Embed Size (px)
Citation preview

Selection and Insertion of VascularAccess Devices in Pediatrics:A Systematic ReviewRebecca S. Paterson, PhD,a,b Vineet Chopra, MD, MSc,c,d,g Erin Brown, PhD,a,b Tricia M. Kleidon, RN, MNursPrac,a,e
Marie Cooke, RN, PhD,a,f Claire M. Rickard, RN, PhD,a,f Steven J. Bernstein, MD, MPH,c,g Amanda J. Ullman, RN, PhDa,e,f
abstractOBJECTIVE: To critically review the evidence for the selection and insertion of pediatric vascularaccess devices (VADs).
DATA SOURCES: Data were sourced from the US National Library of Medicine, Cumulative Index toNursing and Allied Health, the Cochrane Library databases, Embase, and international clinicaltrial databases.
STUDY SELECTION: Clinical practice guidelines, systematic reviews, cohort designs, randomizedcontrol trials (RCTs), quasi RCTs, before-after trials, or case-control studies that reported oncomplications and/or risk as well as reliability of VADs in patients aged 0 to 18 years wereincluded.
DATA EXTRACTION: Articles were independently reviewed to extract and summarize details on thenumber of patients and catheters, population, age of participants, VAD type, study method,indication, comparators, and the frequency of VAD failure or complications.
RESULTS: VAD selection and insertion decision-making in general hospitalized and somespecialized patient populations were well evidenced. The use of single-lumen devices andultrasound-guided techniques was also broadly supported. There was a lack of RCTs, and forneonates, cardiac patients, patients with difficult venous access, midline catheters, catheter-to-vein ratio, and near-infrared devices, the lack of evidence necessitated broadening thereview scope.
LIMITATIONS: Limitations include the lack of formal assessment of the quality of evidence and thelack of RCTs and systematic reviews. Consequently, clinical decision-making in certainpediatric populations is not guided by strong, evidence-based recommendations.
CONCLUSIONS: This is the first synthesis of available evidence for the selection and insertion ofVADs in pediatric patients and is important for determining the appropriateness of VADs inpediatric patients.
WHAT’S KNOWN ON THIS SUBJECT: Individual studies, systematic reviews, andfocused clinical practice guidelines that evaluate vascular access devices (VADs)in various pediatric populations are available. However, to date, no systematicreview examining the appropriateness, and inappropriateness, of VADs acrosscommon pediatric clinical scenarios exists.
WHAT THIS STUDY ADDS: There is strong evidence to support and facilitateappropriate clinical decision-making in some pediatric indications. However,certain populations, device types and characteristics, and insertion proceduresare poorly evidenced, necessitating the application of clinical judgment for VADdecision-making.
To cite: Paterson RS, Chopra V, Brown E, et al. Selectionand Insertion of Vascular Access Devices in Pediatrics:A Systematic Review. Pediatrics. 2020;145(s3):e20193474H
aAlliance for Vascular Access Teaching and Research, Menzies Health Institute Queensland and fSchool of Nursingand Midwifery, Griffith University, Nathan, Queensland, Australia; bChild Health Research Centre, Faculty ofMedicine, The University of Queensland, Brisbane, Queensland, Australia; cPatient Safety Enhancement Programand Center for Clinical Management Research, Veterans Affair Ann Arbor Healthcare System, Ann Arbor,Michigan; dDivisions of Hospital Medicine and gGeneral Medicine, Department of Internal Medicine, MedicalSchool, University of Michigan, Ann Arbor, Michigan; and eQueensland Children’s Hospital, Brisbane, Queensland,Australia
PEDIATRICS Volume 145, number s3, June 2020:e20193474H SUPPLEMENT ARTICLE by guest on December 8, 2020www.aappublications.org/newsDownloaded from

Vascular access devices (VADs) area common and essential componentof pediatric health care.1 A range ofperipheral and central venousdevices that provide a route toadminister critical and supportivetherapies such as antibiotics,nutrition, and chemotherapy exists.Poor choice of VAD can lead to theinsertion of an inappropriatedevice, which reduces treatmentefficiency and places the patient atincreased risk of harm.2–5 Cliniciansneed to make device and insertiondecisions that ensure optimumtherapy provision while preventingor reducing VAD-relatedcomplications (such as infection,thrombosis, and vessel damage),patient distress, and treatmentdelays.6
To make VAD choices that mitigatepatient harm and optimize treatmentprovision, clinical decision-makingneeds to reflect current, evidence-based guidance for pediatricpatients. Individual studies,systematic reviews, and focusedclinical practice guidelines (CPGs),which evaluate VADs in variouspediatric populations, areavailable. However, to date, nosystematic review examiningthe appropriateness andinappropriateness of VADs acrosscommon pediatric clinical scenariosexists. Systematic identification ofhigh-quality evidence is necessary,not just to inform clinical decision-making and improve patientoutcomes, but to further identify gapsin evidence that translate to gaps inpractice and increase the risk ofpatient harm. In this review, weaimed to systematically andpragmatically evaluate all availableevidence and guidance for VADs toinform the determination of MichiganAppropriateness Guide forIntravenous Catheters inPediatrics7,8 using the RANDCorporation–University of California,Los Angeles (RAND-UCLA)Appropriateness Method.9
METHODS
A systematic review was undertakento synthesize existing evidence onselection and insertion of pediatricVADs following the RAND-UCLAAppropriateness Method.9 Thesystematic review protocol wasregistered and published with theInternational Prospective Register ofSystematic Reviews (PROSPERO;CRD201994286)10 and is reported inaccordance with the PreferredReporting Items for SystematicReviews and Meta-Analyses(PRISMA) standards.11
Search Strategy
We conducted searches of theUS National Library of Medicine(Medline), Cumulative Index toNursing and Allied Health, CochraneLibrary databases, Embase, andinternational clinical trial databasesfor all studies in which authorsreported VAD use (success andcomplications) in a pediatricpopulation from 2008 to May 16,2018. Search terms were developedin collaboration with an experiencedmedical librarian. We used explodedMedical Subject Headings (MeSH)terms (eg, catheters) and relevantkeywords and their variants (eg,child, pediatrics). Table 1 reveals theelectronic database search strategy.
Eligibility Criteria
Following the RAND-UCLAAppropriateness Method, our goal wasto provide a critical review of theliterature summarizing the scientificevidence available surroundingthe appropriateness of pediatricVAD selection, insertion, andcharacteristics.9 This meant a range ofstudy designs was eligible forinclusion, including existing CPGs,systematic reviews, randomizedcontrol trials (RCTs), quasi RCTs,before-after trials, cohorts, or case-control studies. Additionally, theguidelines and studies must have beenpublished in a peer-reviewed journaland authors must have reported on
complications and/or risk andreliability of VADs in patients agedterm to 18 years in a pediatric hospital.We defined VADs to includeintraosseous devices; midlinecatheters; peripherally inserted centralcatheters (PICCs); short and longperipheral intravenous catheters(PIVCs); tunneled, tunneled-cuffed, andnontunneled central venous accessdevices (CVADs); totally implantablevenous devices; and umbilicalcatheters. We excluded studies thatwere not published in English andconference abstracts, animal studies,NICU studies, n = 1 studies, casereports, case-series reports, andqualitative reports. Although eligibilitycriteria were focused on pediatricstudies (ie, term to 18 years), wedetermined that including pretermneonate and adult studies waspreferential to no evidence.
Outcome Measures
The primary outcomes were defineda priori as (1) device and insertioncharacteristics that impact thesuccess of VAD insertion and (2)device and insertion characteristicsassociated with VAD failure, due tocomplications before the completionof therapy, or successful VADinsertion. Device characteristicsincluded VAD type, device catheter-to-vein ratio, and device lumens.Insertion characteristics includedinsertion site and location and the useof vessel visualization technology.Complications included but were notlimited to central line–associatedbloodstream infection (CLABSI), VAD-associated thrombosis, occlusion,catheter dislodgement, catheter-tipmigration, catheter breakage orrupture, local infection, and phlebitis.
Screening
Title and abstract screening wasperformed independently by 2 reviewauthors (E.B. and A.J.U.), excludingstudies that did not meet eligibilitycriteria when this could bedetermined by the abstract alone.Full-text articles included for
S244 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

screening were reviewed by 2 reviewauthors (E.B. and A.J.U.) andindependently assessed against theinclusion or exclusion criteria.Duplicate publications were excluded.When individual studies that hadbeen evaluated in a systematic reviewalso returned in the search, theprimary study was excluded to avoidrepetition, and the systematic reviewwas referred to. Any discrepanciesbetween review authors wereresolved through mutual discussionand, when required, a third,independent review author (M.C.)was consulted.
Data Extraction and Synthesis
All full-text articles that met inclusioncriteria were independently reviewedby 3 review authors (R.S.P., E.B., andA.J.U.) to extract details on thenumber of patients and catheters,population, age of participants, VADtype, study method, indication,comparators, and the frequency ofVAD failure or complications. Thesedetails were summarized in a dataextraction sheet and were cross-checked for accuracy and agreement.Additional relevant references wereidentified by examining referencelists of included studies andguidelines. Hand-searched referenceswere evaluated to ensure that theymet inclusion criteria. Afterscreening, pragmatic inclusion of
wider studies was employed. That is,if no studies identified meetingthe preferential inclusion orexclusion criteria, we included widerstudies (eg, a priori area of deficitincluded neonates outside of theNICU). The extracted data werethen combined by using narrative(descriptive) synthesis by categories(ie, outcome, vascular device,indication).
Study Quality and Risk of Bias
The methodologic quality,transparency, and relevance of allindividual included studies wereindependently assessed by 2 reviewauthors (E.B. and A.J.U.) by usingthe Strengthening the Reportingof Observational Studies inEpidemiology (STROBE) guideline12
and Critical Appraisal Skills Program(CASP) Cohort Study checklist.13
RCTs and systematic reviews werepreferentially included as the goldstandard level of evidence forevaluating VADs. However, whenthis level of evidence did not exist,a pragmatic approach was taken sothat studies outside of the scope ofthe review (eg, laboratory, prematureneonate, or adult studies) and CPGs(which may be limited by the numberor quality of included studies) wereincorporated into the review. Toprovide a synthesis of the availableliterature for the purpose of the
RAND-UCLA AppropriatenessMethod,9 studies were categorizedaccording to their methodology: (1)CPG, (2) systematic review or otherreview, (3) RCT, (4) observationalstudy with comparator, and (5) other(clinical review, pilot study,laboratory study).
RESULTS
Study Selection
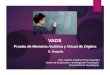
The results of the search strategy andstudy selection are summarized inFig 1. Electronic database searchesidentified 7430 articles, and handsearches of the bibliography ofincluded studies and clinicalguidelines identified 30 additionalarticles for potential inclusion.After removal of duplicates andscreening for eligibility, a total of133 studies and CPGs met eligibilitycriteria and were included in dataextraction.
Study Characteristics
The review includes 27 CPGs(20.4%), 11 systematic reviews(8.3%), 10 RCTs (7.6%), 79observational studies (59.8%), 3 pilotstudies (2.3%), 2 clinical reviews(1.5%), and 1 laboratory study(0.8%). These were sourced fromresearch teams based in Africa(1.6%), Asia (9.3%), Europe (31.0%),
TABLE 1 Summary of Search Terms Used for the Electronic Database Search
BooleanVariable
Search Terms
AND Title and abstract terms: pediatric* OR pediatric* OR child* OR youth* OR adolescen* OR neonate* OR toddler* OR baby OR babiesOR MeSH terms: Child OR Adolescent OR Infant OR “Infant, Newborn”
AND Title and abstract terms: vascular access device* OR central venous catheter* OR midline* OR Central venous access device* OR PICC* ORperipherally inserted central catheter* OR peripheral cannula* OR peripheral catheter* OR peripherally inserted OR intravenous access
OR MeSH terms: Vascular Access Devices OR Central Venous Catheters OR Infusions, Intraosseous OR Infusions, Intravenous OR Infusions,Subcutaneous
AND Title and abstract terms: vessel health OR adverse OR complicat* OR appropriat* OR inappropriat* OR indicat* OR guideline* OR unnecessaryOR publication type: guideline OR practice guidelineOR MeSH terms: Guidelines as Topic OR Unnecessary Procedures
NOT Title and abstract terms: abortion OR blood donor* OR caesar* OR obstet* OR pregnan* OR distraction OR immunization OR immunization ORvenipuncture OR venepuncture OR sucrose OR dose OR case report OR case study
OR MeSH terms: Drug dosage calculationsOR publication type: case reports
FILTERS Language: EnglishAND Publication date: from 2008/01/01
PEDIATRICS Volume 145, number s3, June 2020 S245 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

the Middle East 2.3%), North America(40.3%), Oceania (11.6%), and SouthAmerica (3.9%), with the majoritysourced from the United States(n = 34; 37.8%). Subjects within theincluded studies ranged in age, frompremature neonates up to 66 years,and required treatment of oncologicor hematologic conditions, supportduring critical care admission, orvascular access for hemodialysis,postsurgical, or general infusiontherapy or parenteral nutrition (PN).Due to the heterogeneity across ageand conditions in pediatric patients,included articles were divided intospecific clinical subspecialties (eg,hospitalized pediatric patients,hematology or oncology; see Fig 2).Results from individual studies basedon specific hospitalized populations
are presented in Table 2 andinclude key characteristics foreach study.
VAD Selection in HospitalizedPediatric Populations
A total of 3 CPGs and 26 studies wereincluded for general hospitalizedpediatric patients, including 1systematic review, 1 RCT, and 23observational studies. These studiescompared all VADs in hospitalizedadult (n = 3); child (n = 13), infant(n = 2), and neonatal (n = 3); andsurgical (n = 1) populations. With theexception of 1 CPG, no studiesreported on midlines in the pediatricpopulation, so adult studies werealso included.14,43,94
Neonates
Overall, umbilical catheters wereassociated with high rates ofcomplications, including catheter-related bloodstream infection,occlusion, dislodgement, thrombosis,and local infection or phlebitis,with device failure beingcommon.6,15,30,54,57,125,127 Umbilicalcatheter malposition and catheter-tipmigration during treatment alsofrequently occurred,6,142 withconcerns that malpositioned ordislodged umbilical catheters maylead to severe hemorrhage and evendeath if not detected or rectified ina timely manner.58 Despite this, theliterature reviewed indicated thatumbilical catheter placement iscommon practice in neonates up tothe first 7 days of life.23 Evidence forumbilical catheter dwell time wasscarce and supported placement forshort durations only, due to ofincreased risk of device failure.24,57
Consequently, guidance fromavailable CPGs was limited butrecommended placement only for aslong as clinically necessary, or #14days, if managed aseptically.136
Beyond 15 days, ambiguity in theliterature regarding the patency ofthe umbilical vascular system andcatheter for longer durations wasevident.136,142 One CPG did supportreplacing any umbilical catheter witha PICC for central access .7 daysto reduce risk of infection.136
Alternative VADs for neonates includePICCs and CVADs6,34,66,136; however,it was recognized that neonatesfrequently had poor or difficult-to-access venous assets,45,55 were morelikely to have higher risk of insertion-related complications,55 and were athigh risk of blockage across alldevices.6
Infants
PICCs are commonly the first VADchoice for infants.136 Numerousstudies found that PICCs in infantswere associated with a lower risk ofcomplications, particularly
FIGURE 1PRISMA flowchart of study selection. VA, vascular access.
S246 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

thrombosis,28,122 leading currentCPGs to recommend their use inchildren ,1 year and for therapiesfor longer durations (.7days).56,122,136 Conversely, PIVCshad significantly higher rates ofdysfunction in infants (50%)compared with children .1 yearand for longer dwell times,125
with one CPG only recommendingPIVCs for therapies ,6 days.136 Noneof the included evidence evaluatedthe complications associated withmidline catheters in infants; however,the National Association of NeonatalNurses recommended them asan appropriate alternative forperipherally compatible intravenous(IV) therapy for ,6 to 10 days ininfants.136
Compared to PICCs, tunneled-cuffedCVADs were associated with higherrates of thrombosis (althoughthrombosis tended to occur afterlonger durations in situ), with 60% oftunneled-cuffed CVADs developingdeep vein thrombosis (DVT).67
Tunneled-cuffed CVADs were alsoassociated with higher rates ofinsertion failure in infants and youngchildren.55 Risk of infection in CVADsplaced in infants was high, especiallycompared with toddlers, and waslinked to the use of totally
implantable venous devices.59 Astunneled CVADs and totallyimplantable venous devices restrictthe future use and availability ofaccessed veins and insertion wasrelated to a higher risk ofcomplication, studies and CPGsindicated that their use in infantsshould be limited.97,136
Children and Adolescents
For hospitalized children andadolescents, PIVCs and midlinecatheters were reported asappropriate for short-termperipherally compatible therapies inmultiple studies because of their lowrisk of catheter-related infections andthrombosis in comparison toPICCs.14,43,94,100,127,143 However, inone study, the authors suggested thatthese devices are associated withincreased risk of occlusion withextended dwell times.127 PICCs werereported to have high insertionsuccess rates84 and low failure ratesin children and adolescents,6,59
although one study reported severecomplications in 40.1% of failedPICCs, associated with increasingpatient age.28 PICC insertion wascommonly associated with short-termcomplications such as occlusion,CLABSI, and thrombosis,6,30 with
rates of these events increasing withlonger durations of therapy.30
In comparison, tunneled-cuffedCVADs had high rates of infection(4.8%–19.9%)6 and were associatedwith short-term complications, suchas infection, malfunction, leak, andmalposition,59,134 and high rates ofocclusion (12.1%).6 Although totallyimplantable venous devices had lowrates of infection (0.01–0.28 per 1000catheter days),6 they were associatedwith early complications, such asbleeding, pneumothorax, nervelesions, catheter misplacement,occlusion, and skin damage,97,103 andlong-term complications, such asinfection, thrombosis, catheterfracture or disconnection, secondarydislocation, and skin breakdown overport septum.6,56,103 Overall, tunneled-cuffed CVADs and totally implantablevenous devices had high insertionsuccess rates55,59,87 and low failurerates,1,6 and can be used asalternatives to PICCs in patientsrequiring frequent vascular access.56
Given their high insertion successrate,87 nontunneled CVADs can beplaced after the failed placement ofother CVADs.56
VAD Selection in Special PediatricPopulations
Malignant Hematologic and OncologicalConditions
For patients undergoing treatment ofmalignant hematologic andoncological conditions, infection andthrombotic complications, as well asdisruption to treatment, areimportant considerations for VADselection.25,119 A total of 17 studies,including 1 systematic review and 16observational studies, and 5 CPGswere included. Most studies werefocused on tunneled-cuffed CVADsand totally implantable venousdevices in mixed hematology andoncology (n = 5), PN (n = 1), andleukemia (n = 3) populations. Otherstudies compared PICCs, CVADs, andtotally implantable venous devices in
FIGURE 2Quantity of evidence based on patient subgroup. CVAD includes nontunneled, tunneled, and tunneled-cuffed CVADs.
PEDIATRICS Volume 145, number s3, June 2020 S247 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

