Embed Size (px)
Citation preview

Screening for
Giant Cell Arteritis in the
Vascular LaboratoryMOLLY ZACCARDI MHA, RVT
D.E. STRANDNESS VASCULAR LABORATORY
UNIVERSITY OF WASHINGTON MEDICAL CENTER
1
2

Giant Cell Arteritis (GCA) is an inflammatory
vasculopathy affecting medium and large- sized
arteries.
Referred to as temporal arteritis – often affects branches
of the carotid artery.
Superficial temporal artery branch is particularly
susceptible to inflammation of the vessel wall.
TA is among the most common causes of acute
blindness due to inflammation and blockage of blood
vessels that supply the main nerve of the eyes
GCA/TA is a medical emergency
Blindness occurs in 1/5 of patients with GCA
3Giant Cell Arteritis

4

5Normal artery Giant cell arteritis
E. Jernberg
Demographics:
Elderly patients
Female > male
Northern European

Giant Cell Arteritis
GCA / TA is difficult to diagnose
10-20% False negative biopsies
skip lesions or
being treated with steroids
Delay of treatment >6 days can result in blindness
Treatment is corticosteroids-unpleasant side effects
6

Dr. Diamantopoulos’ question
Is there a better way to diagnose and follow up 7
Giant Cell Arteritis8
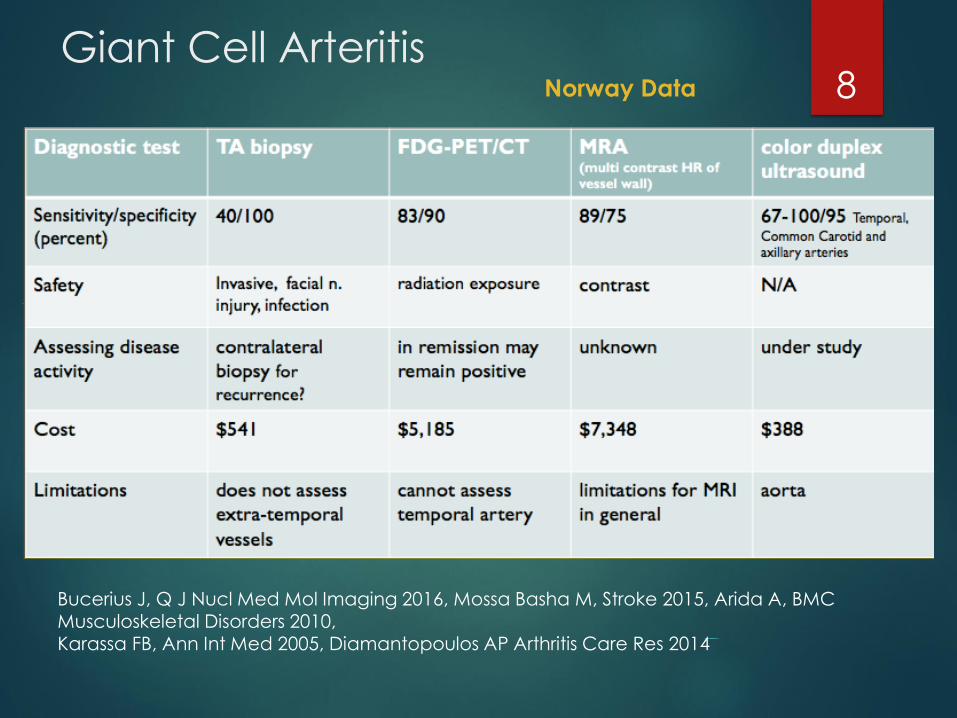
Bucerius J, Q J Nucl Med Mol Imaging 2016, Mossa Basha M, Stroke 2015, Arida A, BMC Musculoskeletal Disorders 2010,Karassa FB, Ann Int Med 2005, Diamantopoulos AP Arthritis Care Res 2014
Norway Data

