Embed Size (px)
Citation preview

Seroprevalence of Hepatitis B, Hepatitis C, and Human ImmunodeficiencyVirus Infections in Children With Cancer at Diagnosis and Following Therapy
in Turkey
Rejin Kebudi, MD,1* Inci Ayan, MD,1 Gulden Yílmaz, MD,2 Ferhan Akící, MD,1
Omer Gorgun, MD,1 and Selim Badur, MD2
Background. Children with cancer receiv-ing intensive chemotherapy require multipletransfusions and are at increased risk for bloodtransmittable diseases such as hepatitis B virus(HBV), hepatitis C virus (HCV), and human im-munodeficiency virus (HIV) infections. Proce-dure. Sera from 50 children (24 female, 26male) admitted between January, 1994, andDecember, 1995, with solid tumors receivingintensive chemotherapy and multiple transfu-sions were investigated for HBsAg , anti-HBs,anti-HBc, anti-HCV, and anti-HIV by ELISA atdiagnosis and at the end of therapy. Results.HBsAg, HBV, HCV, and HIV seropositivitieswere 0%, 4%, 2% and 0% at diagnosis and
10%, 20%, 14% and 0% at the end of therapy,respectively. Conclusions. The high seropreva-lence of HCV may be due to the lack of anti-HCV screening of blood products in the bloodbanks during the study period. Although theHBV seroprevalance of 20% found in this studyis much lower than the value of 56% found ina previous study conducted during 1986–1989in a similar patient population and a similarsetting, it is still high. Children infected withHBV during immunosuppressive therapy are atgreater risk of becoming chronic carriers andprecautions must be taken for immunization ofthese children. Med. Pediatr. Oncol. 34:102–105, 2000. © 2000 Wiley-Liss, Inc.
Key words: HBV; HCV; HIV; transfusions; pediatric oncology; cancer
INTRODUCTION
Survival of children with cancer has increased dra-matically in parallel with the advances in therapy proto-cols including intensive chemotherapy. These childrenrequire multiple transfusions during intensive therapyand are at increased risk for blood-transmittable infec-tions such as hepatitis B virus (HBV), hepatitis C virus(HCV), and human immunodeficiency virus (HIV) in-fection [1–9]. The risks of these infections vary amongcountries depending on the frequency of the infections inthe donor population and screening technology for bloodand blood products used in different countries [9]. Theaim of this study is to investigate the seroprevalence ofHBV, HCV, and HIV infections in fifty multiply trans-fused children with solid tumors at diagnosis and follow-ing therapy and to compare the results to those obtainedin previous years in Turkey.
MATERIALS AND METHODS
One hundred fourty-eight children were admitted tothe Division of Pediatric Oncology, Institute of Oncol-ogy, University of Istanbul, with malignant solid tumorsbetween January, 1994, and December, 1995. One hun-dred four (70%) had received multiple transfusions dur-ing treatment. Among 90 who had completed treatment
and had received multiple transfusions during treatment,50 children (24 female, 26 male) with a median age of 8years (1–16 years) were selected randomly and enrolledin this study. The diagnoses were as follows: 11 rhabdo-myosarcomas, 9 Ewing sarcomas, 6 Hodgkin disease, 6non-Hodgkin lymphomas, 4 Wilms tumors, 3 osteosar-comas, 3 brain tumors, 3 germ cell tumors, 2 retinoblas-tomas, 1 neuroblastoma, 1 nasopharynx carcinoma, and 1pulmonary blastoma. None of the patients had been vac-cinated previously for hepatitis B, nor had they receivedany kind of immunoglobulin products. The median unitsof blood products received per patient in the transfusiongroup was 10 (5–85) units.
Blood samples of 50 children with solid tumors werecollected at diagnosis and at least 3 months (3–6 months)after cessation of therapy, with consent of the family.
1Division of Pediatric Oncology, Institute of Oncology, University ofIstanbul, Istanbul, Turkey2Division of Virology, Department of Microbiology, Istanbul Schoolof Medicine, University of Istanbul, Istanbul, Turkey
Grant sponsor: University of Istanbul Research Fund; Grant number:O180/100196.
