-
8/2/2019 Shaken Baby Syndrome. a Case Report
1/5
-
8/2/2019 Shaken Baby Syndrome. a Case Report
2/5
uncontrolled movements of the upper and lower limbs.
Physicalexamination was unremarkable. The fontanel was normal.
Therewas no fever. Hematologic laboratory data and blood
chemicalvalues were normal. No skin lesions or occult bone
fractures werefound. Both parents denied a history of
craniocerebral trauma.Shortly after admission, the boys clinical
condition deterioratedrapidly. He developed repetitive generalized
tonic-clonic seizuresand severe respiratory depression, requiring
urgent intubation. Thechild was ventilated, and given
phenytoin.
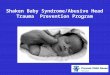
A noncontrast CT scan of the brain (Fig. 1) showed multipleareas
of decreased attenuation in both cerebral hemispheres. Therewere
thin, hypodense subdural collections over both frontal lobes.The
low-density appearance of these collections could point to
subacute or chronic subdural hematomas, or acute traumatic
hy-gromas. The diagnosis of shaken-baby syndrome was
suspected.Fundoscopic examination revealed widespread bilateral
retinalhemorrhages, but no papillary edema. Plain radiographs of
thechest, axial skeleton, and extremities showed no
abnormalities.Emergency MRI of the brain was performed on the same
day(Fig. 2) using the following pulse sequences: axial turbo
fluid-attenuated inversion recovery (FLAIR) images, axial
inversionrecovery T1-weighted images, axial echo-planar DW-MRI
scans
with b values of 0, 500, and 1,000 mm2
/s (trace images and ADCmaps), coronal HASTE T2-weighted scans,
and MR angiography(MRA) with 3D time-of-flight technique and
maximum intensityprojection reconstructions. The MRI examination
confirmedbilateral subdural hematomas, extending into the
interhemisphericfissure (Fig. 2a, b). The DW-MRI scans revealed
gyriform areas ofrestricted diffusion involving the edematous
cortical gray matter ofboth hemispheres (Fig. 2c, d). These areas
were hypointense on thecorresponding ADC maps. This indicates
cytotoxic edema, pre-sumably due to widespread cortical
hypoxic-ischemic brain dam-age. The parenchymal abnormalities were
not well seen on theFLAIR images, though it must be remembered that
FLAIR imagesin infants are relatively insensitive in comparison
with those ofolder children and adults. MRA showed normal
intracranialarteries. There was no evidence of venous sinus
occlusion.
When confronted with the imaging findings, the father
admitted
to vigorous shaking of the baby. The subdural hematomas
wereremoved neurosurgically, and a ventricular catheter was
placed.During the first postoperative day, rapid increase in
intracranialpressure was observed. Despite maximal antiedematous
and anti-convulsive treatment, including administration of
pentobarbital,the elevation of intracranial pressure persisted.
Follow-up CT scanson days 2 and 6 after admission demonstrated a
dramatic increaseof the cerebral parenchymal ischemic areas and the
appearance ofintracerebral hemorrhage (Fig. 3). Over the next few
days, thepatients clinical condition gradually improved. The boy
wasextubated on day 9 and discharged from the ICU to a
pediatricward in hemodynamically and respiratory stable condition,
butwith no evidence of higher cortical functions.
The child survived and was last seen at the age of 9
months.There was eye contact and motor development was scored
atapproximately 4 months. Clinical examination revealed
acquired
microcephaly, a convergent squint, and spastic quadriplegia.
Discussion
The diagnosis of SBS remains a formidable clinicalchallenge. The
consequences of this diagnosis are grave,
Fig. 1 Axial noncontrast CT scan obtained on the day ofadmission
from a 2-month-old baby boy with suspected shakenbaby syndrome
(SBS). Thin, hypodense extra-axial effusions areseen over both
frontal lobes. Multiple hypodense areas areobserved in the frontal,
temporal, and occipital lobes
Fig. 2 MRI examination, obtained 2 h after admission. a, b
Axialturbo FLAIR images reveal bilateral subdural
hematomas,extending into the interhemispheric fissure. c, d Axial
diffusion-weighted MR images (DW-MRI), obtained with a b value
of1,000 mm2/s, show confluent hyperintensities involving the
corticalgray matter and subcortical white matter in the frontal
andtemporal and occipital lobes. The lesions were hypointense on
theapparent diffusion-coefficient (ADC) maps, indicating areas
ofrestricted diffusion. This finding is consistent with diffuse
hypoxic-ischemic brain injury
869
-
8/2/2019 Shaken Baby Syndrome. a Case Report
3/5
both for the baby and his/her parents or caregivers.Missing the
diagnosis of SBS in an acutely ill infant canlead to permanent
neurological damage or even death[14]. On the other hand, when a
false-positive diagnosisof SBS is made, parents or caregivers may
be falselyaccused of assault.
