Embed Size (px)
Citation preview

sixteenThe Hand and WristJohn D. Lubahn, MDD. Patrick Williams, DO

Chapter 16
ANATOMY AND BIOMECHANICSThe carpus, or wrist, is composed of eight
carpal bones that link the forearm to the hand(Figure 16-1). The proximal carpal row(scaphoid, lunate, and triquetrum) articulateswith the distal radius and ulna, as well as thedistal carpal row (trapezium, trapezoid, capi-tate, and hamate). The pisiform, also part ofthe proximal row, is a sesamoid bone in theflexor carpi ulnaris tendon that articulatesonly with the triquetrum. The bones of thehand are the metacarpals and phalanges. The
carpometacarpal (CMC) joint of the thumb issaddle-shaped, a configuration that permitsabduction-adduction, as well as the circum-duction that permits opposition of the thumbto the fingers. The metacarpophalangeal(MP), proximal interphalangeal (PIP), and dis-tal interphalangeal (DIP) joints basically areflexion-extension hinge joints.
The skin on the dorsal surface of the hand isthin and flexible to allow full flexion of the fin-gers, whereas the palmar surface skin isthicker and characterized by creases. The
The human hand, as an extension of the brain, allows us to manipulate and in-teract with our environment and to perform activities as routine as opening adoor or as intimate as caressing a loved one. The hand also functions as part ofthe sensory system, providing tactile sensation for complex hand movementswithout the necessity of constant visual guidance; this function is epitomized
by blind people who read and musicians who entertain. An understanding and careful ex-amination of hand anatomy and function is crucial for the student of medicine.
336
Carpalbones
Lunate
Triquetrum
Pisiform
Capitate
Hamate andHook
BaseShaftsHead
BaseShaftsHead
BaseShaftsHead
BaseShafts
TuberosityHead
Right hand:anterior (palmar)view Sesamoid
bones
Carpalbones
Metacarpal bones
Proximal phalanges
Middle phalanges
Distalphalanges
1
2345
ScaphoidandTubercle
TrapeziumandTubercle
Trapezoid
Figure 16-1: Bones and Joints of Hand

The Hand and Wrist
distal volar crease of the wrist crosses theproximal scaphoid and the pisiform. The distalpalmar crease of the hand corresponds to theMP joint, and the proximal finger crease is atthe base of the proximal phalanx.
The extrinsic muscles of the wrist and handoriginate on the medial and lateral humeralcondyles and the proximal radius and ulna(see Figure 15-2). The extrinsic extensor ten-dons cross the wrist and are surrounded bytendon sheaths in six compartments boundedby the extensor retinacular ligament (Figure16-2). The extrinsic finger and thumb flexortendons and the median nerve enter the handthrough the carpal canal (Figure 16-3). Thetransverse carpal ligament, a thick band ex-tending from the hamate and pisiform to thescaphoid and trapezium, forms the inelasticroof of the carpal canal. A decrease in the sizeof the canal or an increase in the size of itscontents can cause compression of the me-dian nerve (carpal tunnel syndrome).
Intrinsic musculature includes thenar, hy-pothenar, and interosseous muscles (Figure16-4; see also Figures 15-4 and 15-5). Thethenar muscles are the abductor pollicis brevis, the opponens pollicis, and the superfi-cial head of the flexor pollicis brevis. The hy-pothenar muscles are composed of the ab-ductor digiti quinti, the opponens digiti quinti,and the flexor digiti quinti. The dorsal interos-sei, commonly referred to as dorsal intrinsics,abduct the fingers; the palmar interossei (pal-mar intrinsics) adduct the fingers.
The DIP joint of the fingers is flexed by theflexor digitorum profundus (FDP). It has a sep-arate muscle belly for the index finger (whichtherefore flexes independently) but a com-mon muscle belly for the long, ring, and smallfingers (which tend to work as a single unit).The PIP joint of the fingers is primarily flexedby the flexor digitorum superficialis (FDS). Ithas individual muscle bellies for each finger,thus providing the individual finger flexion atthe PIP joint that is necessary for activitiessuch as playing a musical instrument and typ-ing. The FDS separates into two parts beforeits point of insertion, and the FDP passesthrough the split (Figure 16-5). Both finger
flexors are enclosed in a common tendonsheath. The proximity of the FDS and FDP ten-don to the surrounding sheath promotes effi-cient movement, but adhesions from injury orinfection can be problematic in this region.
The interossei, along with the lumbricalmuscles, flex the MP joints and extend the PIPand DIP joints. The lumbrical muscles areunique in that they originate from the profun-dus tendons to insert into the dorsal appara-tus of the antagonistic extensor mechanism(see Figure 16-5). The interossei and the twoulnar lumbricals are innervated by the ulnarnerve, but the two radial lumbricals are inner-vated by the median nerve.
The MP joints of the fingers are extendedby the extensor digitorum longus, extensor in-dicis proprius, and extensor digiti quinti.When the MP joints are flexed, these musclesalso can extend the PIP joints; otherwise, theintrinsic muscles extend the PIP and DIPjoints. The complex arrangement of the ten-dons on the dorsum of the hand provides thenecessary synchrony and balance betweenflexors and extensors during the multiple pre-cise motions of the MP, PIP, and DIP jointsworking in concert. The main insertion of theextrinsic extensor muscle tendon is throughthe central slip at the base of the middle pha-lanx. The intrinsic muscles join with the ex-trinsic extensor through the interdigitatingtransverse and oblique fibers of the dorsal ap-paratus to extend the PIP and DIP joints.
Contracture or spasticity of the intrinsicmuscles creates increased tension on the dor-sal hood. A swan-neck deformity develops,with PIP joint hyperextension and MP andDIP joint flexion (Figure 16-6). Laceration ofthe central extensor tendon proximal to its in-sertion into the middle phalanx allows the lat-eral bands to slip volarly and produces the op-posite flexion, boutonnière (French from“button hole”) PIP joint deformity.
The radial artery lies radial to the flexorcarpi radialis tendon at the wrist (see Figure16-3). After crossing the snuffbox (see Figure16-2), the radial artery passes through the firstintermetacarpal space to the palm as themain contributor to the deep palmar arch,
337

Chapter 16
338
Posterior (dorsal) view
Extensor carpi ulnaris – Compartment 6
Extensor digiti minimi – Compartment 5
Extensor digitorumExtensor indicis
Extensor pollicis longus – Compartment 3
Extensor carpi radialis brevisExtensor carpi radialis longus
Abductor pollicis longusExtensor pollicis brevis
Radial artery inanatomical snuffbox
Dorsal interosseous muscles
Compartment 4
Compartment 2
Compartment 1
Extensor retinaculum
Abductor digitiminimi muscle
Intertendinousconnections
Transverse fibers ofextensor expansions (hoods)
Cross section of most distal portion of forearm
Extensor retinaculumExtensor pollicis longus – Compartment 3
Extensor carpiradialis brevisExtensor carpiradialis longus
Compartment 2
Extensorpollicis brevisAbductorpollicis longus
Compartment 1
Extensor digitorum andextensor indicis
Extensordigiti minimi
Extensorcarpi
ulnaris
Compartment 4
Compartment 5
Compartment 6
Ulna Radius
Plane of cross sectionshown below
6
54 3 2
1
Figure 16-2: Extensor Tendons at the Wrist

The Hand and Wrist
339
Figure 16-3: Flexor Tendons, Arteries, and Nerves at Wrist
Radialartery
Radius Ulna
Abductor digitiminimi muscle
Dorsal view
Palmar view
Tendinous slips tohood of extensordigitorum muscle
Deep transversemetacarpalligament
Palmarinterosseous
muscles
RadiusUlna
Dorsalinterosseousmuscles
Abductorpollicis
brevis muscle
Figure 16-4: Intrinsic Muscles of Hand
Palmaris longus tendon
Median nerve
Radial arteryFlexor carpi radialis
tendonFlexor pollicis longus
tendon in tendonsheath (radial bursa)
Palmar carpal ligament (reflected)(Synovial) tendon sheath
Transverse carpal ligament
Trapezium
1st metacarpal bone
Opponens pollicis muscle
Abductor pollicisbrevis muscle
(reflected)
Flexor pollicis brevismuscle (reflected)
Adductor pollicis muscle
Median duo
Radial trio
Flexor digitorumsuperficialis tendons andflexor digitorum profundustendonsCommon flexor sheath(ulnar bursa)
Ulnar trio
Ulnar arteryUlnar nerveFlexor carpi ulnaristendon
Pisiform
Abductor digiti minimi muscle
Flexor digiti minimi brevis muscle
Opponens digiti minimi muscle
Superficial palmar (arterial) arch
Lumbrical muscles
Twotendonquartets
Palmar view