*Correspondence to: Rejin Kebudi, MD, University of Istanbul On-cology Institute, C¸ apa, Istanbul 34390, Turkey.
Received 22 December 1998; Accepted 26 August 1999
Medical and Pediatric Oncology 34:102–105 (2000)
© 2000 Wiley-Liss, Inc.
Patient sera were tested for HBsAg, anti-HBs, anti-HBcIgG, anti-HCV and anti-HIV by enzyme-linked im-munosorbent assay [10].
The Mann Whitney U test was used to assess thecorrelation of HBV or HCV seropositivity and the num-ber of transfusions. The McNemar test was used to evalu-ate the statistical difference of seropositivity for HBVand HCV at diagnosis and at the end of treatment. Allblood and blood products have been routinely tested forHBsAg since 1975, for anti-HIV since 1987, and foranti-HCV since September, 1995, in the blood bank sup-plying these products to the patients in this study.
RESULTS
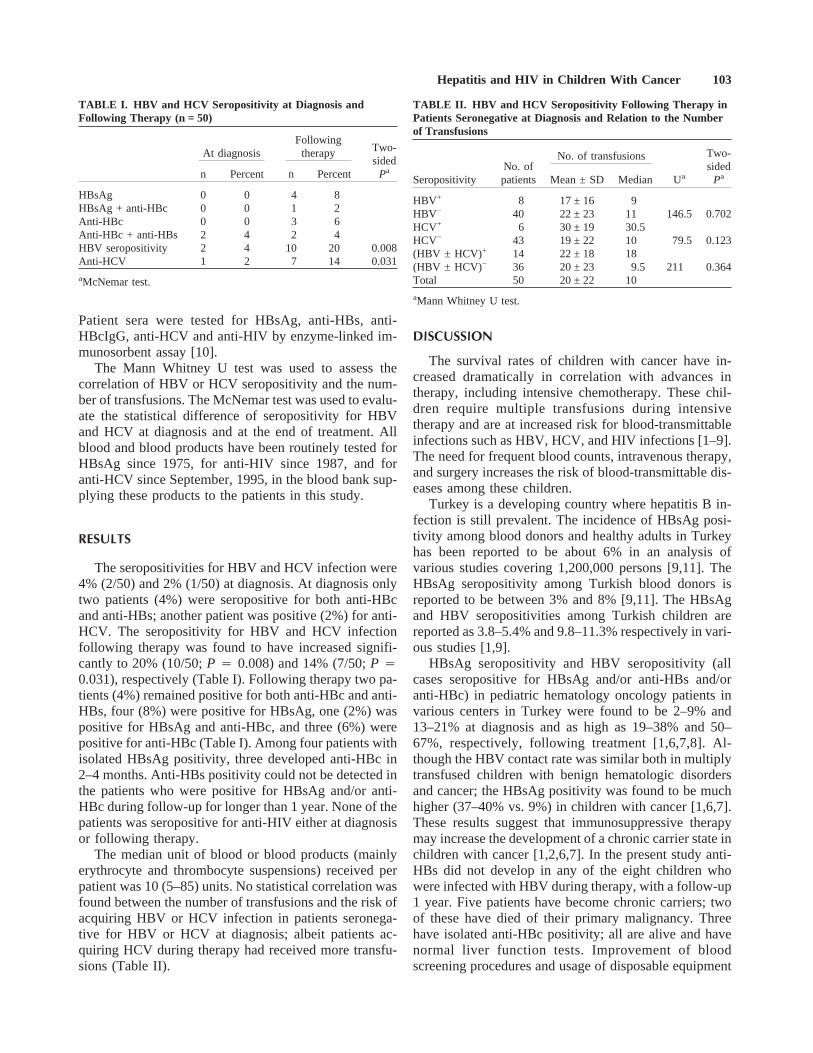
The seropositivities for HBV and HCV infection were4% (2/50) and 2% (1/50) at diagnosis. At diagnosis onlytwo patients (4%) were seropositive for both anti-HBcand anti-HBs; another patient was positive (2%) for anti-HCV. The seropositivity for HBV and HCV infectionfollowing therapy was found to have increased signifi-cantly to 20% (10/50;P 4 0.008) and 14% (7/50;P 40.031), respectively (Table I). Following therapy two pa-tients (4%) remained positive for both anti-HBc and anti-HBs, four (8%) were positive for HBsAg, one (2%) waspositive for HBsAg and anti-HBc, and three (6%) werepositive for anti-HBc (Table I). Among four patients withisolated HBsAg positivity, three developed anti-HBc in2–4 months. Anti-HBs positivity could not be detected inthe patients who were positive for HBsAg and/or anti-HBc during follow-up for longer than 1 year. None of thepatients was seropositive for anti-HIV either at diagnosisor following therapy.
