Embed Size (px)
Citation preview

SIDE EFFECTS OF AMIODARONE/Harris et al.
40. Narula OS, Samet P, Javier RP: Significance of the sinus-noderecovery time. Circulation 45: 140, 1972
41. Strauss HC, Bigger JT, Saroff AL, Giardina EGV: Electrophysio-logic evaluation of sinus node function in patients with sinus nodedysfunction. Circulation 53: 763, 1976
42. Hellestrand KJ, Bexton RS, Nathan AW, Spurrell RAJ, Camm AJ:The acute electrophysiological effects of flecainide acetate on car-diac conduction and refractoriness in man. Br Heart J 48: 140,1982
43. Seipel L, Breithardt G: Sinus recovery time after disopyramidephosphate. Am J Cardiol 37: 1118, 1976
44. Dean RR, Ferguson DM: Effects of disopyramide on the A-Vconduction system. Arch Int Pharmacodyn 190: 183, 1971
45. Ranney RE, Dean RR, Karim A, Radzialowski FM: Disopyramidephosphate: pharmacokinetic and pharmacologic relationships of anew antiarrhythmic agent. Arch Int Pharmacodyn 191: 162, 1971
46. Mathur PP: Cardiovascular effects of a newer antiarrhythmic agent,disopyramide phosphate. Am Heart J 84: 764, 1972
47. Kent KM, Epstein SE, Cooper T, Jacobowitz DM: Cholinergicinnervation of the canine and human ventricular conducting sys-tem. Anatomic and electrophysiologic correlations. Circulation 50:948, 1974
48. Tonkin AM, Tomos P, Heddle WF, Rapp H: Autonomic effects onthe human cardiac conduction system. Evaluation by intracardiac
electrocardiography and programmed stimulation techniques. BrHeart J 44: 168, 1980
49. Bissett JK, De Soyza NDB, Kane JJ, Murphy ML: Electrophysiol-ogy of atropine. Cardiovasc Res 9: 73, 1975
50. Akhtar M, Damato AN, Caracta AR, Batsford WP, Josephson ME,Lau SH: Electrophysiologic effects of atropine on atrioventricularconduction studied by His bundle electrogram. Am J Cardiol 33:333, 1974
51. Stemple DR, Hall RJC, Mason JW, Harrison DC: Electrophysio-logical effects of edrophonium in the innervated and the transplant-ed denervated human heart. Br Heart J 40: 644, 1978
52. Hulting J, Jansson B: Antiarrhythmic and electrocardiographiceffects of single oral doses of disopyramide. Eur J Clin Pharmacol11: 91, 1977
53. Niarchos AP: Disopyramide: serum level and arrhythmia conver-sion. Am Heart J 92: 57, 1976
54. Dhingra RC, Amat-y-Leon F, Wyndham C, Denes P, Wu D,Pouget JM, Rosen KM: Electrophysiologic effects of atropine onhuman sinus node and atrium. Am J Cardiol 38: 429, 1976
55. Simpson MB, Spear J, Moore EN: The relationship between atrio-ventricular nodal refractoriness and the functional refractory periodin the dog. Circ Res 44: 121, 1979
56. Dreifus LS: The electrophysiology of Norpace (part I). Angiology26: 111, 1975
Side Effects of Long-term Amiodarone TherapyLouISE HARRIS, M.B., WILLIAM J. MCKENNA, M.D., EDWARD ROWLAND, M.B.,
DAVID W. HOLT, PH.D., GERARD C.A. STOREY, B.SC., AND DENNIS M. KRIKLER, M.D.
SUMMARY Although amiodarone is an effective antiarrhythmic agent, long-term therapy may be associ-ated with unwanted effects. We report our experience in 140 patients treated over 5 years. Important effectswere seen particularly in the thyroid gland, liver, lung and skin. Some of these effects are dose-dependentand others may be related to the chemical structure and metabolism of amiodarone. Corneal microdepositswere always found when sought, but did not cause impairment of visual acuity.
AMIODARONE has been available in Europe for ap-proximately 20 years for the management of anginapectoris,' but only in the past decade have its uniqueantiarrhythmic properties been recognized.2 It is effec-tive in the management of refractory ventricular ar-rhythmias, including those associated with ischemicheart disease and the cardiomyopathies.3 4 It is particu-larly useful in the management of chronic atrial ar-rhythmias refractory to conventional drugs, with animpressive conversion rate of chronic atrial fibrillationto sinus rhythm.4 Amiodarone is especially effective insuppressing or modifying paroxysmal atrial arrhyth-mias, including those associated with the Wolff-Par-kinson-White syndrome,5 in which sudden death fromrapidly conducted atrial fibrillation is a risk.6
With the more widespread use of amiodarone, sev-eral side effects have been identified. In the majority of
From the Division of Cardiovascular Disease, Department of Medi-cine, Royal Postgraduate Medical School, and the Poisons Units, Guy'sHospital, London, England.
Dr. McKenna is a Research Fellow of the Medical Research Councilof Canada.
Address for correspondence: Dennis M. Krikler, M.D., Cardiovas-cular Division, Hammersmith Hospital, Du Cane Road, London W12OHS, England.
Received April 30, 1982; revision accepted July 7, 1982.Circulation 67, No. 1, 1983.
patients, these are well tolerated and are often modi-fied by a reduction in dosage so that discontinuation oftherapy is rarely necessary. A few patients, however,have more serious complications, including pulmo-nary fibrosis7 I and clinical thyroid disease.9 The inci-dence, mechanisms and management of these compli-cations is uncertain. Our experience in individual casesdates back over 9 years. We are now able to report 140patients in whom we have systematically monitoredthe unwanted effects over the past 5 years.