TABLE2Summaryof
CPGs
andStudiesIncluded
inSystem
aticReview
Study,Year
Participants,n
Design
and/or
Method
Focusand/or
Overview
StudySampleandCharacteristics
Device
Findings
andComments
miniMAGIC
Indication
Adam
set
al,14
2016
—Clinical
review
aClinical
review
ofmidlinecatheter
device
indications
andcomplications
forusein
theED
—Midline
Midlines
have
alowcomplicationrate,longdw
ell
time,andhigh
rateoffirst-attem
ptplacem
ent.
Generalpediatrics
Aiyagariet
al,15
2012
89Observationala
Tocompare
theclinicaloutcom
esforinfantswith
single-
ventriclephysiology
afterum
bilical
catheter
and
femoral
CVAD
placem
ent
Patientswith
single-ventricle
physiology
admitted
totheNICU
(4–13
d)
NontunneledCVAD,u
mbilical
catheter
NontunneledCVADswereassociated
with
higher
ratesof
thrombosisandvein
occlusion.
No
differencewas
seen
amongCLABSI,need
for
transhepaticaccess,and
ultrasound-
documentedthrombusat
theinferior
vena
cava–rightatrial
junction.
Patientswith
nontunneledfemoral
CVAD
for$14
dhad
ahigher
prevalence
ofthrombosisthan
those
for,14
d.No
differencein
theprevalence
of
iliofem
oral
vein
occlusionwas
seen.
Generalpediatrics
Ainsworth
and
McGuire,16
2015
549
System
atic
review
bTo
evaluate
PNdeliveryviaPIVC
orCVAD
inhospitalized
neonates
Included
6RCTs
evaluatingPN
deliveryviaPIVC
or
CVAD
inhospitalized
neonates
PIVC,nontunneled
CVAD
NontunneledCVAD
ledto
asm
allerdeficitof
nutrientsandfewer
catheters;therewas
no
differenceforinvasive
infection.
Long-term
dependent
Altenet
al,17
2012
115
Observationala
Tocompare
USGCVAD
insertionto
landmarktechniques
incritically
illneonates
Retrospectivereview
ofcritically
illneonates
(mean=,14
d)admitted
tothePICU
requiringCVAD
placem
entusingUSGor
landmarktechniques
CVAD
Insertionusingultrasound
guidance
was
associated
with
higher
overallsuccess,first-,
andsecond-attempt
success,andlower
arterial
puncture
rates.
Vessel
visualization
Anilet
al,18
2011
128
Observationala
Toevaluate
complications
associated
with
CVAD
placem
entin
thePICU
Retrospectivereview
ofallpatients(m
edian=21
mo)
admitted
tothePICU
requiringCVAD
placem
ent
CVAD
Therewas
nodifferenceincomplications
forCVAD
insertionat
femoral,subclavian,
orjugular
veins.
Insertionlocation
ANZICS,19
2012
—CPGb
Specificrecommendations
forinsertioncentrallines
for
thepreventionof
CLABSI
—NontunneledCVAD,tunneledCVAD
—Insertionlocation
Allenet
al,20
2008
—Observationala
Todeterm
inetherisk
ofinfectionin
pediatriconcology
patientsrequiringlong-term
vascular
access
12-moprospectivestudyof
pediatriconcology
patients(3
mo–20
yold)
with
aTIVD
or
tunneled-cuffedCVAD
TIVD,tunneled-cuffedCVAD
Therewas
ahigher
rate
ratio
forCLABSIsin
tunneled-cuffedCVAD.
Hematologyand
oncology
ARCandNZRC,21
2010
—CPGb
Specificrecommendations
foraccess
tocirculationin
infantsandchildrenin
thecontextof
cardiorespiratoryarrest
—CVAD,intraosseous,PIVC
—Criticalcare
ARCandNZRC,22
2010
—CPGb
Medicationor
fluids
fortheresuscitationof
the
newborn
infant
—Intraosseous,PICV,um
bilical
catheter
Specificrecommendations
fornewborn
infantsin
thecontextof
resuscitationwereprovided.
Criticalcare
ARCandNZRC,23
2010
—CPGb
Specificrecommendations
forvascular
access
in
pediatricpatientsinthecontextofcardiopulmonary
arrest
—CVAD,intraosseous,PICV
—Generalpediatrics
Arntset
al,24
2014
203
Observationala
Tocompare
theratesof
complications
between
umbilical
cathetersandPIVCsin
newborns
Patientsadmitted
totheNICU
(24–42
wk
gestation)
requiringaPICC
orum
bilical
catheter
PICC,umbilical
catheter
Therewas
nodifferencein
complicationrate
or
dueto
gestationalage.
Generalpediatrics
Athale
etal,25
2012
358
Observationala
Toevaluate
theimpactof
CVAD
on5-yoveralland
event-
free
survival
inchildrenwith
cancer
Childrenwith
non-CNScancer
(#19
yold)
who
required
aCVAD
CVAD
CVAD
dysfunctioncontrolling
for
thromboem
bolism
isassociated
with
poorer
5-yoverallandevent-freesurvival.
Hematologyand
oncology
Avanzini
etal,26
2017
194
Observationala
Todescribe
asingle-centertransitionfrom
CVAD
placem
entviasurgical
cutdow
nto
USGinsertion
techniques
Retrospectivereview
ofpediatricpatients(7
d–18
yold)
who
underw
enttunneled
CVAD
placem
entusingUSGor
surgical
cutdow
n
techniques
Tunneled
CVAD
Double-lumen
PICCswereassociated
with
increasedrisk
ofcomplications,com
paredto
single-lumen
PICCs;complications
were
reported
butnotsignificantlycompared
betweenUSGandsurgical
cutdow
n
techniques.
Device
lumens
Vessel
visualization
Barnwal
etal,27
2016
60Observationala
Tocompare
ECGandlandmarkinsertiontechniques
for
CVAD
placem
ent
Pediatricpatients(0–11
yold)
undergoing
elective
cardiovascular
surgeryrandom
lyassigned
to
CVAD
insertionvialandmarkor
ECG
techniques
CVAD
Therewerefewer
complications
usingUSG
insertiontechniques.
Vessel
visualization
Barrieret
al,28
2012
1280
Observationala
Todeterm
inerisk
factorsforPICC-related
complications
inchildren
Immunocom
prom
ised
children(m
ean=3.2yold;
0–21
yold)
requiringaPICC
PICC
Double-lumen
catheters,PICCsplaced
inthe
femoral
vein
andchildren1–4yold,
comparedwith
olderchildren(5–10
yold,
.10
yold),w
eremoreat
risk
for
complications.
Generalpediatrics
Device
lumens
Insertionlocation
Baskin
etal,29
2019
—CPGb
Specificrecommendations
forcentralvenous
catheters
inchildrenwith
chronicillness
—Midline,PICC,TIVD,
tunneled-cuffedCVAD
—Long-term
dependent
BenAbdelazizet
al,30
2017
215
Observationala
Toexam
inetheincidenceof
PIVC-related
complications
inpediatricpatients
Comparisonof
complications
versus
no
complications
inhospitalized
children
(0.1–18
yold)
requiringaPIVC
PIVC
Longer
durationwas
associated
with
local
complication.
Generalpediatrics
Bezzio
etal,31
2019
205
Observationala
Toinvestigatetherateofandrisk
factorsforinfectionin
childrenundergoing
cardiacsurgeryrequiringCVAD
placem
ent
Prospectivestudyof
pediatricpatients(1
d–25
y
old)
undergoing
cardiacsurgery
CVAD
Infectionrisk
significantlyincreasedwith
increaseddurationof
device
placem
ent;the
SCVvein
was
morelikelyto
developCLABSI.
Congenitalcardiac
Insertionlocation
Blotte
etal,32
2017
162
Observationala
Tocompare
PICC
andCVAD
complications
inpediatric
patientswith
intestinal
failure
Pediatricpatients(1
d–12
yold)
with
intestinal
failure
requiringPN
PICC,tunneled-cuffedCVAD
Tunneled-cuffedCVAD
hadahigher
infectionrate,
andPICCsweremorelikelyto
break.More
Long-term
dependent
S248 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

TABLE2
Continued
Study,Year
Participants,n
Design
and/or
Method
Focusand/or
Overview
StudySampleandCharacteristics
Device
Findings
andComments
miniMAGIC
Indication
tunneled-cuffedCVADshadcentralvenous
thrombosis,whereas
morePICCshadbasilic
vein
thrombosis.
Birhaneet
al,33
2017
178
Observationala
Toassess
factorsthat
impacted
PIVC
lifespan
in
neonates
andinfants
Neonates
andinfants(1
d–11
mo)
requiringPIVC
placem
ent
PIVC
Comparedto
placem
entat
thescalp,hand,orleg,
PIVCsinserted
atthearm
hadalonger
life
span.
Insertionlocation
Bodenham
Chairet
al,34
2016
—CPGb
Specificrecommendations
fortheinsertionof
VADs
in
allpatients
—CVAD,P
IVC
—Criticalcare
Catheter-to-veinratio
Device
lumens
Vessel
visualization
Boeet
al,35
2015
92Observationala
Toevaluate
risk
factorsandcomplications
associated
with
theplacem
entof
transhepaticCVADs
Retrospectivereview
ofcongenitalcardiac
patients(IQ
R=2–10
yold)
undergoing
transhepaticCVAD
placem
ent
Transhepatic
CVAD
Placem
ent$21
dwas
associated
with
increased
transhepaticCVAD
complications.
Criticalcare
Borasino
etal,36
2014
392
Observationala
Todeterm
ineifCVAD
insertioninto
veinsin
theupper
body
isarisk
factor
forchylothorax
Retrospectivereview
ofpediatricpatients(,
1y
old)
undergoing
cardiacsurgery;comparison
amongCVAD
placem
entat
IJVversus
SCV
versus
femoral
vein
CVAD
Insertionat
IJVor
SCVwas
associated
with
ahigher
risk
ofchylothorax.
Insertionlocation
Borettaet
al,37
2018
107
Observationala
Toevaluate
themanagem
entandcomplications
associated
with
PICCsinserted
inpediatriconcology
patients
Pediatriconcology
patients(0–17
yold)
requiring
PICC
placem
ent
PICC
Comparedto
right-sideinsertionlocations,P
ICCs
inserted
ontheleftside
ofthebody
were
associated
with
morecomplications.
Insertionlocation
Bouazizet
al,38
2015
—CPGb
Specificrecommendations
fortheplacem
entof
VADs
underultrasound
guidance
inallpatients
—CVAD,P
IVC
—Vessel
visualization
Bozaan
etal,39
2019
226
Pilotstudya
Toevaluate
theimpact
ofan
interventiondesigned
to
increase
theuseof
single-lumen
PICCs
Pre-andpostinterventio
nof
PICC
placem
entin
hospitalized
adults
(60yold)
PICC
Makingsingle-lumen
PICCsthedefaultoptionand
providingindications
formultilum
endevices
increaseduseof
single-lumen
PICCs.
Device
lumens
Brattonet
al,40
2014
178
Observationala
Toreport
complicationratesof
VADs
inchildren
undergoing
radiotherapy
Retrospectivereview
ofpediatricpatients(1–26
y
old)
undergoing
radiotherapy
who
received
aVAD
PICC,TIVD,
tunneled-cuffedCVAD
TIVDswereassociated
with
lower
infectionand
complicationratesandhadgreaterdurability.
Hematologyand
oncology
Byon
etal,41
2013
98RCTc
Toevaluate
theefficacy
ofUSGSCVcatheterization
Pediatricpatients(0–2.9yold)
undergoing
electivecongenitalcardiacsurgeryor
neurosurgery;randomlyassigned
to
supraclavicularor
infraclavicularapproaches
CVAD
Thesupraclavicularapproach
was
associated
with
shorterpuncture
time,fewer
insertion
attempts,andfewer
misplacem
ents.
Insertionlocation
CamkiranFiratet
al,42
2016
280
RCTc
Tocompare
therate
ofcomplications
associated
with
IJVandSCVCVAD
insertion
Pediatricpatients(16mo–2.2yold)
undergoing
cardiacsurgery;random
lyassigned
toIJVor
SCVinsertion
CVAD
InsertionviatheSCVwas
associated
with
higher
successrates;lower
ratesof
arterial
puncture,catheter-tip
cultures,andCLABSI;
andhigher
ratesofmalposition.Therewas
no
differencein
mechanicalcomplications,ICU
andhospitallength
ofstay,and
in-hospital
mortality.
Insertionlocation
Campagnaet
al,43
2018
1538
Observationala
Todeterm
inethesafety
ofmidlinecathetersused
in
generalhospitalized
adults
Hospitalized
adults
(median=83
yold)
requiring
amidlinecatheter
across
2Italianhospitals
Midline
Atotalof
10%
ofmidlinecathetershadaserious
adverseevent.
Generalpediatrics
Carlsonet
al,44
2015
3846
Observationala
Tocharacterize
procedures
performed
oncritically
ill
childrenby
emergencymedicalservicepersonnelin
out-of-hospitalcontexts
Retrospectivereview
ofpediatricpatients(0–17
y
old)
requiringout-of-hospitalcriticalcare
CVAD,intraosseous
CVADshadhigher
successratescomparedto
intraosseous
devices.
Criticalcare
Carraroet
al,45
2013
—CPGb
Specificrecommendations
fortheuseof
long-term
centralvenous
access
inpediatrichematologyand
oncology
patients
—TIVD,tunneled-cuffedCVAD
—Hematologyand
oncology
Cesaro
etal,46
2016
1161
Observationala
Toreport
thefrequencyandassociated
risk
factorsfor
centralvenous
catheter–associated
complications
inchildrenwith
hemato-oncologicalconditions
Pediatrichematology-oncology
patients(m
edian=
6.1yold)
requiringatunneled-cuffedCVAD
Tunneled-cuffedCVAD
At,6.1yold,
thereweremoremechanical
complications,m
oremalfunctionor
occlusion;
comparedto
single-lumen
devices,double-
lumen
deviceshadmoremechanical
complications,exit-site
ortunnel
infections,
andmalfunctionor
occlusion.
Hematologyand
oncology
Device
lumens
Chen
etal,47
2020
4405
System
atic
review
bTo
compare
risk
associated
with
PICCsplaced
inthe
upperversus
thelower
extrem
ityin
neonates
Neonates
(,28
dold)
requiringPICC
placem
ent
PICC
Therewas
agreaterrisk
ofnonelectiveremovals
andmalpositionin
PICCsplaced
intheupper
versus
lower
extrem
ity;there
was
alower
risk
ofthrombosisin
PICCsplaced
atthe
upperextrem
ity.There
wereno
differences
in
mechanicalcomplications,PICC-related
infection,
orphlebitis.
Insertionlocation
Choi
etal,48
2017
23Observationala
Todeterm
inethesafetyandaccuracy
ofTIVD
placem
ent
usingultrasound
guidance
comparedto
surgical
cutdow
n
Retrospectivereview
ofpediatric(0–16
yold)
hematology,oncology,and
PNpatients
undergoing
TIVD
placem
ent
TIVD
Therewas
nodifferenceusingultrasound
guidance
ininsertiontim
eor
complication
comparedto
surgical
cutdow
n.
Vessel
visualization
Coolinget
al,49
2017
75Observationala
Toexam
inetheperformance
andsafety
offemoral
CVADs
Retrospectivestudyof
pediatricpatients
undergoing
stem
cellcollection(m
edian=3y
old)
requiringCVAD
placem
ent
CVAD
Comparedto
thoracicCVADs,femoral
CVADshad
fewer
flow
-related
adverseevents.
Insertionlocation
Crocoliet
al,50
2015
—CPGb
CVADsin
pediatricpatientswith
cancer
——
PEDIATRICS Volume 145, number s3, June 2020 S249 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

