Embed Size (px)
Citation preview

inSideropenic Dysphagia
a Patient with Ulcerative Colitis*
THE syndrome of dysphagia, glossitis, koilo-nychia and iron deficiency anaemia is
known by several names including the Paterson-Kelly syndrome [1,2], the Plummer-Vinsonsyndrome [3) and sideropenic dysphagia [4) .The view is now generally held that a period ofiron deficiency precedes the dysphagia althougha normal haemoglobin and serum iron levelmay be present at the time the diagnosis isfirst made [5] . An oesophageal web can usuallybe demonstrated roentgenologically [6] andis thought to be the cause of the dysphagia butthe mechanism of its formation is uncertain .
The present case is reported because serialhaemoglobin and serum iron values were avail-able for several months before the developmentof the dysphagia, and the symptom appearedto have been precipitated by blood loss occurringduring an attack of ulcerative colitis . A furtherpoint of interest is the family history of upperoesophageal carcinoma .
CASE REPORT
A thirty-four year old woman was admitted to theRadcliffe Infirmary on March 21, 1962 ; her chiefcomplaint was urgency of defaecation with blood andmucus in the stools for two months . There were noabnormal findings on general physical examination .A red, rather friable rectal mucosa was seen at sig-moidoscopy, and histologic examination of a biopsyspecimen showed some inflammatory cell infiltrationof the mucosa and submucosa. Roentgenologic exami-nation of the colon with barium (barium enema) waswithin normal limits, and examination of the stoolsfor pathogens and parasites was negative . Thehaemoglobin was 13 .8 gm. per 100 ml . and the pe-ripheral blood film normal . No definite diagnosis wasmade and the patient was discharged on the twelfthday because her symptoms had diminished withouttreatment .
When seen three months later, the patient was stillpassing only one stool daily but the rectal bleeding
RALPH WRIGHT, M.D,, M.R.C .P .
Oxford, England
274
had continued . Sigmoidoscopy was repeated andchanges typical of mild ulcerative colitis were ob-served ; these were confirmed histologically . A bariumenema (July 16, 1962) showed fine contour irregu-larities in the rectum and lower sigmoid colon con-sistent with mild ulcerative colitis . The haemoglobinwas 13.8 gm. per 100 ml. and the erythrocyte sedi-mentation rate 6 mm . in 1 hour (Westergren) . Twoweeks later diarrhoea developed for the first time .The patient was admitted to a "clinical trial" and wastreated with 5 mg, of prednisolone given orally every6 hours, a rectal infusion of 100 mg. of hydrocortisonehemisuccinate given nightly, and a milk-free diet . Inthe course of the clinical trial, patients are seen atintervals of approximately one month, when the fre-quency and nature of the stools are recorded, sig-moidoscopy and rectal biopsy performed, haemo-globin and erythrocyte sedimentation rate measured,and serum separated and stored at -20 °c. in spe-cially prepared containers for subsequent immuno-logical testing.
The patient's response to treatment was satis-factory, and both local and systemic corticosteroidtherapy was discontinued after two months . The pa-tient was kept under regular observation and re-mained well on treatment with a milk-free diet andvitamin supplements, although a fragile rectal mu-cosa was sometimes seen at sigmoidoscopy and sheoccasionally noticed blood in her stools . Six monthslater the diarrhoea recurred, with clear-cut changesof ulcerative colitis on sigmoidoscopy and a fall inthe haemoglobin level to 9.5 gm. per 100 ml. A furthercourse of treatment with local and systemic corticos-teroids was given and the diarrhoea settled .
Six weeks after the onset of the relapse, while stillreceiving treatment with corticosteroids, the patientexperienced acute dysphagia with choking bouts oneating dry solids . When seen at the clinic two weekslater, the haemoglobin was 9 .0 gm. per 100 ml . and aperipheral blood film showed changes of mild irondeficiency of the red cells . The patient's tongue andnails were normal but there were painful fissures atthe corners of the mouth. The spleen was not palpa-ble. A diagnosis of sideropenic dysphagia was made ;
* From the Nuffield Department of Clinical Medicine, University of Oxford, Oxford, England . Manuscript re-ceived February 11, 1964 .