Chapter 16
340
Insertion of extensor tendon
to base of middle phalanx
Triangular
aponeurosis
Slips of long
extensor tendon
to lateral bands
Dorsal
expansion
(hood)
Long extensor
tendon
Interosseous muscles
Dorsal
view
Insertion of extensor
tendon to base of
distal phalanxLateral
bandsInterosseous muscle
slip to lateral band
Lumbrical muscle Portion of interosseous
tendon passing to base
of proximal phalanx
and joint capsuleLateral view,
finger extended
Insertion of extensor
tendon to middle phalanx
Insertion of
extensor
tendon
to distal
phalanx
Lateral bandDorsal expansion (hood)
Long extensor tendon
Collateral
ligamentsVinculum
breve
Vincula
longaFlexor digitorum
superficialis tendon
Flexor digitorum
profundus tendon Lumbrical muscle
Interosseous muscles
Lateral view,
finger flexed
Insertion of deep portion of
extensor tendon to proximal
phalanx and joint capsule
Palmar ligament
Flexor digitorum
superficialis tendon (cut)
Collateral ligaments
Flexor digitorum
profundus tendon (cut)Lateral band relaxed
in this position;
correct for splinting
of “mallet finger”
Lumbrical muscle Interosseous muscles
Attachment of interosseous
muscle to base of proximal
phalanx and joint capsule
Note: black arrows indicate
pull of long extensor
tendon; red arrows indicate
pull of interosseous and
lumbrical muscles
Meta-
carpal
Meta-
carpal
Figure 16-5: Flexor and Extensor Tendons in Fingers

The Hand and Wrist
341
which is completed by the deep palmarbranch of the ulnar artery. The ulnar arteryand nerve lie radial to the flexor carpi ulnarisand pisiform as they enter Guyon canal andthe palm. The ulnar artery is the main contrib-utor to the superficial palmar arch, which iscompleted by a branch of the radial artery.
After traversing Guyon canal, the ulnarnerve branches into a superficial cutaneousbranch that provides sensation to the ulnar as-pect of the palm and the ulnar one and a halffingers, and a deep motor branch that sup-plies the hypothenar muscles. The ulnar nervethen travels with the deep palmar arch, sup-plying all the interossei, the third and fourthlumbricals, the adductor pollicis, and thedeep head of the flexor pollicis brevis (see Fig-ure 15-4). The median nerve supplies the re-maining thenar muscles and the first and sec-ond lumbricals, and it provides sensation tothe thumb and radial two and a half fingers(see Figure 15-3).
PHYSICAL EXAMINATIONInspect the hand for atrophy of the thenar
muscles (innervated by the median nerve) orhypothenar and intrinsic muscles (innervatedby the ulnar nerve). Intrinsic muscle weakness
causes atrophy between the metacarpals onthe dorsum of the hand. Look at the nails forevidence of pitting or signs of other systemicdisorders. Palpate bony landmarks and anyswelling or osteophytes. At the wrist, the ra-dial and ulnar styloid processes are palpable;the radial styloid is approximately 1 cm distalto the ulnar styloid. The dorsal tubercle at thedistal radius, commonly called Lister tubercle,is palpable. It functions as a pulley for the ex-tensor pollicis longus and is a marker for sur-gical approaches. The pisiform on the volaraspect of the wrist is a landmark for the ulnarnerve and artery.
The zero starting position for determiningwrist motion is the forearm in pronation andthe carpus aligned with the plane of the fore-arm. In young adults, normal wrist motion isapproximately 75°of flexion, 75° of exten-sion, 20° of radial deviation, and 35° of ulnardeviation (Figure 16-7).
Finger joint motion occurs primarily in theflexion-extension plane, with flexion account-ing for most of the motion. The wrist shouldbe in the neutral position when finger orthumb flexion is measured. When the wrist isflexed, the extensor digitorum communis andthumb extensors are under tension, therebylimiting finger and thumb flexion. Flexion andextension can be measured at the MP, PIP,and DIP joints, but from a functional perspec-tive, finger flexion is a composite movementof motion from the three finger joints. Ask thepatient to touch the distal palmar crease. Inyoung and middle-aged adults, the fingertipshould touch this crease. Lack of full fingerflexion can be quantified by measuring thedistance from the fingertip to the distal palmarcrease (see Figure 16-7).
The planes of thumb motion are flexion-extension, abduction-adduction, and opposi-tion. Opposition is a composite motion at theCMC, MP, and interphalangeal (IP) joints thatis critical to daily activities. In disability ratings,opposition is valued as 50% to 60% of thumbfunction. In normal opposition, the tip of thethumb touches the base of the little finger(see Figure 16-7). Impaired opposition can bequantified by measuring the distance from
Boutonnière deformity
of index finger with
swan-neck deformity of
other fingers in a patient
with rheumatoid arthritis
Figure 16-6

Chapter 16
342
90˚ 75˚
Extension
90˚ 75˚
Flexion
90˚ 90˚
20˚0˚
30˚
Radialrotation
Ulnardeviation
Range of Finger Flexion Distal palmar crease
MP joint
PIP joint
DIP joint
CMC joint MP joint
IP joint
Range of Thumb Opposition
Distal palmarcrease
Normal finger flexion is composite of flexion of MP, PIP, and DIP joints and allows fingertip to touch distal palmar crease.
Normal thumb opposition is composite of movements of CMC, MP, and IP joints. Normal range is to base of little finger.
Limitation of finger flexion may be quantified by measuring distance from fingertip to distal palmar crease.
Limitations of thumb opposition may be quantified by measuring distance from tip of thumb to base of little finger.
0˚
Wrist Range of Motion Deviation
Figure 16-7: Measurement of Wrist Motion and Finger Motion,Lack of Finger Flexion, and Thumb Opposition

The Hand and Wrist
the tip of the thumb to the base of the littlefinger.
All thumb joints move in flexion and exten-sion, but this range is difficult to quantify atthe CMC joint. Flexion at the thumb MP jointis typically 50° to 60°. Extension is not typi-cally observed at the thumb MP joint. Normalthumb IP motion in young adults is 55° to75°of flexion and 5° to 10°of extension.
To assess the strength of the wrist flexors,the most powerful of which is the flexor carpiulnaris, resist the patient’s effort to flex thewrist with the elbow flexed to 90° and thethumb and fingers in the extended, neutralposition (eliminates action of finger flexors).To test the wrist extensors, the most powerfulof which are the extensor carpi ulnaris and theextensor carpi radialis brevis, resist the pa-tient’s effort to extend the wrist with the el-bow flexed to 90° and the fingers flexed(eliminates action of the finger extensors). Totest the integrity of the FDP tendon, hold thePIP joint in extension, and ask the patient toflex the distal phalanx. To assess the flexor dig-itorum sublimis, neutralize the profundus ten-don by holding all the fingers except the onebeing tested in full extension, and ask the pa-tient to flex the finger.
Median nerve paralysis above the elbowcauses weak pronation, wrist flexion, and an“ape hand” with thenar atrophy and weak-ness of thumb opposition. Thenar musclestrength (motor branch of median nerve) can
be evaluated by asking the patient to positionthe thumb in abduction as you push it into ad-duction. Assess sensation of the mediannerve at the volar tip of the thumb.
Test intrinsic muscle weakness (motorbranch of ulnar nerve) by asking the patient toabduct the index finger against resistancewhile you palpate the first dorsal interosseousmuscle. In addition, ask the patient to pinch apiece of paper while you pull on it. Weaknessof the adductor pollicis results in flexion of theIP joint of the thumb (positive Froment sign)(Figure 16-8). Assess ulnar nerve sensation atthe volar tip of the little finger. If ulnar nerveentrapment or laceration occurs above thewrist, sensation may be lost on the dorsum ofthe hand.
If the ulnar nerve is divided distal to themid-forearm, all the intrinsic muscles of thehand are paralyzed except for the first andsecond lumbricals and the thenar muscles.Lack of intrinsic muscle function to the ringand little fingers causes an ulnar claw hand, orhand of benediction, with the fourth and fifthfingers hyperextended at the MP joints andflexed at the PIP and DIP joints (Figure 16-9).The intact lumbricals to the index and long fin-gers provide enough intrinsic muscle functionto prevent clawing of these digits. However, ifthe ulnar nerve is lacerated at or proximal tothe elbow, clawing of the ring and little fingersdoes not occur because the FDP to thesefingers is also paralyzed. A distal forearm
343
When pinching a piece of paper between thumb and index finger, the thumb IP joint will flex if the adductor pollicis muscle is weak (ulnar nerve paralysis).
Figure 16-8: Positive Froment Sign

