Embed Size (px)
Citation preview
Sleep, anesthesia, and the upper airwayDavid R. Hillman, Peter R. Platt, and Peter R. Eastwood
From the Departments of Pulmonary Physiology and Anaesthesia, West Australian Sleep Disorders Research Institute, SirCharles Gairdner Hospital, Perth, Western Australia.
Upper airway obstruction is a common problem during both sleep and anesthesia, and these tendenciesare related in individuals. Patency of the upper airway is determined by the balance of forces across thepharyngeal wall. Airway narrowing, increased extra luminal tissue pressure, and increased airway wallcompliance predispose to collapse, particularly during inspiration as negative intraluminal pressures aregenerated. The tendency to collapse is resisted by airway muscle activation, which is driven by acombination of influences including state-related wakeful stimulation, negative pressure reflexes, andrespiratory neuronal activity. This activation decreases with both sleep and anesthesia increasing thetendency to obstruction, and there are substantial overlaps in the way in which these states modulatethis neuronal compensatory activity. The common ground between sleep and anesthesia in all theseconsiderations emphasizes the importance of seeking and applying information regarding breathingduring sleep to everyday anesthesiology practice.© 2007 Elsevier Inc. All rights reserved.
KEYWORDS:Anesthesia;Sleep;Sedation;Upper airway
Maintenance of upper airway patency is a critical issueduring unconsciousness whether due to illness, other mis-adventure, anesthesia, or sleep. It is the first consideration inresuscitation protocols and in the management of sedated oranesthetized patients. It is also a prime concern in themanagement of patients with obstructive sleep apnea(OSA), a common problem characterized by recurrent epi-sodes of upper airway obstruction during sleep. Not surpris-ingly, vulnerability to OSA indicates increased risk of upperairway obstruction during anesthesia.1
In this paper, the effects of anesthesia and sleep on upperairway patency will be considered with particular regard tothe common ground and differences between these states ofunconsciousness, including the effects of sedation.
Determinants of upper airway patencyThe upper airway begins at the nose and lips and ends at thelarynx. Structurally, it consists of a potentially collapsible
segment (the pharynx) situated between two rigid tubes (thebony nasal passages and the cartilaginous larynx and tra-chea). The patency of this collapsible segment is dictated bythe interaction of a variety of passive mechanical and activeneural forces that together determine caliber of the airway,compliance of the airway wall, and pressure gradient acrossit.2 During inspiration, intraluminal pressure decreases,tending to narrow the airway. This tendency is greater if theairway is already narrow, the airway walls compliant, orextra luminal pressure increased. It is counteracted by acti-vation of pharyngeal dilator muscles, in part as a result oflocal reflexes and in part as a result of central activation,both phasic (generated by respiratory motor neuron activity)and tonic. Longitudinal traction on the upper airway fromlung volume increase may also counteract the tendency toairway narrowing.3
Caliber of the airway
A narrow airway is more vulnerable to collapse forseveral reasons. First, Laplace’s law dictates that recoilpressure generated across a distended curved elastic surfaceis inversely proportional to its radius of curvature. Second,
Address reprint requests and correspondence: Dr. David R. Hillman,Sir Charles Gairdner Hospital, Pulmonary Physiology, Hospital Ave., Ned-lands, WA 6009, Australia.
E-mail address: [email protected].
0277-0326/$ -see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1053/j.sane.2007.04.001
Seminars in Anesthesia, Perioperative Medicine and Pain (2007) 26, 65-72

the absolute change in caliber required for airway closure isless if the airway is already narrow. Third, increased resis-tance of the narrow airway necessitates generation of morenegative intraluminal pressures. Fourth, airway wall com-pliance is increased at lower calibers (see below). Thevelopharynx is usually the narrowest (and most compliant)segment in the upper airway,4 whether or not the subject hasOSA and appears to be most common primary site ofcollapse during both sleep5 and anesthesia.6
Transluminal pressure gradient
The pressure gradient across the airway wall is a functionof pressure in the tissues surrounding the airway (the extraluminal tissue pressure) and the intraluminal pressure.
Extra luminal tissue pressure increases with obesity andother increases in tissue volume (eg, angioedema) or nar-rowing of skeletal confines (as with neck flexion or micro-or retrognathia).7 The magnitude of decrease in intraluminalpressure during inspiration is a function of inspiratory flowrate and airway resistance upstream of the site of interest.Increased nasal resistance from narrowing of the nasal air-way is a common cause of increased upstream resistance.
Compliance of the airway wall
Airway wall compliance is an expression of its degree offlaccidity and, in the absence of muscle activity, is a func-tion of its passive elastic properties and the radial andlongitudinal tension to which it is subjected. A highly com-pliant (flaccid) airway is more likely to collapse and upperairway compliance is increased in OSA.8 While neuromus-cular activation decreases compliance, the passive (non-neuromuscular activation) components that influence com-pliance include the intrinsic elastic properties of the airwaymuscles, connective tissue, bony structures, and fat.9 Sur-face forces are also a potentially important factor withairway drying likely to decrease compliance as result of lossof the detergent-like influence of upper airway secretions.10
The volume-pressure (or cross-sectional area-pressure) re-lationship of the upper airway is alinear with increasedcompliance evident at low volumes/calibers8 increasing itscollapsibility. Longitudinal tension on the upper airwayincreases with increasing lung volume (“tracheal tug”), act-ing to decrease compliance.3 This, along with reflex muscleactivation (see below), stabilizes the airway during inspira-tion when the associated negative intraluminal airway pres-sure favors airway narrowing.