AMERICAN JOURNAL OF MEDICINE

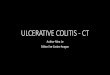
Sideropenic Dysphagia-Wrightthis was confirmed by a roentgenologic examinationwith barium which showed two pharyngeal webs ofmoderate size . (Fig . 1.) These were also demon-strated by means of cineradiography performed byDr. Gordon M . Ardran .
I lie patient was closely questioned to determinewhether she had had any symptoms of iron deficiencypreviously . Apart from pleurisy at the age of sixteenyears, she had never had any serious illnesses and nodifficulty with swallowing. Her diet was adequateand included meat at least three times a week,Menstrual loss had never been excessive . She had hadthree pregnancies fifteen, thirteen and eight years be-fore. A sister had died two years previously at the ageof thirty-one, of a squamous carcinoma of the upperportion of the oesophagus which was confirmed atpostmortem examination . She had been given ironinjections and blood transfusions for some time be-fore her death .
An oesophagoscopy was performed under generalanaesthesia . A small pharyngeal web was seen an-teriorly and a biopsy specimen was taken. Biopsyspecimens were also obtained from the body of thestomach and the small intestine . Histologic sections ofthe specimens were examined by Dr . W. C . D .Richards who reported them to be normal in appear-ance .
By a fortunate coincidence this patient had beenselected for special study for another purpose andserial specimens of serum were available for a periodof eight months preceding the dysphagia . The serumiron content was measured and in Table I and Figure2 the values are related to the haemoglobin levels andthe clinical course of the colitis . It can be seen clearlythat the serum iron values were grossly below normalthroughout, even when the haemoglobin level wasnormal or only slightly diminished .
TABLE IHAEMOGLOBIN AND SERUM IRON VALUES IN RELATION TO TILE CLINICAL COURSE OF THE COI I] IS
"Normal value >60 .t Ulcerative colitis in relapse. On treatment with corticosteroids .
VOL . 38, FEBRUARY 1965
275
Fle_ 1 . Lateral roentgenogram with )arium showingpharyngeal webs.
Tests of gastric and small intestinal function weremade. An augmented histamine test showed hypo-chlorhydria with a low volume of gastric juice. Thetotal acid secretion was 1 .07 mEq. hydrochloride in1 hour after the subcutaneous administration of 1 .5mg. histamine acid phosphate (normal range 2 .57to 46.75 mEq . hydrochloride per hour 7]) . Faecal fat
Date No. of StoolsDaily
Signs of InflammationHaemoglobin(gm. per100 MI .)
I
Serum Iron*(µg,/100 ml .)Sigmoidoscopy Rectal
Biopsy
7/6/62 2-3 + + 13 .88/3/62 2-3 + 11 .7 518/18/62 2-3 ++ 12 .0 15t9/8/62 t + 12 .3 8110/13/62 f ++ 12 .1 12t11/10/62 ++ 14 .2 132/9/63 t f 11 .0 33/16/63 10 .4 04/19/63 + ++ 9 .5 3t6/28/63 1-2 ++ 9 .0 4t

276
CORTCOS :EROIJ TREATMENT
Hb .(gm/100mL)
014 0
; HEMOOLORIN
IRELAPSE OF
0
ULCERATIVE COLITIS
SERUM IRON
I~ 097
3
4
5
9
10
II
12
Month, order ob,,rvorian .
FIG. 2 . Serial serum iron and haemoglobin values inrelation to the clinical course of the colitis and the onsetof the dysphagia. A low serum iron value was presentthroughout the period of observation and preceded theonset of the dysphagia .
excretion was 2 .1 gm. in 24 hours based on a fourday collection . The absorption of CoRE-labeled vitaminBo was normal. Almost the entire dose of Fess-labeled haemoglobin [8] administered orally ap-peared in the blood after ten days, indicating greatlyincreased absorption compatible with severe iron de-ficiency-In
view of the finding of hypochlorhydria, gastricparietal cell antibodies were looked for in the pa-tients' serum using a fluorescent technic [9] . The re-sult was negative. Antibodies to thyroglobulin weredetected at a titre of 1/25,000 by means of the tannederythrocyte haemagglutination technic according tothe method of Fulthorpe and associates [10] . Im-rnunofluorescent tests for antinuclear factor, thyroidcytoplasmic antibodies [11] and antibodies to thesecond colloid antigen [72] were negative .
