Embed Size (px)
Citation preview

L A N I E A L P H I N , S P T
Shoulder Mobilizations: When the Rolls and Glides Don’t Apply

Anatomy Review
� Convex humeral head � Concave glenoid fossa
¡ Faces anteriorly, laterally, and superiorly
¡ Glenoid labrum deepens socket and provides attachment point for capsule
� Passive supports: ¡ Superior, middle, and
inferior GH ligaments ¡ Coracohumeral ligament
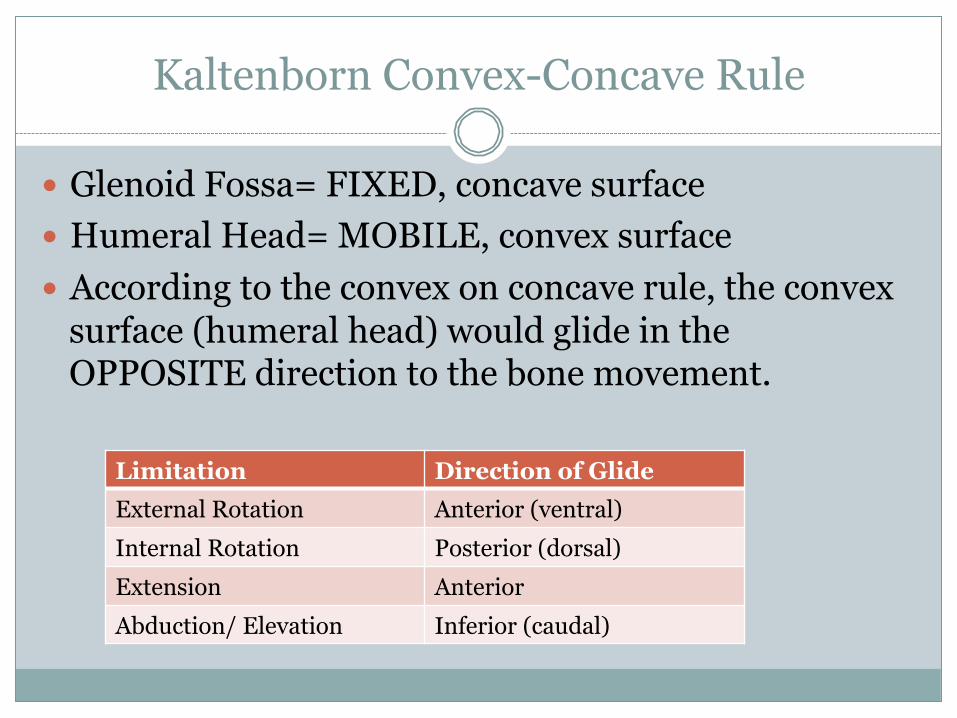
Kaltenborn Convex-Concave Rule
� Glenoid Fossa= FIXED, concave surface � Humeral Head= MOBILE, convex surface � According to the convex on concave rule, the convex
surface (humeral head) would glide in the OPPOSITE direction to the bone movement.
Limitation Direction of Glide External Rotation Anterior (ventral)
Internal Rotation Posterior (dorsal)
Extension Anterior
Abduction/ Elevation Inferior (caudal)
So, why is it not that simple?
� Traditional rolls and glides have been found to be unreliable in the glenohumeral joint.
� Several studies of GH kinematics have concluded that shoulders behave differently depending on the integrity of surrounding passive and active structures.
An Evidence-Based Review on the Validity of the Kaltenborn Rule as Applied to the Glenohumeral Joint
� Capsule/Ligaments AND neuromuscular control influence the translation of the humeral head ¡ Capsule + ligaments responsible for obligatory translation at the end rage ¡ The stabilizing effect of the rotator cuff on the humeral head causes a
centering motion ÷ ANY issue with rotator cuff may disrupt normal translational patterns
� Pain, muscle spasm, and loss of proprioception associated with shoulder dysfunction may lead to changes
� Imbalance/incoordination of the shoulder musculature may influence the translation of the humeral head

Take-Home Message
� So far, all we can be sure of is that evidence indicates the arthrokinematics for normal and dysfunctional joints are different.
� The review authors suggested that clinical judgment must be used to determine direction of mobilization.