By clinical examination one cannot differentiate withcertainty
between accidental and inflicted injury, espe-cially in the absence
of external signs of violence [12, 15].Retinal hemorrhages in an
infant are a cardinal featureof SBS. Traditionally, retinal
hemorrhages were believed
to be caused by an abrupt rise of intracranial pressure(shaking
plus strangulation or suffocation mechanism);however, recent
evidence suggests that the retinal hem-orrhages could be the result
of mechanical shaking for-ces [11]. Whatever the etiology, the
finding of retinalhemorrhages is not specific, nor does their
absence ruleout the possibility of nonaccidental trauma.
Increasingly, therefore, the diagnosis of SBS relies
onradiologic evidence of intracranial damage. CT hasrevolutionized
the assessment and management of sus-pected SBS, and remains the
principal imaging modalityin the acute setting [2, 10]. CT scans of
the brain nearlyalways demonstrate subdural hematomas, which are
the
most common manifestations of SBS. Subdural hema-tomas of
varying ages, or located in the interhemisphericfissure are
considered to be highly suggestive of shakinginjury [1]. It is
believed that the acceleration/decelerationforces which occur
during violent shaking are sufficientto cause rupture of the
vulnerable bridging veins, which,in young babies, can easily be
torn [2]. Infants tend tohave relatively large volumes of
cerebrospinal fluidaround the brain, which allows for greater
movementwithin the cranial vault [11]. Moreover, the neck
muscles
of babies are not strong enough to support the range ofmotion of
their relatively large heads. The presence ofsubdural hemorrhages
can also be explained by a com-bination of severe hypoxia, brain
swelling, and raisedcentral venous pressure, which causes blood to
leak fromintracranial veins into the subdural space [16]. It must
beremembered, however, that not all subdural hematomas
are due to child abuse.MRI has increased the sensitivity for
diagnosing SBS
in detecting and characterizing small extra-axial hem-orrhages
in infants with equivocal CT findings [2, 10].On CT, subdural
collections are often of a nonspecificcharacter (e.g., subacute or
chronic sudural hematomasthat are of low density or isodense), as
shown in ourpatient. MRI has a 50% greater rate of detection
ofsubdural hematomas than CT [17]. Moreover, MRI ismore accurate in
dating subdural hematomas and allowsdifferentiation of a recent
subdural hemorrhage fromone superimposed on a pre-existing one
[18]. Even moreimportantly, MRI reveals the presence of
nonhemor-
rhagic parenchymal brain damage not shown or under-estimated on
the acutely performed cerebral CT scan,such as diffuse axonal
trauma or hypoxic-ischemicencephalopathy [2, 3, 15, 19]. DW-MRI is
a techniquethat is sensitive to restricted diffusion, reflecting
cyto-toxic edema, which occurs in acute hypoxic-ischemicbrain
damage. In our patient, we found widespread,gyriform regions of
decreased diffusion in the corticalgray matter. This pattern
suggests that the neurophys-iopathology of the severe
encephalopathy in SBS ishypoxic-ischemic brain damage, and NOT
diffuse trau-matic axonal injury. Neuropathological studies
byGeddes et al. have confirmed that global severe hypoxic
damage is by far the most common histological findingin
inflicted head injury in children, and that widespreadaxonal damage
is much less frequent [20, 21]. The dif-fusion abnormalities
observed in our patient were pre-dominantly found in cortical gray
matter, whichappeared thickened and edematous. Other
investigatorshave shown diffusion abnormalities in the
subcorticalbrain tissue, consistent with watershed
infarctions,especially in the posterior brain regions [15].
Magneticresonance spectroscopy findings confirm that the
path-ophysiology of nonaccidental head trauma is due
tohypoxic-ischemic injury, by showing the metabolicchanges
occurring in the infant brain after a shakinginjury [22]. Hypoxic
injury to the brain results in loss ofN-acetyl aspartate and
accumulation of lactate, al-though the mechanism in SBS appears to
be somewhatdifferent from hypoxic injury alone [22].