The dysphagia disappeared after oesophagoscopyand a course of intramuscular iron injections, al-though the colitis remained active with some rectalbleeding. Cineradiographic examination of thepharynx and oesophagus was repeated two monthslater and only slight ridging was observed at theoriginal site of the webs.
COMMENTS
Several aspects of the present case are ofparticular interest and will be commentedupon under three separate headings .
Sideropenic Dypphagia in Ulcerative Colitis . Irondeficiency as a result of blood loss is the mostimportant cause of anaemia in ulcerative colitis[13] . In a retrospective survey Truelove andEdwards (14] found that 127 (20 .4 per cent)of 624 patients with ulcerative colitis had ahaemoglobin level of 9 .0 gm. per 100 ml . orless at some time during the course of theirillness . In none of their patients was a diagnosis
Sideropenic Dysphagia- Wright
of sideropenic dysphagia made and the associa-tion is probably rare . The very low serum ironvalues found in this patient despite a normalhaemoglobin level illustrate the limitations ofthe haemoglobin level as an index of iron deple-tion in the presence of chronic blood loss .
Family History of Pharyngeal Carcinoma . Pater-son and Kelly [7,2] first drew attention to theliability of patients with the syndrome of irondeficiency anaemia and dysphagia to thedevelopment of postcricoid carcinoma, andSimpson [15] reported the occurrence of thetwo conditions in different members of thesame family . A neoplasm in the upper part ofthe oesophagus, with the histologic features of asquamous carcinoma, was the cause of deathat the age of thirty-one of a sibling of the patientdescribed herein . She had been treated pre-viously for chronic iron deficiency anaemia .One other patient with sideropenic dysphagiaseen in this Department had a sister who diedof a squamous carcinoma of the pharynx atthe early age of twenty-eight years, and it is ofinterest (aide infra) that there was, in addition,a strong family history of thyrotoxicosis, asibling and an aunt being affected . The occur-rence of upper oesophageal or pharyngealcarcinoma in young siblings of some patientswith sideropenic dysphagia supports the viewthat similar genetic and/or environmentalfactors may he of importance in their aetiology .
The Role of Iron Deficiency in Producing Dysphagia .The main evidence favouring the possibilitythat iron deficiency is responsible for producingdysphagia in the Paterson-Kelly syndrome isthe fact that the symptom may diminish ordisappear when the iron deficiency is corrected[4,16,17] .
A unique feature of the present case is thatit has been possible to show clearly that theserum iron values were extremely low for atleast eight months before the onset of thedysphagia . Furthermore the dysphagia was ofsudden onset during a relapse of ulcerativecolitis when the haemoglobin level fell to 9 .0gm. per 100 ml ., probably indicating furtherdepletion of the iron stores . There is, therefore,suggestive evidence that iron depletion is thecause of dysphagia in this patient . On the otherhand, Wynder and Fryer [5] found that 73 percent of thirty patients with roentgenologicevidence of the Paterson-Kelly syndrome had anormal serum iron level at the time of investiga-tion of their dysphagia, and Jacobs [ 78] believes
AMERICAN JOURNAL OF MEDICINE

that mucosal changes in the pharynx may occurin patients with pernicious anaemia who arenot iron deficient. It is possible, therefore, thatiron deficiency is not essential for the develop-ment of pharyngeal webs and that other factorsmay be responsible in some cases .
Until recently histologic studies of pharyngealwebs and the adjacent pharynx and oesophagushave been confined to postmortem or surgeryspecimens taken from patients with advanceddisease [19,20] . Such studies have usuallydisclosed atrophy and hyperkeratinization of theepithelium with round cell infiltration of thesubmucosa and atrophy and fibrosis of themusculature. In one case a fibrous tissue corecovered on both sides by a layer of epitheliumwas clearly demonstrated in a biopsy specimentaken at open operation [21] .Biopsy specimens of the oesophagus and
pharynx taken at oesophagoscopy may, as inour patient, be normal in appearance [22],but early in the course of the disease it is difficultto be certain that the web itself has beenbiopsied as the lesion may be small and localised .Cheli and his colleagues [23] found atrophicchanges in the oesophagus in seven of sixteenpatients with hypochromic anaemia, whereasother workers did not find any histologic ab-normality in the oesophagus in this condition[24] . It is uncertain, therefore, whether thelesion in the pharynx early in the course islocalised or is part of a more diffuse abnormality .It is of interest that, in the patient describedherein, the dysphagia developed at the sametime as the fissures at the corners of the mouth ;it is possible that similar fissures may developin the pharynx under the mechanical stressof swallowing and progress to fibrosis and webs .