Chapter 16
laceration of the median and ulnar nerves re-sults in a complete claw hand because all in-trinsic muscles are paralyzed, but the extrinsicflexors and extensors are intact.
DEGENERATIVE DISORDERSOsteoarthritis
Osteoarthritis may affect any joint of thehand. It is common in the DIP and PIP joints ofthe fingers with normal aging—a process thatusually begins earlier and is more severe in fe-males. Heberden nodes (in the DIP joints)and Bouchard nodes (in the PIP joints) areprominences caused by osteophytes anddeformation of the joints (see Figure 4-7). Adegenerative cystic lesion, referred to as amucous cyst, may be present on the dorsumof the DIP joint. The joints may be painful andstiff early in the process, but the pain usuallysubsides over time. Although the stiffness andnodules remain, surgical treatment (arthrode-sis) of these joints is not commonly required.
Osteoarthritis of the thumb CMC joint iscommon and affects women more often thanmen. Predisposing factors are ligamentous lax-ity and repetitive stress from pinch maneuversthat load the joint (eg, knitting or cutting). Pa-tients report pain with pinch activities. Exami-nation shows swelling and pain over the CMC
joint that are exacerbated by axial pressure ofthe metacarpal on the trapezium (the grindtest). Radiographs show narrowing of the jointand varying degrees of subluxation of the joint(Figure 16-10). Nonoperative treatment alter-natives include activity modification, non-steroidal anti-inflammatory drugs (NSAIDs),short-term full-time splinting followed by inter-mittent bracing, and steroid injections. Recon-structive operations are indicated in patientswith persistent, disabling symptoms.
Osteoarthritis of other joints in the hand andwrist is uncommon and usually is secondary totrauma. Predisposing injuries in traumatic wristarthropathy include intra-articular fractures ofthe distal radius, unrecognized scaphoid frac-tures, and ligament disruptions that causeabnormal wrist kinematics.
Kienböck DiseaseOsteonecrosis of the lunate, commonly re-
ferred to as Kienböck disease, can occur at anyage but most commonly affects men betweenthe ages of 20 and 40 years. The exact cause isusually not known, but repetitive or single-episode trauma that interrupts the blood sup-ply to a “lunate at risk” is the most acceptedtheory. Risk factors include a lunate suppliedby a single nutrient vessel, which occurs in 7%of the population, and ulnar negative variance(an ulna shorter than the radius). Studies haveshown increased contact stress at the radiolu-nate in patients with negative ulnar variance;however, osteonecrosis of the lunate alsooccurs in patients with positive ulnar variance.
Patients with Kienböck disease typicallypresent with the insidious onset of wrist painthat is increased with activity. Examinationshows variable limitation of wrist motion andmild swelling on the dorsum of the wrist. Rou-tine radiographs are usually diagnostic (Fig-ure 16-11). If no changes are apparent in thelunate, a bone scan or magnetic resonanceimaging (MRI) may be diagnostic.
Treatment is based on the stage of diseaseand the degree of disability. Immobilizationmay be successful if the lunate has notcollapsed; however, the effect of immobi-lization on the natural history of the disease
344
Figure 16-9: Hand of Benediction

The Hand and Wrist
is unclear. Surgical options for patients withno collapse or with some collapse of thelunate but no degenerative changes in theadjacent joints include vascular pedicletransplantation, radial shortening osteo-tomy, ulna-lengthening osteotomy, and
capitate-shortening osteotomy. Surgicaloptions for patients with arthritic changes in-clude limited carpal arthrodesis, resectionarthroplasty with interposition of tendongraft or silicone implant, proximal rowcarpectomy, and wrist arthrodesis.
345
Figure 16-10: Osteoarthritis of Thumb Carpometacarpal Joint
A
B
C
(A) Lateral radiograph and (B) AP radiograph of thumb of 56-year-old male with activity-related pain at base of thumb.Radiographs show early stages of disease with narrowing of thumb CMC and mild subluxation. (C) AP radiograph ofhand of 73-year-old female with severe pain at base of thumb. Exam showed swelling and tenderness to palpation atthe base of the thumb. Radiographs show subluxation and degenerative changes at the thumb CMC joint with a largeosteophyte between the first and second metacarpal. The joint space between the scaphotrapezial was preserved.

Figure 16-11: Radiograph inKienböck Disease
Chapter 16
Tendinitis of the Hand and WristTendinitis (tendinosis) of the hand and wrist
is common. The most common etiology ispredisposing anatomic factors such as a nar-row canal for the tendon exacerbated byoveruse. Fortunately, most patients respondto nonoperative treatment, including modifi-cation of activities, short-term immobilization,NSAIDs, and judicious injections of steroids.
Stenosing tenosynovitis of the finger orthumb flexors, better known as trigger finger, isthe most common cause of hand tendinitis.Bow stringing of the flexor tendons and its re-sultant mechanical disadvantage is preventedby five annular and three cruciate pulleys. Thefirst annular pulley may become thickened,causing snapping or locking of the tendon dur-ing flexion of the finger or thumb. Predisposingfactors include diabetes mellitus, rheumatoidarthritis, and aging.
Patients note pain and catching when mov-ing the finger, as well as a nodule in the distalpalm that moves with flexion and extension.
The finger may lock or stick with flexion of thedigit (Figure 16-12). On awakening, the digitmay be locked in the palm and unlocking thedigit may require that the finger be pushedinto extension. Patients with diabetes mellitusor rheumatoid arthritis may have multipledigit involvement.
Injection of corticosteroid into the tendonsheath is often successful as an initial treat-ment for trigger finger; however, patients withdiabetes mellitus are less likely to improve af-ter an injection. If symptoms persist, releaseof the A1 pulley is indicated (see Figure 16-22).
De Quervain tenosynovitis, the most com-mon cause of tendinitis on the extensor sideof the wrist, involves swelling or stenosis ofthe first dorsal compartment tendon sheath,which surrounds the extensor pollicis brevisand the abductor pollicis longus. It most com-monly occurs in patients who have (1) one ormore additional anomalous tendons withinthe compartment, or (2) a septum withinthe compartment that separates and narrowsthe space for the extensor pollicis brevis andthe abductor pollicis longus. This disordermost commonly occurs in middle-agedwomen and is frequently brought on by repet-itive thumb motion.
Tenosynovitis constricts the tendons asthey glide within the sheath. Patients notepain and swelling in the region of the radialstyloid that are aggravated by use of thethumb (Figure 16-13). Crepitus may besensed as the compartment is palpated dur-ing thumb motion. The Finkelstein test is diag-nostic with exacerbation of pain when thethumb is flexed and the wrist is then placed inulnar deviation. Radiographs are typically nor-mal and are used to exclude other possibili-ties, such as fracture of the scaphoid or arthri-tis of the wrist or thumb CMC joint.
Treatment begins with immobilization ofthe thumb in a splint, as well as the use ofNSAIDs. If this treatment fails, a cortico-steroid injection into the tendon sheath is in-dicated. Surgical treatment to release the areaof stenosis is indicated for relief of persistentsymptoms. Anomalous slips of the abductor
346
Radiograph of wrist shows characteristic sclerosis of lunate.

The Finkelstein test exacerbates the pain; it is performed by flexing the thumb and then placing the wrist in ulnar deviation.
Course of abductor pollicis longus and extensor pollicis brevis tendons through 1st compartment of extensor retinaculum, transverse incision, and relation of sensory branches of radial nerve and synovial sheaths.
Superficial branchof radial nerve
Skin incisionExtensor retinaculum
Extensor pollicis longus,extensor pollicis brevis,
abductor pollicis longustendons.
Point of exquisite tenderness over styloid process of radius and sheath of involved tendons.
Figure 16-13: De Quervain Tenosynovitis
The Hand and Wrist
347
Inflammatory thickening of fibrous sheath (pulley) of flexor tendons with fusiform nodular enlargement of both tendons.
Patient unable to extend affected finger. It can be extended passively, and extension occurs with distinct and painful snapping action. Circle indicates point of tenderness where nodular enlargement of tendons and sheath is usually palpable.
Figure 16-12: Trigger Finger