Glenohumeral Joint Kinematics Related to Minor Anterior Instability of the Shoulder at the End of the Late Preparatory Phase of Throwing
� Translation was found to be in the OPPOSITE direction during active horizontal extension with ER ¡ SAME direction during active abduction in joints with anterior
instability or with rotator cuff tears
� The humeral head remained centered during active abduction in normal shoulder joint
� Again, the evidence indicates different arthro-kinematic behavior for normal and dysfunctional joints ¡ Effected by BOTH passive and active structures

Normal and abnormal mechanics of the glenohumeral joint in the horizontal plane.
� Control group: the humeral head was centered throughout motion in the horizontal plane ¡ Except maximum extension and external rotation: the cocked
stage of the throwing ÷ The center of the HH rested ~4 mm posterior to the center of the
glenoid
� In seven of the twelve patients who had anterior instability, abnormal mechanics were observed: anterior translation of the HH. ¡ This indicates a significant disruption of the structures
responsible for containing the humeral head within the glenoid fossa.

So, how do you determine direction of mobilization if you don’t know the direction of the translation?
Recent research has provided some guidance with ER
mobilizations, especially with regards to adhesive capsulitis.

Defining Adhesive Capsulitis
Adhesive Capsulitis: � Primary: insidious onset � Secondary: result of known associated condition
¡ Stroke, fracture, dislocation, OA � Multiregional synovitis with capsular contractions � Loss of ER in various levels of ABD � Gradual and progressive onset of pain
¡ likely sleep-disturbing night pain ¡ pain at end ranges of movements
� Painful and restricted active and passive ROM in both elevation and rotation that occurs for at least 1 month and has either reached a plateau or worsened

The Effect of Anterior Versus Posterior Glide Joint Mobilization on External Rotation Range of Motion in Patients With Shoulder Adhesive
Capsulitis
� Purpose: Determine direction of mobilization to achieve greatest increase in GH ER ROM.
� Methods: ¡ 20 subjects with primary adhesive capsulitis (4 men, 16
women; ages 37-66 ) ÷ Goal to include patients with ER ROM limitations resulting from
capsular tightness, not muscular. ¢ ER ROM decreases with Abd
÷ Presumed to be in Neviaser’s stage II to IV ¡ Randomly assigned to 2 groups: Anterior or Posterior Mob ¡ Active ER was measured by experienced PTA who was blinded
to intervention group
Intervention
� US prior to mobilization 1 or 3 MHz, 1.5 W/cm2, continuous, 10 min
� Mobilizations: lateral traction with Grade 3 Ant or Post mobilization, held at end range for 1 min, no oscillation ¡ Ant Mobilization: progression from supine, end range Abd/ER à
prone, end range Abd/ER ¡ Post Mobilization: progression from end range Abd/ ER à end range
Flex/ ER ÷ Giving way, audible “pop” noted
¡ Total time: 15 min � UBE 3 min forward direction after mobilization to reduce
soreness � Total of 6 treatments, 2-3x per week

Anterior Mobilization

Posterior Mobilization

Results
� Ant Mob group: ¡ 2 subjects lost external rotation ROM (–16° and –13°) ¡ 1 had no change (0°) ¡ 7 showed improvement (3°-18°)
� Post Mob group: ¡ ERROM improved in all subjects (22°-45°)
� Largest improvement for the Ant Mob group (18°) was less than the smallest ROM improvement for the Post Mob group (22°)
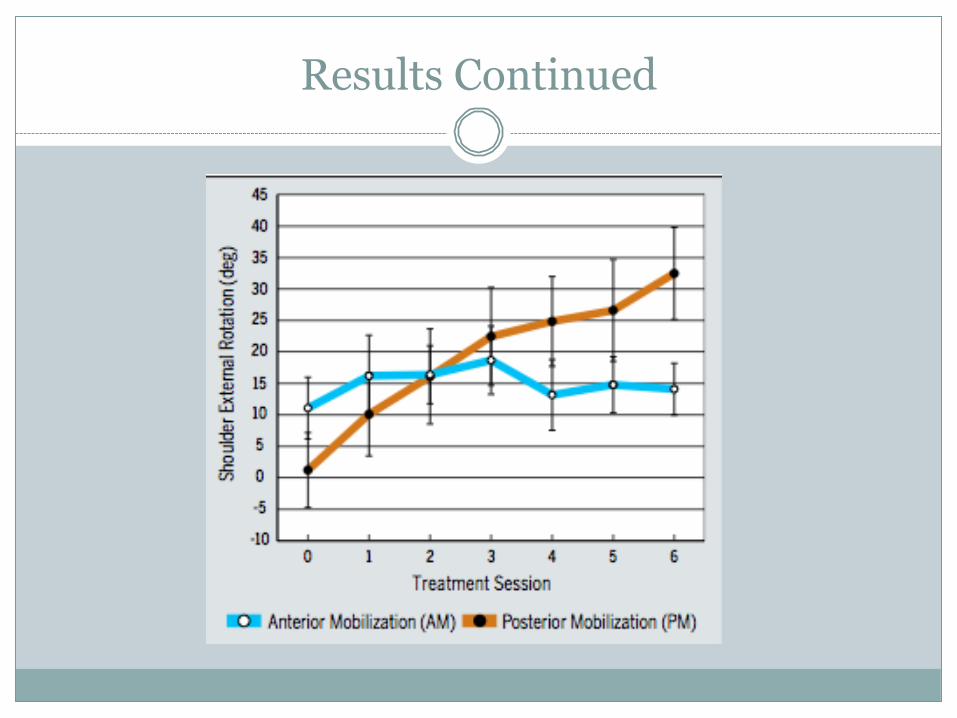
Results Continued