The median unit of blood or blood products (mainlyerythrocyte and thrombocyte suspensions) received perpatient was 10 (5–85) units. No statistical correlation wasfound between the number of transfusions and the risk ofacquiring HBV or HCV infection in patients seronega-tive for HBV or HCV at diagnosis; albeit patients ac-quiring HCV during therapy had received more transfu-sions (Table II).
DISCUSSION
The survival rates of children with cancer have in-creased dramatically in correlation with advances intherapy, including intensive chemotherapy. These chil-dren require multiple transfusions during intensivetherapy and are at increased risk for blood-transmittableinfections such as HBV, HCV, and HIV infections [1–9].The need for frequent blood counts, intravenous therapy,and surgery increases the risk of blood-transmittable dis-eases among these children.
Turkey is a developing country where hepatitis B in-fection is still prevalent. The incidence of HBsAg posi-tivity among blood donors and healthy adults in Turkeyhas been reported to be about 6% in an analysis ofvarious studies covering 1,200,000 persons [9,11]. TheHBsAg seropositivity among Turkish blood donors isreported to be between 3% and 8% [9,11]. The HBsAgand HBV seropositivities among Turkish children arereported as 3.8–5.4% and 9.8–11.3% respectively in vari-ous studies [1,9].
HBsAg seropositivity and HBV seropositivity (allcases seropositive for HBsAg and/or anti-HBs and/oranti-HBc) in pediatric hematology oncology patients invarious centers in Turkey were found to be 2–9% and13–21% at diagnosis and as high as 19–38% and 50–67%, respectively, following treatment [1,6,7,8]. Al-though the HBV contact rate was similar both in multiplytransfused children with benign hematologic disordersand cancer; the HBsAg positivity was found to be muchhigher (37–40% vs. 9%) in children with cancer [1,6,7].These results suggest that immunosuppressive therapymay increase the development of a chronic carrier state inchildren with cancer [1,2,6,7]. In the present study anti-HBs did not develop in any of the eight children whowere infected with HBV during therapy, with a follow-up1 year. Five patients have become chronic carriers; twoof these have died of their primary malignancy. Threehave isolated anti-HBc positivity; all are alive and havenormal liver function tests. Improvement of bloodscreening procedures and usage of disposable equipment
TABLE I. HBV and HCV Seropositivity at Diagnosis andFollowing Therapy (n = 50)
At diagnosisFollowing
therapy Two-sided
Pan Percent n Percent
HBsAg 0 0 4 8HBsAg + anti-HBc 0 0 1 2Anti-HBc 0 0 3 6Anti-HBc + anti-HBs 2 4 2 4HBV seropositivity 2 4 10 20 0.008Anti-HCV 1 2 7 14 0.031
aMcNemar test.
TABLE II. HBV and HCV Seropositivity Following Therapy inPatients Seronegative at Diagnosis and Relation to the Numberof Transfusions
SeropositivityNo. ofpatients
No. of transfusions
Ua
Two-sided
PaMean ± SD Median
HBV+ 8 17 ± 16 9HBV− 40 22 ± 23 11 146.5 0.702HCV+ 6 30 ± 19 30.5HCV− 43 19 ± 22 10 79.5 0.123(HBV ± HCV)+ 14 22 ± 18 18(HBV ± HCV)− 36 20 ± 23 9.5 211 0.364Total 50 20 ± 22 10
aMann Whitney U test.
Hepatitis and HIV in Children With Cancer 103

for invasive diagnostic procedures has decreased the in-cidence of HBV infections in children with cancer inTurkey in recent years [1,9].