Chapter 16
pollicis longus are commonly noted. Themost dorsal tendon of the compartmentshould be identified as the extensor pollicisbrevis; otherwise, a separate septum for thistendon may be overlooked. Complications ofsurgery include failure to completely decom-press all tendons within the sheath, and injuryto the superficial radial nerve.
Other potential, but less common, areas ofwrist tendinitis include the flexor carpi radi-alis, extensor pollicis longus (third compart-ment), extensor digitorum communis (fourthcompartment), extensor digiti minimi (fifthcompartment), and extensor carpi ulnaris(sixth compartment).
Dupuytren DiseaseDupuytren disease is contracture of the
palmar fascia. The pathologic process beginswith a proliferation of fibroblasts and type IIIcollagen to produce cords and nodules in thedermis and skin. Predisposing factors includemale gender, alcoholism, epilepsy, diabetesmellitus, HIV infection, trauma, and possiblysmoking. A genetic, autosomal dominant pre-disposition has been noted; penetrance isvariable, however, as indicated by the factthat the family history is positive in less than10% of affected patients.
The disease is uncommon before 40 yearsof age. A typical presentation is a 40- to 65-year-old patient who notices a painless nodulenear the distal palmar crease on the ulnar sideof the hand. The cords initially may be tenderand may occur in other locations. The nodulesmay remain confined to the palm and causefew symptoms. However, the disease may ex-tend into the fingers, with progressive, albeitvariable, flexion contracture of one or moredigits at the MP and, in more severe cases, thePIP joints (Figure 16-14). The ring finger ismost often involved, followed by the little,long, thumb, and index fingers. Concomitantinvolvement of the plantar fascia, the fascia ofthe penis, or both occurs in less than 3% ofindividuals with Dupuytren disease.
Early treatment of a nodule in the palm con-sists of reassurance that no surgery is neededunless the contracture progresses to func-tional impairment. Splinting is ineffective. Re-cent research on collagenase injections hasshown promising results. Surgery is indicatedfor significant contractures that interfere withextension of the fingers and functional activi-ties such as retrieving objects from a pocket.The goals of surgical treatment are to excisethe diseased tissue and release the contrac-tures; however, the procedure is technically
348
Flexion contracture of 4th and 5th fingers (most common). Dimpling and puckering of skin. Palpable fascial nodules near flexion crease of palm at base of involved fingers with cordlike formations extending to proximal palm.
Partial excision of palmar fascia. Proximal portion of fascia divided and freed via thenar incision, then drawn up into palmar incision, where it is further dissected with care to avoid neurovascular bundles. Dissection is then continued into fingers. Buttonholing of skin must be avoided. Nodules and cordlike fascial thickening are apparent.
Figure 16-14: Dupuytren Disease

The Hand and Wrist
demanding and may be complicated bynerve injury, skin slough, and recurrentcontractures.
Ganglia of the Hand and WristThe most common benign tumor of the
hand and wrist is a ganglion. These cystic le-sions contain a thick, yellowish, mucinousfluid with a composition similar to joint fluid.Ganglia are thought to arise from the degen-eration or tearing of a joint capsule or tendonsheath, which creates a one-way valvethrough which synovial fluid can enter thecyst but cannot easily flow back. The mostcommon age at presentation is 15 to 40years, but ganglia also develop in childrenand older adults.
Ganglia may develop at any site. The mostcommon location is the dorsoradial aspect ofthe wrist over the scapholunate joint (Figure16-15). The lump may be asymptomatic ormay cause aching that is aggravated by activ-ities requiring repetitive wrist movements. Ex-amination reveals a firm, cystic mass thattransilluminates when a penlight is pressedagainst its side. The second most commonsite of ganglia is the volar radial aspect of thewrist between the flexor carpi radialis and the
radial styloid. These ganglia originate fromthe capsule of the scaphotrapezial joint andmay wrap around the radial artery.
A volar retinacular ganglion of the flexor ten-don sheath typically is just proximal to the MPflexion crease of the finger. This “seed gan-glion” is a small, firm nodule that is frequentlytender when gripping objects, but does notlimit or move with finger flexion/extension. Mu-cous cysts, a type of ganglion, develop at os-teoarthritic DIP joints and most commonly arelocated on either side of the extensor tendon.
Treatment options include observation, as-piration, and surgical excision. Ganglia mayspontaneously recede, and observation is ap-propriate for patients with minimal symp-toms. Aspiration is often successful in thetreatment of volar retinacular ganglia, may beuseful in the treatment of dorsal wrist ganglia(although recurrence rates are high), and isused with caution in volar wrist ganglia or mu-cous cysts. Surgical excision includes the jointcapsule attachments. The risk of recurrenceafter surgery is 5% to 10% if the procedure iscombined with 2 weeks of immobilization.Mucous cyst excision at the DIP joint requirescareful removal of the cyst and any associatedosteophytes.
349
Firm, rubbery, sometimes lobulated swelling over carpus, most prominent on flexion of wrist. Broken line indicates line of skin incision.
Excision of ganglion via transverse incision
Extensor tendon retracted
Carpal ligaments and capsule
Figure 16-15: Ganglion of Wrist

Chapter 16
NERVE ENTRAPMENT SYNDROMESAT THE WRIST
For signs and symptoms of nerve entrap-ment syndromes at the wrist, see Chapter 6.Carpal tunnel syndrome is most common inmiddle-aged or pregnant women. The syn-drome is often idiopathic, but predisposingfactors that reduce available space in thecarpal tunnel or affect peripheral nerve func-tion should be investigated. These factors in-clude tenosynovitis of the adjacent flexortendons due to rheumatoid arthritis oroveruse syndrome; edema resulting frompregnancy or hypothyroidism; and peripheralneuropathy caused by diabetes mellitus, al-coholism, or other conditions. The differen-tial diagnosis includes cervical radiculopathythat affects the C6 nerve root, median nerveentrapment at the elbow, ulnar entrapmentat the wrist, and wrist arthritis.
Ulnar nerve entrapment at the wrist inGuyon canal is less common than ulnar en-trapment at the elbow. Predisposing factorsinclude a space-occupying lesion (such as aganglion) or repetitive trauma (such astrauma produced by operating a jackham-mer, or that caused by repetitive pressure as-sociated with extended crutch ambulation).The differential diagnosis includes cervicalradiculopathy that affects the C8 nerve root,thoracic outlet syndrome, ulnar nerve entrap-ment at the elbow, carpal tunnel syndrome,and wrist arthritis. More proximal entrapmentof the ulnar nerve or C8 nerve root typicallycauses numbness of the dorsum of the hand.
BITE WOUNDS OF THE HANDDog, cat, and human bites account for ap-
proximately 1% of all emergency room visits.Dog bites account for approximately 80% to90% of animal bites, but only 10% of woundsfrom dog bites become infected. In contrast,approximately 30% to 50% of wounds fromcat bites become infected, most likely be-cause the sharp, needlelike teeth of cats injectbacteria deep into the tissues. The causativeorganisms of dog and cat bite infections aresimilar. Pasteurella multocida is found in 50%of wounds from cat bites and in some dog
bite wounds. Other bacteria commonlyfound in dog and cat bite wounds include a-hemolytic streptococci, Staphylococcus aureus, Bacteroides species, and Fusobac-terium species.
Human bite wounds often occur at the fin-gers (a direct injury) or MP joints (an indirect,clenched fist injury). Because the circum-stances of the injury are often embarrassingand the laceration is often small, patients com-monly delay evaluation. As a result, many pa-tients with human bite wounds do not presentuntil a well-established infection has devel-oped. Gram-negative, anaerobic organisms—particularly Eikenella corrodens—are commonin human bite wounds.
Examination should assess location,swelling, erythema, and purulent discharge.Evaluate possible tendon or neurovasculardysfunction. Provide appropriate tetanus pro-phylaxis, and débride necrotic tissue. Mostbite wounds should not be closed primarily.Pending culture results, treat animal biteswith oral or intravenous ampicillin-sulbactam.Penicillin and a cephalosporin are the stan-dard initial antibiotic therapy for human bitewounds.
UNIQUE HAND INFECTIONSThe flexor tendons of the fingers and
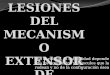
thumb are surrounded by a tenosynovialsheath that extends from the distal palm tothe DIP joint (Figure 16-16; also Figure 16-22). Infections within this sheath usually de-velop from a puncture wound. Because thesheath is a closed space with limited bloodsupply, an infection rapidly becomes an ab-scess. The sheath of the thumb and little fingerflexor tendons extends to the radial and ulnarbursae, so infections in these tendon sheathshave the potential for extension into the fore-arm.
Patients with septic flexor tenosynovitis de-velop progressive pain and swelling of thedigit 24 to 48 hours after injury. Examinationreveals diffuse swelling of the finger, maximaltenderness over the tendon, a finger held in asemiflexed position, and marked increasedpain on passive extension of the digit. Patients
350
The Hand and Wrist
351
Palmar view of hand
Fascia over adductorpollicis muscle
1st dorsal interosseous muscle
Ulnar arteryand nerve
Common flexorsheath (ulnar
bursa)
5th fingertendinous sheathextends to ulnar
bursa
Insertion offlexor digitorum
superficialis tendon
Insertion of flexor digitorumprofundus tendon Annular and cruciform
parts of fibrous sheathover (synovial) flexortendon sheaths
Recurrent branch of median nerve to
thenar muscles
For severe and longstanding purulent flexor tenosynovitis, open
drainage and débridement is done by zigzag volar incision.
Tendon sheath is opened by reflecting cruciate pulleys and
preserving annular pulleys. With more prompt diagnosis, closed
tendon sheath irrigation provides drainage while promoting
healing and return of finger motion. An incision is made in the
palm proximal to the A1 pulley. A second midlateral incision is
made distally in the finger and the tendon sheath incised distal to
the A4 pulley. A catheter is inserted into the proximal end of the
tendon sheath and a drain in the distal end. The tendon sheath is
irrigated until all purulent material is removed. Postoperatively,
the catheter is kept in place for approximately 48 hours to allow
intermittent saline irrigation of the tendon sheath.
Figure 16-16: Infections of the Hand

