Embed Size (px)
Citation preview

HistorySystemic lupus erythematosus (SLE) is a chronic autoimmune disease that can affect almost any organ system. Its presentation and course are highly variable, ranging from indolent to fulminant.
The triad of fever, joint pain, and rash in a woman of childbearing age should suggest the diagnosis of SLE. This is one of the most common presentations of SLE.[30, 31] However, patients may present with any of the following types of manifestations[32, 33] :
Constitutional Musculoskeletal Dermatologic Renal Neuropsychiatric Pulmonary Gastrointestinal Cardiac Hematologic
In patients with suggestive clinical findings, a family history of autoimmune disease should raise further suspicion of SLE.
Constitutional symptoms
Fatigue, fever, arthralgia, and weight changes are the most common symptoms in new cases or recurrent active SLE flares. Fatigue, the most common constitutional symptom associated with SLE, can be due to active SLE, medications, lifestyle habits, or concomitant fibromyalgia or affective disorders.
Fatigue due to active SLE generally occurs in concert with other clinical and laboratory markers. Fever, another common yet nonspecific symptom of SLE, may also result from many causes, the most common of which include active SLE, infection, and medications (ie, drug fever). Careful history taking may help to differentiate these. Weight loss may occur in patients with active SLE. Weight gain may also be due to corticosteroid treatment or active disease such as nephrotic syndrome anasarca.
Musculoskeletal symptoms
Joint pain is one of the most common reasons for the initial clinical presentation in patients with SLE. Arthralgia, myalgia, and frank arthritis may involve the small joints of the hands, wrists, and knees. In contrast to rheumatoid arthritis, SLE arthritis or arthralgia may be asymmetrical, with pain that is disproportionate to swelling.
Dermatologic symptoms

Cutaneous manifestations of SLE comprise 4 diagnostic criteria and multiple other clues to a potential diagnosis of lupus.
The first criterion is malar rash, which is characterized by an erythematous rash over the cheeks and nasal bridge. It lasts from days to weeks and is occasionally painful or pruritic.
The second feature is photosensitivity, which may be elicited from patients who are asked if they have any unusual rash or symptom exacerbation after sun exposure.
The third feature may be discoid rash. Discoid lesions often also develop in sun-exposed areas but are plaquelike in character, with follicular plugging and scarring. They may be part of systemic lupus or may represent discoid lupus without organ involvement, which is a separate diagnostic entity.
Alopecia is the fourth and often less-specific cutaneous feature of SLE. It often affects the temporal regions or creates a patchlike pattern of hair loss.
Other cutaneous manifestations related to but not specific to SLE include the following:
Raynaud phenomenon Livedo reticularis Panniculitis (lupus profundus) Bullous lesions Vasculitic purpura Telangiectasias Urticaria
Renal features
The kidney is the most commonly involved visceral organ in SLE. Although only approximately 50% of patients with SLE develop clinically evident renal disease, biopsy studies demonstrate some degree of renal involvement in almost all patients. Glomerular disease usually develops within the first few years of SLE onset and is usually asymptomatic.
Acute or chronic renal failure may cause symptoms related to uremia and fluid overload. Acute nephritic disease may manifest as hypertension and hematuria. Nephrotic syndrome may cause edema, weight gain, or hyperlipidemia.
Neuropsychiatric features
The CNS lupus nomenclature has been revised to catalog many manifestations.[34, 35] Because of the difficulty in distinguishing causal SLE associations from certain neurologic features of the disease, only seizure and psychosis are included among the diagnostic criteria. Seizures related to SLE may be generalized or partial and may precipitate status epilepticus. Psychosis may manifest as paranoia or hallucinations.

