Embed Size (px)
Citation preview

Aortic Homograft Valve Replacement
A Long-Term Follow-Up of an Initial Series of
101 Patients
By B. G. BARRATT-BOYES, M.B., CH.M., A. H. G. RocmH, M.B., CH.B.,
P. W. T. BRANDT, M.B., CH.B., J. C. SMrIH, M.D.,
AND J. B. LowE, M.B., CH.B.
SUMMARYAn initial series of 101 patients with a homograft aortic valve has been reviewed from
4 to 6 years postoperatively. There were six hospital and 24 late deaths, eight of whichwere due to homograft valve failure. The 71 surviving patients were all symptomaticallyimproved. Anticoagulants were not used, and emboli were thought not to originatefrom the valve.
Important incompetence occurred in 27 patients and reoperation was undertaken in17 of these. The causes were peripheral leaking of the suture line, cusp rupture, bacterialendocarditis, and valve misplacement.
Leaflet calcification produced stenosis, requiring reoperation in two patients, andwas significant in eight other valves. Precipitating causes, present in eight of the 10cases, were imperfections in the original homograft, valve misplacement, or endocarditis.
Both cusp rupture and leaflet calcification were related to the method of valvepreparation as neither was encountered in untreated valves. For this reason, chemicalsterilization and freeze drying have been replaced by sterilization and storage in anantibiotic Hank's solution.
Additional Indexing Words:Homograft valve calcification Homograft leaflet rupture Myocardial diseaseHomograft aortic valve incompetence Homograft aortic valve stenosisCardiothoracic ratio Valve preparation
IN VIEW of the poor prognosis for patientswith severe aortic valve disease and the
low hospital mortality following aortic valvereplacement, it is reasonable to proceed withoperation in such patients. In this hospital theaortic homograft valve has been used foraortic valve replacement, and serial review hasindicated that in the majority of patients thisvalve functions satisfactorily and affords reliefof symptoms.1'2 The first 101 patients oper-ated upon during the first 2 years from theinception of this technic in August 1962 havenow been followed from 50 to 74 months, and
From the Cardiothoracic Surgical Unit, Green LaneHospital, Auckland, New Zealand.
Supported by a grant from the Auckland MedicalResearch Foundation.Circdation, Volume XL, December 1969
the results of this relatively long-termn follow-up are presented here in detail. This samegroup of patients was assessed 4 to 28 monthspostoperatively in an earlier report.3
Clinical MaterialForty-two patients presented with dominant or
pure aortic incompetence, 48 with dominant orpure calcific aortic stenosis, and 11 with bothaortic and mitral valve disease which requiredsurgical correction (10 in this category had aorticincompetence and one had stenosis).The symptomatic state and hospital morbidity,
together with the cause of the six hospital deathsin these 101 patients, have been presented in theprevious report3 and are not, therefore, detailedhere. Much of this information is given in latertables, where age, symptoms, cardiothoracic ratio,and electrocardiographic findings are related toearly and late mortality.
763
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

BARRATT7BOYES ET AL.
The surgical technic used was described in19644 and did not include either aortic roottailoring5 or vertical mattress sutures to obliteratemost of the dead space between graft and host,6both of these latter technics having beenintroduced later to lower t-he incidence ofhomograft valve incompetence.
Sixteen of the homograft valves were collectedunder sterile precautions and stored in Hank'ssolution containing 5,000 units of penicillin and0.2 ml of 50% streptomycin sulfate, hereafteroften referred to as "untreated valves," and a
further 23, also taken under sterile conditions,were freeze dried. Eight homografts were steril-ized with 1% beta propiolactone and stored inHank's solution and 54, also sterilized in this way,were freeze dried.
Late MortalitySeventy-one patients were alive at the time
of review and 66 were examined by one of us
(A.H.G.R.). For the remaining five, adequateclinical data were available from cardiologistsin other centers. Of the 24 late deaths, 13occurred in patients with preoperative aorticincompetence (31%), 10 in patients withstenosis (21%), and one in the multivalvegroup (10%). Eighteen either died in this unitor were seen shortly before death, and six diedelsewhere without being recently seen by us,
adequate data being available in five of these.When it has been brought to our attentionthat the cardiac status of a patient changedsubsequent to review here, the data have beenaltered accordingly, to November 1, 1968.The cause of late death was established by
necropsy in 22 of the 24 patients and is relatedto the time after operation in table 1.Reoperation for homograft valve incompe-
tence had been undertaken in seven of thesepatients (table 1), a second homograft valvebeing inserted.
Homograft Valve IncompetenceThis has been regarded as the major cause
of death in the eight patients regardless ofassociated causes of death, namely coronaryartery atheroma (present in two), moderateresidual mitral incompetence (present inone), or complete heart block (present inone). The valve incompetence was graded asmoderate or severe in these cases. Four ofthese patients died in hospital following a
second operation. The incompetence was dueto a peripheral leak in the suture line in threepatients; in the remaining five the leak was
central and due to cusp rupture in three,malpositioned valve in one, and endocarditisin one.
Coronary Artery AtheromaThese five patients were aged 51, 60, 62, 67,
and 72 at the time of death, which was
relatively sudden in all instances. The young-est was a diabetic, and another dying 4months following operation had had a prob-able infarct 2 months preoperatively. One hadsevere coarctation of the aorta, a congenitalmitral valve deformity with some stenosis, andintermittent complete heart block, beforeoperation and at the time of death.