Upper airway muscle activation
There is a complex array of muscles within and aroundthe upper airway that variously act to constrict and/or dilateit as it fulfills its various roles which, besides providing aconduit for air between the environment and the lungs,include deglutition and phonation.
Apart from nasal and lip muscles, there are four groupsof muscles that directly influence upper airway patency.11
First, there are those that determine palatal position includ-ing muscles that favor oral breathing (such as tensor pala-tini, which stiffens the soft palate, levator palatini, whichelevates it, and musculus uvulae which elevates the uvula)and those that favor nasal breathing (such as palatopharyn-geus). Second, there are the muscles that constrict the phar-ynx (the superior, middle, and inferior pharyngeal constric-tors) which are situated on the posterior and side walls ofthe pharynx. Third, there are the extrinsic muscles of thetongue which suspend the tongue and include the genioglos-sus, geniohyoid, hyoglossus, and styloglossus (all of whichtend to dilate the retrolingual pharynx) and the palatoglos-sus (which also influences palatal position). Last, there arethose that control the position of the hyoid bone and tend tostabilize the anterior wall of the distal pharynx. These in-clude the inferiorly attached thyrohyoid, sternohyoid, andomohyoid muscles and the superiorly attached geniohyoid,mylohyoid, stylohyoid, and digastric muscles. The hyoglos-sus (an extrinsic tongue muscle) could also be consideredpart of this group.
Inspiratory activation of pharyngeal dilator muscles, ofwhich the genioglossus is the most important and beststudied, counteracts the tendency to narrowing and collapsewith inspiration-related decreases in airway pressure. Apartfrom this phasic inspiratory activity, tonic activity is presentduring wakefulness that also acts to stiffen and stabilize theairway wall. The activity of the genioglossus (and otherextrinsic tongue muscles, apart from palatoglossus) is me-diated via the hypoglossal nerve, the nucleus of which issituated in the medulla. The hypoglossal nucleus receives avariety of inputs that together determine its output andtherefore genioglossus activation.12 First, there are negativepressure reflexes initiated by mechanoreceptors principallysituated in the larynx. Second, the nucleus receives phasicinspiratory input from respiratory neurons arising from theponto-medullary central pattern generator. Third, wakeful-ness exerts a tonic excitatory effect on hypoglossal activity.It is these factors that are of most importance when theeffects of sleep and anesthesia on upper airway behavior areconsidered as these state changes influence them all to avarying degree.
Upper airway pressure–flow relationships: theStarling resistor model
The structural arrangement of the upper airway with itscollapsible pharyngeal segment situated between two rigidtubes (nasal and tracheal) corresponds to the basic elementsof a Starling resistor.13,14 This provides a useful model ofthe pressure–flow characteristics of the upper airway which,because of the collapsible nature of this conduit, does notconsistently behave like an ohmic resistor, where flow var-ies with the pressure gradient developed between its ends.
66 Seminars in Anesthesia, Perioperative Medicine and Pain, Vol 26, No 2, June 2007
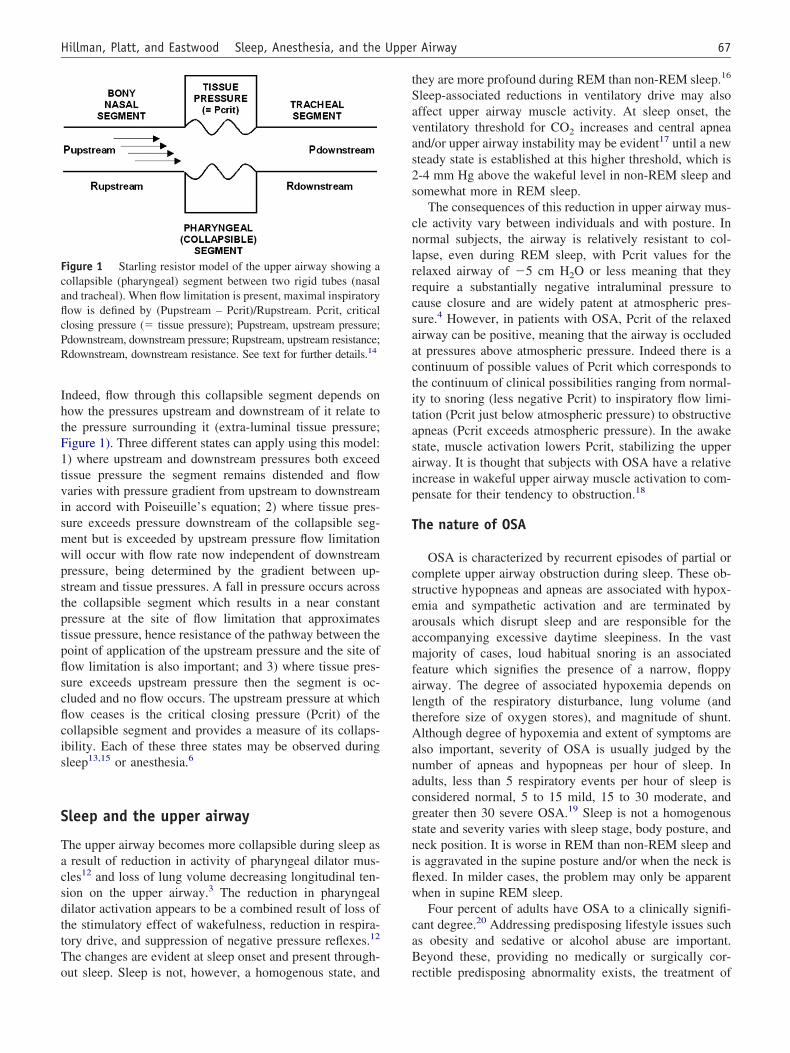
Indeed, flow through this collapsible segment depends onhow the pressures upstream and downstream of it relate tothe pressure surrounding it (extra-luminal tissue pressure;Figure 1). Three different states can apply using this model:1) where upstream and downstream pressures both exceedtissue pressure the segment remains distended and flowvaries with pressure gradient from upstream to downstreamin accord with Poiseuille’s equation; 2) where tissue pres-sure exceeds pressure downstream of the collapsible seg-ment but is exceeded by upstream pressure flow limitationwill occur with flow rate now independent of