Delirium represents a spectrum of fluctuating altered consciousness characteristic of SLE. Delirium may be caused by CNS vasculitis, encephalopathy, or the manifestations previously called organic brain syndrome. Aseptic meningitis, myelopathy, optic neuropathy, or other demyelinating disorders may also require urgent evaluation. Transverse myelitis with spastic paraparesis is a rare but serious complication of SLE.
Cognitive disorders may be variably apparent in patients with SLE. Formal neuropsychiatric testing reveals deficits in 21-67% of patients with SLE. Whether this represents true encephalopathy, neurological damage, medication effects, depression, or some other process is unclear. A study of female patients aged 14-37 years with SLE and posterior reversible encephalopathy syndrome (PRES) noted that PRES occurs in young lupus patients and in the early stages of the disease; it can be the presenting manifestation of lupus.[36]
A 2010 multicenter study found that depression was associated with significantly poorer cognitive function in 111 patients newly diagnosed with SLE.[37] Stroke and transient ischemic attack (TIA) may be related to antiphospholipid antibody syndrome or vasculitis.
Migraine headaches may be linked to antiphospholipid syndrome, although this is less clear. Headache and mood disorders may be the most commonly reported neurologic manifestation of SLE, but cause and effect may be difficult to distinguish.
For additional information on this topic, see the Medscape Reference article Neurologic Manifestations of Systemic Lupus Erythematosus.
Pulmonary features
Pulmonary features of SLE may manifest acutely or indolently, representing many complications. Pleurisy with pleuritic chest pain with or without pleural effusions is the most common feature of acute pulmonary involvement in SLE. Shortness of breath or dyspnea may be due to many causes. Pulmonary embolism, lupus pneumonitis, chronic lupus interstitial lung disease, complement-mediated pulmonary leukoaggregation, or infection may be related to lupus disease.
Rarely, pulmonary hypertension without underlying parenchymal lung disease presents as symptomatic dyspnea or right-sided heart failure. Most seriously, hemoptysis may herald diffuse alveolar hemorrhage, a rare, acute, life-threatening pulmonary complication of SLE.
Gastrointestinal features
Gastrointestinal symptoms secondary to primary SLE and adverse effects of medication are common among persons with SLE. Patients may report vague abdominal discomfort or acute crampy pain, nausea, vomiting, or diarrhea.
Abdominal pain in SLE is significant because it may be directly related to active lupus, including peritonitis, pancreatitis, mesenteric vasculitis, and bowel infarction. Nausea and dyspepsia are common symptoms in patients with active SLE and are sometimes difficult to correlate with

objective evidence of gastrointestinal involvement. Jaundice due to autoimmune hepatitis may also occur.
Cardiac features
Heart failure or chest pain must be carefully assessed in patients with SLE. Pericarditis is the most common cardiac feature of SLE, manifesting as positional chest pain that is often relieved when the patient leans forward. Myocarditis may occur in SLE with heart failure symptoms.
Coronary vasculitis manifesting as angina or infarction is rarely reported. Libman-Sacks endocarditis is noninfectious but may manifest as symptoms similar to those of infective endocarditis. More commonly, accelerated ischemic coronary artery disease (CAD) is associated with SLE and may present indolently as atypical anginal equivalents.
Hematologic features
A history of multiple cytopenias such as leukopenia, lymphopenia, anemia, or thrombocytopenia may suggest SLE, among other etiologies. Leukopenia and, more specifically, lymphopenia are common in SLE; this and hypocomplementemia may predispose persons with SLE to frequent infections.
Anemia is occasionally overlooked in young menstruating women. Thrombocytopenia may be mild or part of a thrombotic thrombocytopenic purpura (TTP)–like syndrome or antiphospholipid antibody syndrome. A history of recurrent early miscarriages or a single late pregnancy loss may be clues to lupus or isolated antiphospholipid antibody syndrome.[38]
Physical ExaminationAlmost any organ system can be involved in active SLE. The constellation of several physical findings may suggest a diagnosis of SLE. The American College of Rheumatology (ACR) diagnostic criteria are discussed in Workup. Examination findings are discussed by system.[32, 33]
Fever is a challenging problem in SLE. It can be a manifestation of active lupus, infection, malignancy, or a drug reaction. Low-grade fever is observed in patients on immunosuppressive agents. Lymphadenopathy or splenomegaly may be found.
Patients with fever need to have infectious causes ruled out—both viral and bacterial. Patients with SLE who are on immunosuppressive therapy are at a higher risk of death due to infection from viruses (eg, herpes simplex virus [HSV], cytomegalovirus [CMV], varicella-zoster virus [VZV]) and should be treated accordingly if a viral illness is suspected.[39] An infection can mimic a lupus flare and delays in diagnosis and institution of treatment result in increased mortality.[40]
Skin and mucous membrane findings

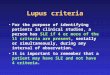
Malar rash is a fixed erythema that typically spares the nasolabial folds (see image below). It is a butterfly-shaped rash that can be flat or raised over the cheeks and bridge of the nose. It also often involves the chin and ears, as shown below.
The classic malar rash, also known as a butterfly rash, with distribution over the cheeks and nasal bridge. Note that the fixed erythema, sometimes with mild induration as seen here, characteristically spares the nasolabial folds.
Photosensitive rash is often macular or diffusely erythematous in sun-exposed areas of the face, arms, or hands. See the image below.
Photosensitive systemic lupus erythematosus (SLE) rashes typically occur on the face or extremities, which are sun-exposed regions. Photo courtesy of Dr. Erik Stratman, Marshfield Clinic.
Discoid rash occurs in 20% of patients with SLE and can result in disfiguring scars. The discoid rash can present as erythematous patches with keratotic scaling over sun-exposed areas of the skin. Follicular plugging may create scarring. Systemic manifestations of SLE may be absent (ie, limited discoid lupus).
Hair loss may occur. Alopecia in SLE often affects the temporal regions or creates a patchy pattern.
Lupus should be considered in all patients who experience painless or painful oral or vaginal ulcers. Palatal ulcers are most specific for SLE.
Many other cutaneous findings are not explicitly diagnostic features of SLE. Livedo reticularis is characterized by a lacy, mottled, erythematous skin pattern that develops in some patients with SLE or antiphospholipid antibody syndrome. Raynaud phenomenon may be observed with blue, white, and red color change at the distal digital tips. Capillaroscopy can be performed with an