The view has been held for some time thatother epithelial changes associated with hypo-chromic anaemia such as koilonychia, glossitisand angular stomatitis are the result of the irondeficiency [4,19,25] . Here, too, the evidence islargely based on the improvement which mayoccur following treatment with iron . A similarexplanation is given for the gastritis and gastricatrophy which may occur in hypochromicanaemia [26,27] . However, Lees and Rosenthal[28] have been unable to demonstrate anyimprovement in the gastric lesion or acid secre-tion after iron therapy . In the present casethere was no evidence of glossitis or koilonychiaand the tissue structure of the gastric mucosawas normal . The hypochlorhydria and transient
VOL . 38, FEBRUARY 1965
Sideropenic Dysphagia-- Wright
277
fissures at the corners of the mouth probablyrepresent early signs of epithelial lesions, andthe underlying cause of all these lesions may besimilar .
The basic cellular abnormality is uncertain .It has been suggested that iron depletion maydamage the cell as a result of lack of iron-containing enzymes essential for cell metabolism[29] . An associated deficiency of vitamins ortrace elements may be responsible and act ina similar way .
An immunologic mechanism is also a possi-bility and may act in conjunction with one ofthe factors already mentioned . In long-standingcases the histologic appearance of round cellinfiltration with atrophy and fibrosis is com-patible with such a mechanism. The incidenceof thyroid antibodies is increased in iron de-ficiency anaemia [30] and a moderately hightitre of antibodies to thyroglobulin was foundin the present case . The second patient referredto previously had a strong family history ofthyroid disease, and Shamma'a and his col-leagues [22] have drawn attention to the fre-quent occurrence of pharyngeal webs andthyroid disease in the same patient . It is possiblethat this association indicates a disturbance ofimmunologic response in patients with sidero-penic dysphagia and iron deficiency anaemia .
SUMMARY
A case of sideropenic dysphagia is describedin a patient with ulcerative colitis . Serialspecimens of the patient's serum were availablefor a period of eight months before the onsetof the dysphagia . The iron content of thesesamples was measured and found to be ex-tremely low even when the haemoglobin levelwas normal. Two other features of the casewhich are of interest is the family history ofupper oesophageal carcinoma and the presencein the patient's serum of a moderately hightitre of antibodies to thyroglobulin .
The role of iron deficiency in the developmentof the dysphagia is discussed and it is suggestedthat an immunologic disturbance may be afactor in the production of the associated tissuechanges .
Acknowledgment : I am indebted to Dr. S. C .Truelove, Dr. S . T. Callender and Dr . B. R .Beveridge for their advice . Mr. D. L. Williamskindly made the serum iron estimations .

278REFERENCES
1 . PATERSON, D . R. A clinical type of dysphagia. J.Larvng. & Otoi ., 34 : 289, 1919 .
2. KELLY, A. B. Spasm at the entrance to the esoph-agus . J. Laryng. & Old ., 34 : 285, 1919 .
3. VwsoN, P. P. Hysterical dysphagia. Minnesota .4 led.,5 : 107, 1922 .
4. WALDENSTROM, J . Iron and epithelium. Some clini-cal observations . Acta med. scandinav., 90 (supp .) :380, 1938 .
5. WYNDER, E. L. and FRYER, J. H. Etiologic con-siderations of Plummer-Vinson (Paterson-Kelly)syndrome. Ann. Int . Med., 49 : 1106, 1958 .
6. WALDENSTROM, J . and KJELLBORG, S . R. Roentgeno-graphic diagnosis of sideropenic dysphagia. Actaradiol ., 20 : 618, 1939 .
7. Bocx, O . A . A., RIctuRns, W. C . D . and WITTS, L . J .The relationship between acid secretion after aug-mented histamine stimulation and the histologyof the gastric mucosa . Gut, 4 : 112, 1963 .
8 . CALLENDER, S . T., MALLETT, B . J . and SMITH, M. D .Absorption of haemoglobin iron . Brit. J. Haemat .,3 : 186, 1957 .