Chapter 16
352
Felon. Line of incision indicated.
Paronychia
Figure 16-17: Felon and ParonychiaInfections
require prompt treatment for prevention oftendon adhesions and necrosis. If the infec-tion is recognized early, parenteral antibiotictherapy that covers both staphylococci andstreptococci may be satisfactory. Most pa-tients, however, require surgical drainage sup-plemented by closed tendon sheath irrigationand appropriate intravenous antibiotics.
The pulp of the fingertip has fibrous septathat provide support for pinching and graspingactivities. These septa create many small com-partments in which a felon (pulp space infec-tion) may develop (Figure 16-17). A felon typ-ically develops after a puncture wound, mostcommonly involves the index and long fingers,and is characterized by intense pain andswelling of the palmar tip of the finger. Un-treated felons progress to osteomyelitis of thedistal phalanx. Surgical drainage can be per-formed through a central incision that extendsfrom the flexion crease to the fingertip whenan abscess collection is identified on the padside of the finger, or through a midaxial inci-sion when the location of the pus is not visible.“Fish mouth incisions” that extend across thetip of the finger cause painful scars and shouldbe avoided. The wound should be packedopen for 24 to 48 hours. The usual infecting or-ganism is S aureus.
Herpetic whitlow, a herpes simplex virus in-fection, can affect the fingertip and may causeswelling that should be differentiated from afelon. Herpetic whitlows have vesicular le-sions and typically have less erythema andswelling than occur with felons. Lesions occurin adults and children and are more commonin medical personnel, who are frequently ex-posed to human saliva. The swelling from aherpetic whitlow resolves within 10 to 21days. Unnecessary surgical drainage predis-poses the patient to secondary infection.
Paronychial infections are the most com-mon hand infections. The paronychia is theskinfold radial and ulnar to the fingernail. Theeponychium is proximal to the nail. Parony-chial infections typically develop from a hang-nail, an ingrown nail, or a poorly performedmanicure; they also may result from fingernailbiting. The infection may involve only one
side of the nail or both sides of the nail and theeponychium (see Figure 16-17). Early-stageinfections may be treated with warm soaksand oral antibiotics that cover S aureus. Later-stage infections require elevation of the skin-fold or partial or complete removal of the nail.
WRIST AND HAND TRAUMAFractures in AdultsFractures of the Distal Radius
When we fall, the most common protectivemechanism involves catching ourselves on anoutstretched, hyperextended hand. As a re-sult, Colles fracture of the distal radius is themost common fracture in adults. This injury ismore common in women and in older adults;after age 50, the female predominance in-creases. Colles fracture begins on the volar as-pect of the distal radius, which fails in tension.The fracture propagates dorsally, and thebone then is loaded in compression. There-fore, Colles fractures typically reveal dorsalcomminution, volar angulation, and dorsal dis-placement of the distal radius (Figure 16-18).
Smith fracture is the opposite of Colles frac-ture and occurs with a backward fall on a
The Hand and Wrist
353
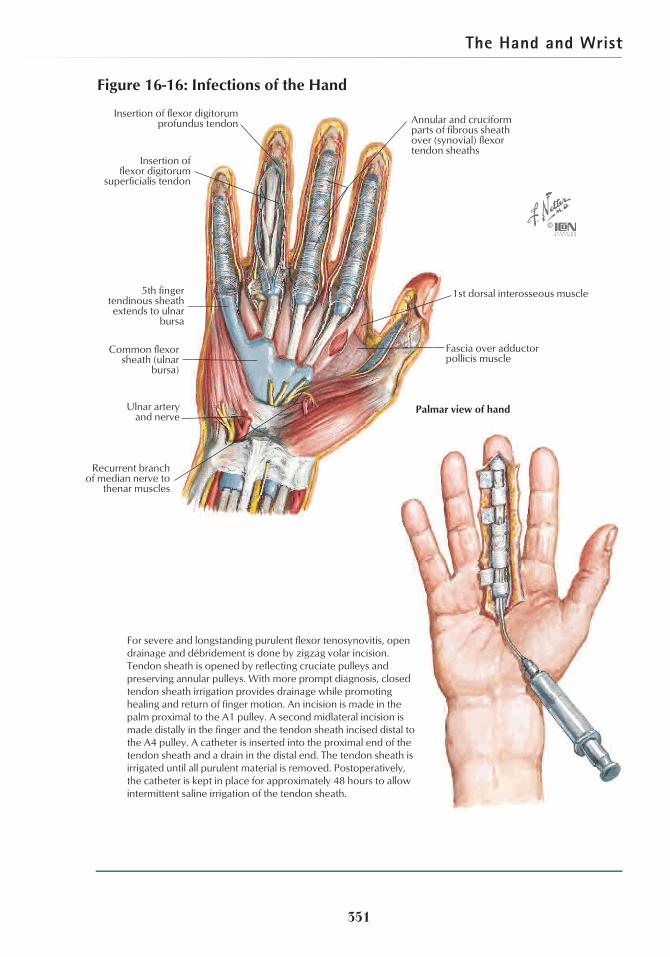
flexed wrist. In these injuries, the distal radius istilted volarly. Barton fracture is a dorsal or pal-mar lip fracture of the distal radius withassociated subluxation of the carpus (see Fig-ure 16-18). A die-punch fracture is an intra-articular, depressed fracture of the distal radiusthat occurs with increased axial compression.A transverse or oblique fracture across the ra-dial styloid (a chauffeur fracture) results from adirect blow to the lateral aspect of the forearm.
Examine the patient to detect swelling anddeformity of the distal forearm, and deter-mine the circulatory and neurologic status ofthe hand. Inspect anteroposterior (AP) and lat-eral radiographs to determine the directionand magnitude of displacement and whetherthe fracture is extra-articular or intra-articular.Median nerve dysfunction is the most com-mon associated injury.
The degree of acceptable displacementvaries according to the age of the person and
whether the fracture is intra-articular or extra-articular. Generally, fractures with 5° to 10°of dorsal angulation, a loss of more than10°of radial inclination, and more than 2 mmof intra-articular step-off should be reducedand stabilized with the use of sugar tongsplints or external or internal immobilizationdevices. Elderly patients with marked os-teopenia and borderline reasons for reduc-tion often function satisfactorily and withfewer complications when treated by short-arm cast or splint immobilization.
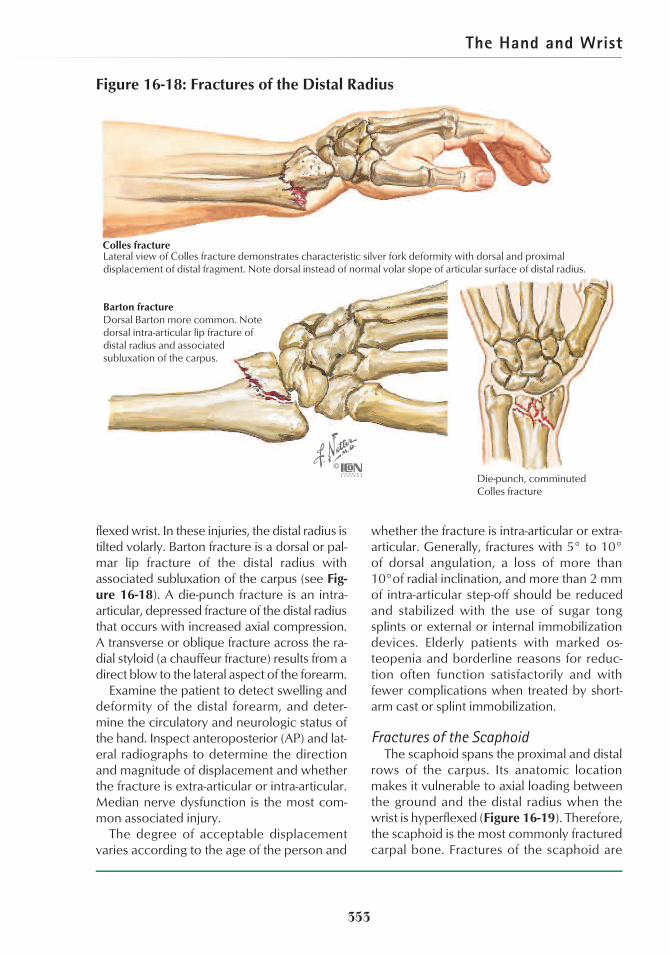
Fractures of the ScaphoidThe scaphoid spans the proximal and distal
rows of the carpus. Its anatomic locationmakes it vulnerable to axial loading betweenthe ground and the distal radius when thewrist is hyperflexed (Figure 16-19). Therefore,the scaphoid is the most commonly fracturedcarpal bone. Fractures of the scaphoid are
Lateral view of Colles fracture demonstrates characteristic silver fork deformity with dorsal and proximal displacement of distal fragment. Note dorsal instead of normal volar slope of articular surface of distal radius.
Barton fractureDorsal Barton more common. Note dorsal intra-articular lip fracture of distal radius and associated subluxation of the carpus.
Die-punch, comminuted Colles fracture
Colles fracture
Figure 16-18: Fractures of the Distal Radius
more common among males; the age groupmost often affected is 15 to 40 years, an ageat which the distal radius is relatively strong.
Scaphoid fractures have an increased inci-dence of nonunion and osteonecrosis for tworeasons. First, the diagnosis is often delayed ormissed. Patients may dismiss the injury as asimple sprain and may not seek medical atten-tion. Furthermore, the radiographic findings ofan acute injury are often subtle and may not beapparent unless routine AP and lateral radio-graphs are supplemented with additionaloblique radiographs. The second reason fornonunion and osteonecrosis is a vulnerableblood supply. Articular cartilage covers 80% ofthe surface of the scaphoid, and the fracturemay interrupt the major blood supply, whichenters the distal pole at the dorsal ridge.
Tuberosity fractures and incomplete waist(middle third) fractures are stable injuries. Un-stable patterns include oblique fractures of thedistal pole, complete waist fractures, and
proximal pole fractures. Displaced fractureshave more than 1 mm of displacement, dorsalangulation, or both. The rate of nonunionmarkedly increases in displaced fractures. Os-teonecrosis is associated with any proximalpole fracture and with displaced waist injuries.
Symptoms include pain and tenderness onthe radial aspect of the wrist localized to theanatomic snuffbox, or pain and tenderness onpressure over the scaphoid tubercle on thepalmar side of the wrist. In addition to routineposteroanterior and lateral radiographs of thewrist, a posteroanterior view with the wrist inulnar deviation and an oblique view shouldbe obtained if examination indicates the pos-sibility of a scaphoid fracture.
If the exam suggests a possible scaphoidfracture but radiographs are not diagnostic,treatment should consist of a short-arm castthat includes the thumb for 2 weeks and re-peated radiographs. Treatment for acute, sta-ble fractures is a short-arm, thumb-spica cast
Chapter 16
354
Usually caused by fall on outstretched hand with impact on thenar eminence.
Lunate
Scaphoid (fractured)
Trapezium
Trapezoid
Triquetrum
Pisiform
Hamulus (hook) of hamate
Capitate
Less commonfractures
Tubercle
Distal pole
Proximal pole
Fracture of middle third (waist) of scaphoid (most common).
withC.A. Luce
Figure 16-19: Fracture of Scaphoid
The Hand and Wrist
355
with the wrist in radial deviation. Nondis-placed, unstable fractures can be treated witheither internal fixation or cast immobilizationfor 12 weeks. Reduction and internal fixationis indicated in patients with displaced frac-tures or delayed diagnosis.
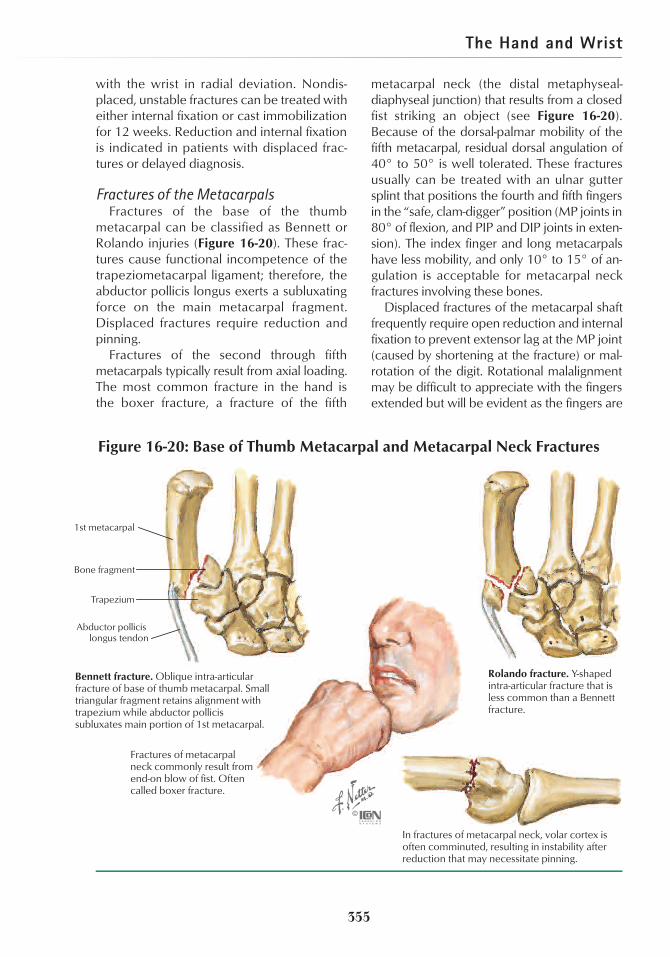
Fractures of the MetacarpalsFractures of the base of the thumb
metacarpal can be classified as Bennett orRolando injuries (Figure 16-20). These frac-tures cause functional incompetence of thetrapeziometacarpal ligament; therefore, theabductor pollicis longus exerts a subluxatingforce on the main metacarpal fragment.Displaced fractures require reduction andpinning.
Fractures of the second through fifthmetacarpals typically result from axial loading.The most common fracture in the hand isthe boxer fracture, a fracture of the fifth
metacarpal neck (the distal metaphyseal-diaphyseal junction) that results from a closedfist striking an object (see Figure 16-20).Because of the dorsal-palmar mobility of thefifth metacarpal, residual dorsal angulation of40° to 50° is well tolerated. These fracturesusually can be treated with an ulnar guttersplint that positions the fourth and fifth fingersin the “safe, clam-digger” position (MP joints in80° of flexion, and PIP and DIP joints in exten-sion). The index finger and long metacarpalshave less mobility, and only 10° to 15° of an-gulation is acceptable for metacarpal neckfractures involving these bones.
Displaced fractures of the metacarpal shaftfrequently require open reduction and internalfixation to prevent extensor lag at the MP joint(caused by shortening at the fracture) or mal-rotation of the digit. Rotational malalignmentmay be difficult to appreciate with the fingersextended but will be evident as the fingers are
1st metacarpal
Bone fragment
Trapezium
Abductor pollicis longus tendon
In fractures of metacarpal neck, volar cortex is often comminuted, resulting in instability after reduction that may necessitate pinning.
Fractures of metacarpal neck commonly result from end-on blow of fist. Often called boxer fracture.
Bennett fracture. Oblique intra-articular fracture of base of thumb metacarpal. Small triangular fragment retains alignment with trapezium while abductor pollicis subluxates main portion of 1st metacarpal.
Rolando fracture. Y-shaped intra-articular fracture that is less common than a Bennett fracture.
Figure 16-20: Base of Thumb Metacarpal and Metacarpal Neck Fractures