CardiomyopathyMyocardial disease with congestive heart
failure and cardiomegaly was the cause ofdeath in six patients, aged 22, 29, 30, 53, 55,
Table 1
Late Mortality: Cause and Time of Death After Operation
Coronary DeathValve artery Myocardial Sudden unrelated Uncertain
Year of death failure atheroma disease death to heart cause Total
First 1 4 1 2(1) - 8(1)Second - - 1 - 2Third 3(2)* - 3(1) - 1 - 7(3)Fourth 2(1) 1 _- - 3(1)Fifth 2(1) I_ -1(1) 3(2)Sixth - 1-- - 1
Totals 8(4) 5 6(1) 2(1) 2 1(1) 24(7)
* Number of reoperations are given in parentheses.Circulation, Volume XL, December 1969
764
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

AORTIC HOMOGRAFT VALVE REPLACEMENT
and 59 at the time of death, which occurredfrom 11 to 71 months after operation. Theoriginal valve lesion was incompetence in fourand stenosis in two. Mild mitral valve diseasecontributed in one and essential hypertensionin another, but in the remaining four therewas no apparent reason for the onset ofcongestive heart failure and progressive car-
diomegaly within months of operation. Nec-ropsy was not performed in one case, but inthe remainder the left ventricle was grosslyhypertrophied with interstitial fibrosis. Moder-ate coronary artery atheroma was present inone and significant narrowing of the smallcoronary arteries by intimal fibrosis7 inthree.Sudden DeathSudden unexpected death, presumably from
arrhythmia, occurred in two asymptomaticpatients, 4 and 5 months after operation.While no obvious cause of death was found atnecropsy, the left ventricle in both showedmarked interstitial fibrosis and widespreadnarrowing of the small coronary arterieswithout significant proximal atheroma.
Unrelated CauseDeath unrelated to the heart occurred from
disseminated carcinoma of the prostate at 24months in one patient and from a stroke at 34months in another. The latter patient hadundergone carotid endarterectomy shortlybefore death.
Cause UncertainThe cause of death is uncertain in one
patient, dying overseas without autopsy 51months after operation. This patient had a
successful reoperation for recurrent incompe-tence 26 months prior to death. The likelycause was hypertensive heart failure.In summary (table 1), late death from
valve failure occurred in eight patients (8.4%of those leaving hospital) and myocardialfactors (coronary atheroma, cardiomyopathy,and arrhythmia) were responsible for all butthree of the remainder (14%).The majority (17) of the late deaths
occurred in the first 3 years, although deathsfrom valve failure were equally distributedbetween the first and second 3-year periods(table 1).
Table 2
Mortality Relative to Symptoms
MortalityLate
Symptoms No. of patients Hospital Myocardial* Other
Absent 0 0 0 0Effort dyspnea
only 12 1 1 1Angina or syncope 25 1 2 2Heart failure or
angina decubitus 64 4 10 8Totals 101 6 13 11
* Includes deaths due to coronary atheroma, cardiomyopathy, and arrhythmias (see tables3, 4, and 5).
Table 3
Mortality Relative to Cardiothoracic Ratio
MortalityCardiothoracic Late
ratio (%) Number of patients Hospital Myocardial Other
55 or less 38 2 2 456 to 60 32 2 4 661 to 75 31 2 7 1
Totals 101 6 13 11
Cirfceation, Volume XL, December 1969
765
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from
BARRATT-BOYES ET AL.
Table 4
Mortality Relative to Electrocardiogram Changes
MortalityNumber of Latepatients Hospital Myocardial Other
Mean frontal axisLeft axis deviation(axis less than -330) 16 0 8 100 to-30° 40 0 2 4Normal 45 6 3 6
Intraventricular conductionComplete bundle 6 0 2 0branch blockNormal 95 6 11 11
Table 5
Mortality Relative to Age at Operation
Valve lesion MortalityAge Aortic Aortic Total Late(yr) incompetence stenosis Multivalve patients Hospital Myocardial Other
10-19 5 0 0 5 0 0 020-2930-3940-4950-5960-69
Totals
876106
42
029
201748
35300
11
1114183023101
1 4 22 0 00 2 11 3 32 4 56 13 11
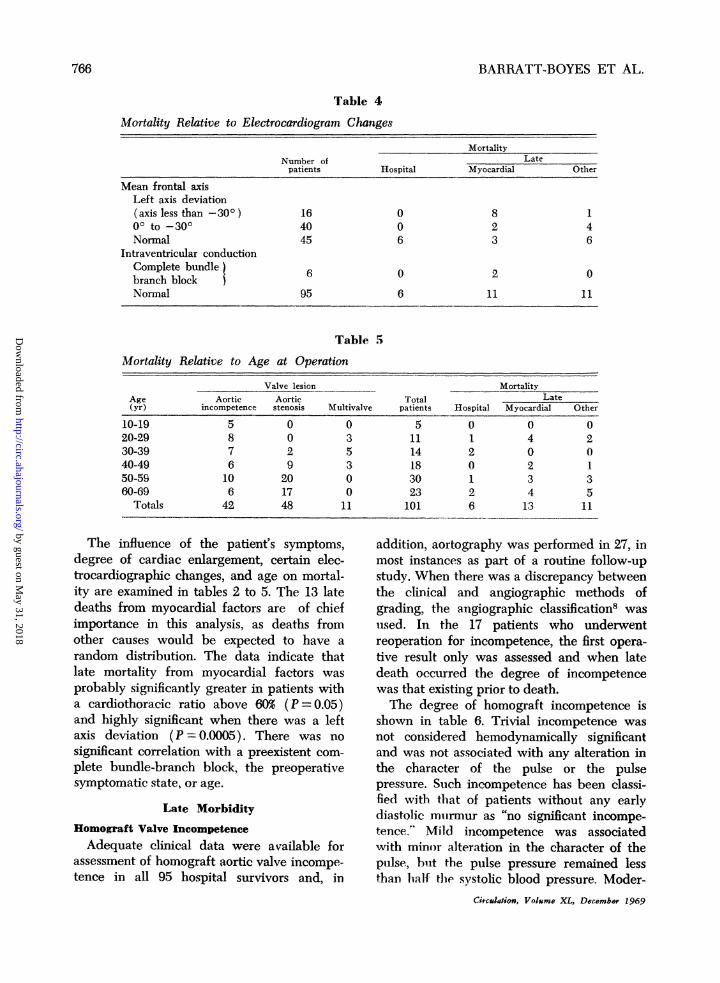
The influence of the patient's symptoms,degree of cardiac enlargement, certain elec-trocardiographic changes, and age on mortal-ity are examined in tables 2 to 5. The 13 latedeaths from myocardial factors are of chiefimportance in this analysis, as deaths fromother causes would be expected to have arandom distribution. The data indicate thatlate mortality from myocardial factors wasprobably significantly greater in patients witha cardiothoracic ratio above 60% (P = 0.05)and highly significant when there was a leftaxis deviation (P - 0.0005). There was nosignificant correlation with a preexistent com-plete bundle-branch block, the preoperativesymptomatic state, or age.