downstreampressure, being determined by the gradient between up-stream and tissue pressures. A fall in pressure occurs acrossthe collapsible segment which results in a near constantpressure at the site of flow limitation that approximatestissue pressure, hence resistance of the pathway between thepoint of application of the upstream pressure and the site offlow limitation is also important; and 3) where tissue pres-sure exceeds upstream pressure then the segment is oc-cluded and no flow occurs. The upstream pressure at whichflow ceases is the critical closing pressure (Pcrit) of thecollapsible segment and provides a measure of its collaps-ibility. Each of these three states may be observed duringsleep13,15 or anesthesia.6
Sleep and the upper airway
The upper airway becomes more collapsible during sleep asa result of reduction in activity of pharyngeal dilator mus-cles12 and loss of lung volume decreasing longitudinal ten-sion on the upper airway.3 The reduction in pharyngealdilator activation appears to be a combined result of loss ofthe stimulatory effect of wakefulness, reduction in respira-tory drive, and suppression of negative pressure reflexes.12
The changes are evident at sleep onset and present through-out sleep. Sleep is not, however, a homogenous state, and
they are more profound during REM than non-REM sleep.16
Sleep-associated reductions in ventilatory drive may alsoaffect upper airway muscle activity. At sleep onset, theventilatory threshold for CO2 increases and central apneaand/or upper airway instability may be evident17 until a newsteady state is established at this higher threshold, which is2-4 mm Hg above the wakeful level in non-REM sleep andsomewhat more in REM sleep.
The consequences of this reduction in upper airway mus-cle activity vary between individuals and with posture. Innormal subjects, the airway is relatively resistant to col-lapse, even during REM sleep, with Pcrit values for therelaxed airway of �5 cm H2O or less meaning that theyrequire a substantially negative intraluminal pressure tocause closure and are widely patent at atmospheric pres-sure.4 However, in patients with OSA, Pcrit of the relaxedairway can be positive, meaning that the airway is occludedat pressures above atmospheric pressure. Indeed there is acontinuum of possible values of Pcrit which corresponds tothe continuum of clinical possibilities ranging from normal-ity to snoring (less negative Pcrit) to inspiratory flow limi-tation (Pcrit just below atmospheric pressure) to obstructiveapneas (Pcrit exceeds atmospheric pressure). In the awakestate, muscle activation lowers Pcrit, stabilizing the upperairway. It is thought that subjects with OSA have a relativeincrease in wakeful upper airway muscle activation to com-pensate for their tendency to obstruction.18
The nature of OSA
OSA is characterized by recurrent episodes of partial orcomplete upper airway obstruction during sleep. These ob-structive hypopneas and apneas are associated with hypox-emia and sympathetic activation and are terminated byarousals which disrupt sleep and are responsible for theaccompanying excessive daytime sleepiness. In the vastmajority of cases, loud habitual snoring is an associatedfeature which signifies the presence of a narrow, floppyairway. The degree of associated hypoxemia depends onlength of the respiratory disturbance, lung volume (andtherefore size of oxygen stores), and magnitude of shunt.Although degree of hypoxemia and extent of symptoms arealso important, severity of OSA is usually judged by thenumber of apneas and hypopneas per hour of sleep. Inadults, less than 5 respiratory events per hour of sleep isconsidered normal, 5 to 15 mild, 15 to 30 moderate, andgreater then 30 severe OSA.19 Sleep is not a homogenousstate and severity varies with sleep stage, body posture, andneck position. It is worse in REM than non-REM sleep andis aggravated in the supine posture and/or when the neck isflexed. In milder cases, the problem may only be apparentwhen in supine REM sleep.
