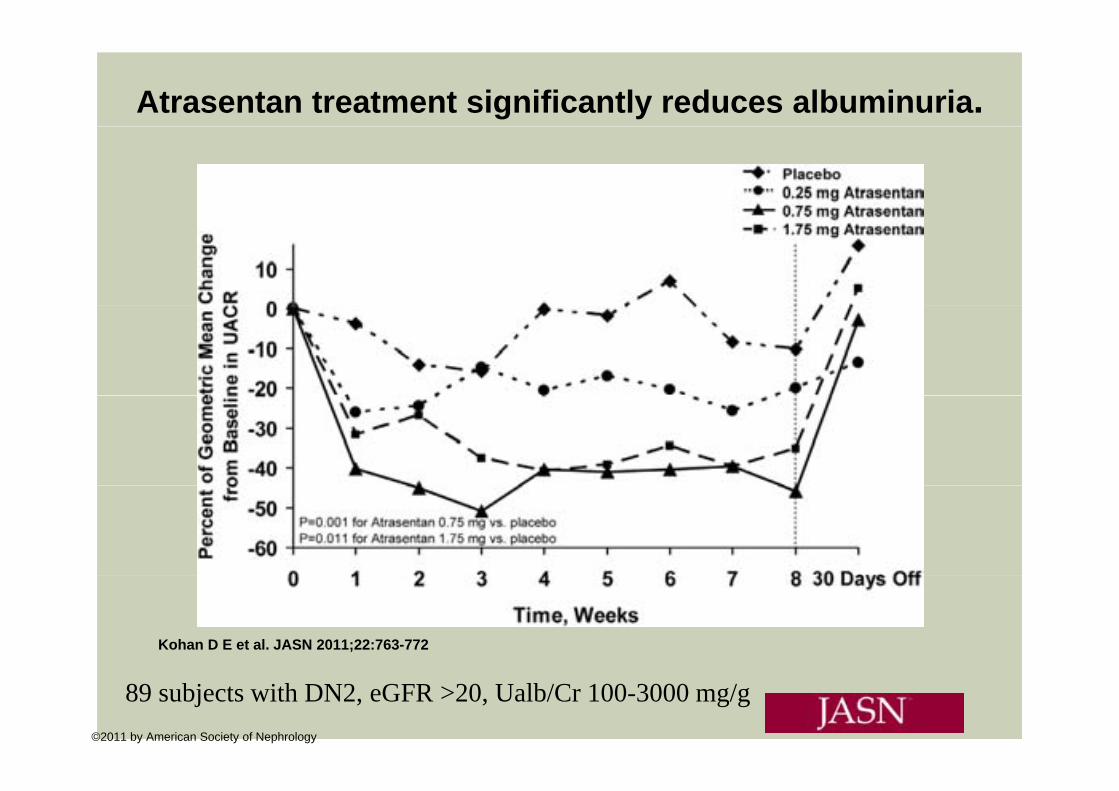
Atrasentan treatment significantly reduces albuminuria.
Kohan D E et al. JASN 2011;22:763-772
©2011 by American Society of Nephrology
89 subjects with DN2, eGFR >20, Ualb/Cr 100-3000 mg/g

Atrasentan treatment significantly increases the percentage of subjects achieving ≥ 40% reduction in UACR compared to placebo.
Kohan D E et al. JASN 2011;22:763-772
©2011 by American Society of Nephrology


• BEAM Study• Antioxidant inflammation modulator - activates nrf 2 –
transcription factor that controls 250 cytoprotective proteins and inhibits NF-kB227 DM2 GFR 20 45• 227 DM2 eGFR 20-45

BEACON: Bardoxolone Methyl Evaluation in Patients with CKD and Type 2 Diabetes: The Occurrence of Renal Events (Phase III)yp ( )
Study stopped - "for safety concerns due to excess serious adverse events and mortality in the bardoxolone methyl arm."


• 113 patients eGFR <60 randomly assigned to allopurinol 100 mg/d orassigned to allopurinol 100 mg/d or usual therapy; measurements at 6, 12 and 24 months
• Decrease in uric acid GFR changes• Decrease in uric acid, GFR changes, decreased CV events

• 77 patients with DN eGFR 20-75, albuminuria• Primary outcome change in eGFR at 1 year• 2400 mg group – high dropout rate (11/25) – GI symptoms fatigue
photosensitivity rashN=26 N=26 N=25
p y

DELIVERY OF CAREDELIVERY OF CARE
Multidisciplinary CKD programs “CKD Clinic”Better adherence to guidelinesg
Fistula first
Outpatient dialysis startsOutpatient dialysis starts
Early nephrology referralEarly nephrology referralAccess to a nephrologist for >1 year before dialysis initiation decreases mortalityinitiation decreases mortality


TELEHEALTHTELEHEALTH
CONCLUSIONSCONCLUSIONS
Lower BP – exact target unclear but be more aggressive in those patients with >proteinuriagg p p
Use RAAS blockade but only single agent
Keep HCO >22; consider low protein dietsKeep HCO3 >22; consider low protein diets
Early nephrology referral and coordinated CKD care
The future: endothelin antagonists, antifibrotic agents, antioxidants, cellular therapy
Future trial to watch for: SPRINT

Questions / Comments?

Courtesy of Jeff Connaire


OTHER THERAPYOTHER THERAPY
Glycemic controlDCCT – decreased transition from micro to macroalbuminuriaACCORD – stringent diabetes control reduced the transition to micro and macro albuminuriaalbuminuriaADVANCE – no difference in ESRDMinimal data of progression
PhosphatePhosphateAssociated with faster decline in GFRNo trials
Vitamin DNo trialsVITAL (paricalcitol) lowered albuminuria in DN
Lipid Observational studies demonstrate association between high lipids and progressionMeta analysis – small but sig effect on decline in GFR with statins vs placeboSHARP – no effect on progression (simvastatin 20 + ezetimibe 10 mgp g ( g

RATES OF PROGRESSIONRATES OF PROGRESSION
Study Disease Rate of progression(ml/min/year)
Normal aging None .5 – 1.0
AASK Hypertensive kidney disease 1.9 – 2.2