Late MorbidityHomograft Valve IncompetenceAdequate clinical data were available for
assessment of homograft aortic valve incompe-tence in all 95 hospital survivors and, in
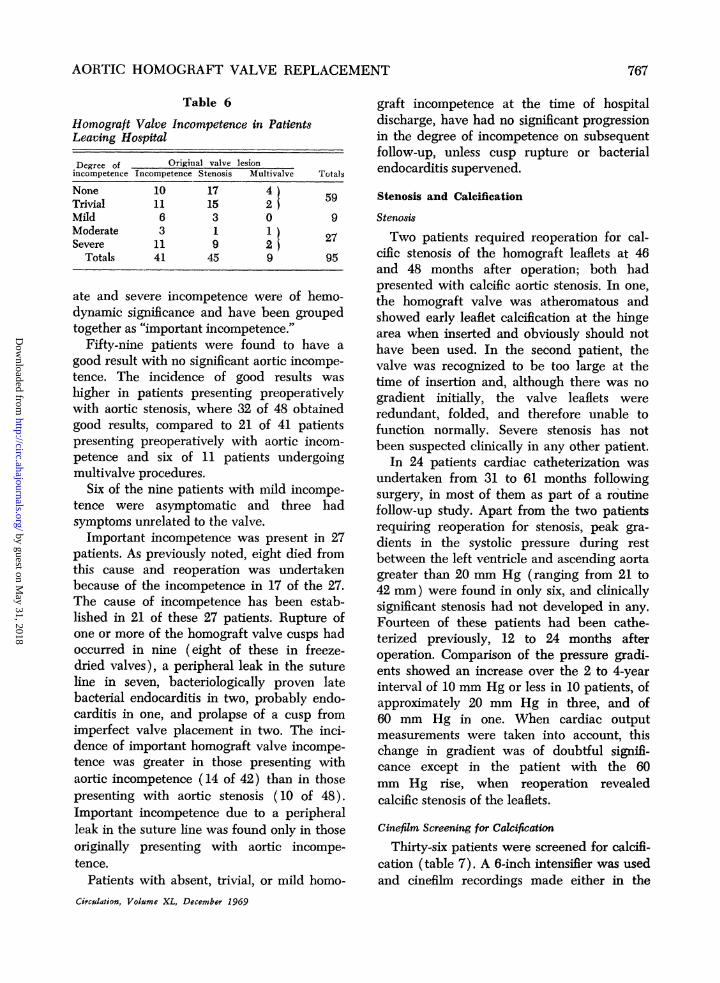
addition, aortography was performed in 27, inmost instances as part of a routine follow-upstudy. When there was a discrepancy betweenthe clinical and angiographic methods ofgrading, the angiographic classification8 wasuised. In. the 17 patients who underwentreoperation for incompetence, the first opera-tive result only was assessed and when latedeath occurred the degree of incompetencewas that existing prior to death.The degree of homograft incompetence is
shown in table 6. Trivial incompetence wasnot considered hemodynamically significantand was not associated with any alteration inthe character of the pulse or the pulsepressure. Such incompetence has been classi-fied with that of patients without any earlydiastolic murmur as "no significant incompe-tence." M;ild incompetence was associatedwith minor alteration in the character of thepulse, but the pulse pressure remained lessthan half the systolic blood pressure. Moder-
Circutatiou, Volume XL, December 1969
766
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from
AORTIC HOMOGRAFT VALVE REPLACEMENT
Table 6
Homograft Valve Incompetence in PatientsLeaving Hospital
Degree of Original valve lesionincompetence Incompetence Stenosis Multivalve Totals
None 10 17 4 5Trivial 11 15 2Mild 6 3 0 9Moderate 3 1 1 27Severe 11 9 2
Totals 41 45 9 95
ate and severe incompetence were of hemo-dynamic significance and have been groupedtogether as "important incompetence.'>
Fifty-nine patients were found to have a
good result with no significant aortic incompe-tence. The incidence of good results was
hiigher in patients presenting preoperativelywith aortic stenosis, where 32 of 48 obtainedgood results, compared to 21 of 41 patientspresenting preoperatively with aortic incom-petence and six of 11 patients undergoingmultivalve procedures.
Six of the nine patients with mild incompe-tence were asymptomatic and three hadsymptoms unrelated to the valve.Important incompetence was present in 27
patients. As previously noted, eight died fromthis cause and reoperation was undertakenbecause of the incompetence in 17 of the 27.The cause of incompetence has been estab-lished in 21 of these 27 patients. Rupture ofone or more of the homograft valve cusps hadoccurred in nine (eight of these in freeze-dried valves), a peripheral leak in the sutureline in seven, bacteriologically proven latebacterial endocarditis in two, probably endo-carditis in one, and prolapse of a cusp fromimperfect valve placement in two. The inci-dence of important homograft valve incompe-tence was greater in those presenting withaortic incompetence (14 of 42) than in thosepresenting with aortic stenosis (10 of 48).Important incompetence due to a peripheralleak in the suture line was found only in thoseoriginally presenting with aortic incompe-tence.
Patients with absent, trivial, or mild homo-
Circulation, Volume XL, December 1969
graft incompetence at the time of hospitaldischarge, have had no significant progressionin the degree of incompetence on subsequentfollow-up, unless cusp rupture or bacterialendocarditis supervened.