Other Findings to Suggest a Posterior Mobilization in This Population
� Posterior gliding manipulation found marked increases in external rotation as well as internal rotation ROM. Believed that the manipulation increased the total allowable excursion of the capsule, thus improving external and internal rotation. ¡ Roubal et al and Placzek et al
� Tension in the capsular tissues rather than joint surface geometry controls the translation of the humeral head. ¡ Asymmetrical capsular tightness impacts humeral head motion,
especially when tension in the capsule increases as the arm is taken further into elevation
¡ Novotny et al
Main Point
� Assess the joint play prior to mobilization to determine direction of restriction…and then mobilize in that direction!
� An anterior glide to increase ER may not always be the most appropriate choice.
� “Treat the source not the symptoms” ¡ InMotion PT

Interesting Facts
� Subscapularis limits external rotation the most with the arm at 0° of abduction ¡ A greater loss of external rotation at 45° vs. 90° of abduction
indicates subscapularis restriction. � 2010 study suggest that C5-6 joint mobilization increases
muscle strength of the shoulder external rotators immediately ¡ Effect carries over for 10 minutes but not after 20 minutes.
� Recent case report suggest that dry needling in pt with adhesive capsulitis may allow for more intense mobilizations due to pain relief ¡ Upper trapezius, levator scapula, deltoid, and infraspinatus
muscles

Resources
� Baeyens JP, Van Roy P, De Schepper A, Declercq G, Clarijs JP. Glenohumeral joint kinematics related to minor anterior instability of the shoulder at the end of the late preparatory phase of throwing. Clinical Biomechanics 16 (2001) 752-757.
� Brandta C, Soleb G, Krausea MW, Nelc M. An evidence-based review on the validity of the Kaltenborn rule as applied to the glenohumeral joint. Manual Therapy 12 (2007) 3–11.
� Clewley D, Flynn TW, Koppenhaver S, Trigger Point Dry Needling as an Adjunct Treatment for a Patient With Adhesive Capsulitis of the Shoulder. Journal of Orthopaedic & Sports Physical Therapy 44 (2014) 92-101.
� Howell SM1, Galinat BJ, Renzi AJ, Marone PJ. Normal and abnormal mechanics of the glenohumeral joint in the horizontal plane. Journalof Bone & Joint Surgery Am. 1988 Feb;70(2):227-32.
� Johnson AJ, Godges JJ, Zimmerman GJ, Ounanian LL. The effect of anterior versus posterior glide joint mobilization on external rotation range of motion in patients with shoulder adhesive capsulitis. J Orthopaedic & Sports Physical Therapy. 2007;37:88-99.
� Novotny JE, Nichols CE, Beynnon BD. Normal kinematics of the unconstrained glenohumeral joint under coupled moment loads. J Shoulder Elbow Surg. 1998;7:629-639.
� Placzek JD, Roubal PJ, Freeman DC, Kulig K, Nasser S, Pagett BT. Long- term effectiveness of translational manipulation for adhesive capsulitis. Clin Orthop Relat Res. 1998:181-191.
� Roubal PJ, Dobritt D, Placzek JD. Glenohumeral gliding manipulation following interscalene brachial plexus block in patients with adhesive capsulitis. Journal of Orthopaedic & Sports Physical Therapy. 1996;24:66-77.
� Wang SS, Meadows J, Immediate and Carryover Changes of C5-6 Joint Mobilization on Shoulder External Rotator Muscle Strength. Journal of manipulative and physiological therapeutics. 2010 Feb;33(2):102-8.





