Patients and DosageWe reviewed 140 patients (95 males and 45 females,
mean age 52 years) who had been taking amiodaronefor an average of 2 years; the longest follow-up was 5years. Although 69 of our patients were taking amio-darone for primary arrhythmias, including the Wolff-Parkinson-White syndrome, we also treated 15 pa-tients with ischemic heart disease and 48 who hadarrhythmias associated with cardiomyopathy, 28 hy-pertrophic and 20 congestive. Five patients had valvu-lar disease, two hypertensive heart disease and onepatient an atrial septal defect. Details of the arrhyth-mias treated are listed in table 1.The dose varied from 100 to 1200 mg/day, but only
11 patients took 600 mg/day or more long-term; the
45
by guest on June 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 67 , No 1, JANUARY 1983
TABLE 1. Arrhythmias Treated with AmiodaroneNo. of Mean dose
Arrhythmia pts (mg/day)Ventricular tachycardia 46 440
(200-1200)Ventricular extrasystoles 10 400
(200-600)Chronic atrial fibrillation! 15 310
flutter (200-400)Paroxysmal atrial arrhythmia 38 280
(100-400)Supraventricular arrhythmias, 31 350
including Wolff-Parkinson-White (100-600)syndrome
mean dosage was 360 mg/day. We gave an initialloading dose of 600-1200 mg/day for 1 week, fol-lowed by 400-600 mg/day for a month; thereafter, themaintenance dose was determined by balancing con-trol of arrhythmia against side effects. Amiodaroneand its desethyl metabolite were measured in plasmaand, where possible, in various tissues, using high-performance liquid chromatography.'10' Plasma con-centrations were assessed relative to side effects andalterations of metabolic function. Drug levels of amio-darone (range 0. 1-5.2 mg/l) and desethyl amiodarone(range 0.1-5.0 mg/l) correlated with dosage (r = 0.59p < 0.001 and r = 0.66 p < 0.001, respectively).
190-
170-
150-
-6E 130-
.c.x0; 110-
90-
70-
weeks months
Duration of therapy
-
Ez
1.2-
1. 0-
0.8-
0.4-
0.2-
O. O-i
The unwanted effects are categorized as thyroid,hepatic, pulmonary and cutaneous. Ocular and neuro-logic changes are also considered, as are alterations incardiac conduction and repolarization.
ThyroidChanges in thyroid function were recognized ear-
1Y;9 12 the most common was a rise in thyroxine (T4)and reverse triiodothyronine (rT3) levels, and a fall intriiodothyronine (T3).'3 There is also an associatedincidence of clinical thyroid disease.We measured T4 in 10 patients and rT3 in nine of the
same 10 patients systematically over an 18-month peri-od. All had normal thyroid function at the start oftreatment (fig. 1). T4 decreased in the first 2 weeks oftreatment in four of the patients, but thereafter levelsincreased in all; rT3 increased in all subjects (increaseof 79% over 18 months). In addition to these detailedserial observations, we measured T4 in 85 additionalpatients. The mean T4 level for the group was elevatedby 20% above the mean for the laboratory (fig. 2). Infive, the T4 level decreased and thyroid-stimulatinghormone (TSH) increased (table 2); two of these pa-tients were clinically myxedematous. In contrast, fourpatients had increased T4 levels of 25% or more abovethe upper limit of normal (table 2); two were clinicallythyrotoxic. To identify predisposing factors in thesepatients with marked alterations in thyroid function,
SB
DWvCH
, NS
TH.wwRC
BN FIGURE 1. (top) Thyroxine levels (nmol/l) intDS 10 patients before and during amiodarone
therapy for as long as 18 months (nglml =-{,_ nmol/l x 1.287). (bottom) Reverse triiodothy-
24 ronine (T3) in nine patients before and duringtreatment with amiodarone for as long as 18months (ng/ml = nmol/l x 0.651).
_ DW* NSBN
-THGRRC
I0 12 1
weeks months
I I I I nI .
3 6
Duration of therapy
12 24
46 CIRCULATION
by guest on June 10, 2018http://circ.ahajournals.org/
Dow
nloaded from
SIDE EFFECTS OF AMIODARONE/Harris et al.
300-
200-
100-
O0
Thyroxine (nmol 11)
n = 95
es
I
0
m
0
.
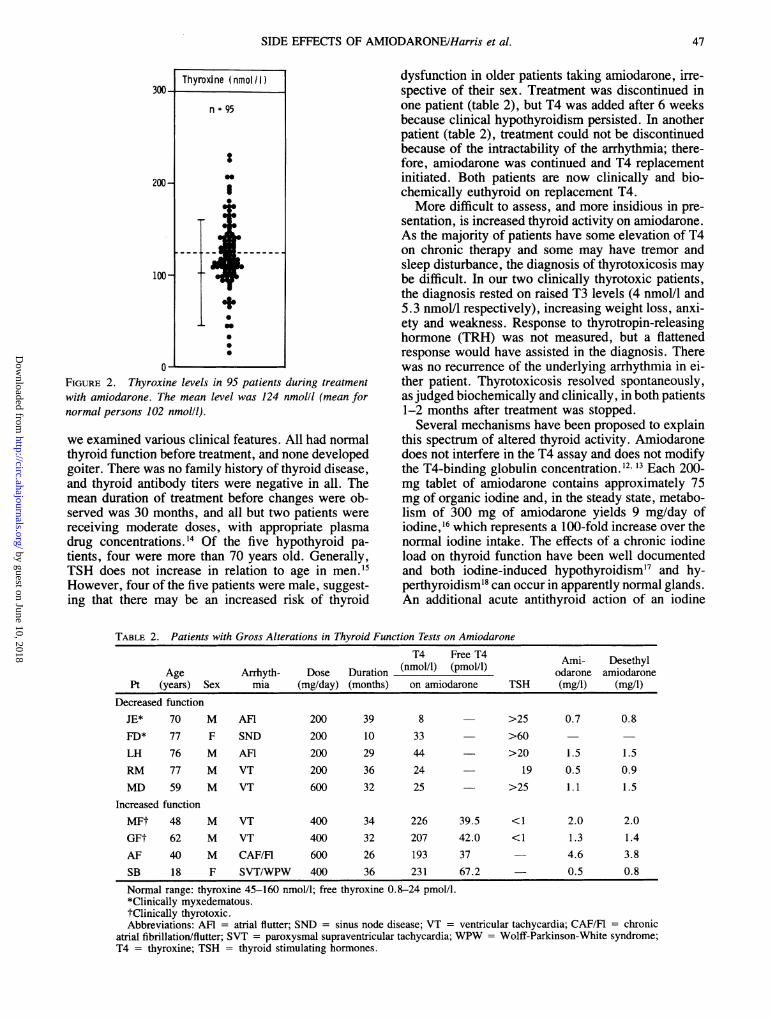
FIGURE 2. Thyroxine levels in 95 patients during treatmentwith amiodarone. The mean level was 124 nmol/l (mean fornormal persons 102 nmol/l).