Stenosis and Calcification
Stenosis
Two patients required reoperation for cal-cific stenosis of the homograft leaflets at 46and 48 months after operation; both hadpresented with calcific aortic stenosis. In one,the homograft valve was atheromatous andshowed early leaflet calcification at the hingearea when inserted and obviously should nothave been used. In the second patient, thevalve was recognized to be too large at thetime of insertion and, although there was nogradient initially, the valve leaflets wereredundant, folded, and therefore unable tofunction normally. Severe stenosis has notbeen suspected clinically in any other patient.
In 24 patients cardiac catheterization wasundertaken from 31 to 61 months followingsurgery, in most of them as part of a routinefollow-up study. Apart from the two patientsrequiring reoperation for stenosis, peak gra-dients in the systolic pressure during restbetween the left ventricle and ascending aortagreater than 20 mm Hg (ranging from 21 to42 mm) were found in only six, and clinicallysignificant stenosis had not developed in any.Fourteen of these patients had been cathe-terized previously, 12 to 24 months afteroperation. Comparison of the pressure gradi-ents showed an increase over the 2 to 4-yearinterval of 10 mm Hg or less in 10 patients, ofapproximately 20 mm Hg in three, and of60 mm Hg in one. When cardiac outputmeasurements were taken into account, thischange in gradient was of doubtful signifi-cance except in the patient with the 60mm Hg rise, when reoperation revealedcalcffic stenosis of the leaflets.
Cinefilm Screening for CalcificationThirty-six patients were screened for calcifi-
cation (table 7). A 6-inch intensifier was usedand cinefilm recordings made either in the
767
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

BARRATT-BOYES ET AL.
Table 7Postoperative Cinefilm Screening for Valve Calcification (6-Inch Intensifier)
CalcificationAortic wall Homograft
Preoperative lesion No. of patients Absent Grade 1 Grade 2 Grade 3 cusp
Incompetence 14 3 7 2 2 0Calcific stenosis 22 1 7 10 4 1
Totals 36 4 14 12 6 1
lateral projection at the time that an aorto-gram was performed (16) or in three separateprojections (20).
In four patients no calcification could beseen in the aortic root region. Scattered flecksof calcification were seen in the aortic wall ofthe remaining 32, but in only one (one of thetwo patients requiring reoperation for steno-sis) was calcification considered to be in cusp
tissue because of the relative movementbetween cusps and aortic ring. The extent ofcalcification was limited to sparsely scatteredflecks, which were not visible using a 9-inchintensifier (grade 1) in 14 patients. Morenumerous flecks of calcification of mild tomoderate extent (grade 2) were seen in 12,and more extensive calcification, usually in-
volving the entire circumference of the aorticring (grade 3) in six, this including the tworequiring reoperation for homograft stenosis,but in all instances the calcification was
considerably less than that seen in patientspresenting with calcific aortic stenosis.
In the group with preoperative aorticincompetence (table 7) late calcification maybe more significant than in patients withcalcific aortic stenosis, where some calciumwas usually left behind in the valve bed, for itwas not possible to differentiate betweencalcification in the homograft aortic remnantand host aortic root. Analysis of the fourpatients with preoperative incompetence andgrades 2 or 3 aortic wall calcification indi-cated, however, that three had heavy calcifi-cation of the aortic root preoperatively (intwo this was syphilitic in origin) and the otherhad late bacterial endocarditis which hadpresumably produced the calcification.Gross and Microscopic Calcification
Valves obtained at autopsy or reoperation
less than 3 years after insertion rarely showedcalcification, and when present it was neversignificant. After 3 years, however, calcifica-tion was visible to the naked eye in both theaortic remnant of the graft and the leaflets in12 of the 18 specimens. A detailed descriptionof these valves follows.
Aortic wall calcification was evident micro-scopically in every case but was trivial in six ofthe 18 where the deposits were confined totissue compressed by sutures at the upper orlower margins of the graft. In nine casescalcification, while never bulky, involved thewhole graft annulus in circumferential fashionwith scattered or confluent foci in other partsof the aortic remnant. In the remaining three,calcification was intermediate in extent.
Leaflet tissue calcification was absent in fivespecimens (36, 37, 40, 40, and 60 monthspostoperatively) and trivial in three (36, 47,and 70 months postoperatively). In thesethree it presented as an isolated deposit inacellular graft collagen in the right cusp notvisible macroscopically in one specimen, andas a single tiny vegetation in the other two.Significant leaflet calcification was noted inthe remaining 10 specimens. It was of a milddegree and not sufficient to interfere withleaflet function in five (fig. 1) and moderateto severe in five (44, 46, 47, 48, and 56 monthspostoperatively). In two of these five speci-mens the calcification had produced valvestenosis, and in three it was associated withdominant incompetence. Precipitating causeswere present in eight of the 10 valves withsignificant calcification, namely, imperfectionsin two of the grafts when they were inserted(early leaflet calcification and a bicuspidhomograft); one valve was too large and theleaflets were folded and redundant; in three
Circulation, Volume XL, December 1969
768
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

AORTIC HIOMOCRAFT VALVE REPLACEMENT
Figure I
Cross fiesh specim-ten of horrioAgraft yolve removed surgically at 36 miionthts because of moderateaortic incomipetence due mataitn to a peripheral suture line leak. The valve had been twistedslightly durin-tg inisertion so that cusp approximation was also imperfect. Calcified nodules arepresenit in the leaflets but they do rot itnterfere with leaflet movement. Harnograft sterilizedwith beta propiolactone anid stor-ed in Hank's solution.
there was mnajor associated peripylheral -spacefilling anid leak with resultant leaflet distor-tion; and in two, proven endocarditis. It isperhaps significant that all five valves withmoderate to severe leaflet calcification camefrom patients who presented initially withheavy aortic root anid leaflet calcification.
There was no clear correlation between thedegree of leaflet calcification and the methodof valve preparatiorn. However, the twountreated valves available for examinration 40and 60 months after operation were free ofcalcification (table 8). Moreover, althougheight of the 10 valves witlh significantcalcification had been freeze dried, five of theeight with absent or trivial calcification werealso freeze dried, including the specimenexamined at 70 montlhs.