In summary, in our patient with SBS, DW-MRIshowed a dramatically
greater lesion extent than wasseen on conventional MR images or on
CT scans. DW-MRI may represent the most sensitive and
specifictechnique in the evaluation of cerebral damage in
shakenbabies. The use of DW-MRI may help to guide clinical
Fig. 3 Follow-up noncontrast CT scan (day 6 after
admission)shows a dramatic increase of the cerebral parenchymal
abnormal-ities, which are seen as hypodense regions (suggestive of
edema)and hyperdense areas (indicating intraparenchymal
hemorrhage).The density in the left frontal horn is a shunt
catheter. There is asmall amount of blood in the occipital horn on
the right
870
-
8/2/2019 Shaken Baby Syndrome. a Case Report
4/5
management of these patients, to identify children athigh risk
for poor outcome, and to provide an estimateregarding the timing of
the alleged assault. Thus, thetime-dependent signal intensity
changes on DW-MRImay be of great importance in forensic medicine.
Theareas of restricted diffusion indicate cytotoxic edemaand
confirm the neuropathological observations that the
parenchymal brain damage in SBS is predominantly dueto diffuse
hypoxic-ischemic encephalopathy, and not todiffuse axonal injury
[21].
Acknowledgements We are grateful to V. De Groot, MD,
forproviding fundoscopic evidence of retinal hemorrhages. We
alsothank G. Van Hoorde for photographic assistance.
References
1. Kleinman PK (1998) Diagnostic imag-ing of child abuse.
Mosby-Year Book,St. Louis
2. Committee on Child Abuse and Neglect(2001) Shaken baby
syndrome: rota-tional cranial injuriestechnical report.Pediatrics
108:206210
3. Blumenthal I (2002) Shaken baby syn-drome. Postgrad Med J
78:732735
4. King WJ, MacKay M, Sirnick A, withthe Canadian Shaken Baby
Group
(2003) Shaken baby syndrome in Can-ada: clinical characteristics
and out-comes of hospital cases. CMAJ168:155159
5. Barlow KM, Minns RA (2000) Annualincidence of shaken impact
syndrome inyoung children (research letter). Lancet356:15711572
6. Bruce DA, Zimmerman RA (1989)Shaken impact syndrome. Pediatr
Ann18:482494
7. Mehl AL (1990) Shaken impact syn-drome (letter). Child Abuse
Negl14:603604
8. David TJ (1999) Shaken baby (shakenimpact) syndrome:
non-accidental head
injury in infancy. J R Soc Med 92:556561
9. Cho DY, Wang YC, Chi CS (1995)Decompressive craniotomy for
acuteshaken/impact baby syndrome. PediatrNeurosurg 23:192198
10. Duhaime AC, Christian CW, RorkeLB, et al (1998)
Nonaccidental headinjury in infantsthe shaken-babysyndrome. N Engl
J Med 338:18221829
11. Morad Y, Kim YM, Armstrong DC,et al (2002) Correlation
between retinal
abnormalities and intracranial abnor-malities in the shaken baby
syndrome.Am J Ophtalmol 134:354359
12. Editorial. Shaken babies (1998) Lancet352:335
13. Kleinman PK (1998) Shaken babies(correspondence). Lancet
352:815
14. Jenny C, Hymel KP, Ritzen A, et al(1999) Analysis of missed
cases of abu-sive head trauma. JAMA 281:621626
15. Biousse V, Suh DY, Newman NJ, et al(2002) Diffusion-weighted
magneticresonance imaging in shaken baby syn-drome. Am J Ophtalmol
133:249255
16. Geddes JF, Tasker RC, Hackshaw AK,et al (2003) Dural
haemorrhage in
non-traumatic infant deaths: does itexplain the bleeding in
shaken babysyndrome? Neuropathol Appl Neuro-biol 29:1422
17. Sato Y, Yuh WT, Smith WL, et al(1989) Head injury in child
abuse:evaluation with MR imaging. Radiol-ogy 173:653657
18. Lee Y, Lee KS, Hwang DH, et al (2001)MR imaging of shaken
baby syndromemanifested as chronic subdural hema-toma. Korean J
Radiol 2:171174
19. Suh DY, Davis PC, Hopkins KL, et al(2001) Nonaccidental
pediatric headinjury: diffusion-weighted imaging find-
ings. Neurosurgery 49:30932020. Geddes JF, Hackshaw AK, Vowles
GH,
et al (2001) Neuropathology of inflictedhead injury in children.
I. Patterns ofbrain damage. Brain 124:12901298
21. Geddes JF, Vowles GH, Hackshaw AK,et al (2001)
Neuropathology of inflictedhead injury in children. II.
Microscopicbrain injury in infants. Brain 124:12991306
22. Haseler LJ, Phil M, Arcinue E, et al(1997) Evidence from
proton magneticresonance spectroscopy for a metaboliccascade of
neuronal damage in shakenbaby syndrome. Pediatrics 99:414
871
-
8/2/2019 Shaken Baby Syndrome. a Case Report
5/5
Reproducedwithpermissionof thecopyrightowner. Further
reproductionprohibitedwithoutpermission.