we examined various clinical features. All had normalthyroid function before treatment, and none developedgoiter. There was no family history of thyroid disease,and thyroid antibody titers were negative in all. Themean duration of treatment before changes were ob-served was 30 months, and all but two patients werereceiving moderate doses, with appropriate plasmadrug concentrations. '4 Of the five hypothyroid pa-tients, four were more than 70 years old. Generally,TSH does not increase in relation to age in men. sHowever, four of the five patients were male, suggest-ing that there may be an increased risk of thyroid
dysfunction in older patients taking amiodarone, irre-spective of their sex. Treatment was discontinued inone patient (table 2), but T4 was added after 6 weeksbecause clinical hypothyroidism persisted. In anotherpatient (table 2), treatment could not be discontinuedbecause of the intractability of the arrhythmia; there-fore, amiodarone was continued and T4 replacementinitiated. Both patients are now clinically and bio-chemically euthyroid on replacement T4.More difficult to assess, and more insidious in pre-
sentation, is increased thyroid activity on amiodarone.As the majority of patients have some elevation of T4on chronic therapy and some may have tremor andsleep disturbance, the diagnosis of thyrotoxicosis maybe difficult. In our two clinically thyrotoxic patients,the diagnosis rested on raised T3 levels (4 nmol/l and5.3 nmol/l respectively), increasing weight loss, anxi-ety and weakness. Response to thyrotropin-releasinghormone (TRH) was not measured, but a flattenedresponse would have assisted in the diagnosis. Therewas no recurrence of the underlying arrhythmia in ei-ther patient. Thyrotoxicosis resolved spontaneously,as judged biochemically and clinically, in both patients1-2 months after treatment was stopped.
Several mechanisms have been proposed to explainthis spectrum of altered thyroid activity. Amiodaronedoes not interfere in the T4 assay and does not modifythe T4-binding globulin concentration. 12 13 Each 200-mg tablet of amiodarone contains approximately 75mg of organic iodine and, in the steady state, metabo-lism of 300 mg of amiodarone yields 9 mg/day ofiodine,16 which represents a 100-fold increase over thenormal iodine intake. The effects of a chronic iodineload on thyroid function have been well documentedand both iodine-induced hypothyroidism'7 and hy-perthyroidism'8 can occur in apparently normal glands.An additional acute antithyroid action of an iodine
TABLE 2. Patients with Gross Alterations in Thyroid Function Tests on AmiodaroneT4 Free T4 Ami- Desethyl
Age Arrhyth- Dose Duration (nmol/l) (pmol/l) odarone amiodaronePt (years) Sex mia (mg/day) (months) on amiodarone TSH (mg/i) (mg/i)
Decreased functionJE* 70 M AFI 200 39 8 >25 0.7 0.8
FD* 77 F SND 200 10 33 >60 -
LH 76 M AFI 200 29 44 >20 1.5 1.5
RM 77 M VT 200 36 24 19 0.5 0.9
MD 59 M VT 600 32 25 >25 1.1 1.5Increased function
MFt 48 M VT 400 34 226 39.5 <1 2.0 2.0
GFt 62 M VT 400 32 207 42.0 <1 1.3 1.4
AF 40 M CAF/FI 600 26 193 37 4.6 3.8
SB 18 F SVT/WPW 400 36 231 67.2 0.5 0.8
Normal range: thyroxine 45-160 nmol/l; free thyroxine 0.8-24 pmol/l.*Clinically myxedematous.tClinically thyrotoxic.Abbreviations: AFR = atrial flutter; SND = sinus node disease; VT = ventricular tachycardia; CAF/Fl = chronic
atrial fibrillation/flutter; SVT = paroxysmal supraventricular tachycardia; WPW = Wolff-Parkinson-White syndrome;T4 = thyroxine; TSH = thyroid stimulating hormones.
47
by guest on June 10, 2018http://circ.ahajournals.org/
Dow
nloaded from
VOL 67, No 1, JANUARY 1983
load, the Wolff-Chaikoff effect,'9 may explain the ini-tial fall in T4 in some of our patients (fig. 2). In normalpersons, as in our patients, this effect is transient evenwith continued iodine administration, because of au-toregulatory inhibition of intrathyroid iodide transport.Amiodarone itself may have a direct action on thethyroid gland, but in vitro studies have shown no alter-ation of active iodide transport, iodine organificationor iodotyrosine deiodination.20 However, a direct in-trathyroid action in vivo cannot be ruled out if amio-darone is substantially concentrated in the gland. In asingle postmortem observation of a patient not includ-ed in this series, concentrations of amiodarone anddesethyl amiodarone of 15 mg/kg and 92 mg/kg, re-spectively, were found in the thyroid gland. Amiodar-one is also reported to inhibit the peripheral conversionof T4 to T3 with increased conversion along the alter-native pathway to rT3, resulting in a rise in T4 and rT3,with a low or normal T3;'2 our findings are consistentwith this suggestion.