TABLE2
Continued
Study,Year
Participants,n
Design
and/or
Method
Focusand/or
Overview
StudySampleandCharacteristics
Device
Findings
andComments
miniMAGIC
Indication
Midline,PICC,nontunneled
CVAD,TIVD,
tunneled
CVAD,tunneled-cuffedCVAD
Hematologyand
oncology
Long-term
dependent
Catheter-to-veinratio
Device
lumens
Vessel
visualization
Debourdeau
etal,51
2009
—CPGb
Preventionofthrombosisassociated
with
centralvenous
cathetersin
patientswith
cancer
—TIVD,tunneledCVAD
—Hematologyand
oncology
Device
lumens
Insertionlocation
DeCarvalho
Onofre
etal,52
2012
42RCTc
Tocompare
theuseof
ultrasound
andpalpation
insertionsuccessforPICC
placem
entin
pediatric
patients
Anypediatricpatient
(1mo–16
yold)
requiringIV
therapyfor.7d;
random
lyassigned
toUSG
PICC
insertionor
palpation
PICC
USGPICC
insertionwas
associated
with
higher
first-attem
ptsuccessrate,b
ettercatheter
positioning
andshorterinsertiontim
e.
Vessel
visualization
deSouzaet
al,53
2018
80RCTc
Todeterm
ineifUSGPICC
placem
entledto
higher
insertionsuccesscomparedto
landmark
techniques
Critically
illpediatricpatients(IQ
R=3mo–1.3y
old)
admitted
tothePICU
requiringPICC
insertionviatheIJV;random
lyassigned
to
USGor
landmarkinsertion
PICC
USGPICC
insertionwas
associated
with
higher
overallsuccessrate,fi
rst-andthird-attempt
successrate,low
erinsertiontim
e,andfewer
hematom
asandarterialpuncturescompared
tolandmark.
Vessel
visualization
DeWitt
etal,54
2015
180
Observationala
Todeterm
ineprocedural
successandfailure
ratesin
umbilical
catheter
placem
ent
Patientswith
congenitalheartdisease,20
hold
versus
.20
holdrequiringan
umbilical
catheter
Umbilical
catheter
Therewas
ahigher
successrate
foryounger
patients.
Generalpediatrics
Dheeret
al,55
2011
103
Observationala
Tocompare
theratesof
immediate
insertion-related
complications
afterCVAD
placem
entin
pediatric
patients
Hospitalized
children(,
12yold)
requiring
aCVAD;com
parisonof
complications
among
neonateversus
infant
versus
.1–12
yold
CVAD
Neonates
wereat
higher
risk
ofimmediate
insertion-relatedcomplications;m
ore
insertionattemptswereassociated
with
insertion-relatedproblems.
Generalpediatrics
Doellman
etal,56
2015
—CPGb
Specificrecommendations
regardingcentralvenous
cathetersthat
accountfortheunique
needsof
pediatricpatients
—Hemodialysiscatheter,P
ICC,nontunneledCVAD,
TIVD,tunneledCVAD
—Generalpediatrics
Hematologyand
oncology
Criticalcare
Congenitalcardiac
Long-term
dependent
Catheter-to-veinratio
Device
lumens
Vessel
visualization
Dongaraet
al,57
2017
144
RCTc
Tocompare
successandcomplicationrates,cost,and
insertiontim
ebetweenPICCsandum
bilical
cathetersinserted
intheNICU
Patientsadmitted
totheNICU
(mean=34
wk’
gestation)
requiringaPICC
orum
bilical
catheter
PICC,umbilical
catheter
Therewas
nodifferenceinsuccessrate,time,and
short-term
complications
betweenPICCsand
umbilical
catheters.
Generalpediatrics
Elser,5
82013
—Clinical
review
aClinical
review
ofum
bilical
catheter
placem
ent
Patientsadmitted
totheNICU
requiringan
umbilical
catheter
Umbilical
catheter
Umbilicalcatheter
malpositionor
dislodgementis
associated
with
hemorrhaginganddeath.
Generalpediatrics
Fallonet
al,59
2014
244
Observationala
Todeterm
inedevice-related
complications
ininfants
requiringaVAD
Hospitalized
children(0–3yold)
requiring
acentralvenous
catheter
forprolonged
therapy
TIVD,tunneledCVAD
Infants(#
1yold)
hadhigher
complicationrate,
higher
operativeexchange
rate,h
igher
infectionrate,and
shorterdurationcompared
with
toddlers
(.1yold).
Generalpediatrics
Faustinoet
al,60
2013
101
Observationala
Toexploretheincidenceof
DVTin
PICU
patients
requiringacentralvenous
catheter
Critically
illchildren(0–17
yold)
admitted
tothe
PICU;com
parisons
madeam
ongage(,
1y
oldversus
1–13
yoldversus
13–17
yold)
NontunneledCVAD
Comparedwith
infants(,
1yold),P
ICUpatients
13–17
yoldhadhigher
odds
ofDVT.
Criticalcare
Froehlichet
al,61
2009
93Observationala
Todeterm
ineifCVAD
placem
entusingultrasound
guidance
increasesinsertionsuccessand
decreasescomplications
aftersingle-center
transitionto
USGinsertiontechniques
Prospectivestudyofcritically
illpediatricpatients
(median=2.5yold)
admitted
tothePICU
requiringCVAD
placem
entwith
USGor
landmarktechniques
CVAD
Ultrasound
guidance
was
associated
with
significantlylower
arterial
puncturesand
fewer
No.attem
pts.Therewas
nodifference
insuccessrate
orinsertiontim
ebetween
ultrasound
guidance
andlandmarkgroups.
Vessel
visualization
Frykholm
etal,62
2014
—CPGb
Specificguidelines
forpatientsrequiringcentralvenous
cathetersregardingvascular
approach,u
ltrasound
guidance,andpreventionof
complications
—Dialysiscatheters,nontunneledCVAD,P
ICC,
TIVD,
tunneled-cuffedCVAD
—Long-term
dependent
Device
lumens
Vessel
visualization
Gaballahet
al,63
2014
150
Observationala
Todescribe
complicationratesassociated
with
CVAD
placem
entusingultrasound
guidance
and
fluoroscopicguidance
inneonates
andinfants
Retrospectivereview
ofcritically
illneonates
and
infants(premature–1yold)
requiringCVAD
placem
entwith
USGversus
fluoroscopic
guidance
CVAD
Therewas
nodifferencein
complicationrates.
Insertionlocation
Vessel
visualization
Gallagher
etal,64
2014
168
Observationala
Todeterm
ineifCVAD
placem
entusingUSGtechniques
improved
insertionsuccessin
pediatricED
patients
Retrospectivestudyof
pediatric(3–15
yold)
emergencypatientsrequiringCVAD
placem
entwith
orwithoutultrasound
guidance
CVAD
Therewas
higher
insertionsuccesswhenusing
ultrasound
guidance.
Vessel
visualization
Gonzalez
etal,65
2012
172
Observationala
Todeterm
ineifearlyplacem
entof
TIVDsor
tunneled-
cuffedCVADsin
patientsat
high
risk
ofthrombosis
andinfectionledto
higher
surgical
complications
Retrospectivereview
ofchildrenwith
ALL(4
d–16
yold)
athigh
risk
ofinfectionand
thrombosis
TIVDs,tunneled-cuffedCVADs
Therewas
nodifferencein
infectionrate
between
TIVD
andtunneled-cuffedCVADsandno
differenceinrateofinfectioninsingle-versus
double-lumen
devices.
Hematologyand
oncology
Device
lumens
Gorski
etal,66
2016
—CPGb
——
Criticalcare
S250 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

TABLE2
Continued
Study,Year
Participants,n
Design
and/or
Method
Focusand/or
Overview
StudySampleandCharacteristics
Device
Findings
andComments
miniMAGIC
Indication
Specificpracticerecommendations
foradultand
pediatricpatientsrequiringinfusion
therapy,
includingdevice
selection,
placem
ent,and
complicationprevention
Hemodialysiscatheters,intraosseous,longPIVC,
midline,nontunneledCVAD,P
ICC,shortPIVC,
TIVD,tunneledCVAD,u
mbilical
catheter
Congenitalcardiac
Long-term
dependent
Catheter-to-veinratio
Device
lumens
Vessel
visualization
Gray
etal,67
2012
333
Observationala
Toidentifyrisk
factorsforcatheter-related
DVTininfants
,1yold
Hospitalized
infants(m
ean=34
wk’gestation)
requiringaVAD
PICC,tunneled-cuffedCVAD
Meancatheter
days
before
DVTdiagnosiswere
shorterforPICCsthan
fortunneled-cuffed
CVADs;higher
ratesofDVTwereinmultilum
en
CVADs;themajority
ofDVTwas
infemoral
veins.Femoral
CVADswereassociated
with
greaterDVTratesthan
jugularor
SCVCVADs.
Therewas
moreDVTin
femoral
lines
than
in
sapheno-femoral
tunneled-cuffedCVADs.
Long-term
dependent
Device
lumens
Insertionlocation
Gurien
etal,68
2016
1134
Observationala
Todeterm
inetheincidenceof
complications
associated
with
CVAD
placem
entusingUSGtechniques
Retrospective,multicenterreview
ofpediatric
patients(1.5–12
yold)
who
underw
entCVAD
placem
entwith
landmarkor
USGinsertion
CVAD
Therewas
ahigher
first-attempt
successrate
usingultrasound
guidance
buthigher
risk
of
hemothoraxusingultrasound
guidance.
Vessel
visualization
Habaset
al,69
2018
225
Observationala
Todeterm
inethecomplications
associated
with
CVAD
placem
entat
theBCVinsertionsite
Retrospectivereview
ofpediatricpatients(m
ean
=7yold)
admitted
toPICU
requiringCVAD
placem
ent;BCVinsertionsite
versus
all
others
(fem
oral,subclavian,
jugular)
CVAD
Comparedto
otherinsertionsites,BCVhadfewer
complications.
Insertionlocation
Hamed
etal,70
2013
300
Observationala
Todescribe
insertionsuccessrate
andcomplication
rate
afterdeliveryof
anesthesia
tocritically
ill
infantsandtoddlers
Critically
illinfantsandtoddlers
(21d–1.3yold)
requiringem
ergencysurgery
Intraosseous
Intraosseous
access
was
appropriatefor
unobtainable
peripheral
orcentralaccess.
Criticalcare
Hancock-Howardet
al,71
2010
60Observationala
Todeterm
inethecost-effectivenessof
TIVD
placem
ent
usinginterventionalradiology
Retrospectivereview
ofpediatriconcology
patientsundergoing
placem
entof
aTIVD
usinginterventionalradiology(m
ean=7y
old)
orsurgical
cutdow
n(m
ean=4yold)
techniques
TIVD
Insertiontim
ewas
shorterandresultedin
fewer
complications
usinginterventionalradiology
comparedto
surgical
cutdow
n.
Vessel
visualization
Handrupet
al,72
2010
98Observationala
Toevaluate
theratesof
VAD-relatedcomplications
associated
with
placem
entof
aTIVD
ortunneled-
cuffedCVAD
Retrospectivereview
ofchildrenwith
ALL
(,4–.9yold)
who
received
aTIVD
or
tunneled-cuffedCVAD
over
an8-yperiod
TIVD,tunneled-cuffedCVAD
Therewas
ahigher
CLABSI
rate
andnonelective
removal
fortunneled-cuffedCVAD.
Hematologyand
oncology
Hanson
etal,73
2012
1070
Observationala
Toinvestigatetherate
ofandrisk
factorsforVTEin
childrenwith
cardiacdiseaseadmitted
tothePICU
Childrenwith
cardiacdisease(m
edian=10
mo)
admitted
tothePICU;com
parisons
made
among,6moversus
6mo–1yoldversus
1–2yoldversus
2–12
yoldversus
12–18
yold
versus
.18
yold
CVAD
VTEincidencewas
associated
with
increasing
No.
CVAD
days.Inyoungchildren(,
6mo),VTE
incidencewas
significantlyhigher.
Criticalcare
Heinrichset
al,74
2013
1076
System
atic
review
bTo
evaluate
assistivetechnologies,other
than
ultrasound
guidance,inimprovingPIVC
insertion
success
SevenRCTs
ofpediatricpatients(0–21
yold)
requiringPIVC
insertionusingnovel
interventions
PIVC
Transilluminationwas
associated
with
higher
first-attem
ptsuccesscomparedto
traditional
insertiontechniques;first-attem
ptsuccess
usingNIRandtraditional
methods
was
not
significantlydifferent.There
was
no
differencein
timeor
No.attem
ptsbetween
insertionmethods.
Vessel
visualization
Included
studies
Hosokawa,
2010
Katsogridakis,2008
Nager,1992
Perry,2011
Chapman,2011
Kim,2012
Maynard,1989
Institute
forHealthcare
Improvem
ent,7
52012
—CPGb
Specificrecommendations
forthepreventionof
CLABSI
—CVAD
—Vessel
visualization
IVNN
Z,762012
—CPGb
Specificpracticerecommendations
foradultand
pediatricpatientsrequiringinfusion
therapy,
includingdevice
selection,
placem
ent,and
complicationprevention
—Intraosseous,m
idline,nontunneledCVAD,P
ICC,
TIVD,tunneledCVAD,u
mbilical
catheter
—Criticalcare
Long-term
dependent
Device
lumens
Vessel
visualization
Katsogridakiset
al,77
2008
240
Observationala
Todeterm
ineiftransilluminationincreasesPIVC
insertionsuccessin
pediatricpatients
Pediatricpatients(m
ean=13
yold)
with
difficult
venous
access
admitted
totheED
requiring
nonurgentPIVC
placem
ent;random
ly
assigned
towith
orwithouttransillumination
PIVC
Insertionusingtransilluminationwas
associated
with
higher
first-andsecond-attem
ptsuccess
comparedto
withouttransillumination.
Vessel
visualization
Kim
etal,78
2017
132
RCTc
Tocompare
ultrasound
guidance
tolandmark
techniques
forCVAD
insertionin
children
Pediatriccardiacsurgery,neurosurgery,or
generalsurgical
patients(1
mo–6yold)
requiringCVAD
insertion;
random
lyassigned
toUSGinsertionto
theaxillaryvein
orLM
insertionviatheSCV
CVAD
USG1
axillaryinsertionwas
associated
with
fewer
attemptsandshorterinsertiontim
e.
Therewas
nodifferenceincomplicationrates.
Results
wereconfounded
bylocationand/or
imaging.
Insertionlocation
Vessel
visualization
Kulkarni
etal,79
2014
—System
atic
review
bTIVD,tunneled-cuffedCVAD
PEDIATRICS Volume 145, number s3, June 2020 S251 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

TABLE2
Continued
Study,Year
Participants,n
Design
and/or
Method
Focusand/or
Overview
StudySampleandCharacteristics
Device
Findings
andComments
miniMAGIC
Indication
Asystem
aticreview
ofTIVDsandtunneled-cuffedCVADs
inadults
andchildrenreceivingchem
otherapy
5RCTs
and25
observationalstudies
ofadultsand
childrenundergoing
chem
otherapy
Tunneled
CVAD
was
associated
with
more
infections,n
oninfectious
complications,and
device
removal.
Hematologyand
oncology
Kulkarni
etal,80
2017
176
Observationala
Todescribe
thecomplications
relatedtoVADinsertionin
infantswith
hemophilia
Infants(0–2yold)
with
hemophilia
requiring
either
aPICC,TIVD,
ortunneled
CVAD
PICC,TIVD,
tunneled
CVAD
TIVDshadthelowestratesof
complications.
Hematologyand
oncology
Lam
etal,81
2018
954
Observationala
Toevaluate
theimpact
ofdefaultingto
single-lumen
PICCs
Hospitalized
adults
(mean=66
yold)
requiring
PICC
placem
ent;comparisonof
single
versus
double
lumens
PICC
Single-lumen
PICCswereassociated
with
lower
complications.
Device
lumens
Lampertiet
al,82
2012
—CPGb
Specificrecommendations
regardingUSGVAD
placem
ent
—CVAD,P
ICC
—Catheter-to-veinratio
Vessel
visualization
LauandCham
berlain,83
2016
760
System
atic
review
bTo
exam
inethesafety
andefficacy
ofCVAD
insertion
usingultrasound
guidance
Atotalof
8RCTs
comparing
theuseof
USGand
landmarkCVAD
placem
entin
pediatric
patients(,
18yold)
CVAD
Ultrasound
guidance
hadahigher
successrate
andfewer
No.insertionattemptscomparedto
landmarktechniques.
Vessel
visualization
Included
studies
Alderson,1993
Verghese,1999
Verghese,2000
Grebenik,2004
Chuan,
2005
Ovezov,2010
Aouad,
2010
Bruzoni,2013
Levy
etal,84
2010
279
Observationala
Todeterm
inetherate
ofandpotentialrisk
factorsfor
infectious
andnoninfectious
complication
associated
with
PICCsin
pediatricpatients
Hospitalized
children(10d–21
yold)
requiring
aPICC
PICC
Olderagewas
associated
with
infectious
complications.
Generalpediatrics
Lindquesteret
al,85
2017
33Observationala
Toexam
inethesafety
andefficacy
oftunneled
CVAD
placem
entat
theinternal
andexternal
jugularin
neonates
andinfants,5kg
Multicenterretrospectivereview
ofhospitalized
infantsweighing,5kg
(0–1yold)
with
atunneled
CVAD
Tunneled
CVAD
Therewas
nodifferencein
complications
associated
with
jugularandfemoral
vein
insertionlocations.
Insertionlocations
Lovedayet
al,86
2014
—CPGb
Specificrecommendations
forthepreventionof
hospital-acquiredinfections
—PICC,TIVD,
tunneled
CVAD
—Long-term
dependent
Device
lumens
Malbezinet
al,87
2013
5435
Observationala
Toprospectivelydeterm
inetheoverallsuccessand
complicationrate
ofCVAD
insertionover
a22-y
period
Hospitalized
children(m
ean=5yold)
requiring
anyCVAD
CVAD
Device
failure
was
morelikelyin
children,3kg.
Generalpediatrics
Marshallet
al,88
2017
19Observationala
Tocompare
transhepaticCVADsto
nontunneledCVADs
asan
alternativeforpreserving
future
central
venous
access
Retrospectivereview
ofinfants(1.8–7.8mo)
with
congenitalheartdiseasewho
underw
ent
placem
entof
1or
moretranshepaticCVADs
NontunneledCVAD,transhepatic
CVAD
TranshepaticCVAD
hadalonger
duration.
There
was
nodifferencein
thrombi,throm
bolytic
burden,orcatheter
sitesrequiringwound
care
consultation.Therewas
ahigher
frequencyof
infectionin
transhepaticCVAD.
Therewas
nodifferencein
therate
of
infection-relatedremoval.
Congenitalcardiac
Marquez
etal,89
2016
175
Observationala
Todeterm
inerisk
factorsforthrombosisafter
placem
entof
nontunneledCVADsin
PICU
patients
Prospective,multicenterstudyof
pediatric
patients(4
mo–8.6yold)
admitted
tothePICU
undergoing
CVAD
placem
ent
NontunneledCVAD
Therewerehigher
ratesof
DVTin
patientswith
right-sidenontunneledCVAD
placem
entand
insertionat
SCV.
Insertionlocation
May
etal,90
2018
912
Observationala
Todeterm
inetheratesof
thrombosis,infection,
and
insertionsite
symptom
safterplacem
entof
PICCs
andTIVDsin
patientswith
cysticfibrosis
Retrospectivereview
ofadultandpediatric
patents(m
ean=7.4yold)
with
cysticfibrosis
PICC,TIVD
Double-lumen
PICCswereassociated
with
greater
ratesof
complications.
Long-term
dependent
Device
lumens
Menéndezet
al,91
2016
256
Observationala
Toevaluate
theincidenceandrisk
factorsforPICC-
relatedthrombosisin
children
Hospitalized
children(IQ
R=2.4–13
yold)
requiringPICC
placem
ent
PICC
Acatheter-to-veinratio
of.0.33
predictedPICC-
relatedsuperficial
vein
thrombosisandDVT.
Catheter-to-veinratio
Mermel
etal,92
2009
—CPGb
Specificrecommendations
forthepreventionof
catheter-related
infection
—CVAD,m
idline,PICC,PIVC,TIVD
—Long-term
dependent
Moonet
al,93
2018
629
Observationala
Todeterm
inerisk
factorsforCLABSI
inchildrenwith
hemato-oncologicaldiseaserequiringlong-term
VADs
Retrospectivereview
ofchildrenwith
hemato-
oncologicdisease(m
edian=6yold;
14
d–17.9yold)
requiringanylong-term
CVAD
TIVD,tunneled-cuffedCVAD
Therewas
nodifferencein
therate
ofCLABSI.
Hematologyand
oncology
Mushtaq
etal,94
2018
693
Observationala
Todeterm
inethesafety,specifically
ratesof
CLABSI,
mechanicalcomplications,h
ospitallength
ofstay,
readmission
within90
dof
discharge,andmortality
ofmidlinecatheterscomparedto
CVADsin
adults
admitted
tointensivecare
Adults
.18
yoldadmitted
totheICUor
medical-
surgical
wardwith
either
aCVAD
ormidline
catheter
CVAD,m
idline
CVADswereassociated
with
higher
ratesof
CLABSI,crudemortality,readmission,and
transfer
totheICU.
Midlinecathetershad
moremechanicalcomplications.
Generalpediatrics
Noailly
Charny
etal,2
2018
295
Observationala
Tocompare
therisk
ofthrombosisin
PICCsand
tunneled-cuffedCVADs
Children(,
18yold)
diagnosedwith
leukem
ia
who
received
aPICC
ortunneled-cuffedCVAD
PICC,tunneled-cuffedCVAD
PICCswereassociated
with
anincreasedrisk
of
thrombosis.
Hematologyand
oncology
Nifong
andMcDevitt,95
2011
—Laboratory
studya
Todeterm
inetheeffect
ofcatheter
size
offluidflow
rates
—PICC
Fluidflow
ratedecreasedwith
increasing
catheter
size.
Catheter-to-veinratio
O’Gradyet
al,96
2011
—CPGb
Specificrecommendations
forthepreventionof
intravascularcatheter-related
infections
—Midline,nontunneledCVAD,P
ICC,PIVC,TIVD,
tunneled
CVAD
—Device
lumens
Vessel
visualization
Ohno
etal,97
2016
120
Observationala
Todeterm
inetheratesof
complications
andCLABSI
in
infantsandsm
allinfants(,
1yoldor
,10
kg)
comparedwith
children(.
1yoldor
.10
kg)
Children(4
mo–22
yold)
requiringaTIVD
TIVD
Agewas
notassociated
with
increasedrisk
of
complications.
Generalpediatrics
S252 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