In sumnmary, it would appear that calcifica-tion invariably occurred in the aortic wallGCrcoianion, Volumne XL, December 1969
remnanit of the graft after 3 years, but wasconfined to tissue compressed by sutures' inone third of the specimens and was apparentinacroscopically in onily two thirds. It was nota cause of outflow obstruction, Leaflet calcifi-cation was significant in 10 of 18 specimens. Itwas a cause of stenosis, however, in only twopatients. In five of the 10 specimens exhibitingleaflet calcification, the deposits were smalland in eight (including the two with stenosis)precipitating factors were present. It was ofinterest that both the untreated valves ex-amined after 3 years were free of leafletcalcification.
Complete Heart BlockPernanent complete heart biock, niot pres-
ernt preoperatively, occurred in two patients,although in one it did not appear until 6months after operation. Implantable pace-makers were inserted into both; one remains
769
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

CZ cea) 000P4m m
I I I I I t
"
I I I I KtI0
II O I I
BARRATT-BOYES ET AL.
C) Cd
"e0 0 0 0 0 0 Po 0, zz Z z ez
I o o
II 10=00000
I Iq)0) 4) C)
I I I4 C)-c M 0 C' C
0 -
C "o r .-0
~04
eq= U t0̂0c
-T
eq
q
cv
>Cm C C4
C)-, C
CIS0
10
CC)
0 0D
"-4
10cD
1010
co r
tx~~~~*0
0~~~~~~~
C)e =i*C) CtC
CDe 00 00co 00V
1 XCCO o Chv CY) P-00ZZZZ000qm"0Z co
Ci4". 0o
C)11cnC)
t S C C C t o X~0
. 44
V)>
<¢w¢ ¢ - ¢ < < a44 4
00 O) o -4 cq cs oQo*
Crculation, Volucme XL, De)cember 1969
770
U2
c4 E
r.
u;I.?C1
E
be 4-
404
Cl) C
444.
200z 0
CZ =4J0
0
o n
v0
0
r.S
0
a._
0
Q
C0
co
1.
0
0
la
03
C)~t31.24)
Q120gC).b00
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

AORTIC HOMOGRAFT VALVE REPLACEMENT
well 5 years after surgery, and the other diedat reoperation for homograft incompetence 3years after surgery.
Systemic EmboUThree patients suffered transient visual loss
in the early postoperative period and in onethis was associated with aphasia of a few daysduration. These episodes were probably dueto platelet emboli from the healing suture lineof the valve, as these were seen in the retinalarteries in one patient. Three patients havebeen thought to have had systemic emboli at alater stage. One patient suddenly developedpain in the left side of the body 2 months afteroperation, at a time when his heart revertedfrom atrial fibrillation to sinus rhythm, and hehas residual hemi-anesthesia; one patientsuffered transient obscuration of vision associ-ated with bacterial endocarditis 5 years aftersurgery, and one multivalve patient with aStarr-Edwards mitral valve prosthesis had anepisode of ataxia lasting several days, with
104
8(
7A
64
54
44
o\L*6
t ( ): death due to valve failure
Q ~~~~x(73)3 (2)
REOPERATION 12
AORTIC INCOMPETENCE 6
symptoms 10
GOODVALVE
<asymptomatic43;FUNCTIONasymptomatic 43
0)
0
3J
SurvivalI 2 3 4YEAR OF FOLLOW-UP
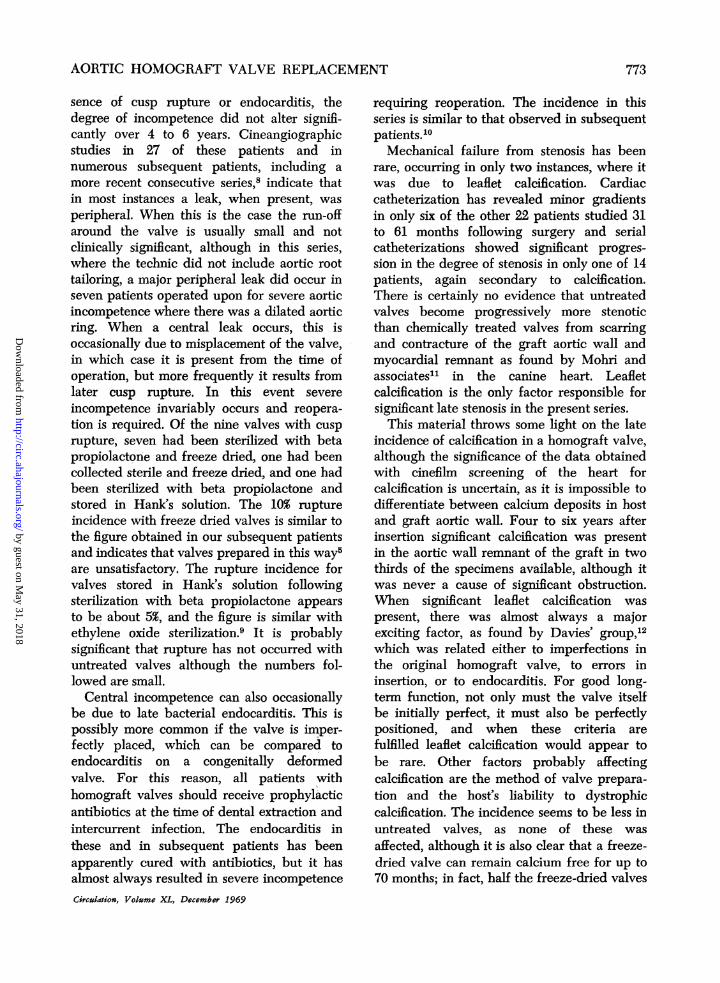
Figure 2
CURRENTSTATUS
Annual survival and final assessment at follow-up 50to 74 months after operation.