Chapter 16
356
partially flexed. A malrotated metacarpal orphalangeal fracture causes the finger to over-lap the adjacent digit. Nondisplaced and mini-mally displaced fractures are common whenonly the third or fourth metacarpal is injured. Inthese injuries, the transverse metacarpal liga-ment stabilizes and suspends the injuredmetacarpal between the adjacent ones.
Fractures of the PhalangesIn adults, the distal phalanx is the most
commonly injured finger bone, followed bythe proximal and middle phalanges. Fracturesof the middle and distal phalanges are oftennondisplaced and may be managed by splint-ing or buddy-taping the injured finger to anadjacent digit. Maintenance of reduction isdifficult in displaced fractures of the proximalphalanx, so these injuries typically require in-ternal fixation (Figure 16-21).
Fractures in ChildrenThe distal third of the forearm is the most
common location for fractures in children.Several patterns of injury may occur (Table16-1). These injuries are relatively uncommonbefore age 4 years and in this age group aremostly torus or greenstick fractures. A torusfracture is the least complicated distal fore-arm fracture and most commonly involvesthe dorsal cortex of the radius (see Figure 10-1). A metaphyseal fracture isolated to thedistal radius is typically minimally displaced.
Most distal forearm fractures in children, in-cluding fractures with complete displacementand shortening, can be treated by closedmeans. Because the distal radial and ulnar physis contribute approximately 80% of fore-arm length, residual angulation typically re-models completely in 1 to 2 years. Loss of ro-tational alignment is the only absolute
Transverse fractures of proximal phalanx tend to angulate volarly because of pull of interosseous muscles on base of proximal phalanx and collapsing action of long extensor and flexor tendons.
Reduction of fractures of phalanges or metacarpals requires correct rotational as well as longitudinal alignment. In normal hand, tips of flexed fingers point toward tuberosity of scaphoid, as in hand at left. Hand at right shows result of healing of ring finger in rotational malalignment. Rotational malalignment, usually discernible clinically, may also be evidenced on radiographs by discrepancy in cross-sectional diameter of fragments, as shown at extreme right. Discrepancy in diameter is most apparent in true lateral radiograph but is visible to some extent in anteroposterior view.
Figure 16-21: Fracture of Proximal Phalanx
The Hand and Wrist
indication for reduction or remanipulation.The reason for reduction is to relieve pressureon adjacent soft tissues and to facilitate heal-ing. Closed reduction generally is indicated forangulation of 10° to 15°.
Fractures of the wrist and hand are uncom-mon in children. The most common suchinjury is a Peterson II (Salter II) physeal frac-ture of the proximal phalanx. This injury mostoften involves the little finger and occurswhen the finger is caught on an object and ispushed in a lateral direction.
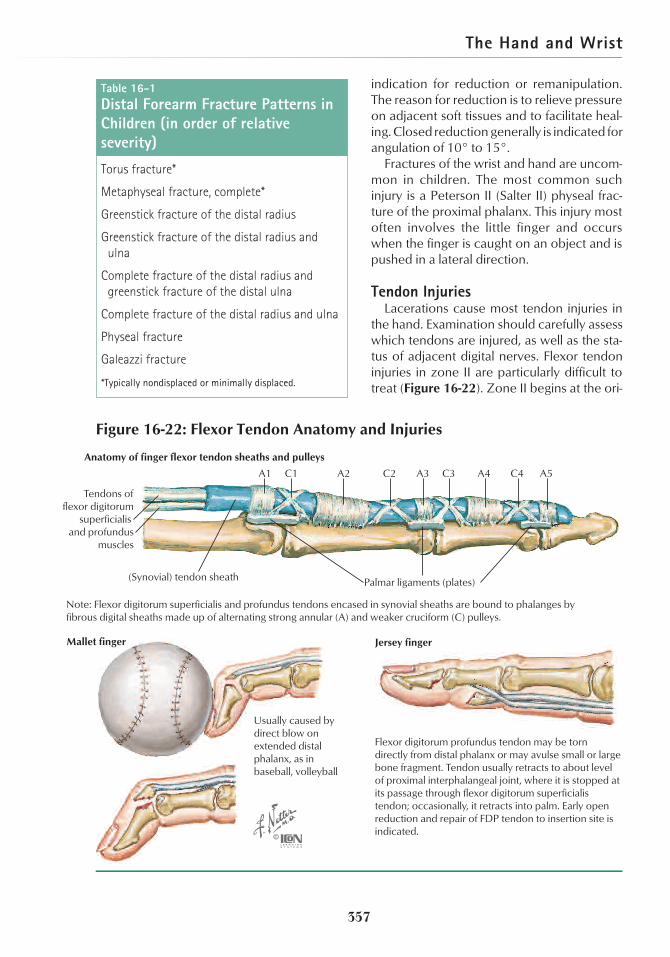
Tendon InjuriesLacerations cause most tendon injuries in
the hand. Examination should carefully assesswhich tendons are injured, as well as the sta-tus of adjacent digital nerves. Flexor tendoninjuries in zone II are particularly difficult totreat (Figure 16-22). Zone II begins at the ori-
357
Torus fracture*
Metaphyseal fracture, complete*
Greenstick fracture of the distal radius
Greenstick fracture of the distal radius andulna
Complete fracture of the distal radius andgreenstick fracture of the distal ulna
Complete fracture of the distal radius and ulna
Physeal fracture
Galeazzi fracture
*Typically nondisplaced or minimally displaced.
Table 16-1Distal Forearm Fracture Patterns inChildren (in order of relativeseverity)
Palmar ligaments (plates)
A2 C2 A3 C3 A4 C4 A5
(Synovial) tendon sheath
Tendons offlexor digitorum
superficialis and profundus
muscles
A1 C1
Mallet finger
Flexor digitorum profundus tendon may be torn directly from distal phalanx or may avulse small or large bone fragment. Tendon usually retracts to about level of proximal interphalangeal joint, where it is stopped at its passage through flexor digitorum superficialis tendon; occasionally, it retracts into palm. Early open reduction and repair of FDP tendon to insertion site is indicated.
Usually caused by direct blow on extended distal phalanx, as in baseball, volleyball
Note: Flexor digitorum superficialis and profundus tendons encased in synovial sheaths are bound to phalanges by fibrous digital sheaths made up of alternating strong annular (A) and weaker cruciform (C) pulleys.
Anatomy of finger flexor tendon sheaths and pulleys
Jersey finger
Figure 16-22: Flexor Tendon Anatomy and Injuries