TABLE2
Continued
Study,Year
Participants,n
Design
and/or
Method
Focusand/or
Overview
StudySampleandCharacteristics
Device
Findings
andComments
miniMAGIC
Indication
Oulego-Erroz
etal,98
2016
46Pilotstudya
Todeterm
ineifCVAD
insertionto
theBCVusingUSG
techniques
hadgreaterinsertionsuccesscompared
toinsertionto
theIJV
Prospectivestudyof
critically
illchildren(0.6
mo–13
yold)
requiringurgent
CVAD
insertion;
nonrandom
assignmentto
BCV1
USGor
IJV
insertion
CVAD
BCV1
ultrasound
guidance
hadahigher
first-
attempt
successrate,few
erinsertion
attempts,andlower
insertiontim
ecompared
toIJV.Therewas
nodifferencein
overall
successrates.
Insertionlocation
Vessel
visualization
Oulego-Erroz
etal,99
2018
500
Observationala
Todeterm
ineifCVAD
placem
entoutcom
escanbe
improved
byusingUSGinsertion
Prospective,multicenterstudyof
allcritically
ill
children(IQ
R=2mo–4.9yold)
requiring
temporary
CVAD
placem
entusingUSGor
landmarktechniques
CVAD
Ultrasound
guidance
hadahigher
first-attem
pt
successrate
andfewer
puncture
attempts
andmechanicalcomplications.
Vessel
visualization
Pacilli
etal,10
02018
18Observationala
Todeterm
inetheappropriatenessof
long
PIVCsin
pediatricpatientsundergoing
surgery
Childrenundergoing
surgery(m
ean=6.3yold)
requiringlong
PIVC
insertion
Long
PIVC
Therewereno
immediatecomplications.Onday3,
removalsweremadebecauseof
3occlusions
and1red/pain.
Generalpediatrics
Paladini
etal,10
12018
40Pilotstudya
Tocompare
thesuccessof
USGlong
PIVC
insertionin
childrenadmitted
totheED
toshortPIVCs
Children.10
yold(m
ean=13
yold)
who
were
admitted
totheED;com
parisonofblindshort
PIVC
versus
USGPIVC
insertion
Long
PIVC,short
PIVC
ShortP
IVCs
hadashorterdw
elltimedurationand
morecomplications
comparedto
long
PIVCs;
ultrasound
guidance
hadalower
risk
of
failure
andcomplications
butresults
confounded.
Criticalcare
Vessel
visualization
Park
etal,10
22016
3832
System
atic
review
bTo
determ
inetheutility
ofNIRlight
devices
Atotalof
11RCTs
ofanypediatricpatient
(,21
y
old)
undergoing
PIVC
placem
entusingNIRor
noassistivedevice
PIVC
Therewas
nooveralldifference
inoverallsuccess
rate
betweenNIRlight
device
andtraditional
methods;however,N
IRlight
deviceshad
ahigher
successrate
forsubsetsdeem
ed
high
risk
offailure.
Vessel
visualization
Included
studies
Chapman,2011
Perry,2011
Kaddoum,2012
Kim,2012
Cuper,2013
Graaff,
2013
Sun,
2013
Szmuk,2013
Woude,2013
Graaff,
2014
Curtis,2015
Pasteuret
al,10
32010
—CPGb
Specificrecommendations
forpatientswith
non-CF
bronchiectasis
—TIVD
—Long-term
dependent
Peterson
etal,10
42012
1399
Observationala
Todeterm
ineifassistivedevicesimprovePIVC
insertion
success
Hospitalized
children(m
ean=1yold)
requiring
PIVC
placem
ent;random
lyassigned
to
unassisted
versus
assisted
(transillum
ination
versus
NIRlight
device–guided)insertion
PIVC
PIVC
insertionsuccesswas
higher
whenno
assistivedevice
was
used
comparedto
assisted
methods.
Vessel
visualization
PerinandScarpa,10
5
2015
—System
atic
review
bTo
review
evidence
relatedto
theassessmentof
catheter-tippositioning
inpediatricpatients
Included
42pediatricstudiesexam
iningoutcom
es
forpatientsundergoing
VADplacem
entusing
vessel
visualizationtechniques
CVAD,P
ICC,
umbilical
catheter
Therewas
insufficienthigh-qualityevidence
to
makespecificrecommendationforusein
pediatricpatients.
Vessel
visualization
Pinonet
al,10
62009
915
Observationala
Todeterm
inetheincidenceandrisk
factorsof
central
venous
catheter-related
complications
inpediatric
hemato-oncologicalandimmunologic
conditions
Single-center,prospectivestudyof
children
(0–19
yold)
with
oncological,hematologic,or
immunologicdiseases
TIVD,tunneledCVAD
Tunneled-cuffedCVADswereassociated
with
more
CLABSI;being#3yoldwas
associated
with
moredislodgements
andmoretunnel
infections;C
LABSIwas
moreprevalentin
double-versus
single-lumen
devices.
Hematologyand
oncology
Device
lumens
Pittirutiet
al,10
72009
—CPGb
Specificrecommendations
forCVADsandcomplication
preventionin
patientsrequiringPN
—Midline,PICC,PIVC,TIVD,tunneledCVAD
—Long-term
dependent
Device
lumens
Vessel
visualization
Polkinghorne
etal,10
8
2013
—CPGb
Specificrecommendations
forvascular
access
in
patientswith
chronicrenaldisease
—NontunneledCVAD,tunneledCVAD
—Vessel
visualization
Qian
etal,10
92014
40Observationala
Toexam
inecomplicationratesinpediatricpatientswith
CFaftertheplacem
entof
along
PIVC
Prospectiveauditof
pediatricpatientswith
CF
with
infectiveexacerbation
Long
PIVC
Complicationrateswerehigh;noseriousadverse
outcom
eswerereported.
Long-term
dependent
Ramer
etal,11
02016
53RCTc
Toevaluate
theeffectivenessof
NIRlight
device
technology
forPIVC
placem
entin
pediatric
hematologyandoncology
patients
Pediatrichematologyandoncology
patients
(1–21
yold)
requiringPIVC
placem
ent;
random
lyassigned
toNIRlight
device
or
landmarkinsertiontechniques
PIVC
NIRlight
device
was
associated
with
faster
insertiontim
eandhigher
satisfaction.
Vessel
visualization
Rauthet
al,11
12008
138
Observationala
Toinvestigatetherate
ofinfectionin
infantswhenthe
venous
catheter
isexchangedforatunneled-cuffed
CVAD
afterECMOdecannulation
PICU
patients(m
ean=13
d)requiringCVAD
placem
entafterdecannulationfrom
ECMO
Tunneled-cuffedCVAD
Increasing
thedurationof
ECMOandCVAD
placem
entindependently
predictedCLABSI.
Criticalcare
Revel-Vilk
etal,11
22010
d423
Observationala
Todeterm
inetherate
ofcatheter-related
complications
inchildrenundergoing
chem
otherapy
during
12mo
oftherapy
Single-center,prospectivestudyof
pediatric
patients(29d–28
yold)
undergoing
chem
otherapy
PICC,tunneled-cuffedCVAD
PICCswereassociated
with
ahigher
risk
ofDVT;
tunneled
CVAD
hadahigher
risk
ofocclusion
at1y.
Hematologyand
oncology
Reyet
al,11
32009
825
Observationala
Toidentifyrisk
factorsforearlymechanical
complications
inCVADs
CVAD
Difficultvenous
access
Insertionsite
PEDIATRICS Volume 145, number s3, June 2020 S253 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

TABLE2
Continued
Study,Year
Participants,n
Design
and/or
Method
Focusand/or
Overview
StudySampleandCharacteristics
Device
Findings
andComments
miniMAGIC
Indication
Pediatricpatients(m
edian=22
mo)
admitted
to
thePICU;com
parisons
amongfemoral,
jugular,andSCVCVAD
insertionsites
SCVandjugularvein,aswellas
increasing
No.
attemptswereassociated
with
significantly
moreearlymechanicalcomplications.
Rivera-Tocancipa
etal,11
4
2018
201
Observationala
Todescribe
theincidenceof
complications
associated
with
USGCVAD
insertionin
childrencomparedto
anatom
iclandmarktechniques
Allhospitalized
children(0–18
yold)
requiring
CVAD
insertionusingUSGor
LMinsertion
techniques
CVAD
Ultrasound
guidance
hadfewer
immediate
complications,no
arterial
punctures,and
higher
ratesof
insertionsuccesscompared
tolandmarktechniques.
Vessel
visualization
Rosado
etal,11
52013
255
Observationala
Toexam
inetherate
ofCVAD-associatedinfectionin
PICU
patients
Prospective,single-centerreview
ofchildren
(majority
,6yold)
admitted
tothePICU
requiringaCVAD
CVAD
CVADsinserted
$7dwereassociated
with
ahigher
risk
ofCLABSI.
Criticalcare
Rossettiet
al,11
62015
309
Observationala
Toinvestigatethesafety
andaccuracy
ofintracavitary
ECG-guided
insertionin
pediatricpatients
Prospective,multicenterstudyof
hospitalized
pediatricpatients(1
mo–18
yold)
requiring
aVAD;
insertionusingintracavitary
ECG
versus
intracavitary
ECGwith
dedicatedECG
monitorcompared
CVAD,P
ICC
Insertionaccuracy
was
higher
with
adedicated
ECGmonitor.
Vessel
visualization
Schifferet
al,11
72013
—CPGb
Specificrecommendations
forcentralvenous
catheters
inpatientswith
cancer
—NontunneledCVAD,P
ICC,tunneled
CVAD,TIVD
—Hematologyand
oncology
Vessel
visualization
Sharpet
al,11
82015
136
Observationala
Toidentifytheoptim
alratio
cutoffto
reduce
ratesofVTE
Prospectivestudyof
hospitalized
adults
(mean=
57yold)
requiringPICC
insertion,comparison
between#45%versus
$45%catheter-to-vein
ratio
PICC
A.45%
ratio
was
morelikelyto
developVTE.
Catheter-to
vein
ratio
Shenep
etal,11
92017
90Observationala
Todeterm
inetheinteractionbetweenPN
andexternal
centralvenous
devicesin
increasing
risk
of
complications
Ratesof
complications
during
PNandnon-PN
periodsin
pediatriconcology
patients
(median=7.3yold)
requiringcentralvenous
devices
TIVD,tunneledCVAD
Risk
ofCLABSI
was
higher
during
PNforchildren
with
TIVDs.Occlusionrisk
was
higher
for
TIVDs.ComplicationratesforTIVDswere
lower
during
thenon-PN
period
butsimilar
during
thePN
period.
Long-term
dependent
Sibson
etal,12
02018
—CPGb
Specificrecommendations
forpreventingthrombosisin
pediatricpatientswith
cancer
—PICC,PIVC,TIVD,tunneledCVAD
—Hematologyand
oncology
Sigaut
etal,12
12009
359
System
atic
review
bTo
evaluate
theadvantages
ofUSGCVAD
placem
entover
anatom
iclandmarktechniques
inpediatricpatients
Children(2
d–8yold)
undergoing
cardiacsurgery
requiringCVAD
CVAD
Forultrasound
guidance,nodifferenceinratesof
artery
puncture,h
ematom
a,hemothorax,
pneumothorax,or
timeto
insert
was
found.
Ultrasound
guidance
hadhigher
success
ratesforsubsetsof
novice
operatorsand
during
intraoperativeuse.
Vessel
visualization
Included
studies
Alderson,1993
Chuan,
2005
Verghese,1999
Verghese,2000
Grabenic,2004
Smitherman
etal,12
2
2015
1135
Observationala
Todeterm
inerisk
factorsforthedevelopm
entof
catheter-associatedVTEin
generalhospitalized
pediatricpatients
Chartreview
ofhospitalized
children(m
ean=8y
old)
requiringaVAD
PICC
Increasing
agewas
relatedtoan
increasedrisk
of
thrombosis;lumen
No.w
asnotassociated
with
thrombosisrisk;insertionsite
(brachial
orcephalic,S
CV,jugular,orfemoral
or
saphenous)
was
notassociated
with
an
increasedrisk
ofthrombosis.
Generalpediatrics
Device
lumens
Insertionlocation
Takeshita
etal,12
32015
96Observationala
Toexam
inethefactorsthat
affect
insertionsuccessfor
invisibleandimpalpableperipheralveinsinchildren
Pediatricpatients(1.1–2.8yold)
with
invisibleor
impalpable
veinsundergoing
electivesurgery
PIVC
PIVC
with
ultrasound
guidance
hadbetter
success
ratescomparedto
PIVC
withoutultrasound
guidance;com
paredto
insertionto
thedorsal
hand
vein,the
cephalicvein
hadahigher
successrate
andshorterinsertiontim
e.
Difficultaccess
Insertionlocation
Vessel
visualization
Takeshita
etal,12
32015
196
RCTc
Toexam
inethefactorsthat
affect
insertionsuccessfor
invisibleandimpalpableperipheralveinsinchildren
Pediatricpatients(10–40
mo)
with
invisibleor
impalpable
veinsundergoing
electivesurgery
PIVC
Comparedto
insertionto
thedorsal
hand
or
saphenousvein,the
cephalicvein
had
ahigher
successrate.
Insertionlocation
TheJointCommission,12
4
2013
—CPGb
Specificrecommendations
forpreventingCLABSI
in
CVADs
—CVAD
—Device
lumens
Tripiet
al,12
52016
108
Observationala
Todeterm
inethefrequencyof
PIVC-related
dysfunction
inpediatricpatients
ComparedPIVC
dysfunctionin
hospitalized
children(0–.12
yold)
over
device
durations
of1–2dversus
2–3dversus
.3d
PIVC
Higher
ratesof
PIVC
dysfunctionwereassociated
with
PIVCsin
placefor.3dor
inserted
in
lower
extrem
ities.
Generalpediatrics
Troianos
etal,12
62011
—CPGb
Specificrecommendations
forVADplacem
entusing
ultrasound
guidance
inpediatricpatients
—CVAD,P
ICC,
PIVC
—Vessel
visualization
Ullman
etal,62015
31933
System
atic
review
bTo
review
theincidenceof
VADfailure
inpediatric
patients
Hospitalized
pediatricpatientsacross
74studies
requiringanyVAD
Hemodialysiscatheter,n
ontunneled
CVAD,P
ICC,
TIVD,tunneledCVAD,u
mbilical
catheter
Hemodialysiscathetersandum
bilical
catheters
hadthehighestfailure
rate;TIVDs
hadthe
lowestfailure
rate.
Generalpediatrics
Ullman
etal,12017
1027
Observationala
Toexam
inetheprevalence,m
anagem
ent,andassociated
complications
ofCVADsin
pediatricpatients
Hospitalized
pediatricpatients(IQ
R=1–12
yold)
requiringanyVAD
Hemodialysiscatheter,n
ontunneled
CVAD,P
ICC,
TIVD,tunneledCVAD,u
mbilical
catheter
PICCshadhigher
proportions
ofCVAD-associated
complications
intheprevious
7d.
Generalpediatrics
S254 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