Circudation, Volume XL, December 1969
complete recovery. Possible systemic embo-lism has occurred in four others. Thispresented as transient visual loss in two olderpatients, one with associated mitral valvedisease and atrial fibrillation and as a stroke intwo patients, both with known cerebrovascu-lar disease and severe widespread arterio-sclerosis. Anticoagulants were not used post-operatively, except in the four multivalvepatients with a Starr-Edwards mitral prosthe-Sis.
Symptomatic Result (Fig. 2)At the time of review all 71 surviving
patients were symptomatically improved.Forty-three were symptom free or sufferedfrom mild effort dyspnea only and did nothave important incompetence of the homo-graft valve. Forty of these showed a convinc-ing reduction in heart size and in 31 thecardiothoracic ratio was less than 55%.
Significant symptoms not related to dys-function of the homograft valve were presentin 10. In six, symptoms were secondary tocoronary atheroma, in three to mitral valvedisease, and in one to asthma.Five patients with moderate or severe aortic
incompetence were asymptomatic, and four ofthese were actively employed, while onepatient with moderate aortic incompetencehad moderate effort breathlessness but wasimproved by her operation.Twelve patients were alive following reop-
eration, which in three was too recent to assessthe result. In seven a good result was achievedand in two minor symptoms only werepresent, but incompetence had recurred.
Result with Untreated ValvesAs particular interest attaches to the valves
which were collected sterile and stored for 1to 26 days in Hank's solution, the outcome inthe 16 patients receiving these valves has beensummarized in table 8.Two patients died 4 and 16 months
postoperatively from myocardial factors withgood valve function, and three underwentsuccessful reoperation at 9, 40, and 60 monthsbecause of valve incompetence resulting from
771
3N by guest on M
ay 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

BARRATT-BOYES ET AL.
either technical error or probable late endo-carditis, a second (chemically treated)valve being inserted. Eleven were avail-able for review with the untreated valvestill functioning 55 to 74 months postopera-tively. Of these, all were symptomaticallyimproved and seven were symptom free.
Five valves were available for histologicexamination, the findings on which are to bereported separately. In brief, all the leafletscontained fibroblasts, the number varyingwith the duration of graft storage and thelength of time it had been in the host. Thecollagenous and elastic tissue were wellpreserved, and there was no leaflet calcifica-tion. The specimen obtained 60 months afteroperation (fig. 3) had pliable cusps of normalthickness, with well-preserved elastic tissueand rather more fibroblasts than normal. Theonly calcification present was a small fragmentadjacent to sutures in the graft aortic wall.The aortic root calcification noted on cine
Figure 3Gross fixed specimen of homograft valve removedsurgically at 60 months because of severe incompe-tence, due to malplacement with prolapse of one cusp.
Incompetence, was initially moderate but had increasedslightly over the 5 years. Leaflets appear normal andmicroscopically there was good preservation of col-lagenous and elastic tissue and a slightly increasednumber of fibroblasts and no calcification. Homograftcollected sterile and stored in Hank's solution for 5
days (see case 5 and table 8).
film study was grade 2 in two patients withheavy valve calcification preoperatively andgrade 3 in case 10 in which heavy syphiliticcalcification was present preoperatively in theaortic wall.
Important incompetence was present in fivevalves. As noted above, three patients (cases3, 4, and 5) required reoperation. In case 10,cineangiography demonstrated a peripheralleak in the suture line. With the exception ofcase 4, the degree of incompetence had notchanged significantly over the years. Cusprupture was not encountered.The systolic pressure gradient across the
valve was measured in 10 of these patientsbetween 1 and 2 years or at an average of 59months postoperatively or both. It was trivialin all instances and showed no significantincrease between the early and late studies.
DDiscussionThis review of our first 101 patients allows a
detailed and accurate assessment of thebehavior of a homograft valve over a 4 to 6-year period. As three quarters of the valveswere freeze dried5 and most were sterilized bybeta propiolactone, the results relate chiefly tothis method of valve preparation and storage.However, 16 of the earliest grafts wereuntreated (collected sterile and preserved inHank's solution) so that these two methodscan be compared.The results indicate that all 71 surviving
patients are symptomatically improved and53, or approximately half the total numberoperated upon, have good functioning of thehomograft valve. In six there is importantresidual incompetence with few or no symp-toms, but in 12 survivors reoperation wasrequired for valve failure. As a total of 19patients were reoperated upon, and fourothers died from incompetence without reop-eration, the valve failed completely in 23 ofthe 95 patients leaving the hospital (in 21from incompetence and in two from stenosis).
Clearly the major cause of mechanicalfailure has been incompetence, althoughapproximately two thirds of the patientsleaving the hospital had absent or only trivialincompetence subsequently and, in the ab-
Circulasion, Volume XL, December 1969
772
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from
AORTIC HOMOGRAFT VALVE REPLACEMENT
sence of cusp rupture or endocarditis, thedegree of incompetence did not alter signifi-cantly over 4 to 6 years. Cineangiographicstudies in 27 of these patients and innumerous subsequent patients, including amore recent consecutive series,8 indicate thatin most instances a leak, when present, wasperipheral. When this is the case the run-offaround the valve is usually small and notclinically significant, although in this series,where the technic did not include aortic roottailoring, a major peripheral leak did occur inseven patients operated upon for severe aorticincompetence where there was a dilated aorticring. When a central leak occurs, this isoccasionally due to misplacement of the valve,in which case it is present from the time ofoperation, but more frequently it results fromlater cusp rupture. In this event severeincompetence invariably occurs and reopera-tion is required. Of the nine valves with cusprupture, seven had been sterilized with betapropiolactone and freeze dried, one had beencollected sterile and freeze dried, and one hadbeen sterilized with beta propiolactone andstored in Hank's solution. The 10% ruptureincidence with freeze dried valves is similar tothe figure obtained in our subsequent patientsand indicates that valves prepared in this way5are unsatisfactory. The rupture incidence forvalves stored in Hank's solution followingsterilization with beta propiolactone appearsto be about 5%, and the figure is similar withethylene oxide sterilization.9 It is probablysignificant that rupture has not occurred withuntreated valves although the numbers fol-lowed are small.