9. TAYLOR, K . B ., ROUT, I . M., DONIACH, D., COUCH-MAN, K. G. and SHAPLAND, C . Autoimmunephenomena in pernicious anaemia : gastric anti-bodies . Brit. M. J., 2 : 1347, 1962 .
10. FULTHORPE, A. J ., ROUT, 1 . M., DONIACH, D . andCOUCHMAN, K . G. A stable sheep cell preparationfor detecting thyroglobulin auto-antibodies andits clinical applications . J. Clin . Path ., 14 : 654,1961 .
11 . HOLBOROW, E . J ., BROWN, P. C., RorTT, I. M. andDONACH, D. Cytoplasmic localization of "com-plement-fixing" auto-antigen in human thyroidepithelium . Brit. J. Exper . Path., 40 : 583, 1959 .
12. BALFOUR, B . M., DomAcH, D., ROUT, 1 . M. RodCOUCHMAN, K . G. Fluorescent antibody studies inhuman thyroiditis : auto-antibodies to an antigenof the thyroid colloid distinct from thyroglobulin .Brit . J. Exper. Path ., 42 : 307, 1961 .
13. BEAL, R. W., SKYRING, A . P., MCRAE, J. and Put-BEN, B . G. The anemia of ulcerative colitis . Castro-enterology, 45 : 589, 1963 .
14. TRUELOVE, S . C. and EDwARDs, F. C. The courseand prognosis of ulcerative colitis. HI. Complica-tions. Cut, in press .
Sideropenic Dysphagia- Wright
15. SIMPSON, R . R. Anaemia with dysphagia : a pre-Cancerous condition? Prac. Roy . Sac. Med., 32 :1447, 1939 .
16, WITTS, L. J. The syndrome of glossitis, dysphagiaand anaemia. Guy's Hosp. Rep ., 81 : 193, 1931 .
17 . JONES, R. F. MCNAE. The Paterson-Brown-KellySyndrome . J. Laryng. & Otal ., 75 : 529, 1961 .
18. JACOBS, A . Post-cricoid carcinoma in patients withpernicious anaemia . Brit. M. J.,2 : 91, 1962 .
19. SUZMAN, M. M. Syndrome of anemia, glossitis anddysphagia : report of eight cases, with special refer-ence to the observations at autopsy in one in-stance . Arch . Int . Med., 51 : 1, 1933 .
20. SAVILAHTI, M. On the pathologic anatomy of thePlummer-Vinson syndrome . Acta med. scandinav .,125 : 40, 1946 .
21 . Hoovri, W. B. The syndrome of anemia, glossitisand dysphagia : report of cases. New England J.Med., 213 : 394, 1935 .
22. SHAMMA'A, M. H. and BENEDICT, E . B. Esophagealwebs. A report of 58 cases and an attempt atclassification . New England J. Med., 259 : 378,1958 .
23. CHELI, R., DODERO, M., CELLE, G . and VASSALOTTI,M. Gastric biopsy and secretory findings in hypo-chromic anaemias . Acta heamat ., 22 : 1, 1959 .
24. MCLEAN, B . I ., DODGE, O. G., PALMER, F . J. andWAwMAN, R . J. The tongue and oesophagus iniron-deficiency anaemia and the effect of irontherapy. J. Clin . Path ., 14 : 603, 1961 .
25. DARBY, W. J. The oral manifestations of irondeficiency. J.A.M.A ., 130: 830, 1946.
26. DAVIDSON, W. M. B. and MARxsoN, J . L. The gas-tric mucosa in iron-deficiency anaemia, Lancet, 2 :639, 1955 .
27. BADENOCH, J., EVANS, J . R. and RICHARDS, W. C . D.The stomach in hypochromic anaemia . Brit. J.Haemat., 3 : 175, 1957.
28 . LEES, F. and ROSENTHAL, F . D. Gastric mucosallesions before and after treatment in iron defi-ciency anaemia . Quart . J. Med., 27 : 19, 1958 .
29 . BEUTLER, E . Iron enzymes in iron deficiency . 1 .Cytochrome C. Am . J. M. Sc., 234 : 517, 1957 .
30 . MARxsON, J. L. and MOORE, J. M . Autoimmunityin pernicious anaemia and iron-deficiency anae-mia . Lancet, 2 : 1240, 1962 .
AMERICAN JOURNAL OF MEDICINE