TABLE2
Continued
Study,Year
Participants,n
Design
and/or
Method
Focusand/or
Overview
StudySampleandCharacteristics
Device
Findings
andComments
miniMAGIC
Indication
Unbeck
etal,12
72015
2032
Observationala
Toidentifyrisk
factorsforPIVC-associatedcomplications
inpediatricpatients
Comparisonof
hospitalized
neonatal
versus
pediatricpatients(0–18
yold)
requiring
aPIVC
PIVC
Occlusionwas
associated
with
longer
dwelltim
e.
Neonatal:P
IVCsurvival
timewas
shorter;
therewas
moreinfiltration.
Insertionat
the
arm
bend
oranklewas
associated
with
higher
ratesof
infiltrationandocclusion.
Generalpediatrics
Insertionlocation
vanGent
etal,12
82017
538
Observationala
Todeterm
inetheratesof
infectionandcomplications
in
pediatrichematology,oncology,and
stem
cell
transplant
patients
Retrospectivereview
ofpediatricpatients(m
ean
=7.8yold)
aftersurgical
placem
entof
any
CVAD
TIVD,tunneled-cuffedCVAD
Tunneled-cuffedCVAD
hadalower
risk
ofinfection.
Hematologyand
oncology
Vierboom
etal,12
92018
232
Observationala
Toevaluate
thesafety
oftunneled
CVAD
insertionin
childrenweighing,10
kg
Retrospectivereview
ofallchildren(,
1mo–4y
old)
receivingsurgicalinsertionofatunneled
CVAD
with
ultrasound
guidance
orviasurgical
cutdow
n
Tunneled
CVAD
USGinsertionwas
associated
with
lower
mechanicalblockages,buttherewas
no
differenceinintraoperativeandpostoperative
complications,tim
eto
insert,ordevice
longevity.
Vessel
visualization
Vinograd
etal,13
02018
300
Observationala
Toevaluate
PIVC
insertionsuccessin
patientswith
difficultvenous
access
usingUSGtechniques
Pediatricpatients(m
edian=14
yold)
inan
ED
who
hadafailedPIVC
attempt
viatraditional
insertiontechniques
PIVC
PIVC
usingUSGtechniques
ledto
68%
and87%
first-andsecond-attem
ptsuccessratesafter
failedtraditional
method.
Difficultaccess
Vessel
visualization
Voigtet
al,13
12012
—System
atic
review
bTo
review
theevidence
fortheuseof
intraosseous
devicesin
emergent
contexts
Studiesevaluatingintraosseous
devicesin
patientsrequiringem
ergent
vascular
access
ornonhum
anrandom
ized
prospectivestudies
Intraosseous
Comparedto
alternativeaccess,there
was
no
differencein
complications
using
intraosseous
devices.
Criticalcare
Wiegering
etal,13
22014
43Observationala
Todeterm
inetheincidenceof
catheter-related
thrombosisin
pediatriconcology
patients
Single-centerretrospectivereview
ofpediatric
oncology
patients(m
ean=9.4yold)
requiring
centralvenous
access
TIVD,tunneled-cuffedCVAD
TIVDsshow
edan
earlierpeak
ofthrombosis
occurrence
than
that
oftunneled-cuffedCVAD
catheters;thehighestincidenceof
thrombosisoccurred
intheSCV,followed
by
externaljugularandcephalicsites.Therewas
nodifferencein
complications
between
insertionat
theleftandrightside.
Hematologyand
oncology
Insertionlocation
White
etal,13
32012
322
Observationala
Tocompare
therate
ofcomplications
andearlyremoval
betweenTIVDsandtunneled-cuffedCVADs
Retrospectivereview
ofchildren(1
mo–19
yold)
with
ALLrequiringaTIVD
oratunneled-cuffed
CVAD
TIVD,tunneled-cuffedCVAD
TIVDshadless
complications.
Hematologyand
oncology
Wragg
etal,13
42014
100
Observationala
Todeterm
inetherate
ofocclusionassociated
with
tunneled-cuffedCVAD
insertionunderultrasound
guidance
Children(21d–16
yold)
requiringelectiveor
emergencyremovalof
atunneled-cuffedCVAD
Tunneled-cuffedCVAD
Completevenous
occlusionwas
associated
with
youngerage.
Generalpediatrics
Vessel
visualization
Wuet
al,13
52013
508
System
atic
review
bTo
evaluate
whether
USGCVAD
insertionwas
more
successful
comparedto
anatom
iclandmark
techniques
Meta-analysis
ofRCTs
comparing
USGversus
landmarkCVAD
insertioninpediatricpatients
(mean=0.5–,8yold)
CVAD
Therewerefewpediatricstudies(n
=2),w
hich
limitedanalysis.For
ultrasound
guidance,
therewas
noreductionin
therisk
of
cannulationfailure,arterialpuncture,
hematom
a,pneumothorax,andhemothoraxin
childrenor
infants.
Vessel
visualization
WyckoffandSharpe,13
6
2015
—CPGb
Specificrecommendations
forvascular
access
in
neonates
andinfants
—Midline,PICC,PIVC,TIVD,tunneledCVAD,umbilical
catheter
—Generalpediatrics
Congenitalcardiac
Catheter-to-veinratio
Vessel
visualization
Xiaet
al,13
72016
48RCTc
Todeterm
inetheefficacy
andrate
ofcomplications
in
pediatricpatientswith
moderate-to-severeburn
injuries
Pediatricpatients(m
ean=2.2yold)
with
moderate-to-severeburn
injuries
PICC,PIVC
Therewas
ahigher
1-tim
epuncture
successrate,
longer
retentionduration,
andmore
complicationforPICCscomparedto
PIVCs
Criticalcare
Yacobovich
etal,13
82015
d423
Observationala
Todeterm
inepatient-andcatheter-related
risk
factors
forCLABSI
inchildrenreceivingchem
otherapy
Prospectivestudyof
pediatricpatients(29d–28
y
old)
receivingchem
otherapy
requiringaVAD
PICC,TIVD,
tunneled-cuffedCVAD
Tunneled-cuffedCVADsandPICCshadahigher
risk
forCLABSI
inthegroupof
diseases
with
lower
rate
ofinfection.
Indiseases
with
high
rate
ofinfection,
therewas
nodifference.
Hematologyand
oncology
Zanolla
etal,13
92018
51RCTc
Todeterm
ineifUSGtechniques
reduce
theNo.puncture
attempts,proceduretim
e,andcomplicationrates
during
CVAD
insertionviatheIJVin
children
Prospectivestudyof
anychild
(11mo–9yold)
requiringCVAD
insertionviatheIJV;random
ly
assigned
toUSGversus
landmarkinsertion
groups
CVAD
USGtechniques
required
fewer
attempts,took
less
time,andresultedin
fewer
complications,comparedto
landmark
techniques.
Vessel
visualization
Zengin
etal,14
02013
64Observationala
Todeterm
inerisk
factorsforCVAD-related
complications
inchildrenadmitted
totheED
Retrospectivereview
ofpediatricpatients(2–16
y
old)
admitted
totheED
NontunneledCVAD
Morecomplications
wereassociated
with
.3
attempts.
Difficultvenous
access
Zhou
etal,14
12017
281
Observationala
Toevaluate
thefeasibilityandsafetyofintracavitary
ECG
techniquein
guidingPICC
placem
entin
neonates
Hospitalized
neonates
(27–41
wk)
requiringPICC
placem
entusinglandmarktechniques
or
intracavitary
ECGguidance
PICC
Intracavitary
ECG-guided
PICC
placem
enthad
ahigher
correcttip
positionon
thefirst
attempt
comparedto
landmarktechniques.
Vessel
visualization
ALL,acutelymphoblasticleukem
ia;ANZICS,AustralianandNewZealandIntensiveCare
Society;ARC,AustralianResuscitationCouncil;BCV,brachiocephalic
vein;CF,CysticFibrosis;CNS,CentralNervousSystem
;ECM
O,Extracorproeal
mem
brane
oxygenation;IJV,internaljugularvein;IQR,interquartilerange;IVNN
Z,IntravenousNursingNewZealandIncorporated
Society;LM
,Landm
ark;miniMAGIC,M
ichiganAppropriatenessGuideforIntravascularCathetersinPediatrics;m
o,monthsold;
NZRC,N
ewZealandResuscitationCouncil;SCV,subclavian
vein;TIVD,
totally
implantablevenous
device;VTE,venousthromboem
bolism;—
,not
applicable.
aLowstrength
ofevidence:observationalstudy(with
comparator)
andother(eg,clinical
review
orpilotstudy).
bHigh
strength
ofevidence:C
PG,systematicreview
.cModeratestrength
ofevidence:R
CT.
dSamesample.
PEDIATRICS Volume 145, number s3, June 2020 S255 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

mixed hematology and oncologypopulations (n = 5).
Overall, tunneled-cuffed CVADs andtotally implantable venous deviceshad low rates of insertion-relatedcomplications, device failure, andmalfunction40,65,79,80,119,128 andwere associated with low rates ofthrombosis.2,112,132 Reporting onrates of infection between deviceswas variable. Two studies found thatrates of infection were notstatistically different betweentunneled-cuffed CVADs and totallyimplantable venous devices.79,93 Incontrast, other studies found higherrates of CLABSI in totallyimplantable venous devicescompared to CVADs119 and higherrisk of overall infection in totallyimplantable venous devicescompared to tunneled-cuffedCVADs.128 Additional studies foundthat overall infection rates werehigher in tunneled-cuffed CVADscompared to totally implantablevenous devices.20,40,72,106 Althoughocclusion was common in thispopulation,46,65,112,119 rates were notdifferent between tunneled-cuffedCVAD and totally implantable venousdevices.65,133 Compared to totallyimplantable venous devices andtunneled-cuffed CVADs, PICCs hadhigher rates of device-relatedcomplications as well as overallinfection and CLABSI, thrombosis,and occlusion.2,40,112,138
International guidelines recommendthe use of tunneled-cuffed CVADs forpediatric patients undergoinghematologic and oncologicaltreatment requiring frequent andcontinuous vascular access,particularly for frequent bloodsampling, PN, and complex IVtherapies.50,56 Totally implantablevenous devices may also beappropriate across theseindications,51 especially in patients$10 kg.45 These devices were onlyrecommended for intermittent use,however, due to the increased risk ofinfection and thrombosis.45,50 One
CPG endorsed the use of PICCs forshort- to medium-term treatments,50
although there was insufficientevidence to support their routineuse,117,120 and chemotherapytreatment via peripheral venousaccess was not recommended.50,120
No included studies reported onnontunneled CVADs; however, oneinternational guideline supported theplacement for intrahospital use orshort durations only.50
Critically Ill Patients
Unlike other patient groups, forcritically ill infants, children, andadolescents, choice of VAD may beprioritized by whether the patient isstable or unstable.21,22 Sevenobservational studies, 1 systematicreview, and 1 RCT were includedfor critical care patients andincluded the emergency department(ED) (n = 2), emergency surgery(n = 1), moderate-severe burns(n = 1), out-of-hospital criticalcare (n = 1), and PICU (n = 4)populations. No studies exploredmidline devices in the critical carepopulation, although one studycompared short and long PIVCs.101
Overall, the focus of the studies in thispopulation was on infection andthrombosis and not on outcomes suchas dwell time, occlusion, infiltration,extravasation, or bleedingcomplications.
Stable, Critically Ill Patients
Regarding stable, critically ill patientsrequiring short-term acute therapy, 2CPGs supported the use ofnontunneled CVADs for any type ofinfusion therapy up to 7 to 10 daysdespite risk of infection andthrombosis.34,56 Evidence to supportthe use of PICCs in this populationwas mixed. Whereas the InfusionTherapy Standards of Practicecautioned against the use of PICCs incritically ill patients (adults andpediatrics) because of the risk ofinfection or thrombosis,66 2 otherclinical guidelines recommendedPICCs for both short-34,76 and long-
term34 durations in critically illpatients. This variability may be dueto the scarcity of high-qualityevidence directly comparing thesedevices. PIVCs were frequentlyreported within this population101,137
and were recommended overintraosseous devices in nonemergentsituations.21,22 However, comparedto PICCs, PIVCs were commonlyassociated with obstruction, leakage,and dislodgment,137 with short PIVCsin particular linked to higher ratesof local infections, dislocation,infiltration, occlusion, and thrombosiscompared to long PIVCs.101 Therewere limited studies reporting onnontunneled CVAD use in critically illchildren; however, authors of onestudy reported children .13 yearsold with a nontunneled CVAD were athigher risk of DVT compared withchildren ,1 year.60 Tunneled-cuffedCVADs and totally implantablevenous devices were associatedwith high rates of infection andthrombosis but were reportedas suitable for long-term therapiesin this population.34,73,111,115 Nostudies or CPGs reported on thesuitability of midline devices inthis population specifically, althoughthey were more broadly consideredappropriate for therapies lasting1 to 4 weeks.76
Unstable, Critically Ill Patients
In unstable, critically ill patients,speed of access was prioritized.International guidelines recommendvenous access via PIVC placementunless attempts to cannulate take.60 seconds or $2 attempts.21,22
When IV access was difficult,intraosseous devices wereconsistently reported as fastalternatives for children andadolescents,21,44,66,70,76,131 andumbilical catheter was recommendedfor neonates in the first week ofage.22
Congenital Cardiac Conditions
For patients with congenital cardiacconditions, VAD selection prioritizes
S256 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

vessel preservation to ensure keyvasculature can be used for futurelife-saving procedures.56 Overall, 3CPGs and 4 observational studiesof pediatric and young adultpatients were included in thesystematic review and encompassedpatients with univentricular andbiventricular physiology andpatients in cardiac surgerysubgroups. Comparisons betweenumbilical catheters, PICCs, tunneledCVADs, and nontunneled CVADsbased on dwell time, occlusion,thrombosis, and infection risk werethe primary focus of the includedstudies.15,31,35,88
Generally, short-term peripheral andnonperipheral compatible therapydelivered via umbilical catheters ininfants can be used.66 PICCs wererecommended for patients withcongenital cardiac conditionsrequiring $7 days of IV therapy.136
because of lower complication rates,PICCs inserted in lower extremityvessels were recommended.136
CVAD (tunneled and nontunneled)use was reported in this population;however, placement $7 days wasassociated with an increased risk ofCLABSI.31,56 None of the includedstudies or guidelines includedevidence to support the use of totallyimplantable venous devices in thispopulation.
Regarding specific use in neonateswith univentricular physiology,umbilical catheters had low rates ofCLABSI, thrombosis, and occlusionwhen compared to other devices,15
and they can be used whenpreventing significant vessel loss forfuture procedures is a prioirity.Although PICCs were generallyrecommended in congenital cardiacpopulations, clinical guidelinesemphasized the need for specialistconsultation for patients with cardiacmalformations.136 Femoralnontunneled CVADs were reported asappropriate for therapies lasting,14 days in single-ventriclepopulations, with $14-day durations
associated with a higher risk ofthrombosis but not occlusion.15
Comparatively, other femoral devices(tunneled, uncuffed) were not relatedto an increased risk of thrombosisor occlusion for therapies lasting$14 days.15
Long-term Vascular Access Dependent
Long-term vascular accessdependency encompassednonmalignant hematologic,respiratory, gastrointestinal,metabolic, and immunologicconditions requiring long-term (.2months) and very long-term (.1year) VAD placement.29 In total, 4studies and 9 CPGs describedthis diverse patient populationacross PN and non-PN therapiesand continuous or intermittenttherapies. Despite the heterogeneityof reported populations, vesselpreservation and complicationprevention were the commonthemes when comparingPICC, short- and long-catheterPIVC, midline, tunneled-cuffed CVAD, and totallyimplantable venous deviceindications.16,32,90,109
Long-term PN Infusates
CLABSI, occlusion, and thrombosiswere common complications of long-term PN therapy across all VADs.16,32
Peripheral devices (PIVCs andmidlines) are unsafe for delivering PNbecause of the risk of venousdamage50,62,66; however, they may beindicated for limited time periodsin hospitalized patients withrestricted dextrose and proteinconcentrations (,10% and/or 5%,respectively).66,76,107 One single-center observational study supportedPICCs for long-term PN,32 andanother CPG recommended PICCs forhome PN107; although totallyimplantable venous devices weregenerally preferred when PN wasrequired for long durations, despitebeing associated with an increasedrisk of infection.16,29,32,50,56,92
Long-term Non-PN Infusates
Evidence for the use of VADsin patients requiring long-termnon-PN infusates was similar.Specifically, except for in oneCPG, all peripheral devices(PIVCs and midlines) wereregarded as inappropriate for long-term–dependent non-PN therapies,especially in patients with chronicrenal failure.56,62,66,76,109 TunneledCVADs and totally implantablevenous devices were insteadpreferred for non-PN therapiesrequired for continuous orintermittent and extended durations,respectively.56,62,66,76,103,109
Difficult Venous Access
For pediatric patients with difficultvenous access, insertion success ratesand the number of attempts arepriority considerations for VADselection. Factors that affect theseinclude patient physiology, pathology,damage caused by VAD, and theprocedural skill of the clinician.144
Five observational studies wereincluded for patients with difficultvenous access in ED (n = 2), electivesurgery (n = 1), PICU (n = 1), andhospitalized children (n = 1)populations. The majority of studiescompared nontunneled CVADs (n = 3)and evaluated the insertion successrates and complications associatedwith the number of insertionattempts. Two studies evaluatedPIVCs with and without ultrasound-guided (USG) techniques in pediatricpopulations.123,130
In patients with difficult vascularaccess, USG PIVC insertion wasassociated with higher overall andfirst- and second-attempt successrates after failed insertion via thelandmark method.130 Up to 17.2% ofCVADs in an ED setting experienceda complication (arterial puncture,hematoma, pneumothorax, andarrhythmia), and $3 attempts weresignificantly related to complicationdevelopment.140 In a studycomparing insertion success in
PEDIATRICS Volume 145, number s3, June 2020 S257 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

neonates and nonneonates,nontunneled CVAD failure wascommon (63.1%–76.3%), and thesuccess rate after .1 attempts wassignificantly lower with decreasingpatient age and associated withgreater insertion-relatedcomplications.55 Similarly,nontunneled CVAD placement inPICU patients led to high earlymechanical complications (17.5%)and was associated with moreinsertion attempts and insertionusing the subclavian or jugularapproach.113
Recommendations Regarding DeviceCharacteristics
Catheter-to-Vein Ratio
Determining the appropriatecatheter-to-vein ratio is a difficultbalancing act of optimizing patientand therapy needs while ensuringrisk of catheter-related complications,such as occlusion, is minimized.Although catheter-to-vein ratio wasrecognized as important forpreventing phlebitis, occlusion, andthrombosis,56 few studies reportedon catheter-to-vein ratios in neonateand pediatric patients. Only oneobservational study reported onPICCs in hospitalized children91;therefore the included studies werebroadened to incorporate an adultand laboratory study.95,118 Anadditional 6 CPGs were referred to forguidance.34,50,56,66,82,136
Clinical guidelines emphasizedselecting the smallest practical sizedgauge or French (F) that mettreatment and patientneed.34,56,66,95,136 Inadequatecatheter-to-vein ratio was linked toan increased risk of thrombosis in 2studies, especially in infants withcongenital heart disease, and smallercatheter size was associated withhigher rates of occlusion.50,56 Incontrast, larger catheters hada corresponding increase in rates ofphlebitis.66 For any VAD (PICC, PIVC,midline, CVAD, or totally implantablevenous device) a catheter-to-vein
ratio of ,50% in pediatric patientsand,33% in neonates was generallyrecommended.56,66,136 Specific toPICCs, thrombosis risk increasedwith a catheter-to-vein ratio $0.3391
and $0.45,118 in hospitalizedchildren and adults, respectively.Depending on the patient vessel size,22- to 24-gauge peripheral catheterswere considered appropriate forboth pediatric patients andneonates.66,76 According to thePeripherally Inserted CentralCatheters: Guideline for Practice fromthe National Association of NeonatalNurses, 1.1F to 3F catheters (20–28gauge) were commonly usedcatheter sizes for neonates.136
There were no specificrecommendations or empiricalevidence for the size of CVADs(tunneled or nontunneled), midlinecatheters, or totally implantablevenous devices.
Device Lumens
Choosing the optimum number ofdevice lumens to deliver plannedtherapy while reducing the risk ofcatheter-associated complications,particularly infection, occlusion, andthrombosis, is both complex andimportant.34 Nine studies describedlumen number outcomes inhospitalized adult (n = 2), children(n = 2) and infant (n = 1), immune-competent (n = 1), and hematologyand oncology (n = 3) populations. Anadditional 11 CPG recommendationswere included in the review. Allcompared single- versus double- ormultilumen catheters in CVADs (n =3), tunneled-cuffed CVADs (n = 2),and PICCs (n = 4).
Universally, CPGs recommended theminimum number of lumensnecessary for therapy provision.Because of increased risk of infection,occlusion, and thrombosis,multilumen VADs are onlyappropriate when indicated (ie, forhematopoietic stem cell transplant,critically ill patients, and patientsrequiring concurrent infusion of
noncompatible infusates such asblood and blood product, PN, orchemotherapy).* A dedicated lumenfor PN was also frequentlyendorsed,34,50,86,107 but authors of 2CPGs stated there was insufficientevidence to support thisrecommendation.56,96 Similarly,a dedicated lumen for bloodsampling, through the largest lumen,was recommended by some, but withlimited evidence.66,76
Evidence evaluating multilumen PICCoutcomes was mixed. One studyfound DVT risk increased with $2lumens,67 another study reporteda nonsignificant reduction in CLABSIrisk with single-lumen use,39 whilea number of other studies reportedthat PICC lumen number was notsignificantly associated with the riskof thrombosis81,122 or infection.81
Overall, most studies found occlusionwas the most common complicationassociated with catheter lumennumber, and $2 lumen PICCs wereassociated with the highest risk ofocclusion.28,39,81 Similarly, studiesreported mixed outcomes on thebasis of CVAD lumen number. Twostudies reported no associationbetween single- and double-lumencatheters and rates of infection65 andmajor CVAD-related complications,26
whereas others reported higher ratesof CLABSI,46,106 exit-site or tunnelinfection,46 malfunction orocclusion,46 and complicationsrequiring repositioning26 for double-lumen CVADs.
Recommendations for Insertion
Insertion Locations
Optimal catheter site selection inpediatric patients is more complexthan in adults as pediatric patientstypically have fewer accessible veinsdue to their smaller size.56,124
Determining the appropriateinsertion site is important forminimizing risk of insertion andpreventing post-insertion related
* Refs 34, 50, 51, 56, 62, 66, 76, 86, 107, and 124.
S258 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