Four percent of adults have OSA to a clinically signifi-cant degree.20 Addressing predisposing lifestyle issues suchas obesity and sedative or alcohol abuse are important.Beyond these, providing no medically or surgically cor-rectible predisposing abnormality exists, the treatment of
Figure 1 Starling resistor model of the upper airway showing acollapsible (pharyngeal) segment between two rigid tubes (nasaland tracheal). When flow limitation is present, maximal inspiratoryflow is defined by (Pupstream – Pcrit)/Rupstream. Pcrit, criticalclosing pressure (� tissue pressure); Pupstream, upstream pressure;Pdownstream, downstream pressure; Rupstream, upstream resistance;Rdownstream, downstream resistance. See text for further details. 14
67Hillman, Platt, and Eastwood Sleep, Anesthesia, and the Upper Airway

choice is continuous positive airway pressure therapy, de-livered by a nasal mask.21 Dental splints designed to holdthe mandible forward during sleep are a useful but lesspredictably effective alternative.22
Factors predisposing to OSA
There are a number of patient and other factors thatpredispose to sleep apnea either through their effects onmorphology or neural control of the upper airway.
Patient factors include: age23; male gender24; meno-pause25; obesity26; increased neck circumference27; macro-glossia28; retrognathia29; maxillary constriction30; and nasalcongestion.31 These morphological changes may be presentto varying degrees in otherwise normal individuals or bepart of a disease syndrome, such as acromegaly, Down’ssyndrome, or Pierre-Robin syndrome or other syndromesassociated with craniofacial abnormality.
The reason why there is a male predisposition is multi-factorial24 but includes the effects of a longer airway, po-tentially higher extra luminal pressures because of bulk oftissues and hormonal effects on upper airway muscle acti-vation. It is notable that therapeutic or recreation use ofanabolic steroids increases risk of OSA and that the male:female differences in prevalence are less for post-meno-pausal women.
Obesity also increases OSA risk through several mech-anisms, including increase in upper airway extra luminaltissue pressure, and decreased functional residual capacity,particularly when recumbent.25
Shared morphological characteristics mean that familialpredispositions are common.32 Neuromuscular disorders in-volving upper airway muscles also predispose to obstruc-tion,33 as do endocrine, connective tissue, and storage dis-eases decreasing upper airway calibre. Examples ofendocrine diseases associated with increased risk of OSAinclude hypothyroidism and acromegaly. Specific abnor-malities in the upper airway predispose to upper airwayobstruction at discrete sites. Examples include nasal ob-struction,31 tonsillar and adenoidal hypertrophy,34 pharyn-geal and laryngeal tumors, foreign bodies, hematomas,edema, and laryngomalacia. Stroke and head injury can alsorender the patient vulnerable to upper airway obstruction bydepressing both muscle tone and arousal responses.
Other factors predisposing to sleep apnea include: alco-hol35 and sedative consumption,36 which also depress mus-cle tone and arousal responses; postural changes includingneck flexion37; recumbency; supine versus lateral posture38;smoking, probably because of associated nasal congestionand pharyngeal edema; and snoring itself which may causepharyngeal edema.
OSA and anesthesiology practice
It is important for anesthesiologists to understand thiscondition as its presence indicates an airway that may be
difficult to intubate or is vulnerable to obstruction under theinfluence of anesthetic, narcotic analgesic, or sedativedrugs. This vulnerability is compounded by the fact that, tovarying degrees, these drugs suppress arousal, the mecha-nism that protects the sleeping patient from prolonged as-phyxia. The factors that predispose to OSA also predisposeto upper airway obstruction under anesthesia, and those withOSA have a greater tendency to obstruction during anesthe-sia than those without.1 The reverse is also likely to be true,so that the possibility of OSA should be considered in allpatients who present difficulties with airway managementunder anesthesia.39
Anesthesia and the upper airway
Relative to sleep, anesthesia could be considered a “worstcase” for the upper airway. Unlike sleep, it is a relativelyhomogenous state and is characterized by profound depres-sion of upper airway muscle activity and abolition ofarousal responses. It is usually conducted with the patientsupine. Hence, it provides a milieu in which predisposedindividuals are highly likely to develop upper airway ob-struction while removing arousal as their source of protec-tion from prolonged asphyxiation.
Pathogenesis of upper airway obstruction underanesthesia
As with sleep, anesthesia predisposes to upper airwayobstruction through its depressant effects on upper airwaymuscle activity6 and lung volume.40 Like sleep,12 the re-duction in tonic and phasic muscle activity is a result of lossof wakeful drive (state change)41 together with a depressionin phasic drive deriving from upper airway reflexes6 andinput from the central respiratory pattern generator.42 Forthe major, and archetypical, upper airway dilator muscle,genioglossus, such changes are mediated via the hypoglos-sal nucleus. It is likely that anesthesia exerts its depressanteffects both directly on the nucleus and on its sources ofinput (wakeful drive from higher centers, upper airwayreflexes, respiratory drive) through activation of inhibitoryGABAA- and glycine-ergic pathways and inhibition of stim-ulatory on cholinergic, serotonergic, and glutamate path-ways. The hypoglossal nucleus is replete with such recep-tors as are its sources of input.43,44 In considering theinfluence of wakeful drive, it is again instructive to considerthe parallels between the states of sleep and anesthesia. Acommon narcotic mechanism has been proposed for bothstates that has as its basis a “thalamo-cortical switch” thatdetermines consciousness.45,46 It is thought that this derivesfrom a reciprocal interaction between sleep and wake pro-moting regions in or adjacent to the thalamus that producea bistable flip-flop switch controlling the transmission ofsensory information through the thalamus to the cortex. Keycenters include the inhibitory ventrolateral preoptic nucleus
68 Seminars in Anesthesia, Perioperative Medicine and Pain, Vol 26, No 2, June 2007

which is active in and necessary for normal sleep and thestimulatory posterior lateral hypothalamus activity which isnecessary for normal wakefulness. The ventrolateral preop-tic nucleus is heavily populated with the GABAA- andglycine-ergic receptors which are so readily activated byanesthetic drugs.46
There are also similarities in lung volume changes duringsleep47 and anesthesia.40 Functional residual capacity de-creases by approximately 20% in both states, leading to aloss of longitudinal traction on the upper airway and in-crease in extra luminal tissue pressure adjacent to the tho-racic inlet. Both effects contribute to increased upper airwaycollapsibility.