HepaticHepatic dysfunction from drugs is well recognized.
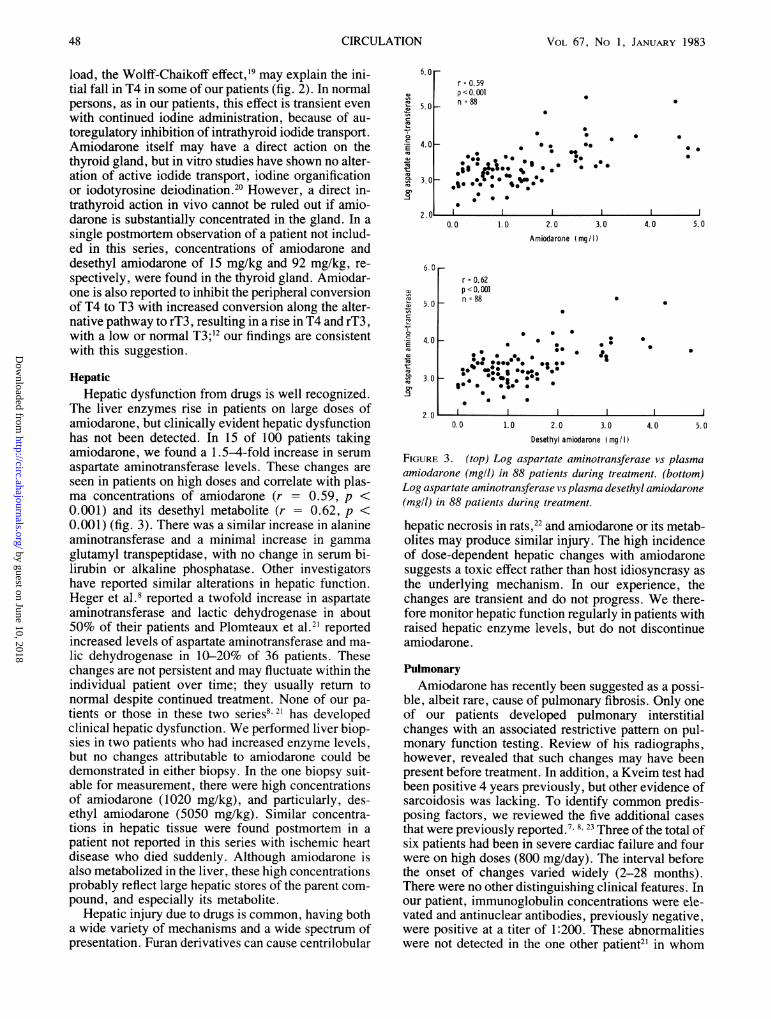
The liver enzymes rise in patients on large doses ofamiodarone, but clinically evident hepatic dysfunctionhas not been detected. In 15 of 100 patients takingamiodarone, we found a 1.5-4-fold increase in serumaspartate aminotransferase levels. These changes areseen in patients on high doses and correlate with plas-ma concentrations of amiodarone (r - 0.59, p <0.001) and its desethyl metabolite (r = 0.62, p <0.001) (fig. 3). There was a similar increase in alanineaminotransferase and a minimal increase in gammaglutamyl transpeptidase, with no change in serum bi-lirubin or alkaline phosphatase. Other investigatorshave reported similar alterations in hepatic function.Heger et al.8 reported a twofold increase in aspartateaminotransferase and lactic dehydrogenase in about50% of their patients and Plomteaux et al.21 reportedincreased levels of aspartate aminotransferase and ma-lic dehydrogenase in 10-20% of 36 patients. Thesechanges are not persistent and may fluctuate within theindividual patient over time; they usually return tonormal despite continued treatment. None of our pa-tients or those in these two series8' 21 has developedclinical hepatic dysfunction. We performed liver biop-sies in two patients who had increased enzyme levels,but no changes attributable to amiodarone could bedemonstrated in either biopsy. In the one biopsy suit-able for measurement, there were high concentrationsof amiodarone (1020 mg/kg), and particularly, des-ethyl amiodarone (5050 mg/kg). Similar concentra-tions in hepatic tissue were found postmortem in apatient not reported in this series with ischemic heartdisease who died suddenly. Although amiodarone isalso metabolized in the liver, these high concentrationsprobably reflect large hepatic stores of the parent com-pound, and especially its metabolite.
Hepatic injury due to drugs is common, having botha wide variety of mechanisms and a wide spectrum ofpresentation. Furan derivatives can cause centrilobular
6.0f
5.0k
4.01-
3.01-
r = 0.59p <0. 001n =88
0
* 0.
0 * 0 0
0* . 000 0
1000*.a
*: 6S
0.0 1.0 2.0 3.0 4.0 5.0Amiodarone (mg/I)
6. 0
5.0 Fa)
.E
nsm
_
ow'
4.0 -
3.0 F
2.0
r = 0.62p <0.001n = 88
0 00
0 S.0 @0000 * * 0go *.0000.0 ***1 .0. *00
S:w.0::..:.0
0* *
0 :
ft
0.0 1.0 2.0 3.0 4.0 5.0
Desethyl amiodarone (mg I I)
FIGURE 3. (top) Log aspartate aminotransferase vs plasmaamiodarone (mgll) in 88 patients during treatment. (bottom)Log aspartate aminotransferase vs plasma desethyl amiodarone(mg/l) in 88 patients during treatment.
hepatic necrosis in rats,22 and amiodarone or its metab-olites may produce similar injury. The high incidenceof dose-dependent hepatic changes with amiodaronesuggests a toxic effect rather than host idiosyncrasy asthe underlying mechanism. In our experience, thechanges are transient and do not progress. We there-fore monitor hepatic function regularly in patients withraised hepatic enzyme levels, but do not discontinueamiodarone.