Central incompetence can also occasionallybe due to late bacterial endocarditis. This ispossibly more common if the valve is imper-fectly placed, which can be compared toendocarditis on a congenitally deformedvalve. For this reason, all patients withhomograft valves should receive prophylacticantibiotics at the time of dental extraction andintercurrent infection. The endocarditis inthese and in subsequent patients has beenapparently cured with antibiotics, but it hasalmost always resulted in severe incompetenceCirculation, Volume XL, December 1969
requiring reoperation. The incidence in thisseries is similar to that observed in subsequentpatients.10Mechanical failure from stenosis has been
rare, occurring in only two instances, where itwas due to leaflet calcification. Cardiaccatheterization has revealed minor gradientsin only six of the other 22 patients studied 31to 61 months following surgery and serialcatheterizations showed significant progres-sion in the degree of stenosis in only one of 14patients, again secondary to calcification.There is certainly no evidence that untreatedvalves become progressively more stenoticthan chemically treated valves from scarringand contracture of the graft aortic wall andmyocardial remnant as found by Mohri andassociates1' in the canine heart. Leafletcalcification is the only factor responsible forsignificant late stenosis in the present series.
This material throws some light on the lateincidence of calcification in a homograft valve,although the significance of the data obtainedwith cinefilm screening of the heart forcalcification is uncertain, as it is impossible todifferentiate between calcium deposits in hostand graft aortic wall. Four to six years afterinsertion significant calcification was presentin the aortic wall remnant of the graft in twothirds of the specimens available, although itwas never a cause of significant obstruction.When significant leaflet calcification waspresent, there was almost always a majorexciting factor, as found by Davies' group,12which was related either to imperfections inthe original homograft valve, to errors ininsertion, or to endocarditis. For good long-term function, not only must the valve itselfbe initially perfect, it must also be perfectlypositioned, and when these criteria arefulfilled leaflet calcification would appear tobe rare. Other factors probably affectingcalcification are the method of valve prepara-tion and the host's liability to dystrophiccalcification. The incidence seems to be less inuntreated valves, as none of these wasaffected, although it is also clear that a freeze-dried valve can remain calcium free for up to70 months; in fact, half the freeze-dried valves
773
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

BARRATT-BOYES ET AL.
examined had no calcification or only a trivialamount. The factors influencing the hostliability to dystrophic calcification are un-
known but are certainly important. Forexample, the rarity of calcific aortic stenosisamong the Asian and Chinese people needsdocumentation and irnvestigation. It may besignificant that in this series all five patientswith marked homograft leaflet calcificationhad heavy valve calcification before operation.The causes of late mortality in the 24
patients differ from those reported with aStarr-Edwards aortic prosthesis. Thus, onlyone third of our patients died from valvefailure compared with two thirds of the totallate deaths in Herr and co-workers' series'3and about one half in the Mayo Clinic series.'4This difference is largely explained by thevirtual if niot complete absence of emboli froma homograft valve in this and other reportedseries12 and of deaths due to complicationsof long-tenn anticoagulation, which is notrequired with a homograft valve. It is alsoworth noting that, in contrast to thromboem-bolism and ball variance, homograft valvefailure from whatever cause, including cusp
rupture, has never resulted in sudden death,and reoperation with insertion of a secondhomograft valve is technically little differentfrom the first procedure. While seven deathsfollowed reoperation on 19 patients in thisseries (two for stenosis and 17 for incompe-tence), four of these deaths were directlyrelated to late referral of moribund patients.Now that cusp rupture is a recognized clinicalentity, this seldom occurs.
Myocardial factors, including coroniaryatheroma, cardiomyopathy, essential hyper-tension, and arrhythmia, were the cause of 13and probably 14 of the late deaths in thisseries. Coronary atherosclerosis accounted forfive deaths in diabetic or elderly subjects, as
well as being the probable cause of persistentangina in six others with good valve function.Primary myocardial disease or cardiomyop-athy with progressive cardiomegaly andcongestive heart failure despite good valvefunction and the absence of coronary athero-sclerosis was the cause in six patients. It is
possible that extensive myocardial fibrosisoften associated with mural vessel disease7may be irreversible in patients with long-standing severe aortic valve disease, despitecorrection of the valve lesion. The fact,however, that only eight subsequent patientshave followed this course in the next 400operations up to December 1967, suggests thatcoronary artery perfusion technics, particular-ly over perfusion, played a part in this earlyseries. The data indicate that deaths due tomyocardial factors were more common inpatients with a large heart or a left axisdeviation, although there was no correlationwith symptomatic severity or age.The current value of this review is limited
by the fact that it represents our earliestexperience of an original and difficult technicwhich has required modification as furtherexperience has been gained. Firstly, altera-tions in the method of valve insertion, namely,additional sutures to obliterate most of thedead space between graft and host aortic walland aortic root tailoring when the root islarge, have virtually abolished significant leakaround the graft.8 Secondly, importantchanges have been made in the method ofhomograft valve preparation, in the hope ofdiminishing cusp rupture and late calcifica-tion. Chemical sterilization results in a deadhomeostatic graft with acellular leaflets whichare not adequately supported or replaced byhost tissue and may subsequently rupture.7There is also a definite, although low inci-dence of important leaflet calcification within4 to 6 years. Conversely, the untreated graftsstored in antibiotic Hank's solution haveneither ruptured nor calcified and the onespecimen examined at 5 years contained anear-normal number of fibroblasts. Because ofthese observations, valves are now collected ascleanly as possible by the pathologist andplaced in Hank's solution, containing penicil-lin, streptomycin, kanamycin, and amphoteri-cin B, for a minimum of 14 days at 4C.15While such grafts may not be vital,16 it isanticipated that cusp rupture will be rare andthe long-term behavior superior to eitherchemically treated or irradiated valves.'7
Circulation, Votame XL, December 1969
774
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

AORTIC HOMOGRAFT VALVE REPLACEMENT
Comparison of these results, in which 71% ofall patients operated upon were alive 4 to 6years later, with those achieved with otherprosthetic devices is difficult, as no trulycomparable data are available. Effler andassociates,18 however, report that, with a Starr-Edwards aortic prosthesis, 53% of their pa-tients leaving hospital were alive after 4 to 6years; from the figures given by Cooleyand associates,19 the 4 and 5-year survival forall patients undergoing isolated aortic valvereplacement with a prosthetic device wouldappear to be approximately 51%. Thesecomparative figures should be correlated withthe fact that, after the fourth year, thehomograft valve data show a decreasingmortality (fig. 2) and a minor morbidity fromendocarditis and leaflet calcification only. Incontrast, the aortic ball valve data are reportedto show a high late incidence of ballvariance3 20 and a continuous morbidity fromembolization13 18 and hemolytic anemia.13 Itremains to be seen whether the changes inhomograft preparation will further improvethe long-term function of this graft andwhether changes in ball-valve design willreduce the incidence of ball variance andthromboembolism and eliminate the need foranticoagulants.