Sleep, hypnosis, sedation, and anesthesia
Hence, there are strong parallels between the sleep andanesthetic states that go well beyond the metaphorical use ofthe term “sleep” to describe anesthesia. The vital differencesfrom the clinical standpoint relate both to the magnitude ofeffect on neural drive to the upper airway muscles and toeffects on rousability. During sleep, some phasic and tonicmuscle activity is retained during non-REM sleep. In REMsleep, this is profoundly depressed and the conditions mostclosely approximate anesthesia.6 This is reflected in themore direct relationship seen between individual upper air-way collapsibility between anesthesia and REM than non-REM sleep.1
Hypnotics induce sleep which is a little different in itsarchitecture from natural sleep: benzodiazepines typicallycause a reduction in slow wave sleep and increase in gen-eration of sleep spindles.48 Beyond offset of their directsedative actions, the effect of these drugs is restorative interms of wakeful function. For the time that the hypnoticsare active, there is an increased propensity to sleep withattendant dose-related depression of ventilation, upper air-way muscle activation, and rousability which may precipi-tate or aggravate OSA.
Conscious sedation is a state in which mild noxiousstimuli are tolerated while the patient remains readily rous-able and the upper airway relatively protected. With deepersedation, arousal is less readily achieved and upper airwaypatency is at greater risk. Loss of rousability is a way-pointin a continuum of effect of sedative and anesthetic drugsthat ranges from hypnosis through sedation, terminating inoverdose and respiratory arrest. With anesthesia, thisboundary of rousability is crossed and asphyxiation is theinevitable consequence of unrecognized, untreated upperairway obstruction. Some anesthetic drugs, such as Propo-fol, have a wide clinical spectrum of action and are used toprovide sedation in subanesthetic doses. Although there isvariation between classes of drugs, in general, anestheticagents (for example, Propofol, Etomidate and inhalationalagents such as Sevoflurane) have a biphasic EEG effect withan increase in alpha (8-12 Hz) and beta (13-30 Hz) activity
during light sedation followed by a decrease that is accom-panied by an increase in delta (�4 Hz) activity such that theEEG slows and the amplitude increases.49,50 Alpha activityis also seen during relaxed wakefulness but disappears withthe transition to stage 2 sleep. The biphasic effect of anes-thetics has complicated attempts to design anesthetic depthmonitors on the basis of changes in EEG frequency alone.This problem has been addressed in the bispectral EEGindex (BIS) monitor by combining analysis of frequencycontent with that of phase relationships between individualwaveforms and burst suppression during deeper anesthe-sia.51 Although these monitors are primarily used to ensurethat awareness is abolished, it is possible that there is asystematic relationship between BIS score and vulnerabilityto upper airway obstruction and asphyxia, as a score of 100reflects full wakefulness, 85 to 90 loss of implicit memory,65 to 80 moderately heavy sedation, and less than 50 anes-thesia.50,51 However, not all anesthetic drugs are so readilycategorized: for example, the effect of Ketamine differs inthat, while the patient may be amnesic and unresponsive,there is little depression of the BIS score.52
Sleep in the postoperative period
Return of ready rousability is an important criterion to bemet before discharge from the recovery room followinganesthesia of patients without cause for prolonged uncon-sciousness. The similarities between the behavioral appear-ances of anesthesia and sleep and the potential obfuscationproduced by anesthesia EEG signatures cloud the analysisof post-anesthetic sleep.53 It is quite probable that anesthe-sia frequently transposes into natural sleep where postoper-ative pain in not an issue, particularly late at night whenpropensity to natural sleep is greatest.
In outpatient surgery, discharge from recovery room isfollowed by discharge home in a few hours. However, whilethe effects of anesthetic drugs dissipate in the early postop-erative period, the heavy postoperative analgesia/sedationrequired for more invasive surgery means that upper airwayobstruction remains a potential problem for the vulnerablepatient requiring use of these drugs. Regional anesthetictechniques provide a method of circumventing some ofthese potential difficulties.