PulmonaryAmiodarone has recently been suggested as a possi-
ble, albeit rare, cause of pulmonary fibrosis. Only oneof our patients developed pulmonary interstitialchanges with an associated restrictive pattern on pul-monary function testing. Review of his radiographs,however, revealed that such changes may have beenpresent before treatment. In addition, a Kveim test hadbeen positive 4 years previously, but other evidence ofsarcoidosis was lacking. To identify common predis-posing factors, we reviewed the five additional casesthat were previously reported.7 8 23 Three of the total ofsix patients had been in severe cardiac failure and fourwere on high doses (800 mg/day). The interval beforethe onset of changes varied widely (2-28 months).There were no other distinguishing clinical features. Inour patient, immunoglobulin concentrations were ele-vated and antinuclear antibodies, previously negative,were positive at a titer of 1:200. These abnormalitieswere not detected in the one other patient2' in whom
Z. u =
48 CIRCULATION
a)'A(aI
4!c17
0a
.EmQ)coV-mV.cu4mq
:
.
.
* 0
I Il
by guest on June 10, 2018http://circ.ahajournals.org/
Dow
nloaded from
SIDE EFFECTS OF AMIODARONE Harris et al.
they were sought. Lung biopsies were performed infour of the patients, but only nonspecific features-alveolar wall fibrosis and atypical pneumocyteswere demonstrated. In our patient and in three pre-viously described, the pulmonary changes resolvedafter the amiodarone had been discontinued and corti-costeroids commenced. None has been rechallengedwith amiodarone. The two remaining patients died ofsevere coexistent heart failure.The mechanism of pulmonary injury is unknown.
Our patient had positive antinuclear antibodies andelevated immunoglobulin levels; one possibility is adrug-induced autoimmune disorder. No conclusionscan be drawn, however, as these tests were normal inthe one other patient in whom they were measured.Alternatively, a direct toxic effect may occur. Theroles of high dosage and of cardiac failure must beexplored.
Amiodarone DermatopathyTwo types of skin reaction have been described.
Photosensitivity is common, but there is also a rareslate-gray pigmentation of the exposed areas. Photo-sensitivity is the commonest side effect reported by ourpatients (57%). There is a wide spectrum of skin reac-tion, ranging from an increased propensity to suntanduring the summer months to intense burning, erythe-ma and swelling of the exposed areas. We revieweddosage and measured plasma concentrations of amio-darone and its metabolite in patients with and withoutphotosensitivity, but fbund no significant differencebetween the two groups. lHowever, the intensity of thereaction can be alleviated by a reduction in dosage andmost patients can be protected by prophylactic barriercreams. None of our patients had to stop treatment. Weobserved a different skin reaction in the first 2 weeksafter starting amiodarone in six patients: a pruritic,erythematous, fine maculopapular rash with a pre-dominantly truncal distribution. It resolved spontane-ously within days and did not require treatment orcessation of therapy.Two patients have developed a slate gray/purple
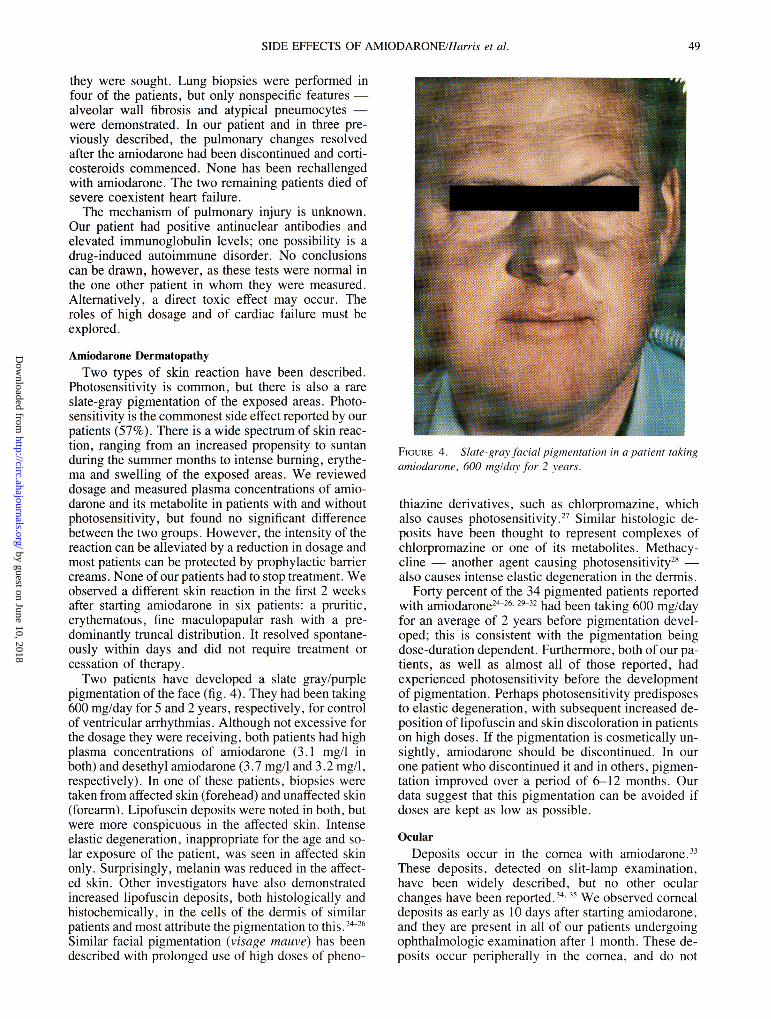
pigmentation of the face (fig. 4). They had been taking600 mg/day for 5 and 2 years, respectively, for controlof ventricular arrhythmias. Although not excessive forthe dosage they were receiving, both patients had highplasma concentrations of amiodarone (3.1 mg/I inboth) and desethyl amiodarone (3.7 mg/l and 3.2 mg/I,respectively). In one of these patients, biopsies weretaken from affcted skin (fbrehead) and unaffected skin(forearm). Lipofuscin deposits were noted in both, butwere more conspicuous in the affected skin. Intenseelastic degeneration, inappropriate for the age and so-lar exposure of the patient, was seen in affected skinonly. Surprisingly, melanin was reduced in the affect-ed skin. Other investigators have also demonstratedincreased lipofuscin deposits, both histologically andhistochemically, in the cells of the dermis of similarpatients and most attribute the pigmentation to this.6Similar facial pigmentation (visage mauve) has beendescribed with prolonged use of high doses of pheno-
FIG,URE 4. Slategara facial pigmentation in a patient takingamiodarone, 600 mg1dav fir 2 vears.