In a previous study conducted on 50 multiply trans-fused children with cancer during 1986–1989 in a similarpatient population and in a similar setting, the HBsAgpositivity and HBV seropositivity were found to be 40%and 56%, respectively [1]. All blood and blood productshave been routinely tested for HBsAg since 1975 in thelocal blood bank supplying these products to the patientsin the previous and the present studies. In the previousstudy, the seropositivity for HBV infection found in pa-tients transfused prior to 1986 when the counterimmuneelectrophoresis (CIE) method was used for screening ofblood and blood products (70.9%) was significantlyhigher (P < 0.001) than the value found for patients trans-fused after 1986 when the indirect hemagglutination(IHA) method began to be used (42.6%) [1]. In the pres-ent study, patients received blood and blood productsscreened by the ELISA method for HBsAg, as well as foranti-HCV and anti-HIV. The HBsAg positivity and HBVpositivity of 10% and 20%, respectively, at the end oftreatment are much lower than the rates of 40% and 56%obtained in oncology patients treated between 1986 and1989. These results suggest that the use of more sensitiveand specific screening methods for HBsAg is importantin reducing the risk of transmission of HBsAg by trans-fusions. Although the HBsAg positivity and HBV con-tact rate in this study are much lower than in the previousstudy, they are still quite high. HBV infections duringtherapy delay therapy in these children, and immunosu-pressed children are at increased risk for becoming car-riers and developing chronic hepatitis. Therefore, precau-tions for preventing HBV infection in these childrenshould be taken.
Children with cancer who are seronegative for HBVand who are to receive intensive therapy and thus requiremultiple transfusions should be considered at high riskfor HBV, especially if living in intermediate- and high-endemicity areas of the world. HBV vaccination of theseseronegative patients at diagnosis may be recommended[1]. The seroconversion rate following three doubledoses of vaccine administered at monthly intervals wasreported to be 19–41% in children with solid tumors[12,13]. We have also obtained a seroconversion rate of40% in 25 children with solid tumors (unpublished re-sults). In several studies, the best seroconversion rateswere obtained in patients who do not receive intensivechemotherapy [12,13]. As antineoplastic therapy inten-sity increases, the antibody response to chemotherapydecreases. In patients receiving such intensive treatment,the use of hepatitis B immunglobulin with or withouthepatitis B vaccine may be considered [14,15].
The initiation of free routine immunization of all in-fants in Turkey seems to be a better solution of this
problem. Patients with protective levels of anti-HBsseem to maintain those levels during therapy.
Hepatitis C virus (HCV) is now the most commonlyencountered blood-transmittable hepatitis infectionamong cancer patients. The previously reported risk ofacquiring HCV infection of 25% in multiply transfusedadults in the United States has dropped to 0.1% afterroutine screening for anti-HCV in blood and blood prod-ucts and elimination of high-risk donors [16]. The sero-prevalence of HCV in Turkish blood donors is reportedto be 0.3–1.8% [9]. The seroprevalence of HCV inhealthy children in the United States is reported as 0.2–0.4%; this value was found to be 0% in healthy Turkishchildren. The HCV seroprevalences in children withthalasemia and with cancer were found to be 14% and4.5% respectively in one study in Turkey [7]. In ourstudy this value was 2% at diagnosis and 14% followingtherapy. Most of these patients received transfusionsprior to September, 1995, before initiation of routinescreening for HCV. We expect that this rate will drop inpatients transfused with blood and blood productsscreened for HCV. Among the seven children with anti-HCV seropositivity, three are long-term survivors; fourhave died, three of primary disease and one with secondmalignancy.
The incidence of HIV infection among childrenthroughout the world has increased dramatically, consti-tuting 5–30% of all cases of autoimmune deficiency syn-drome (AIDS) [5]. The risk of HIV infection in multi-transfused patients is well known. In a previous studyconducted by us in Istanbul, seropositivity for anti-HIVwas found to be 0% in 50 children with cancer and 0.9%in 109 children with benign hematologic disorders [1].HIV contact was not found in any of the children in thisstudy. This may be due to the low seroprevalance of HIVin Turkey compared to European countries or the UnitedStates and also to the fact that all patients received trans-fusions screened for anti-HIV. The use of detailed ques-tionnaires in blood banks to eliminate high-risk donorseven if they are seronegative is an important precautionfor decreasing the risk of HBV, HCV, and HIV infectionsin multiply transfused children.