complications19,56,75,86,124; however,only partial evidence for appropriatevessels and insertion locations forVADs was available. A total of 21studies and 12 CPGs were includeddescribing insertion locationoutcomes. Overall, most studies (n =15) compared CVADs in cardiac,neurology, and general surgical (n =5), PICU (n = 4), hospitalized infant(n = 1), oncology (n = 1), and stem cellcollection (n = 1) populations. Fivestudies compared PIVC devicelocation in surgical (n = 3),hospitalized children (n = 1), andneonate and infant(n = 1) populations, and 3 studiesevaluated PICC device location inoncology (n = 1), hospitalizedchildren (n = 1), andimmunocompetent (n = 1)populations.
According to the guidelines reviewed,common insertion sites varied bydevice type. PIVC insertion wasfrequently recommended in the handand upper extremities,66,76 withthe scalp and foot suggested asalternative insertion sites for infantsand toddlers.66 The Infusion TherapyStandards of Practice66 andProvisional Infusion TherapyStandards of Practice76 guidelinesrecommended avoidance of areas offlexion including the wrist. Insertionof PICCs via the basilic vein was thepreferred insertion site, although thebrachial, cephalic, axillary, temporal,and posterior auricular veins wereacceptable alternatives.56,62,66,76,107
For neonates, the best available veinwas recommended without specificguidance as to what constituted thebest vein.66 Infants could also havePICCs inserted at saphenous andpopliteal veins.56,66,76 Similarly, formidline catheter insertion, the basilic,brachial, and cephalic veins weresuggested for neonates, infants, andpediatric patients,76,96 as well asalternative insertion sites such as thescalp and leg.66,76 For PIVCs, theexternal jugular vein wasrecommended only in emergency
settings or if no other vein wasavailable.66 Overall, there were nopreferred insertion sites for tunneledand nontunneled CVADs or totallyimplantable vascular devices inneonates, infants, and pediatricpatients.66,76,82,117,120 No studiesevaluated the insertion locations fortunneled and nontunneled CVADs inchildren; however, in adults, tunneledand nontunneled CVADs werecommonly inserted into the internaland external jugular, subclavian, orfemoral vein, although the subclavianvein was the recommended insertionsite.56,62,76,107
Insertion Success Is Dependent onVessel and Insertion Site
PIVCs had higher success rates wheninserted in the cephalic vein in theproximal forearm under USGtechniques or the antecubitalfossa109,123 and a longer life spanwhen inserted into the arm comparedto scalp, hand, or leg insertion sites.33
CVAD insertion via the axillary veinusing USG techniques resulted infewer insertion attempts andsignificantly shorter time to guide-wire insertion and time tocannulation.78 Similarly, CVADinsertion in the subclavian vein wasassociated with shorter medianpuncture time, less insertionattempts, and significantly less guide-wire misplacement compared toinsertion via the infraclavicularapproach.41 In one study, there washigher overall insertion success forinsertion via the subclavian comparedto the internal jugular vein whenusing the landmark technique.42 Ina sample of critically ill newborns andchildren (0–14 years), USGbrachiocephalic insertion hadsignificantly higher first-attemptsuccess, fewer insertion attempts, anda shorter procedure time comparedto the internal jugular vein.98 Incritically ill neonates and infants,image-guided placement of tunneledCVADs via saphenous or femoralveins using a surgical cutdown was
associated with high placementsuccess.63
Complications Are Associated WithVessel and Insertion Site
In pediatric patients, PIVCs insertedat the bend of the arm or lowerextremities were associated withincreased risk of infiltration,erythema, pain, inability toadminister medications, no or poorflow due to gravity, and kinkedcatheter,125,127 whereas insertion atthe foot, ankle, or scalp wassignificantly associated withincreased risk of occlusion.125,127 Inneonates and infants, PICC insertionat foot or ankle sites was significantlyassociated with an increasedrisk of phlebitis, thrombosis, anddysfunction.47,125,136 Overall, therewas no direct association betweenPICC insertion at brachial, cephalic,or saphenous insertion sites andthrombosis in pediatric patients122;however, left-sided PICC insertionwas associated with higher rates ofPICC-related complications.37 Themajority of studies, with 2exceptions,18,78 found that rates ofinfection and complication variedsignificantly on the basis of CVADinsertion sites.† Generally,complications were similar betweeninternal jugular and subclavianveins.42 One study, however, reportedhigher rates of early mechanicalcomplications in nontunneled CVADsinserted through the subclaviancompared to the jugular or femoralvein.113
Across CVAD types, insertion via theinternal jugular in infants andpediatric patients was associatedwith increased risk of high arterialpuncture,42,113 postoperativechylothorax,36 thrombosis,67,69,89 andinfection.42,69 Insertion through thesubclavian vein was correlated withan increased risk of high arterialpuncture (left-side approaches),42,113
arrhythmias and misplacement
† Refs 31, 36, 42, 49, 67, 69, 85, 89, 113, and 132.
PEDIATRICS Volume 145, number s3, June 2020 S259 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

(right-side approaches),113
malposition and occlusion,42
postoperative chylothorax,36 andsepsis.31 In pediatric oncologypatients, subclavian insertion siteshad higher rates of thrombosiscompared to external jugular andcephalic sites, but there was nodifference in rates between right- orleft-side insertion sites.132
Comparatively, brachiocephalicinsertion sites were associated withsignificantly lower CLABSI andthrombosis compared to jugular andsubclavian approaches.69 Overall,CVAD insertion through the femoralvein was linked to higher risk ofthrombosis51,67,89 but lowercomplication and infection rates ininfants ,5 kg.85
Vessel Visualization
Vessel and catheter-tip visualizationtechnologies, including ultrasoundguidance, transillumination, near-infrared (NIR) light device guidance,fluoroscopy, and electrocardiogram(ECG), are commonly used inpediatric clinical practice.34,82 Despitethe variety of available technologies,all vessel visualization technologiesaim to minimize complications andincrease success rates duringcannulation. Overall, 31 studiesdescribing vessel visualizationoutcomes for PIVC, midline, PICC,CVAD, and totally implantable venousdevices and 15 CPGs were included.Among those, 17 studies werefocused on VADs in critically illchildren, neonate, and infant (n = 4);hospitalized children (n = 3); cardiac,neurologic, and general surgical (n =3); mixed cardiac surgical, congenitalheart disease, and PICU (n = 1); ED(n = 1); and neonate (n = 1)populations. Across theseheterogeneous populations, the focuswas on increasing first-attemptsuccess rates and overall successfulinsertion and correct catheter-tippositioning.
Across all CPGs, USG insertion bytrained clinicians was recommended
for all pediatric populations, devicetypes, and insertion sites.‡ It wasindicated in most of the evidencereviewed that USG insertions wereassociated with high insertionsuccess, first-attempt success rates,lower procedure time, fewerattempts, and fewer complications inPIVCs and CVADs.x Only 2 systematicreviews reported no difference inCVAD insertion success rates betweenultrasound guidance and landmarktechniques.121,135 PIVC insertion wasfrequently improved by use of vesselvisualization devices,101,123,130 withfewer complications noted.101 Fewstudies compared visualizationtechniques for totally implantablevenous device placement. One studyreported USG percutaneous punctureof totally implantable venous deviceshad similar success rates, proceduretimes, and complication rates whencompared to surgical cutdownmethods.48 Another study found thatinsertion of totally implantablevenous devices by using ultrasoundguidance was significantly moreeffective in reducing complicationrates, had shorter procedure times,and was more cost-efficient comparedto open surgical cutdowntechniques.71
However, recommendations for othervisualization techniques in pediatricpopulations, including NIR light(vessel visualization) and ECG(catheter-tip confirmation) deviceuse, were scant. Use of NIR lightdevices may be efficacious in selectedhigh-risk subpopulations102 and maymodestly improve first-attemptsuccess rates77,104,110; however, thecurrent evidence does not support anoverall benefit74 or a benefit that isbetter than non–image-guidedmethods.104 Similarly, lowlevels of evidence prevent therecommendation of ECG assistancefor PICC placement105; however, one
study also found higher first-attemptsuccess and correct tip positionsuccess by using intracavitary ECGPICC insertion compared to landmarktechniques.141 Other techniques, suchas ECG techniques, for CVADplacement were reported assuccessful and accurate.27,116 Inparticular, the ECG technique wassignificantly more accurate and wasassociated with fewer complicationswhen compared to landmarktechniques27 and when intracavitaryECG was undertaken by usinga dedicated ECG monitor.116 Anarticle discussed vessel visualizationtechniques for umbilical cathetersand recommended plain radiographsfor confirming catheter course andlocation.142
DISCUSSION
VAD selection and insertion groundedin evidence-based, standardizeddecision-making can reduce risk ofcomplications, pain, length of hospitalstay, and costs and can improveoverall safety and treatmentefficacy.1–6 Despite many individualstudies, systematic reviews, andtargeted CPGs, there is no evidence-based guide to assist clinical decision-making in common pediatricindications. This systematic review isthe first of its kind to evaluate theevidence that informs VAD selectionand insertion for common pediatricindications by using rigorousmethodology and a wide breadth ofscope. Overall, our reviewsynthesized the available high-qualityevidence to inform clinical decision-making, while also highlightingpractices in need of further inquiry.
This systematic review revealedevidence- and guideline-basedrecommendations for VAD selectionand insertion in numerous pediatricpopulations.56,66,76,136 There wasa large quantity of evidence tosupport VAD selection and insertiondecision-making in generalhospitalized pediatric patients and
‡ Refs 34, 38, 50, 56, 62, 66, 75, 76, 82, 96, 107, 108,117, 126, and 136.x Refs 17, 26, 52, 53, 61, 63, 64, 68, 78, 83, 99, 114,129, and 139.
S260 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

specialized populations, such asmalignant hematologic andoncological and critically ill pediatricpatients. Use of most VADs and theirassociated complications, especiallyfor PICCs, was well evidenced withinthese population groups. Evidence tosupport the use of single-lumendevices unless otherwise indicated(eg, for PN) was broadly supportedwithin the literature and in CPGs.‖
Similarly, evidence to suggest thatVAD insertion assisted by USGtechniques reduced complicationsand improved insertion success wasrepeatedly reported by high-qualitystudies and recommended acrossmultiple CPGs.{ The strength of theevidence for device selection andinsertion in these populationstherefore facilitates theimplementation of quality clinicaldecision-making.
On the other hand, our reviewhighlighted gaps in evidence,especially in the form of RCTs, forsome pediatric populations, devices,and indications. In some pediatricpopulations, evidence was so sparsethat the scope of the review had to bebroadened to include adult andlaboratory studies. Specificpopulations, such as neonates, cardiacpatients, and patients with difficultvenous access, relied on a fewobservational studies, makingrecommendations on device selectionchallenging. Similarly, although therewas a significant proportion of qualityevidence on VADs in patientsdependent on long-term PN, therewas limited evidence for other long-term VAD-dependent populations (eg,cystic fibrosis). Universally, there wasa dearth of evidence evaluatingmidline catheters for the majority ofpediatric indications. The literaturefor recommendations regardingoptimal catheter-to-vein ratio was
also limited; therefore, this reviewhad to be broadened to include adultand laboratory studies. Finally,although there was abundantevidence to support use of USGtechniques for the majority of deviceinsertions, there was a shortage ofevidence for the use of othertechnologies, particularly NIR lightdevices. As such, additional high-quality research evaluating thesepopulations, device typesand characteristics, and insertionprocedures iswarranted.
Although this study undertooka systematic and rigorous review ofthe available literature, the resultsshould be interpreted with cautionand in the context of its limitations.First, we did not undertake formalassessment of the quality of evidence(eg, using the Grading ofRecommendations Assessment,Development and Evaluation[GRADE] approach); however, allindividual included studies wereindependently assessed by 2 reviewauthors, and their quality indicatedby their study methodology, inaccordance with the RAND-UCLAmethodology.9 Additionally, althoughthis study prioritized the review ofRCTs and systematic reviews as thegold standard for evaluating VADs,this level of evidence was rarelyavailable. In accordance with theRAND-UCLA AppropriatenessMethod, the purpose of this reviewwas to include the best availableevidence to provide a synthesis ofinformation to guide panel decision-making.9 To avoid indications forwhich there was no evidence, weincluded evidence from lower-qualitystudies (eg, cross-sectional studies,surveillance studies, consecutivecases) and studies outside the initialscope of this review (NICU, adult, andlaboratory studies). The inclusion ofthese studies for some indicationsmeans that future clinical decision-making in certain pediatricpopulations is not guided by strong,
evidence-based recommendations.However, most of the evidence thatwas broadened beyond the originalscope of the systematic review waswell supported by CPGs, suggestingthat these findings can beimplemented into clinical practicewith confidence.
CONCLUSIONS
In this systematic review, we providethe first synthesis of the breadth ofevidence available for the selectionand insertion of VADs in pediatricpatients to guide clinical decision-making. There was strong evidenceto support and facilitate appropriateclinical decision-making in somepediatric indications. However,certain populations, device typesand characteristics, and insertionprocedures were poorly evidenced,necessitating the application of clinicaljudgment for some indications.Overall, the findings of this review willbe vital to inform criteria using theRAND-UCLA Appropriateness Methodto determine the appropriateness ofVADs in pediatric patients.
ABBREVIATIONS
CPG: clinical practice guidelineCVAD: central venous access
deviceDVT: deep vein thrombosisECG: electrocardiogramED: emergency departmentIV: intravenousMeSH: Medical Subject HeadingsNIR: near-infraredPICC: peripherally inserted central
catheterPIVC: peripheral intravenous
catheterPN: parenteral nutritionRAND-UCLA: RAND Corporation–
University ofCalifornia, LosAngeles
RCT: randomized control trialUSG: ultrasound-guidedVAD: vascular access device
‖ Refs 26, 28, 34, 39, 46, 50, 56, 62, 66, 76, 81, 86,106, 107, and 124.{ Refs 17, 26, 34, 38, 50, 52, 53, 56, 61, 62, 64, 66,68, 75, 76, 78, 82, 83, 96, 99, 107, 108, 114, 117, 126,129, 136, and 139.
PEDIATRICS Volume 145, number s3, June 2020 S261 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