thiazine derivatives, such as chlorpromazine, whichalso causes photosensitivity.' Similar histologic de-posits have been thought to represent complexes ofchlorpromazine or one of its metabolites. Methacy-cline- another agent causing photosensitivity'8also causes intense elastic degeneration in the dermis.
Forty percent of the 34 pigmented patients reportedwith amiodarone2t26 29-32 had been taking 600 mg/dayfor an average of 2 years before pigmentation devel-oped; this is consistent with the pigmentation beingdose-duration dependent. Furthermore, both of our pa-tients, as well as almost all of those reported, hadexperienced photosensitivity before the developmentof pigmentation. Perhaps photosensitivity predisposesto elastic degeneration, with subsequent increased de-position of lipofuscin and skin discoloration in patientson high doses. If the pigmentation is cosmetically un-sightly, amiodarone should be discontinued. In ourone patient who discontinued it and in others, pigmen-tation improved over a period of 6-12 months. Ourdata suggest that this pigmentation can be avoided ifdoses are kept as low as possible.
OcularDeposits occur in the cornea with amiodarone.33
These deposits, detected on slit-lamp examination,have been widely described, but no other ocularchanges have been reported.34 We observed comealdeposits as early as 10 days after starting amiodarone,and they are present in all of our patients undergoingophthalmologic exam:ination after I month. These de-posits occur peripherally in the comea, and do not
49
by guest on June 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 67, No 1, JANUARY 1983
produce symptoms. However, two of our patientsusing 600 mg/day complained of blue/green haloes onlooking at bright lights and were found to have comealdeposits encroaching on the pupil. Both responded to areduction in dosage. We have observed no other oph-thalmologic complications, and no patient has requireddiscontinuation of therapy for ocular side effects.Therefore, we no longer advise serial ophthalmologicexaminations in asymptomatic patients on long-termamiodarone.
NeurologicPeripheral neuropathy has been seen in rare in-
stances with long-term amiodarone therapy, and intra-cellular inclusion bodies, similar to those seen in skin,have been demonstrated in peripheral nerve fibers.36Proximal weakness, with predominant involvement ofthe thigh muscles, was observed in eight of our pa-tients in the first weeks of therapy. It occurred in pa-tients taking high doses (800 mg/day or more) andresolved spontaneously or with a reduction in dose. Adelay in nerve conduction but normal electromyo-grams were demonstrated in two other patients taking1800 and 2000 mg/day, respectively; both respondedto a reduction in dosage.8
Clinically distinct from this is the problem of periph-eral neuropathy. There are several reports of a sensori-motor neuropathy, with a glove and stocking distribu-tion, in patients using moderate (400 mg/day) to largedoses (1800 mg/day) for 1 year or longer.36-9 Nerveconduction velocity is reduced. Histologically, seg-mental demyelination of the nerve fibers has beendemonstrated as well as lipid-containing lysosomalinclusion bodies in the Schwann cells. Although theneuropathy resolves when treatment is discontinued,this is often slow and incomplete. Some of the patientsdescribed were using other drugs, including perhexi-line, but in other cases there were no apparent predis-posing factors. None of our patients developed thiscomplication, and there does not appear to be a meansof identifying which patients are at risk.
Cardiac Conduction and RepolarizationThe electrophysiologic effects of amiodarone in-
clude depression of sinus"' and atrioventricular nodalfunction and prolongation of myocardial refractori-ness,41 reflected in the surface ECG as a decrease inheart rate and repolarization changes.