Chapter 16
gin of the flexor tendon sheath and extends tothe insertion of the FDS. In this zone, both theFDP and the FDS are often lacerated. Lacera-tion may involve the tendons at which theFDS splits to allow passage of the FDP. In ad-dition, injury and repair processes violate thetendon sheath and its associated annular andcruciate pulleys that normally facilitate glidingand nutrition of the tendons. As a result, thesite of injury is often complicated by peri-tendinous adhesions that can seriously com-promise function.
Extensor tendon injuries in the distal fore-arm or wrist often heal well, but lacerationsover the metacarpal head and the dorsum ofthe fingers can be complicated by injury to thesagittal bands and adhesions to surroundingstructures that limit flexion. Both flexor andextensor tendon injuries require meticulousoperative technique and a postoperativerehabilitation protocol that minimizes adhe-sions, contracture, and disruption of the re-paired tendon. The A2 and A4 pulleys must berepaired or preserved to prevent bow string-ing and dysfunction of the flexor tendons.
Avulsion injuries also may disrupt fingertendons. A mallet finger results from forcedflexion of the extended finger (eg, when a ballstrikes the tip of the finger) and subsequentavulsion of the extensor tendon at the distalphalanx (see Figure 16-22). A similar mecha-nism can result in an intra-articular fracture ofthe distal phalanx (bony mallet finger). Exami-nation shows a flexion posture of the DIP jointand an inability to actively extend this joint.Splinting the DIP joint in full extension for 6 weeks if the injury is acute, and for 8 weeksif diagnosis is delayed, is often successful.
Avulsion ruptures of the central slip of theextensor tendon insertion into the middlephalanx result in an inability to fully extendthe PIP joint. If diagnosis is delayed, lateralbands displace below the axis of rotation,resulting in flexion of the PIP joint and hyper-extension of the DIP joint (boutonnière defor-mity; see Figure 16-6). Acute injuries can betreated by splinting of the PIP joint in exten-sion. Chronic injuries may require surgical reconstruction.
Avulsion of the FDP insertion into the distalphalanx usually involves the ring finger (seeFigure 16-22) and occurs when the flexed fin-ger is caught and is forcefully pulled into ex-tension, as when a sports player is graspingthe jersey of another player (“jersey finger”).Examination reveals an inability to flex theDIP joint. Treatment requires operative rein-sertion of the FDP to its bony insertion point.
Ligament Injuries and Dislocations ofthe Hand
Sprains of the hand are common and typi-cally involve a collateral ligament and/or volarplate of the MP, PIP, or DIP joint. Patients notepain and swelling after a jamming type of in-jury. After obtaining radiographs to rule out afracture, assess stability by gently stressing theadjacent ligaments. Most sprains of the hand,even those that demonstrate complete dis-ruption, can be treated with splinting. A digitwith collateral ligament injury can be buddy-taped to an adjacent digit. Complete rupturesof the volar plate are initially splinted in 30°offlexion for 1 to 3 weeks, with transition tobuddy-taping and motion.
Disruption of the ulnar collateral ligamentof the thumb MP joint results from forced ab-duction of the thumb. This injury requires spe-cial consideration because this ligament is animportant stabilizer of the thumb, and the ad-ductor pollicis tendon may become inter-posed between bone and torn ligament, thuspreventing adequate healing. The term game-keeper thumb is used because English game-keepers sustained this injury when they killedrabbits by means of a forceful blow from theirthumb web space to the back of the hare’sneck. The injury is also observed in skiers(from forced abduction of the thumb againstthe ski pole), in sports players (from the ball’sforcing the thumb into abduction), and in per-sons who have fallen (Figure 16-23). Partialinjuries can be treated with cast immobiliza-tion. Complete disruption requires surgicalstabilization.
Finger joint dislocations are typically dorsaland result from hyperextension injuries thatdisrupt the volar plate. Dislocation of the PIP
358