Whereas anesthesia itself appears to have some restor-ative properties when unmodified by the effects of sur-gery,53 sleep is usually disturbed in the postoperative periodto a degree that varies with type and extent of surgery, pain,and its treatment, personality, and the nursing environment.The disturbances in sleep pattern include sleep deprivation,fragmentation, and disturbed sleep architecture with partic-ular loss of REM sleep and may persist for many dayspostoperatively.54 Not surprisingly, this can lead to seriouscognitive and psychomotor disturbance, although the effectsare offset to some extent, but the restorative effects ofdrug-induced sedation itself.55 The potential dangers to pa-tients with OSA are twofold. First, the effects of the post-operative sleep fragmentation compound those of fragmen-
69Hillman, Platt, and Eastwood Sleep, Anesthesia, and the Upper Airway

tation due to OSA itself. Second, re-establishment of normalsleep after a substantial period of sleep deprivation is char-acterized by a state of “REM-sleep rebound” where theamount of sleep spent in REM, the most vulnerable stage ofsleep for depression of neural drive to the upper airway andtherefore OSA, increases above the usual adult proportionof 20% to 25% of total sleep time.54
Implications for patient safety
The potential vulnerability of patient with OSA to theseperi-operative effects is a subject of increasing concern toanesthesiologists, leading to the development of guidelinesby bodies such as the American Society of Anesthesiolo-gists.56
Essentially these entail increased awareness of the prob-lem through better preoperative screening and interpretationof pre-, intra-, and postoperative observations combinedwith therapeutic strategies to circumvent or treat it.
Prudent steps in the management of such patients couldinclude57:
1. Screening all patients presenting for surgery for thepossibility of OSA. Beyond identifying those with pre-viously diagnosed OSA, this should include history (ofsnoring, witnessed apnoeas, disturbed sleep, excessivedaytime sleepiness, and hypertension) and examina-tion [body mass index, neck circumference and upperairway evaluation including pharyngeal appearance(width, Mallampati score)], mandibular size, and dentalocclusion.
2. Where the possibility of previously undiagnosed OSAhas been raised by this evaluation, probability of itspresence is assessed using a prediction rule approach,such as that of Flemons.58 Surgery is postponedwhere this assessment indicates an intermediate orhigh likelihood of OSA or the anaesthesiologist isotherwise concerned and surgery is elective and likelyto require narcotic analgesia or sedation postopera-tively. Where postponed, the patient is referred to asleep physician for evaluation and, where indicated,initiation of treatment.
3. Patients with diagnosed OSA on CPAP therapy areinstructed to bring the equipment to hospital for usewhenever asleep and/or sedated.
4. Patients in whom OSA has been diagnosed, either in-dependently or as part of preoperative work-up, butwho do not use CPAP regularly, are instructed in its usepreoperatively, so that it is readily applicable wheneverunder the influence of narcotics or sedatives.
5. Premedication with sedatives or opioids is avoidedwherever possible where OSA is known or suspected.Where required because of anxiety or pain then thepatient is observed in a high dependency area.
6. Regional anaesthetic and analgesic techniques are usedwhere feasible. Where general anesthesia is needed the
technique/drugs used are selected to allow early returnof consciousness and minimal post-anaesthetic sedationwherever possible.
7. CPAP is available for immediate use postoperatively inall patients with known or suspected OSA.
8. Patients with diagnosed OSA, or where the suspicion ofit has arisen preoperatively (but not been investigatedbecause of emergency), intraoperatively (because ofdifficulty with tracheal intubation or maintenance ofairway patency), or in the recovery room, are nursedpostoperatively in a high dependency area. This con-tinues until the patient is sentient and able to reliablyadminister CPAP unassisted or, in cases where OSAhas only been suspected, airway stability during sleepor sedation has been confirmed.
9. Where CPAP is refused and upper airway obstructioncontinues to be problematic, use of lateral positioning,a nasopharyngeal airway, and oxygen therapy are alter-nate strategies.
10. Where suspicion of OSA has arisen as a result of pre-,intra-, or postoperative events, the patient is informed andreferred to a sleep physician for further investigation.
Conclusion
Recognition of the parallels between sleep and anesthesiaon their effect on the upper airway has importance beyondperioperative management. A vulnerable airway under an-esthesia may also be vulnerable during sleep and sedationand the possibility of obstructive sleep apnea must alwaysbe considered in patients who present difficulty in terms ofinstrumentation or maintenance of airway patency duringanesthesia. Conversely, presence of OSA can indicate in-creased risk of problems perioperatively. Anesthesiologistsare well placed to screen large numbers of patients for thepossibility of OSA, and its identification has potential ben-efits for the patient beyond the perioperative period. Fur-thermore, there are overlapping therapeutic considerationsand techniques used in one domain have applicability in theother. It is likely, for instance, that CPAP, which is widelyused to treat OSA, is underused to prevent or treat upperairway obstruction in the recovery room. Conversely the oldanesthesiology principle of “jaw thrust” (mandibular ad-vancement) is now widely used in dental splints to treatobstructive sleep apnea.