Although amiodarone has been used safely in pa-tients with the sick sinus syndrome,42 it does prolongsinus cycle length8 and sinus node recovery time.40 Theconcurrent administration of other antiarrhythmicdrugs, such as /8 blockers, may result in sinus arrest.43Amiodarone increases plasma digoxin concentra-tions," but the effect of this interaction on arrhythmiasis uncertain. Prolongation of the QTc interval occurs inthe majority of patients and is the electrocardiographicexpression of the drug effect on the action potentialduration. It does not appear to have the same implica-tions as a similar degree ofQTc prolongation seen withquinidine-like antiarrhythmic agents. McComb et al.45
suggested an association between amiodarone andatypical ventricular tachycardia. We do not agree thattheir patient had torsade de pointes,46 which has notoccurred in any of our patients; nor had it been foundwhen amiodarone was given as the sole agent in anextensive review of use of amiodarone in France.47The mechanisms of the unwanted effects seen in
patients receiving amiodarone fall into two broadgroups. Some of the effects are dose-related. This isparticularly clear in the elevation of the serum amino-transferases, where almost all patients who take 600mg/day or more have raised levels. Other effects areboth dose- and duration-dependent; the extent of thecorneal microdeposits and the abnormal facial pigmen-tation are the best examples. These effects of long-termhigh doses make careful balance of dose against ar-rhythmia control imperative. In contrast, the effects onthe thyroid gland and the peripheral nerves appear tobe independent of these factors and suggest specificreactions in individual patients; thus, older patients onamiodarone appear to run an increased risk of myxe-dema. Until we have a better understanding of themechanism of the pulmonary reaction, this effect can-not be defined.
Regardless of the mechanisms of these unwantedeffects, almost all, with the possible exception of myx-edema, resolve when treatment is discontinued. Amio-darone has proved sufficiently valuable for serious ar-rhythmias that its judicious administration is oftenrequired; its benefit will clearly be greatest whenknowledge of its side effects is complete.
References1. Vastesaeger M, Gillot P, Rasson G: Etude clinique d'une nouvelle
medication anti-angoreuse. Acta Cardiol (Brux) 22: 483, 19672. Coumel Ph, Bouvrain Y: Etude clinique des effects pharmacody-
namiques et antiarythmiques de l'amiodarone. J Agreges 6: 69,1973
3. Rosenbaum MB, Chiale PA, Halpern MS, Nau GT, Przybylski J,Levi RJ, Lazzari JO, Elizari MV: Clinical efficacy of amiodaroneas an anti-arrhythmic agent. Am J Cardiol 38: 934, 1976
4. McKenna WJ, Harris L, Perez G, Krikler DM, Oakley C, Good-win JF: Arrhythmia in hypertrophic cardiomyopathy. Il. Compari-son of amiodarone and verapamil in treatment. Br Heart J 46: 173,1981
5. Rowland E, Krikler DM: Electrophysiological assessment of amio-darone in treatment of resistant supraventricular arrhythmias. BrHeart J 44: 82, 1980
6. Dreifus LS, Haiat R, Watanabe Y, Arriaga J, Reitman NC: Ven-tricular fibrillation: a possible mechanism of sudden death in pa-tients with Wolff-Parkinson-White syndrome. Circulation 43: 520,1971
7. Rotmensch HH, Liron M, Tupilski M, Laniado S: Possible associ-ation of pneumonitis with amiodarone therapy. Am Heart J 100:412, 1980
8. Heger JJ, Prystowsky EN, Jackman WM, Naccarelli GV, WarfelKA, Rinkenberger RL, Zipes DP: Amiodarone: clinical efficacyand electrophysiology during long term therapy for recurrent ven-tricular tachycardia or ventricular fibrillation. N Engl J Med 305:539, 1981
9. Jonckheer MH, Blockx P, Kaivers R, Wyffels G: Hyperthyroidismas a possible complication of the treatment of ischaemic heartdisease with amiodarone. Acta Cardiol (Brux) 28: 192, 1973
10. Flanagan RJ, Storey GCA, Holt DW: Rapid high performanceliquid chromatographic method for the measurement of amioda-rone in blood plasma or serum at the concentrations attained duringtherapy. J Chromatogr 187: 391, 1980
CIRCULATION50
by guest on June 10, 2018http://circ.ahajournals.org/
Dow
nloaded from
SIDE EFFECTS OF AMIODARONE/Harris et al.
11. Flanagan RJ, Harris L, Holt DW, McKenna WJ, Rowland E,Storey GCA: High-performance liquid chromatographic measure-ment of amiodarone and its desethyl metabolite in plasma. InProceedings of the British Pharmacological Society meeting. Ox-ford, 1981, p 139
12. Burger A, Dinichert D, Nicod P, Jenny M, Lemarchand-Beraud T,Vallotton MD: Effect of amiodarone on serum tri-iodothyronine,reverse triodothyronine, thyroxine and thyrotropin: a drug influ-encing peripheral metabolism of thyroid hormones. J Clin Invest58: 255, 1976
13. Jonckheer MH, Blockx P, Broeckaert I, Comette C, Beckers C:Low T3 syndrome in patients chronically treated with an iodine-containing drug, amiodarone. Clin Endocrinol 9: 27, 1978
14. Holt DW, Storey GCA: Measurement of amiodarone. In Amioda-rone and Arrhythmias, edited by Krikler DM, McKenna WJ,Chamberlain DA. Oxford, Pergamon Press, 1983. In press