The Hand and Wrist
joint is the most common. MP dislocationsare more common in the thumb and may besimple or complex (interposition of the volarplate between the metacarpal head andthe proximal phalanx). Treatment of a PIP orDIP joint dislocation consists of closed reduc-tion after the administration of a digital blockanesthetic. Distal traction is followed byappropriate volar and dorsal applied pres-sure. Stability should be assessed after reduc-tion. Stable injuries can be buddy-taped.When instability is observed with the jointpositioned in full extension, the finger shouldbe immobilized with a dorsal extensionblock splint. Complex dorsal dislocations ofthe MP joint often benefit from regionalblock anesthesia. These injuries are reducedby pushing the proximal phalanx over themetacarpal rather than by traction. Complexdislocations of the MP joint may require openreduction.
Nail InjuriesNail bed and fingertip injuries are common.
These include simple lacerations, stellate/crushing lacerations, and avulsion injurieswith loss of nail bed tissue. Associated frac-tures of the distal phalanx are common, as isextension of the laceration through the sur-rounding skin and pulp. Various levels offingertip amputation may occur.
The goal of treatment is to prevent hyper-sensitivity of the fingertip and deformity of thenail such as split, ridged, ingrown, or poorlyadherent nails. Assess the extent of injury, in-cluding whether the nail bed laceration in-volves the sterile matrix, germinal matrix, orboth. Obtain AP and lateral radiographs ofthe finger, and note the location and dis-placement of any fractures.
Simple and stellate/crushing lacerationsshould be treated by primary repair using digi-tal block anesthesia, a finger tourniquet, loupemagnification, 6-0 chromic suture for the nailbed, and 5-0 nylon suture for any associatedskin lacerations. If the germinal matrix isavulsed and lying on top of the nail plate, thenail bed should be repositioned and secured inits anatomic position. Loss of nail bed tissue re-quires split-thickness or more complicatedgrafting procedures. Soft tissue loss without ex-posed bone and with a defect of ,1 cm healswell by secondary intention. More compli-cated injuries with bone exposed require theuse of local or regional flaps or shortening ofthe digit with primary closure. Tuft fracturesand nondisplaced fractures of the distal pha-lanx are treated with symptomatic splinting.
PEDIATRIC CONDITIONSSyndactyly
Syndactyly is a congenital condition char-acterized by failure of normal separation ofthe fingers or toes. At a genetically predeter-mined time, production of apical ectodermalridge maintenance factor (AERMF) ceases. IfAERMF continues to be produced, apoptosisand disruption of the interdigital space do notoccur. The degree of syndactyly can varyfrom the presence of a thin web of skin to syn-ostosis (bony fusion) of the phalanges. Thewebbing may extend to the tips of the digits(complete webbing) or may involve only avariable extent of the digit (partial webbing)(Figure 16-24). Syndactyly occurs twice as of-ten in males, is 10 times more common inwhites than in blacks, and most often involvesthe long and ring fingers.
Syndactyly may occur in association withother syndromes. Apert syndrome is an auto-
359
Stress test for ruptured ulnar collateral ligament of thumb (gamekeeper thumb).
Figure 16-23: Gamekeeper Thumb

Chapter 16
somal dominant condition that results in pre-mature closure of the cranial sutures andcomplete, complex syndactyly of the handsand feet. Poland syndrome is a sporadic con-genital deficiency of the pectoralis majorranging from hypoplasia to absence of themuscle that has a 3:1 male and 3:1 right-sidedpredominance. Hypoplasia of the distal up-per extremity and varying degrees of brachy-dactyly and syndactyly may be present.
Because fingers differ in length, angulardeformity may occur, and release before age1 year is recommended for index-thumb andring finger–small finger syndactyly. Long fin-ger–ring finger syndactyly release may be de-layed. The results of surgery are improvedwith a well-designed dorsal commissural flapand liberal use of full-thickness skin grafts. Re-current web space contracture is the mostcommon long-term complication.
PolydactylyPolydactyly is the presence of extra digits on
the hand or foot (Figure 16-25). The conditionis usually postaxial (ulnar to the little finger orlateral to the fifth toe) or preaxial (radial to thethumb or medial to the great toe), but it mayoccur in a central location. Extra digits rangefrom a vestigial digit attached by a narrowbridge of skin to a completely developed digitwith its own metacarpal or metatarsal. Poly-dactyly may occur sporadically or as an auto-somal dominant disorder. It is frequently ob-
served in 16 syndromes and is occasionallynoted in 31 associated conditions.
Polydactyly of the foot usually causes diffi-culty with shoe wear. Even when polydactylyof the hand does not create functional diffi-culties, it causes a significant cosmetic defor-mity. Vestigial digits can be ablated with theuse of a constricting, circumferential suture atthe skin bridge. Otherwise, removal of acces-sory digits should be delayed until the child is9 to 10 months old.
CamptodactylyCamptodactyly (bent fingers) usually
occurs at the PIP joint of the little finger. Theextent of the flexion deformity varies. Ap-proximately 70% of all patients have bilateralinvolvement. Other fingers may be involved,but incidence decreases toward the radialside of the hand. The natural history of un-treated, severe camptodactyly is no improve-ment or a gradual increase in deformity withgrowth.
Camptodactyly may occur in isolation ormay be associated with syndromes. Almostevery conceivable structure has been im-plicated in the pathogenesis of isolated camp-todactyly. Dynamic muscular imbalance isthought to be the primary cause in mostcases. No treatment is uniformly successful,probably because it is difficult to differentiateprimary and secondary contractures. Treat-ment begins with splinting. For the young
360
Figure 16-24: Syndactyly Figure 16-25: Polydactyly
Postaxial Preaxial

The Hand and Wrist
child with persistent PIP joint contractures of40°or greater and no bony changes, soft tis-sue releases are useful.
ClinodactylyClinodactyly is curvature of the finger in the
radial or ulnar plane. The most common de-formity is radial angulation of the little fingersecondary to a delta-shaped middle phalanx.Clinodactyly is more common in males and isusually bilateral. The disorder is frequentlyseen in 30 syndromes and is found occasion-ally in 22 conditions. Isolated clinodactyly isusually simple (no rotation and less than 45°of angulation) and does not require treat-ment. Surgical realignment is indicated whenoverlap of the fingers interferes with grippingof objects.
Hypoplasia/Aplasia of the Thumb andRadial Hemimelia
Radial hemimelia and hypoplasia/aplasiaof the thumb are part of a spectrum of con-genital deletions of the radial portion of theupper limb. Radial hemimelia, also called ra-dial club hand, is characterized by partial orcomplete absence of the radius, variableshortening and bowing of the ulna, radial de-
viation of the hand, variable defects in the ra-dial carpal bones, and variable presence andstiffness of the thumb and index fingers (Fig-ure 16-26). The extent of deficiency is alsovariable in congenital hypoplasia/aplasia ofthe thumb.
Both conditions may be associated withother disorders, including congenital heartdisease (Holt-Oram syndrome), craniofacialabnormalities, vertebral anomalies (VATER as-sociation), and Fanconi anemia. TAR syn-drome (thrombocytopenia with absent ra-dius) is unique because in this syndrome,the thumb is normal. In other syndromes, if theradius is deficient, the thumb is also hypoplas-tic or absent.
Operative management is based on theseverity of the deficiency. Reconstructiveprocedures are indicated when the hypoplas-tic thumb is adequately sized and the CMCjoint is stable. Transfer of the index fingerto the position of the thumb (index polliciza-tion) is used in the treatment of severe thumbhypoplasia/aplasia. In patients with radialhemimelia, procedures to centralize the handare performed at approximately 1 year of age,except when a short forearm and limited el-bow motion are present.
361
Short, bowed forearm with marked radial deviation of hand. Thumb absent. Radiograph shows partial deficit of radial ray (vestige of radius present). Scaphoid, trapezium, and metacarpal and phalanges of thumb absent.
Figure 16-26: Paraxial Radial Hemimelia

Chapter 16
Ulnar HemimeliaChildren with ulnar hemimelia have a defi-
ciency of bone and soft tissue on the ulnar as-pect of the forearm and hand. Deficiency ofthe ulna ranges from the presence of an ulnathat is well formed but short to complete ab-sence of the ulna, which may be associatedwith radiohumeral synostosis. In contrast toradial defects, ulnar hemimelia is uncom-monly associated with abnormalities of otherorgan systems. However, patients with ulnarhemimelia are more likely to have other skele-tal anomalies, including tibial hemimelia andscoliosis. Except to correct the associated dig-
ital deformities, surgical reconstruction is notcommonly required in ulnar hemimelia.
ADDITIONAL READINGSBerger RA, Weiss A-PC, eds. Hand Surgery. Philadelphia,
Pa: Lippincott Williams and Wilkins; 2004.Green DP, Hotchkiss RN, Pederson WC, Scott WW, eds.
Green’s Operative Hand Surgery, 5th edition. NewYork, NY: Churchill Livingstone; 2005.
Mackin EJ, Callahan AD, Osterman AL, Skirven TM,Schneider LH, Hunter JM, eds. Hunter, Mackin, andCallahan’s Rehabilitation of the Hand and Upper Ex-tremity, 5th edition. Philadelphia, Pa: Mosby; 2002.
Smith PJ, Lister G. Lister’s The Hand: Diagnosis and Indi-cations. Smith P, ed. New York, NY: Churchill Living-stone; 2002.
362