References
1. Eastwood PR, Szollosi I, Platt PR, et al: Comparison of upper airwaycollapse during general anaesthesia and sleep. Lancet 359:1207-1209,2002
2. Remmers JE, deGroot WJ, Sauerland EK, et al: Pathogenesis of upperairway occlusion during sleep. J Appl Physiol 44:931-938, 1978
70 Seminars in Anesthesia, Perioperative Medicine and Pain, Vol 26, No 2, June 2007
3. Stanchina M, Malhotra A, Fogel RB, et al: The influence of lungvolume on pharyngeal mechanics, collapsibility, and genioglossusmuscle activation during sleep. Sleep 26:851-856, 2003
4. Isono S, Remmers JE, Tanaka A, et al: Anatomy of pharynx in patientswith obstructive sleep apnea and in normal subjects. J Appl Physiol82:1319-1326, 1997
5. Morrison DL, Launois SH, Isono S, et al: Pharyngeal narrowing andclosing pressures in patients with obstructive sleep apnea. Am RevRespir Dis 148:606-611, 1993
6. Eastwood PR, Szollosi I, Platt PR, et al: Collapsibility of the upperairway during anesthesia with isoflurane. Anesthesiology 97:786-793,2002
7. Watanabe T, Isono S, Tanaka A, et al: Contribution of body habitusand craniofacial characteristics to segmental closing pressures of thepassive pharynx in patients with sleep-disordered breathing. Am JRespir Crit Care Med 165:260-265, 2002
8. Isono S, Morrison DL, Launois SH, et al: Static mechanics of thevelopharynx of patients with obstructive sleep apnea. J Appl Physiol75:148-154, 1993
9. Rowley JA, Sanders CS, Zahn BR, et al: Gender differences in upperairway compliance during NREM sleep: role of neck circumference.J Appl Physiol 92:2535-2541, 2002
10. Kirkness J, Madronio M, Stavrinou R, et al: Relationship betweensurface tension of upper airway lining liquid and upper airway col-lapsibility during sleep in obstructive sleep apnea hypopnea syndrome.J Appl Physiol 95:1761-1766, 2003
11. Van Lunteren E, Strohl KP: The muscles of the upper airways. ClinChest Med 7:171-188, 1986
12. White DP: Pathogenesis of obstructive and central sleep apnea. Am JRespir Crit Care Med 172:1363-1370, 2005
13. Gold AR, Schwartz AR: The pharyngeal critical pressure. Chest 110:1077-1088, 1996
14. Hillman DR, Platt PR, Eastwood PR: The upper airway during anaes-thesia. Br J Anaesth 91:31-39, 2003
15. Smith PL, Wise RA, Gold AR, et al: Upper airway pressure-flowrelationships in obstructive sleep apnea. J Appl Physiol 64:789-795,1988
16. Horner RL: Motor control of the pharyngeal musculature and impli-cations for the pathogenesis of obstructive sleep apnoea. Sleep 19:827-853, 1996
17. Badr MS: Central sleep apnea. Prim Care 32:361-374, 200518. Mezzanotte WS, Tangel DJ, White DP: Waking genioglossal electro-
myogram in sleep apnea patients versus normal controls (a neuromus-cular compensatory mechanism). J Clin Invest 89:1571-1579, 1992
19. Practice parameters for the indications for polysomnography and re-lated procedures. Polysomnography Task Force, American Sleep Dis-orders Association Standards of Practice Committee. Sleep 20:406-422, 1997
20. Young T, Palta M, Dempsey J, et al: The occurrence of sleep-disor-dered breathing among middle-aged adults. N Engl J Med 328:1230-1235, 1993
21. Sullivan CE, Issa FG, Berthon-Jones M, et al: Reversal of obstructivesleep apnoea by continuous positive airway pressure applied throughthe nares. Lancet 18:862-865, 1981
22. O’Sullivan RA, Hillman DR, Mateljan R, et al: Mandibular advance-ment splint: an appliance to treat snoring and obstructive sleep apnea.Am J Respir Crit Care Med 151:194-198, 1995
23. Malhotra A, Huang Y, Fogel R, et al: Aging influences on pharyngealanatomy and physiology: the predisposition to pharyngeal collapse.Am J Med 119:e9-e14, 2006
24. Malhotra A, Huang Y, Fogel RB, et al: The male predisposition topharyngeal collapse: importance of airway length. Am J Respir CritCare Med 166:1388-1395, 2002
25. Dancey DR, Haly PJ, Soong C, et al: Impact of menopause on theprevalence and severity of sleep apnea. Chest 120:151-155, 2001
26. Grunstein RR, Wilcox I: Sleep-disordered breathing and obesity. Bal-lieres Clin Endocrinol Metab 8:601-628, 1994
27. Davies RJ, Stradling JR: The relationship between neck circumfer-ence, radiographic pharyngeal anatomy, and the obstructive sleepapnoea syndrome. Eur Respir J 3:509-514, 1990
28. Schellenberg JB, Maislin G, Schwab RJ: Physical findings and the riskfor obstructive sleep apnea. The importance of oropharyngeal struc-tures. Am J Respir Crit Care Med 162:740-748, 2000
29. Tangugsorn V, Skatvedt O, Krogstad O, et al: Obstructive sleepapnoea: a cephalometric study. Part I. Cervico-craniofacial skeletalmorphology Eur J Orthod 17:45-56, 1995
30. Cistulli P, Richards GN, Palmisano RG, et al: Influence of maxillaryconstriction on nasal resistance and sleep apnea severity in patientswith Marfan’s syndrome. Chest 110:1184-1188, 1996