Dr Paterson assisted with data extraction and synthesis and drafted the initial manuscript; Dr Brown conducted data collection, article screening, and initial data
extraction and synthesis; Dr Chopra, Ms Kleidon, Prof Cooke, Prof Rickard, and Dr Bernstein assisted with the conception and design of the study; Dr Ullman
conceptualized and designed the study and conducted article screening and data extraction and synthesis; and all authors reviewed and revised the manuscript,
approved the final manuscript as submitted, and agree to be accountable for all aspects of the work.
DOI: https://doi.org/10.1542/peds.2019-3474H
Accepted for publication Jan 21, 2020
Address correspondence to Amanda J. Ullman, RN, PhD, School of Nursing and Midwifery, Menzies Health Institute Queensland, Griffith University, Kessels Rd,
Nathan, QLD 4111, Australia. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2020 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Dr Paterson reports employment from Griffith University and The University of Queensland. Dr Chopra reports grants from the Agency for
Healthcare Research and Quality, American Hospital Association; book royalties from Oxford University Publishing for The Saint-Chopra Guide to Inpatient Medicine;
and honoraria for invited external talks as visiting professor. Dr Brown reports employment from Griffith University. Ms Kleidon reports employment by Queensland
Health; grants from the Children’s Hospital Foundation, the National Health and Medical Research Council (NHMRC), and Emergency Medicine Foundation; and
investigator-initiated research grants and speaker fees provided to Griffith University from 3M Medical; AngioDynamics; Baxter; BD-Bard; Centurion Medical
Products; Cook Medical; Medical Specialties Australasia, Smiths Medical; and Vygon (unrelated to the current project). Prof Cooke reports employment from Griffith
University and grants from Griffith University, the Children’s Hospital Foundation, Royal Brisbane and Women’s Hospital Foundation, Cancer Council Queensland,
Australasian College for Infection Prevention and Control, and investigator-initiated research grants and speaker fees provided to Griffith University by vascular
access product manufacturers (Baxter, BD, Entrotech Life Sciences) unrelated to this project. Prof Rickard reports a fellowship from Queensland Health;
employment from Griffith University; and grants from NHMRC, Griffith University, the Children’s Hospital Foundation, Princess Alexandra Hospital Foundation, Royal
Brisbane and Women’s Hospital Foundation, American Society for Parenteral and Enteral Nutrition Rhoads Foundation, Cancer Council Queensland, Australasian
College for Infection Prevention and Control, Association for Vascular Access Foundation, Australian College of Nursing, Australian College of Critical Care Nurses,
and Emergency Medicine Foundation; and investigator-initiated research grants and speaker fees provided to Griffith University by vascular access product
manufacturers (3M Medical, AngioDynamics, Baxter, B. Braun Medical, BD-Bard, Medtronic, ResQDevices, Smiths Medical) unrelated to this project. Dr Bernstein
reports grants from the Agency for Healthcare Research and Quality and US Department of Veterans Affairs. Dr Ullman reports fellowships and grants from the
NHMRC; employment from Griffith University; grants by the Children’s Hospital Foundation, Royal Brisbane and Women’s Hospital Foundation, Emergency Medicine
Foundation, and Australian College of Critical Care Nurses; and investigator-initiated research grants and speaker fees provided to Griffith University from 3M
Medical, AngioDynamics, and BD (unrelated to the current project). Dr Ullman also reports investigator-initiated research grants and speaker fees provided to
Griffith University from vascular access product manufacturers (3M Medical, AngioDynamics, BD, Cardinal Health) unrelated to the current project.
FUNDING: Supported by grants from the Association for Vascular Access Foundation, Griffith University, and the University of Michigan.
POTENTIAL CONFLICT OF INTEREST: Dr Chopra reports grants from the Agency for Healthcare Research and Quality, American Hospital Association; book royalties
from Oxford University Publishing for The Saint-Chopra Guide to Inpatient Medicine; and honoraria for invited external talks as visiting professor. Ms Kleidon
reports investigator-initiated research grants and speaker fees provided to Griffith University from 3M Medical; AngioDynamics; Baxter; BD-Bard; Centurion Medical;
Cook Medical; Medical Specialties Australasia; and Vygon (unrelated to the current project). Prof Cooke reports investigator-initiated research grants and speaker
fees provided to Griffith University by vascular access product manufacturers (Baxter, BD, Entrotech Life Sciences) unrelated to this project. Prof Rickard reports
investigator-initiated research grants and speaker fees provided to Griffith University from vascular access product manufacturers (3M Medical; AngioDynamics;
Baxter; B. Braun; BD-Bard; Medtronic; ResQDevices; Smiths Medical) unrelated to this project. Dr Bernstein reports grants from the Agency for Healthcare Research
and Quality and the US Department of Veterans Affairs. Dr Ullman reports investigator-initiated research grants and speaker fees provided to Griffith University
from vascular access product manufacturers (3M Medical, AngioDynamics, and BD) unrelated to the current project. Drs Paterson and Brown have indicated they
have no potential conflicts of interest to disclose.
REFERENCES
1. Ullman AJ, Cooke M, Kleidon T, RickardCM. Road map for improvement:point prevalence audit and surveyof central venous access devicesin paediatric acute care.J Paediatr Child Health. 2017;53(2):123–130
2. Noailly Charny PA, Bleyzac N,Ohannessian R, Aubert E, Bertrand Y,Renard C. Increased risk ofthrombosis associated with
peripherally inserted centralcatheters compared with conventionalcentral venous catheters in childrenwith leukemia. J Pediatr. 2018;198:46–52
3. LaRusso K, Schaack G, Fung T, et al.Should you pick the PICC? Prolongeduse of peripherally inserted centralvenous catheters in children withintestinal failure. J Pediatr Surg. 2019;54(5):999–1004
4. Gibson C, Connolly BL, Moineddin R,Mahant S, Filipescu D, Amaral JG.Peripherally inserted centralcatheters: use at a tertiary carepediatric center. J Vasc Interv Radiol.2013;24(9):1323–1331
5. Noonan PJ, Hanson SJ, Simpson PM,Dasgupta M, Petersen TL. Comparisonof complication rates of centralvenous catheters versus peripherallyinserted central venous catheters in
S262 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

pediatric patients. Pediatr Crit CareMed. 2018;19(12):1097–1105
6. Ullman AJ, Marsh N, Mihala G, CookeM, Rickard CM. Complications ofcentral venous access devices:a systematic review. Pediatrics. 2015;136(5). Available at: www.pediatrics.org/cgi/content/full/136/5/e1331
7. Ullman AJ, Chopra V, Brown E, et al.Developing appropriateness criteriafor pediatric vascular access.Pediatrics. 2020;145(suppl 3):e20193474G
8. Ullman AJ, Bernstein SJ, Brown E, et al.The Michigan Appropriateness Guidefor Intravenous Catheters inPediatrics: miniMAGIC. Pediatrics.2020;145(suppl 3):e20193474I
9. Fitch K, Bernstein SJ, Aguilar MD, et al.The RAND/UCLA AppropriatenessMethod User’s Manual. Santa Monica,CA: RAND Corporation; 2001
10. Brown E, Ullman A. Which vascularaccess devices are most likely topromote function and least likely tocause harm and under whichcircumstances in paediatrics?PROSPERO 2019 CRD42019094286.Available at: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=94286. Accessed April 27,2020
11. Moher D, Liberati A, Tetzlaff J, AltmanDG; PRISMA Group. Preferred reportingitems for systematic reviews and meta-analyses: the PRISMA statement. BMJ.2009;339:b2535
12. von Elm E, Altman DG, Egger M, PocockSJ, Gøtzsche PC, Vandenbroucke JP;STROBE Initiative. Strengthening theReporting of Observational Studies inEpidemiology (STROBE) statement:guidelines for reporting observationalstudies. BMJ. 2007;335(7624):806–808
13. Critical Appraisal Skills Programme.2018. CASP (Cohort Study) Checklist.[Online]. Available at: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Cohort-Study-Checklist_2018.pdf.Accessed June 1, 2018
14. Adams DZ, Little A, Vinsant C,Khandelwal S. The midline catheter:a clinical review. J Emerg Med. 2016;51(3):252–258
15. Aiyagari R, Song JY, Donohue JE, Yu S,Gaies MG. Central venous catheter-
associated complications in infantswith single ventricle: comparison ofumbilical and femoral venous accessroutes. Pediatr Crit Care Med. 2012;13(5):549–553
16. Ainsworth S, McGuire W. Percutaneouscentral venous catheters versusperipheral cannulae for delivery ofparenteral nutrition in neonates.Cochrane Database Syst Rev. 2015;(10):CD004219
17. Alten JA, Borasino S, Gurley WQ, LawMA, Toms R, Dabal RJ. Ultrasound-guided femoral vein catheterization inneonates with cardiac disease. PediatrCrit Care Med. 2012;13(6):654–659
18. Anil AB, Anil M, Kanar B, et al. Theevaluation of central venouscatheterization complications ina pediatric intensive care unit. TurkPediatri Ars. 2011;46:215–219
19. Australian and New Zealand IntensiveCare Society. Central Line Insertion andMaintenance Guideline. Melbourne,Australia: Australian and New ZealandIntensive Care Society Safety andQuality Committee; 2012
20. Allen RC, Holdsworth MT, Johnson CA,et al. Risk determinants for catheter-associated blood stream infections inchildren and young adults withcancer. Pediatr Blood Cancer. 2008;51(1):53–58
21. Australian Resuscitation Council; NewZealand Resuscitation Council.Advanced life support for infants andchildren diagnosis and management.ARC and NZRC Guideline 2010. EmergMed Australas. 2011;23(4):400–402
22. Australian Resuscitation Council; NewZealand Resuscitation Council.Medication or fluids for theresuscitation of the newborn infant.ARC and NZRC Guideline 2010. EmergMed Australas. 2011;23(4):442–444
23. Australian Resuscitation Council; NewZealand Resuscitation Council.Techniques in Paediatric Advanced LifeSupport. ARC and NZRC Guideline 2010.Emerg Med Australas. 2011;23(4):412–416
24. Arnts IJ, Bullens LM, Groenewoud JM,Liem KD. Comparison of complicationrates between umbilical andperipherally inserted central venous
catheters in newborns. J ObstetGynecol Neonatal Nurs. 2014;43:205–215
25. Athale UH, Siciliano S, Cheng J, ThabaneL, Chan AKC. Central venous linedysfunction is an independentpredictor of poor survival in childrenwith cancer. J Pediatr Hematol Oncol.2012;34(3):188–193
26. Avanzini S, Mameli L, Disma N, et al.Brachiocephalic vein for percutaneousultrasound-guided central linepositioning in children: a 20-monthpreliminary experience with 109procedures. Pediatr Blood Cancer. 2017;64(2):330–335
27. Barnwal NK, Dave ST, Dias R. Acomparative study of two techniques(electrocardiogram- and landmark-guided) for correct depth of the centralvenous catheter placement inpaediatric patients undergoing electivecardiovascular surgery. IndianJ Anaesth. 2016;60(7):470–475
28. Barrier A, Williams DJ, Connelly M,Creech CB. Frequency of peripherallyinserted central catheter complicationsin children. Pediatr Infect Dis J. 2012;31(5):519–521
29. Baskin KM, Mermel LA, Saad TF, et al;Venous Access: National Guideline andRegistry Development (VANGUARD)Initiative Affected Persons AdvisoryPanel. Evidence-based strategies andrecommendations for preservation ofcentral venous access in children. JPENJ Parenter Enteral Nutr. 2019;43(5):591–614
30. Ben Abdelaziz R, Hafsi H, Hajji H,et al. Peripheral venous cathetercomplications in children: predisposingfactors in a multicenter prospectivecohort study [published correctionappears in BMC Pediatr. 2018;18(1):307]. BMC Pediatr. 2017;17(1):208
31. Bezzio S, Scolfaro C, Broglia R, et al.Prospective incidence study ofbloodstream infection in infants andchildren with central venous cathetersafter cardiac surgery in Italy. InfectControl Hosp Epidemiol. 2009;30(7):698–701
32. Blotte C, Styers J, Zhu H,Channabasappa N, Piper HG. Acomparison of Broviac® andperipherally inserted central cathetersin children with intestinal failure.J Pediatr Surg. 2017;52(5):768–771
PEDIATRICS Volume 145, number s3, June 2020 S263 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

33. Birhane E, Kidanu K, Kassa M, et al.Lifespan and associated factors ofperipheral intravenous cannula amonginfants admitted in public hospitals ofMekelle city, Tigray, Ethiopia, 2016. BMCNurs. 2017;16:33
34. Bodenham Chair A, Babu S, Bennett J,et al. Association of Anaesthetists ofGreat Britain and Ireland: safe vascularaccess 2016 [published correctionappears in Anaesthesia. 2016;71(12):1503]. Anaesthesia. 2016;71(5):573–585
35. Boe BA, Zampi JD, Yu S, Donohue JE,Aiyagari R. Transhepatic central venouscatheters in pediatric patients withcongenital heart disease. Pediatr CritCare Med. 2015;16(8):726–732
36. Borasino S, Diaz F, El Masri K, Dabal RJ,Alten JA. Central venous lines are a riskfactor for chylothorax in infants aftercardiac surgery. World J PediatrCongenit Heart Surg. 2014;5(4):522–526
37. Borretta L, MacDonald T, Digout C,Smith N, Fernandez CV, Kulkarni K.Peripherally inserted central cathetersin pediatric oncology patients: a 15-yearpopulation-based review fromMaritimes, Canada. J Pediatr HematolOncol. 2018;40(1):e55–e60
38. Bouaziz H, Zetlaoui PJ, Pierre S, et al.Guidelines on the use of ultrasoundguidance for vascular access. AnaesthCrit Care Pain Med. 2015;34(1):65–69
39. Bozaan D, Skicki D, Brancaccio A,et al. Less lumens-less risk: a pilotintervention to increase the use ofsingle-lumen peripherally insertedcentral catheters. J Hosp Med. 2019;14(1):42–46
40. Bratton J, Johnstone PA, McMullen KP.Outpatient management of vascularaccess devices in children receivingradiotherapy: complications andmorbidity. Pediatr Blood Cancer. 2014;61(3):499–501
41. Byon HJ, Lee GW, Lee JH, et al.Comparison between ultrasound-guided supraclavicular andinfraclavicular approaches forsubclavian venous catheterization inchildren--a randomized trial. BrJ Anaesth. 2013;111(5):788–792
42. Camkiran Firat A, Zeyneloglu P, Ozkan M,Pirat A. A randomized controlledcomparison of the internal jugular veinand the subclavian vein as access sites
for central venous catheterization inpediatric cardiac surgery. Pediatr CritCare Med. 2016;17(9):e413–e419
43. Campagna S, Gonella S, Zerla PA, et al.The risk of adverse events related toextended-dwell peripheral intravenousaccess. Infect Control Hosp Epidemiol.2018;39(7):875–877
44. Carlson JN, Gannon E, Mann NC, et al.Pediatric out-of-hospital criticalprocedures in the United States.Pediatr Crit Care Med. 2015;16(8):e260–e267
45. Carraro F, Cicalese MP, Cesaro S, et al.Guidelines for the use of long-termcentral venous catheter in childrenwith hemato-oncological disorders. Onbehalf of Supportive Therapy WorkingGroup of Italian Association of PediatricHematology and Oncology (AIEOP). AnnHematol. 2013;92(10):1405–1412
46. Cesaro S, Cavaliere M, Pegoraro A,Gamba P, Zadra N, Tridello G. Acomprehensive approach to theprevention of central venous cathetercomplications: results of 10-yearprospective surveillance in pediatrichematology-oncology patients. AnnHematol. 2016;95(5):817–825
47. Chen H, Zhang X, Wang H, Hu X.Complications of upper extremityversus lower extremity placedperipherally inserted central cathetersin neonatal intensive care units:a meta-analysis. Intensive Crit CareNurs. 2020;56:102753
48. Choi JS, Park KM, Jung S, et al.Usefulness of percutaneous puncture ininsertion of totally implantable venousaccess devices in pediatric patients.Vasc Spec Int. 2017;33(3):108–111
49. Cooling L, Hoffmann S, Webb D, YamadaC, Davenport R, Choi SW. Performanceand safety of femoral central venouscatheters in pediatric autologousperipheral blood stem cell collection.J Clin Apher. 2017;32(6):501–516
50. Crocoli A, Tornesello A, Pittiruti M, et al.Central venous access devices inpediatric malignancies: a positionpaper of Italian Association of PediatricHematology and Oncology. J VascAccess. 2015;16(2):130–136
51. Debourdeau P, Kassab Chahmi D, Le GalG, et al; Working Group of the SOR;French National Feberation of Cancer
Centers. 2008 SOR guidelines for theprevention and treatment ofthrombosis associated with centralvenous catheters in patients withcancer: report from the Working Group.Ann Oncol. 2009;20(9):1459–1471
52. de Carvalho Onofre PS, da LuzGonçalves Pedreira M, Peterlini MAS.Placement of peripherally insertedcentral catheters in children guided byultrasound: a prospective randomized,and controlled trial. Pediatr Crit CareMed. 2012;13(5):e282–e287
53. de Souza TH, Brandão MB, Santos TM,Pereira RM, Nogueira RJN. Ultrasoundguidance for internal jugular veincannulation in PICU: a randomisedcontrolled trial. Arch Dis Child. 2018;103(10):952–956
54. DeWitt AG, Zampi JD, Donohue JE, Yu S,Lloyd TR. Fluoroscopy-guided umbilicalvenous catheter placement in infantswith congenital heart disease. CongenitHeart Dis. 2015;10(4):317–325
55. Dheer G, Chaudhry GK, Singh T.Immediate complications ofpercutaneous central venouscannulation in children. J Indian AssocPediatr Surg. 2011;16(4):145–147
56. Doellman D, Buckner JK, HudsonGarrett J Jr., Catudal JP, Frey AM,Lamagna P. Best Practice Guidelines inthe Care and Maintenance of PediatricCentral Venous Catheters, 2nd ed.Herriman, UT: Association for VascularAccess; 2015
57. Dongara AR, Patel DV, Nimbalkar SM,Potana N, Nimbalkar AS. Umbilicalvenous catheter versus peripherallyinserted central catheter in neonates:a randomized controlled trial. J TropPediatr. 2017;63(5):374–379
58. Elser HE. Options for securing umbilicalcatheters. Adv Neonatal Care. 2013;13(6):426–429
59. Fallon SC, Kim ME, Fernandes CJ,Vasudevan SA, Nuchtern JG, Kim ES.Identifying and reducing earlycomplications of surgical central linesin infants and toddlers. J Surg Res.2014;190(1):246–250
60. Faustino EV, Spinella PC, Li S, et al.Incidence and acute complications ofasymptomatic central venous catheter-related deep venous thrombosis in
S264 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