AcknowledgmentTwenty-one of these patients were operated upon
by Dr. D. S. Cole.
References1. BAR,RATr-BoymS, B. G.: Homograft replacement
for aortic valve disease. Mod Conc CardiovascDis 36: 1, 1967.
2. BARRATT-BoYEs, B. G., ROCHE, A. H. G., ANDCOLE, D. S.: Aortic homograft valve replace-ment: A review of 511 patients with a latefollow-up extending to 65 months. J Cardio-vase Surg. In press.
3. BARRATT-BOYES, B. C., LOWE, J. B., CoLE, D. S.,AND KELLY, D. T.: Homograft valve replace-ment for aortic valve disease. Thorax 20: 495,1965.
4. BARRAT-r-BoYEs, B. G.: Homograft aortic valvereplacement in aortic incompetence and steno-sis. Thorax 19: 131, 1964.
5. BARRATT-BoYEs, B. G.: Method for preparingand inserting a homograft aortic valve. Brit JSurg 52: 847 ,1965.
6. GONZALEZ-LAvIN, L., AND BARRATT-BOYES, B. G.:
Circulation, Volume XL, December 1969
Sturgical considerations in the treatment ofventricular septal defect associated with aorticvalvular incompetence. J Thor Cardiovasc Surg57: 422, 1969.
7. SMITH, J. C.: Pathology of human aortic valvehomografts. Thorax 22: 114, 1967.
8. BRANDT, P. W. T., RocHE, A. H. G., BARumTr-BoYES, B. G., AND LowE, J. B.: Radiology ofhomograft aortic valves. Thorax 24: 129,1969.
9. Rocn, A. H. G., BARRATr-BoYEs, B. G., ANDHITcHCocK, G.: Cusp rupture in homograftaortic valves. Unpublished data.
10. CLARKSON, P., AND BARRArr-BoYEs, B. G.:Endocarditis in homograft aortic valves. Un-published data.
11. MoHRI, H., REICHENBACH, D. D., BARNES, R.W., AND MERENDINO, K. A.: A biological studyof the homologous aortic valve in dogs. J ThorCardiovasc Surg 54: 622, 1967.
12. DAVEEs, H., MIssEN, G. A. K., BLANDFORD, G.,ROBERTS, C. I., LEssoF, M. H., AND Ross, D.N.: Homograft replacement of the aorticvalve: A clinical and pathological study. AmerJ Cardiol 22: 195, 1968.
13. HERR, R. H., STARR, A., PiEwIE, W. R., WOOD, J.A., AND BIGELOW, J. L.: Aortic valvereplacement: A review of six years experiencewith the ball-valve prosthesis. Ann ThoracSurg 6: 199, 1968.
14. DuvoIsiN, G. E., WALLACE, R. B., ELLIs, F. H.,JR., ANDERSON, M. W., AND MCGOON, D. C.:Late results of cardiac valve replacement.Circulation 37 X suppl. II): II-75, 1968.
15. BARRATT-BOYES, B. 0., AND ROCHE, A. H. G.: Areview of aortic valve homografts over a six-and-one-half year period. Ann Surg. 170: 483,1969.
16. LOWER, R. R., PILLSBURY, R. C., ANGELL, W. W.,AND KosEK, J. C.: Homograft heart valves.Circulation 23 (suppl. I): I-135, 1966.
17. MALM, J. R., BowMAN, F. O., JR., HARmS, P. D.,AND KowALIy, A. T. W.: An evaluation ofaortic valve homografts sterilized by electronbeam energy. J Thor Cardiovasc Surg 54: 471,1967.
18. EFFLER, D. B., GROVES, L. K., AND FAVALORO, R.G.: Cumulative experience with ball-valveprosthesis: Late results in the replacement ofaortic valves. In Prosthetic Heart Valves,Brewer, L. A., III, ed. Springfield, Illinois,Charles C Thomas, 1969, p. 515.
19. COOLEY, D. A., ET AL.: Long-term results aftercardiac valve replacement: Clinical experiencewith 2,097 patients. In Prosthetic Heart Valves,Brewer, L. A., III, ed. Springfield, Illinois,Charles C Thomas, 1969, p. 530.
20. STARR, A. W.: Proceedings of cardiac surgeryconference. Med J Aust 2: 1013, 1968.
775
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

B. LOWEB. G. BARRATT-BOYES, A. H. G. ROCHE, P. W. T. BRANDT, J. C. SMITH and J.
Series of 101 PatientsAortic Homograft Valve Replacement: A Long-Term Follow-Up of an Initial
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1969 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.40.6.763
1969;40:763-775Circulation.
http://circ.ahajournals.org/content/40/6/763located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from





