ophthalmoscope to search for dilated capillary nailfold loops. Panniculitis, bullous lesions, vasculitic purpura, and urticaria are other skin lesions that are sometimes seen in SLE.
Musculoskeletal findings
Arthritis of the proximal interphalangeal (PIP) and metacarpophalangeal (MCP) joints of the hands as well as the wrists is the most common musculoskeletal finding in SLE, followed by arthritis of the knees. Tenderness, edema, and effusions accompany a polyarthritis that is symmetric, nonerosive, and usually nondeforming. Jaccoud arthropathy is the term used to describe the nonerosive hand deformities due to chronic arthritis and tendonitis that develop in 10% of patients with SLE.
Myositis that may manifest as weakness rarely occurs and is more commonly related to overlap syndromes or corticosteroid-induced myopathy. Fibromyalgia, which should be distinguished by myofascial tenderness without weakness, is commonly concomitant with SLE, causing generalized widespread pain, arthralgia, and myalgia.
Consider avascular necrosis in patients who are taking glucocorticoids. Consider septic arthritis when one joint is inflamed out of proportion to all other joints.
Renal findings
Hypertension or hematuria may signal nephritic SLE. Edema of periorbital or peripheral regions and anasarca are common physical findings related to nephrotic syndrome or volume overload with renal failure. Specific signs and symptoms of renal disease may not be apparent until advanced nephrotic syndrome or renal failure is present; therefore, obtaining a urine analysis and serum BUN and creatinine levels on a regular basis is important.
Neuropsychiatric findings
About 28-40% of neuropsychiatric SLE findings arise before or around the time of diagnosis.[41]
Headache is the most commonly seen CNS finding in SLE, occurring in 39-61% of adults and 72% of children.[41] Altered mental status in SLE may be secondary to aseptic meningitis, seizures, psychosis, or organic brain syndrome. All types of seizures have been reported; the most frequent is the grand mal seizure. Sensory or sensorimotor neuropathies are also common.
Focal neurologic deficits may represent stroke, transient ischemic attack (TIA), or mononeuritis. Mononeuritis may manifest as the functional loss of one or a few isolated peripheral nerves and is observed in some patients with SLE vasculitis or antiphospholipid disease.
Incidence of stroke is high in the first 5 years of disease. Patients with antiphospholipid antibodies are at higher risk for such events.
Cardiopulmonary findings

Pleuropericardial friction rubs and signs of effusions may be found. Tachypnea, cough, and fever are common manifestations of lupus pneumonitis. Hemoptysis may signify pulmonary hemorrhage secondary to the disease. However, infection is the most common cause of infiltrates seen on radiographs. Hemodynamic instability and hypoxia may suggest pulmonary embolism. Heart failure signs or arrhythmias may point to ischemia or inflammatory myocarditis.
Systolic murmurs are reported in up to 70% of cases. Murmurs may represent Libman-Sacks endocarditis, superimposed infective endocarditis, thromboembolic disease, fever, hypoxia, or anemia.
Pulmonary hypertension, vasculitis with digital infarcts, and splinter hemorrhages may be observed.
Pericarditis has an incidence of 20-30% and is the most common presentation of heart involvement. It is usually associated with small effusions, but it may involve larger effusions when uremia is concomitant. Myocarditis can cause heart failure, arrhythmias, and sudden death.
Gastrointestinal findings
Abdominal tenderness and pain may be observed in peritonitis, pancreatitis, mesenteric vasculitis, or non–lupus-related processes. Lupus peritonitis is a less-common serositis that may be present, even in the absence of ascites.
Eye findings
Funduscopic examination is important in patients with visual complaints. Retinal vasculitis can lead to blindness and is demonstrated by sheathed narrow retinal arterioles with white exudates adjacent to the vessels. SLE-associated optic neuritis is uncommon, but should be considered as well in those patients with severe vision loss.[42]
http://emedicine.medscape.com/article/332244-clinical#showall