31. Rappai M, Collop N, Kemp S, et al: The nose and sleep-disorderedbreathing: what we know and what we do not know. Chest 124:2309-2323, 2003
32. Redline S, Tosteson T, Tishler PV, et al: Studies in the genetics ofobstructive sleep apnoea. Familial aggregation of symptoms associatedwith sleep related breathing disturbances. Am Rev Respir Dis 145:440-444, 1992
33. Guilleminault C, Stoohs R, Quera-Salva MA: Sleep-related obstruc-tive and nonobstructive apneas and neurologic disorders. Neurology42:53-60, 1992
34. Helfaer MA, Wilson MD: Obstructive sleep apnea, control of ventilation,and anesthesia in children. Pediatr Clin North Am 41:131-151, 1994
35. Taasan VC, Block AJ, Boysen PG, et al: Alcohol increases sleep apneaand oxygen desaturation in asymptomatic men. Am J Med 71:240-245,1981
36. Berry RB, Kouchi K, Bower J, et al: Triazolam in patients withobstructive sleep apnea. Am J Respir Crit Care Med 151:450-454,1995
37. Choi JK, Goldman M, Koyal S, et al: Effect of jaw and head positionon airway resistance in obstructive sleep apnea. Sleep Breath 4:163-168, 2000
38. Penzel T, Moller M, Becker HF, et al: Effect of sleep position andsleep stage on the collapsibility of the upper airways in patients withsleep apnea. Sleep 24:90-95, 2001
39. Hiremath AS, Hillman DR, James AL, et al: Relationship betweendifficult tracheal intubation and obstructive sleep apnoea. Br J Anaesth80:606-611, 1998
40. Rehder K, Marsh HM: Respiratory mechanics during anesthesia andmechanical ventilation, in Macklem PT, Mead J (eds). Handbook ofPhysiology: The Respiratory System. Bethesda, MD, American Phys-iological Society, 1986, pp 737-752
41. Lydic R, Baghdoyan H: Sleep, anesthesiology and the neurobiology ofarousal state control. Anesthesiology 103:1268-1295, 2005
42. Eastwood PR, Platt PR, Shepherd K, et al: Collapsibility of the upperairway at different concentrations of propofol anesthesia. Anesthesi-ology 103:470-477, 2005
43. Liu X, Sood L, Liu H, et al: Suppression of genioglossus muscle toneand activity during reflex hypercapnic stimulation by GABA(A) mech-anisms at the hypoglossal motor nucleus in vivo. Neuroscience 116:249-259, 2003
44. Morrison JL, Sood L, Liu X, et al: Glycine at hypoglossal motornucleus: genioglossus activity, CO(2) responses, and the additive ef-fects of GABA. J Appl Physiol 93:1786-1796, 2002
45. Alkire MT, Haier RJ, Fallon JH: Toward a unified theory of narcosis:brain imaging evidence for a thalamocortical switch as the neurophys-iological basis of anesthetic-induced unconsciousness. ConsciousCogn 9:370-386, 2000
46. Saper CB, Chou TC, Scammell TE: The sleep switch: hypothalamiccontrol odf sleep and wakefulness. Trends Neurosci 24:726-731, 2001
47. Ballard RD, Irvin CG, Martin RJ, et al: Influence of sleep on lungvolume in asthmatic patients and normal subjects. J Appl Physiol68:2034-2041, 1990
48. Aeschbach D, Dijk DJ, Trachsel L, et al: Dynamics of slow-waveactivity and spindle frequency activity in the human sleep EEG: effectof midazolam and zopiclone. Neuropsychopharmacology 11:237-244,1994
71Hillman, Platt, and Eastwood Sleep, Anesthesia, and the Upper Airway

49. Kuizenga K, Wierda JM, Kalkman CJ: Biphasic EEG changes inrelation to loss of consciousness during induction with thiopental,propofol, etomidate, midazolam or sevoflurane. Br J Anaesth 86:354-360, 2001
50. Rampil IJ: A primer for EEG signal processing in anesthesia. Anes-thesiology 89:980-1002, 1998
51. Chan MTV, Gin T: What does the bispectral EEG index monitor? EurJ Anaesthesiol 17:146-148, 2000
52. Hans P, Dewandre PY, Brichant JF, et al: Comparative effects ofketamine on bispectral index and spectral entropy of the electroen-cephalogram under sevoflurane anaesthesia. Br J Anaesth 94:336-340,2005
53. Tung A, Mendelson WB: Anesthesia and sleep. Sleep Med Rev 8:213-225, 2004
54. Knill RL, Moote CA, Skinner MI, et al: Anesthesia with abdominalsurgery leads to intense REM sleep during the first postoperative week.Anesthesiology 70:52-61, 1990
55. Treggiari-Venzi M, Borgeat A, Fuchs-Buder T, et al: Overnight seda-tion with midazolam or propofol in the ICU: effects on sleep quality,anxiety and depression. Intensive Care Med 22:1186-1190, 1996
56. American Society of Anesthesiologists Task Force on PerioperativeManagement of Patients with Obstructive Sleep Apnea: Practiceguidelines for the perioperative management of patients with obstruc-tive sleep apnea. Anesthesiology 104:1081-1091, 2006
57. Hillman DR, Loadsman JA, Platt PR, et al: Obstructive sleep apnoeaand anaesthesia. Sleep Med Rev 8:459-471, 2004
58. Flemons WW: Obstructive sleep apnea. New Engl J Med 347:498-504,2002
72 Seminars in Anesthesia, Perioperative Medicine and Pain, Vol 26, No 2, June 2007