critically ill children. J Pediatr. 2013;162(2):387–391
61. Froehlich CD, Rigby MR, Rosenberg ES,et al. Ultrasound-guided central venouscatheter placement decreasescomplications and decreasesplacement attempts compared with thelandmark technique in patients ina pediatric intensive care unit. CritCare Med. 2009;37(3):1090–1096
62. Frykholm P, Pikwer A, Hammarskjöld F,et al; Swedish Society ofAnaesthesiology and Intensive CareMedicine. Clinical guidelines on centralvenous catheterisation. ActaAnaesthesiol Scand. 2014;58(5):508–524
63. Gaballah M, Krishnamurthy G, KellerMS, McIntosh A, Munson DA, Cahill AM.US-guided placement and tip positionconfirmation for lower-extremitycentral venous access in neonates andinfants with comparison versusconventional insertion. J Vasc IntervRadiol. 2014;25(4):548–555
64. Gallagher RA, Levy J, Vieira RL,Monuteaux MC, Stack AM. Ultrasoundassistance for central venous catheterplacement in a pediatric emergencydepartment improves placementsuccess rates. Acad Emerg Med. 2014;21(9):981–986
65. Gonzalez G, Davidoff AM, Howard SC,et al. Safety of central venous catheterplacement at diagnosis of acutelymphoblastic leukemia in children.Pediatr Blood Cancer. 2012;58(4):498–502
66. Gorski L, Hadaway L, Hagle M,McGoldrick M, Orr M, Doellman D.Infusion therapy standards of practice.J Infus Nurs. 2016;39:S1–S169
67. Gray BW, Gonzalez R, Warrier KS, et al.Characterization of central venouscatheter-associated deep venousthrombosis in infants. J Pediatr Surg.2012;47(6):1159–1166
68. Gurien LA, Blakely ML, Russell RT, et al;Pediatric Surgery Research (PedSRC)Collaborative. Real-timeultrasonography for placement ofcentral venous catheters in children:a multi-institutional study. Surgery.2016;160(6):1605–1611
69. Habas F, Baleine J, Milési C, et al.Supraclavicular catheterization of thebrachiocephalic vein: a way to prevent
or reduce catheter maintenance-related complications in children. EurJ Pediatr. 2018;177(3):451–459
70. Hamed RK, Hartmans S, Gausche-Hill M.Anesthesia through an intraosseousline using an 18-gauge intravenousneedle for emergency pediatricsurgery. J Clin Anesth. 2013;25(6):447–451
71. Hancock-Howard R, Connolly BL,McMahon M, et al. Cost-effectivenessanalysis of implantable venous accessdevice insertion using interventionalradiologic versus conventionaloperating room methods in pediatricpatients with cancer. J Vasc IntervRadiol. 2010;21(5):677–684
72. Handrup MM, Møller JK, Frydenberg M,Schrøder H. Placing of tunneled centralvenous catheters prior to inductionchemotherapy in children with acutelymphoblastic leukemia. Pediatr BloodCancer. 2010;55(2):309–313
73. Hanson SJ, Punzalan RC, ChristensenMA, Ghanayem NS, Kuhn EM, Havens PL.Incidence and risk factors for venousthromboembolism in critically illchildren with cardiac disease. PediatrCardiol. 2012;33(1):103–108
74. Heinrichs J, Fritze Z, Klassen T, Curtis S.A systematic review and meta-analysisof new interventions for peripheralintravenous cannulation of children.Pediatr Emerg Care. 2013;29(7):858–866
75. Institute for Healthcare Improvement.How-to Guide: Prevent Central Line-Associated Bloodstream Infection(CLABSI). Cambridge, MA: Institute forHealthcare Improvement; 2012
76. Intravenous Nursing New ZealandIncorporated Society. ProvisionalInfusion Therapy Standards of Practice.Auckland, New Zealand: IntravenousNursing New Zealand IncorporatedSociety; 2012
77. Katsogridakis YL, Seshadri R, Sullivan C,Waltzman ML. Veinlite transilluminationin the pediatric emergency department:a therapeutic interventional trial.Pediatr Emerg Care. 2008;24(2):83–88
78. Kim EH, Lee JH, Song IK, et al. Real-timeultrasound-guided axillary veincannulation in children: a randomisedcontrolled trial. Anaesthesia. 2017;72(12):1516–1522
79. Kulkarni S, Wu O, Kasthuri R, Moss JG.Centrally inserted external cathetersand totally implantable ports for thedelivery of chemotherapy: a systematicreview and meta-analysis of device-related complications. CardiovascIntervent Radiol. 2014;37(4):990–1008
80. Kulkarni R, Presley RJ, Lusher JM, et al.Complications of haemophilia in babies(first two years of life): a report fromthe Centers for Disease Control andPrevention Universal Data CollectionSystem. Haemophilia. 2017;23(2):207–214
81. Lam PW, Volling C, Chan T, et al. Impactof defaulting to single-lumenperipherally inserted central catheterson patient outcomes: an interruptedtime series study. Clin Infect Dis. 2018;67(6):954–957
82. Lamperti M, Bodenham AR, Pittiruti M,et al. International evidence-basedrecommendations on ultrasound-guided vascular access. Intensive CareMed. 2012;38(7):1105–1117
83. Lau CS, Chamberlain RS. Ultrasound-guided central venous catheterplacement increases success rates inpediatric patients: a meta-analysis.Pediatr Res. 2016;80(2):178–184
84. Levy I, Bendet M, Samra Z, Shalit I,Katz J. Infectious complications ofperipherally inserted central venouscatheters in children. Pediatr Infect DisJ. 2010;29(5):426–429
85. Lindquester WS, Hawkins CM, MonroeEJ, et al. Single-stick tunneledcentral venous access using thejugular veins in infants weighing lessthan 5 kg. Pediatr Radiol. 2017;47(12):1682–1687
86. Loveday HP, Wilson JA, Pratt RJ, et al; UKDepartment of Health. epic3: nationalevidence-based guidelines forpreventing healthcare-associatedinfections in NHS hospitals in England.J Hosp Infect. 2014;86(suppl 1):S1–S70
87. Malbezin S, Gauss T, Smith I, et al. Areview of 5434 percutaneous pediatriccentral venous catheters inserted byanesthesiologists. Paediatr Anaesth.2013;23(11):974–979
88. Marshall AM, Danford DA, Curzon CL,Anderson V, Delaney JW. Traditionallong-term central venous cathetersversus transhepatic venous catheters
PEDIATRICS Volume 145, number s3, June 2020 S265 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

in infants and young children. PediatrCrit Care Med. 2017;18(10):944–948
89. Marquez A, Shabanova V, Faustino EV;Northeast Pediatric Critical CareResearch Consortium. Prediction ofcatheter-associated thrombosis incritically ill children. Pediatr Crit CareMed. 2016;17(11):e521–e528
90. May TL, Gifford AH, Lahiri T, et al.Complications of long and intermediateterm venous catheters in cystic fibrosispatients: a multicenter study. J CystFibros. 2018;17(1):96–104
91. Menéndez JJ, Verdú C, Calderón B, et al.Incidence and risk factors of superficialand deep vein thrombosis associatedwith peripherally inserted centralcatheters in children. J ThrombHaemost. 2016;14(11):2158–2168
92. Mermel LA, Allon M, Bouza E, et al.Clinical practice guidelines for thediagnosis and management ofintravascular catheter-related infection:2009 update by the Infectious DiseasesSociety of America [publishedcorrection appears in Clin Infect Dis.2010;50(7):1079]. Clin Infect Dis. 2009;49(1):1–45
93. Moon HM, Kim S, Yun KW, et al. Clinicalcharacteristics and risk factors of long-term central venous catheter-associated bloodstream infections inchildren. Pediatr Infect Dis J. 2018;37(5):401–406
94. Mushtaq A, Navalkele B, Kaur M, et al.Comparison of complications inmidlines versus central venouscatheters: are midlines safer thancentral venous lines? Am J InfectControl. 2018;46(7):788–792
95. Nifong TP, McDevitt TJ. The effect ofcatheter to vein ratio on blood flowrates in a simulated model ofperipherally inserted central venouscatheters. Chest. 2011;140(1):48–53
96. O’Grady NP, Alexander M, Burns LA, et al;Healthcare Infection Control PracticesAdvisory Committee. Guidelines for theprevention of intravascular catheter-related infections. Am J Infect Control.2011;39(4 suppl 1):S1–S34
97. Ohno K, Nakaoka T, Takama Y, HigashioA, Santo K, Yoneda A. Implantablecentral venous access device in infants:long-term results. Pediatr Int. 2016;58(10):1027–1031
98. Oulego-Erroz I, Muñoz-Lozón A, Alonso-Quintela P, Rodríguez-Nuñez A.Comparison of ultrasound guidedbrachiocephalic and internal jugularvein cannulation in critically ill children.J Crit Care. 2016;35:133–137
99. Oulego-Erroz I, González-Cortes R,García-Soler P, et al; RECANVACollaborative Study. Ultrasound-guidedor landmark techniques for centralvenous catheter placement in criticallyill children. Intensive Care Med. 2018;44(1):61–72
100. Pacilli M, Bradshaw CJ, Clarke SA. Useof 8-cm 22G-long peripheral cannulas inpediatric patients. J Vasc Access. 2018;19(5):496–500
101. Paladini A, Chiaretti A, Sellasie KW,Pittiruti M, Vento G. Ultrasound-guidedplacement of long peripheral cannulasin children over the age of 10 yearsadmitted to the emergency department:a pilot study. BMJ Paediatr Open. 2018;2(1):e000244
102. Park JM, Kim MJ, Yim HW, Lee WC, JeongH, Kim NJ. Utility of near-infrared lightdevices for pediatric peripheralintravenous cannulation: a systematicreview and meta-analysis. Eur J Pediatr.2016;175(12):1975–1988
103. Pasteur MC, Bilton D, Hill AT; BritishThoracic Society Bronchiectasis non-CFGuideline Group. British ThoracicSociety guideline for non-CFbronchiectasis. Thorax. 2010;65(suppl1):i1–i58
104. Peterson KA, Phillips AL, Truemper E,Agrawal S. Does the use of an assistivedevice by nurses impact peripheralintravenous catheter insertion successin children? J Pediatr Nurs. 2012;27(2):134–143
105. Perin G, Scarpa MG. Defining centralvenous line position in children: tips forthe tip. J Vasc Access. 2015;16(2):77–86
106. Pinon M, Bezzio S, Tovo PA, et al. Aprospective 7-year survey on centralvenous catheter-related complicationsat a single pediatric hospital. EurJ Pediatr. 2009;168(12):1505–1512
107. Pittiruti M, Hamilton H, Biffi R, MacFie J,Pertkiewicz M; ESPEN. ESPEN Guidelineson Parenteral Nutrition: central venouscatheters (access, care, diagnosis andtherapy of complications). Clin Nutr.2009;28(4):365–377
108. Polkinghorne KR, Chin GK, MacGinley RJ,et al. KHA-CARI Guideline: vascularaccess - central venous catheters,arteriovenous fistulae andarteriovenous grafts [publishedcorrection appears in Nephrology(Carlton). 2014;19(1):64]. Nephrology(Carlton). 2013;18(11):701–705
109. Qian SY, Horn MT, Barnes R, ArmstrongD. The use of 8-cm 22G Seldingercatheters for intravenous access inchildren with cystic fibrosis. J VascAccess. 2014;15(5):415–417
110. Ramer L, Hunt P, Ortega E, Knowlton J,Briggs R, Hirokawa S. Effect ofintravenous (IV) assistive device(VeinViewer) on IV access attempts,procedural time, and patient and nursesatisfaction. J Pediatr Oncol Nurs. 2016;33(4):273–281
111. Rauth TP, Scott BP, Thomason CK,Bartilson RE, Hann TM, Pietsch JB.Central venous catheter placement atthe time of extracorporeal membraneoxygenation decannulation: is it safe?J Pediatr Surg. 2008;43(1):53–57;discussion 58
112. Revel-Vilk S, Yacobovich J, Tamary H,et al. Risk factors for central venouscatheter thrombotic complications inchildren and adolescents with cancer.Cancer. 2010;116(17):4197–4205
113. Rey C, Alvarez F, De La Rua V, et al.Mechanical complications duringcentral venous cannulations inpediatric patients. Intensive Care Med.2009;35(8):1438–1443
114. Rivera-Tocancipá D, Díaz-Sánchez E,Montalvo-Arce CA. Ultrasound versusanatomical landmarks: immediatecomplications in the central venouscatheterization in children under18 years of age. Rev Esp AnestesiolReanim. 2018;65(7):366–372
115. Rosado V, Camargos PA, Clemente WT,Romanelli RM. Incidence of infectiouscomplications associated with centralvenous catheters in pediatricpopulation. Am J Infect Control. 2013;41(9):e81–e84
116. Rossetti F, Pittiruti M, Lamperti M,Graziano U, Celentano D, Capozzoli G.The intracavitary ECG method forpositioning the tip of central venousaccess devices in pediatric patients:results of an Italian multicenter study.J Vasc Access. 2015;16(2):137–143
S266 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

117. Schiffer CA, Mangu PB, Wade JC, et al.Central venous catheter care for thepatient with cancer: American Societyof Clinical Oncology clinical practiceguideline. J Clin Oncol. 2013;31(10):1357–1370
118. Sharp R, Cummings M, Fielder A,Mikocka-Walus A, Grech C, Esterman A.The catheter to vein ratio andrates of symptomatic venousthromboembolism in patients witha peripherally inserted centralcatheter (PICC): a prospective cohortstudy. Int J Nurs Stud. 2015;52(3):677–685
119. Shenep MA, Tanner MR, Sun Y, et al.Catheter-related complications inchildren with cancer receivingparenteral nutrition: change in risk ismoderated by catheter type. JPENJ Parenter Enteral Nutr. 2017;41(6):1063–1071
120. Sibson KR, Biss TT, Furness CL, et al;British Society for Haematology. BSHGuideline: management of thromboticand haemostatic issues in paediatricmalignancy. Br J Haematol. 2018;180(4):511–525
121. Sigaut S, Skhiri A, Stany I, et al.Ultrasound guided internal jugular veinaccess in children and infant: a meta-analysis of published studies. PaediatrAnaesth. 2009;19(12):1199–1206
122. Smitherman AB, Alexander T, ConnellyM, et al. The incidence of catheter-associated venous thrombosis innoncritically ill children. Hosp Pediatr.2015;5(2):59–66
123. Takeshita J, Nakayama Y, Nakajima Y,et al. Optimal site for ultrasound-guidedvenous catheterisation in paediatricpatients: an observational study toinvestigate predictors forcatheterisation success anda randomised controlled study todetermine the most successful site. CritCare. 2015;19:15–23
124. The Joint Commission. Central line-associated bloodstream infectionstoolkit and monograph: preventingcentral line–associated bloodstreaminfections. With useful tools and aninternational perspective. 2013.Available at: www.jointcommission.org/CLABSIToolkit. Accessed June, 2018
125. Tripi PA, Thomas S, Clebone A,Goldfinger MM, Tobias JD. Peripheral
intravenous catheter problems ininfants and children presenting foranesthesia and surgery. Middle EastJ Anaesthesiol. 2016;23(4):411–414
126. Troianos CA, Hartman GS, Glas KE, et al;Councils on IntraoperativeEchocardiography and VascularUltrasound of the American Societyof Echocardiography. Guidelinesfor performing ultrasoundguided vascular cannulation:recommendations of the AmericanSociety of Echocardiography and theSociety of CardiovascularAnesthesiologists. J Am SocEchocardiogr. 2011;24(12):1291–1318
127. Unbeck M, Förberg U, Ygge BM,Ehrenberg A, Petzold M, Johansson E.Peripheral venous catheterrelated complications are commonamong paediatric and neonatalpatients. Acta Paediatr. 2015;104(6):566–574
128. van Gent MB, van der Made WJ,Marang-van de Mheen PJ, van der BogtKE. Contemporary insertion of centralvenous access catheters in pediatricpatients: a retrospective record reviewstudy of 538 catheters in a singlecenter. Surg Infect (Larchmt). 2017;18(2):105–111
129. Vierboom L, Darani A, Langusch C,Soundappan S, Karpelowsky J.Tunnelled central venous accessdevices in small children: a comparisonof open vs. ultrasound-guidedpercutaneous insertion in childrenweighing ten kilograms or less.J Pediatr Surg. 2018;53(9):1832–1838
130. Vinograd AM, Zorc JJ, Dean AJ,Abbadessa MKF, Chen AE. First-attempt success, longevity, andcomplication rates of ultrasound-guided peripheral intravenouscatheters in children. Pediatr EmergCare. 2018;34(6):376–380
131. Voigt J, Waltzman M, Lottenberg L.Intraosseous vascular access for in-hospital emergency use: a systematicclinical review of the literature andanalysis. Pediatr Emerg Care. 2012;28(2):185–199
132. Wiegering V, Schmid S, Andres O, et al.Thrombosis as a complication ofcentral venous access in pediatricpatients with malignancies: a 5-year
single-center experience. BMC Hematol.2014;14(1):18
133. White AD, Othman D, Dawrant MJ,Sohrabi S, Young AL, Squire R.Implantable versus cuffed externalcentral venous catheters for themanagement of children andadolescents with acute lymphoblasticleukaemia. Pediatr Surg Int. 2012;28(12):1195–1199
134. Wragg RC, Blundell S, Bader M, et al.Patency of neck veins followingultrasound-guided percutaneousHickman line insertion. Pediatr SurgInt. 2014;30(3):301–304
135. Wu SY, Ling Q, Cao LH, Wang J, Xu MX,Zeng WA. Real-time two-dimensionalultrasound guidance for centralvenous cannulation: a meta-analysis. Anesthesiology. 2013;118(2):361–375
136. Wyckoff MM, Sharpe EL. PeripherallyInserted Central Catheters: Guidelinefor Practice, 3rd ed. Chicago, IL:National Association of NeonatalNurses; 2015
137. Xia Y, Wu Y, Zhang W, et al. Applicationof peripherally inserted centralcatheter via femoral vein for pediatricburns. Int J Clin Exp Med. 2016;9:20105–20108
138. Yacobovich J, Ben-Ami T, Abdalla T,et al. Patient and central venouscatheter related risk factors forblood stream infections in childrenreceiving chemotherapy. PediatrBlood Cancer. 2015;62(3):471–476
139. Zanolla GR, Baldisserotto M, Piva J. Howuseful is ultrasound guidance for internaljugular venous access in children?J Pediatr Surg. 2018;53(4):789–793
140. Zengin Y, Içer M, Gündüz E, Dursun R,Durgun HM, Gülo�glu C. Assessment ofcentral venous catheters applied inpediatric patients at emergencydepartment. J Exp Clin Med (Turkey).2013;30:345–348
141. Zhou L, Xu H, Liang J, Xu M, Yu J.Effectiveness of intracavitaryelectrocardiogram guidance inperipherally inserted centralcatheter tip placement in neonates.J Perinat Neonatal Nurs. 2017;31(4):326–331
PEDIATRICS Volume 145, number s3, June 2020 S267 by guest on December 8, 2020www.aappublications.org/newsDownloaded from

142. Oestreich AE. Umbilical veincatheterization--appropriateand inappropriate placement.Pediatr Radiol. 2010;40(12):1941–1949
143. DeVries M, Lee J, Hoffman L. Infectionfree midline catheter implementation ata community hospital (2 years).Am J Infect Control. 2019;47(9):1118–1121
144. Kleidon TM, Cattanach P, Mihala G, UllmanAJ. Implementation of a paediatricperipheral intravenous catheter care bundle:a quality improvement initiative. J PaediatrChild Health. 2019;55(10):1214–1223
S268 PATERSON et al by guest on December 8, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2019-3474H2020;145;S243Pediatrics
Claire M. Rickard, Steven J. Bernstein and Amanda J. UllmanRebecca S. Paterson, Vineet Chopra, Erin Brown, Tricia M. Kleidon, Marie Cooke,
ReviewSelection and Insertion of Vascular Access Devices in Pediatrics: A Systematic
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/145/Supplement_3/S243including high resolution figures, can be found at:
References
#BIBLhttp://pediatrics.aappublications.org/content/145/Supplement_3/S243This article cites 133 articles, 6 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on December 8, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2019-3474H2020;145;S243Pediatrics
Claire M. Rickard, Steven J. Bernstein and Amanda J. UllmanRebecca S. Paterson, Vineet Chopra, Erin Brown, Tricia M. Kleidon, Marie Cooke,
ReviewSelection and Insertion of Vascular Access Devices in Pediatrics: A Systematic
http://pediatrics.aappublications.org/content/145/Supplement_3/S243located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2020has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on December 8, 2020www.aappublications.org/newsDownloaded from