ACKNOWLEDGMENTS
We thank Prof. Dr. Rian Dis¸ci, from the Division ofCancer Epidemiology and Biostatistics, Institute of On-cology, University of Istanbul, for assistance in statisticalevaluation and Leyla Yalc¸ínkaya, MS, from the Divisionof Basic Oncology, Institute of Oncology, University ofIstanbul, and Emine O¨ zkan, MS, from the Department ofMicrobiology, University of Istanbul, for their technicalhelp.
104 Kebudi et al.

REFERENCES
1. Kebudi R, Agaoglu L, Badur S. The seroprevalance of HIV-1 andHBV infections in multitransfused pediatric hematology-oncologypatients in Istanbul. Pediatr Hematol Oncol 1992;9:389–391.
2. Hoofnagle JH, Dusheiko GM, Schafer DF, et al. Reactivation ofchronic hepatitis B virus infection by cancer chemotherapy. AnnIntern Med 1982;96:447–449.
3. Myers B, Irving W, Hollingsworth R, et al. Hepatitis C in multi-transfused children with hematological malignancy. Br J Haema-tol 1995;91:480–482.
4. Neilson JR, Harrison P, Skidmore SJ, et al. Chronic hepatitis C inlong term survivors of haematological malignancy treated in asingle centre. J Clin Pathol 1996;49:230–232.
5. Fisher M. Transfusion associated acquired immunodeficiencysyndrome—what’s the risk? Pediatrics 1987;79:156–160.
6. Akyol H, Sarialioglu F, Bu¨yukpamukcu M, et al. Hepatitis B virusinfections in pediatric patients receiving anti-cancer chemo-therapy. Turk J Cancer 1990;20:104–108.
7. Cetingul N, Kavakli K, Vergin C, et al. Hepatitis-B, hepatitis-C,CMV and HIV markers in pediatric malignancies. Turk J Cancer1994;24:175–180.
8. Berberoglu S. The seroprevalance of hepatitis B, hepatitis C andhuman immundeficiency virus infections in pediatric oncologypatients in Turkey. Postgrad Med J 1996;72:609–611.
9. Badur S. Viral hepatitis in Turkey. Status report of the Turkish
Society for Prevention of Viral Hepatitis (in Turkish). In: Kilic¸-turgay K, editor. Viral hepatitis 94. Istanbul: Nobel Tip Publisher;1994. p 15–38.
10. Yelken RH. Solid phase enzyme immunoassays for the detectionof microbial antigens in body fluids. In: Lenette EH, Balows A,Hausler WJ, Shadomy HJ, editors. Manual of clinical microbiol-ogy, 4th ed. Washington, DC: American Society for Microbiol-ogy; 1985. p 949–957.
11. Ariogul S, Akalin E, Kanra T. HBsAg among Turkish blood do-nors. Infection 1987;15:456.
12. Berberoglu S, Bu¨yukpamukcu M, Sarialioglu F, et al. Hepatitis Bvaccination in children with cancer. Pediatr Hematol Oncol 1995;12:171–178.
13. Entacher U, Ju¨rgenssen O, Simbruner G, et al. Hepatitis B vacci-nation and immune response in children with malignant disease.Eur J Pediatr 1985;144:160–163.
14. Hoofnagle JH; Seeff LB, Bales ZB, et al. Passive-active immunityfrom hepatitis B immunoglobulin. Ann Intern Med 1979;91:813–818.
15. Boguslawska Jaworska J, Gorczynska E, Seyried H, et al. Passiveand active antihepatitis B immunization of children with hemato-logical malignancies. Hematol Blood Transfus 1987;30:530–534.
16. American Academy of Pediatrics. Hepatitis C. In: Peter G, editor.1997 Red book. Report of the Committee on Infectious Diseases,24th ed. Elk Grove Village, IL: American Academy of Pediatrics;1997. p 260–264.
Hepatitis and HIV in Children With Cancer 105





