15. Tunbridge WMG, Evered DC, Hall R, Appleton D, Brewis M,Clark F, Grimley Evans J, Young E, Bird T, Smith P: The preva-lence of thyroid disorders in an English community. In ThyroidResearch, edited by Robbins J, Braverman LE. Amsterdam, Ex-cerpta Medica, 1976, pp 520-522
16. Broekhuysen J, Laruel R, Sion R: Recherches dans la serie desbenzofuranes. Etude comparee du transit et du metabolisme deI'amiodarone chez diverses especes animales et chez l'homme.Arch Int Pharmacodyn 177: 340, 1969
17. Wolff J: Iodide goitre and the pharmacologic effects of excessiodide. Am J Med 47: 101, 1969
18. Savoie JC, Massin P, Thomopoulos P, Leger F: Iodine-inducedthyrotoxicosis in apparently normal thyroid glands. J Clin Endo-crinol Metab 41: 685, 1975
19. Wolff J, Chaikoff IC: The inhibitory action of iodide upon organicbinding of iodine by the normal thyroid gland. J Biol Chem 172:855, 1948
20. Gluzman BE, Coleoni AH, Targovnik HM, Niepomniscze H: Ef-fects of thyroid iodine metabolism in vitro. Acta Endocrinol 85:781, 1977
21. Plomteaux G, Heusghem C, Ernould H, Vandeghen N: Longtermhepatic tolerance of amiodarone in the clinic. Eur J Pharmacol 8:369, 1969
22. Boyd MR, Burka LT: In vivo studies on the relationship betweentarget organ alkylation and the pulmonary toxicity of a chemicallyreactive metabolite of 4-ipomeanol. J Pharmacol Exp Ther 207:687, 1978
23. Riley SA, Williams SE, Cooke NH: Alveolitis after treatment withamiodarone. Br Med J 284: 161, 1982
24. Morand Ph, Benatre J, Viau G, Carli-Basser C, Laine JL, Neel JL,Brochier M, Raynaud R: Etude clinique et histologique (ultra-structure) de la pigmentation par le chlorhydrate d'amiodarone.Sem H6p Paris 48: 553, 1972
25. Labouche F, Balouet G, Daoulas R, Masse R, Le Moigne P,Coignard A, Baret MF: Les accidents cutanes de l'amiodarone.Arch Med Ouest 5: 37, 1973
26. Texier L, Meunier J, Gauthier Y, Dubiau JM, Gaillard G: Pigmen-tations cutanees accidentelles au cours de traitements par l'amio-
darone. Concours Medical 93: 4859, 197127. Satanove H: Pigmentation due to phenothiazine in high and pro-
longed dosage. JAMA 191: 263, 196528. Dysner-Aas K, Jansson H, Miorner G: Pigment deposits in eyes
and light exposed skin during long term methacycline therapy.Acta Derm Venereol (Stockh) 54: 209, 1974
29. Wanet J, Achten G, Barchewitz G, Mestdagh G, Vastesaeger M:Amiodarone et depots cutanes. Etude clinique et histologique. AnnDermatol Syph 98: 131, 1971
30. Heme N, Marion J, Brisou B, Antiglio V, Rousselot M: Pigmenta-tions cutanees induites par le chlorhydrate d'amiodarone. LyonMed 226: 205, 1971
31. Vulliemin JF: Les effets secondaires cutanes de la Cordarone.Schweiz Rundschau Med (Praxis) 62: 1426, 1973
32. Lambert D, Noble JP, Justrabo E, Hewitt J: Pigmentation cutan6esecondaire a l'administration d'amiodarone: problemes histogene-tiques. Ann Dermatol Syph 102: 277, 1975
33. Wrin P, Gendre P, Barchewitz G, Laurent-Bronchat G, YacoubiM, Morax S: Thesaurismose corneenne par amiodarone: donn6esrecentes. Arch Ophtalmol 31: 581, 1971
34. Ingram DV: Ocular changes during oral amiodarone therapy. InAmiodarone and Arrhythmias, edited by Krikler DM, McKennaWJ, Chamberlain DA. Oxford, Pergamon Press, 1983. In press
35. Babel J: Amiodarone et tissus oculaires. Schweiz Rundschau Med(Praxis) 61: 1571, 1972
36. Dudognon P, Hauw JJ, de Baecque C, Derrida JP, Escourolle R,Nick J: Neuropathie au chlorhydrate d'amiodarone: etude cliniqueet histopathologique d'une nouvelle lipidose m6dicamenteuse. RevNeurol (Paris) 135: 527, 1979
37. Lustman F, Monseu G: Amiodarone and neurological side effects.Lancet 1: 568, 1974
38. Kaeser HE: Amiodaron-neuropathie. Schweiz Med Wschr 104:606, 1974
39. Meier C, Kauer B, Muller U, Ludin HP: Neuromyopathy duringchronic amiodarone therapy. J Neurol 220: 231, 1979
40. Touboul P, Atallah G, Gessard A, Kirkorian G: Effects of amioda-rone on sinus node in man. Br Heart J 42: 573, 1979
41. Wellens HJJ, Lie KI, Bir FW, Wesdorp JC, Dohmen HJ, DurerDR, Durrer D: Effect of amiodarone in the Wolff-Parkinson-Whitesyndrome. Am J Cardiol 38: 189, 1976
42. Brown AK, Primhak RA, Newton P: Use of amiodarone in brady-cardia-tachycardia syndrome. Br Heart J 40: 1149, 1978
43. McGovern B, Garan H, Ruskin JN: Sinus arrest during treatmentwith amiodarone. Br Med J 284: 160, 1982
44. Moysey JO, Jaggarao NSV, Grundy EW, Chamberlain DA: Amio-darone increases plasma digoxin concentrations. Br Med J 282:272, 1981
45. McComb JM, Logan KR, Khan MM, Geddes JS, Adgey AAJ:Amiodarone-induced ventricular fibrillation. Eur J Cardiol 11:381, 1980
46. Krikler DM, Curry PVL: Torsade de pointes, an atypical ventricu-lar tachycardia. Br Heart J 38: 117, 1976
47. Brochier M, Fauchier JP: Torsades de pointe et rentrees provo-quees par les anti-arythmiques. Arch Mal Coeur 71: 477, 1978
51
by guest on June 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

L Harris, W J McKenna, E Rowland, D W Holt, G C Storey and D M KriklerSide effects of long-term amiodarone therapy.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1983 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.67.1.45
1983;67:45-51Circulation.
http://circ.ahajournals.org/content/67/1/45.citationthe World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 10, 2018http://circ.ahajournals.org/
Dow
nloaded from





