Giant Cell Arteritis9

Giant Cell Arteritis10

Giant Cell Arteritis
DISADVANTAGES OF ULTRASOUND
Operator dependent- not universally reproducible
Imaging is dependent on transducer selection
Sensitivity and specificity reduces quickly after introduction of treatment (>4 days: US 50% and MRI 56% )
Hauenstein C, Rheumatology (Oxford) 2012

Giant Cell Arteritis12
Include IMT measurement
Add other susceptible vessels
Sensitivity Specificity
Temporal artery evaluation 96% 90%
Temporal
Axillary /subclavian arteries98% 91%
Temporal
Axillary /subclavian arteries
Carotid arteries
100% 95%

13Pathology
Temporal Artery
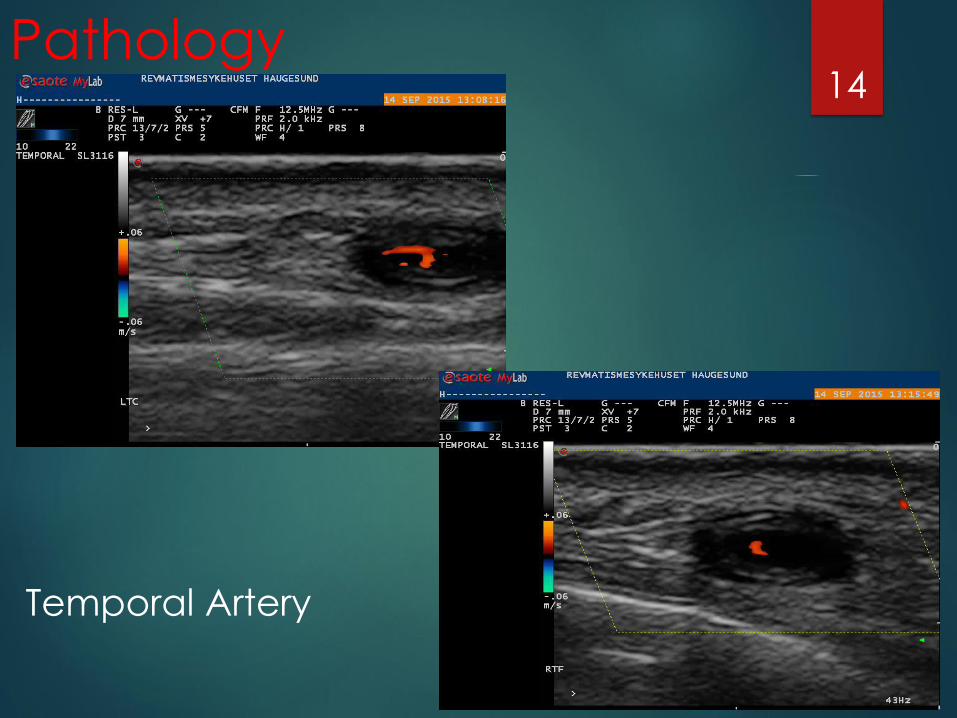
14
Temporal Artery
Pathology

15
Axillary ArteryCourtesy Dr S Chrysidis
Pathology

Schäfer VS, et al. Ann Rheum Dis 2016 (Abstract FRI0393)
Artery N IMT in mm
Cut-off
in mm
Sensitivity Specificity Correctly
classified
Common
superficial
temporal artery
40 C: r. 0.23 (SD 0.03)
l. 0.23 (SD 0.04) r. 0.42
l. 0.45
100 %
100 %
100 %
100 %
100 %
100 % 28 P: r. 0.66 (SD 0.18)
l. 0.65 (SD 0.19)
Frontal branch 40 C: r. 0.19 (SD 0.03)
l. 0.19 (SD 0.04) r. 0.35
l. 0.34
100 %
100 %
100 %
100 %
100 %
100 % 26 P: r. 0.53 (SD 0.19)
l. 0.55 (SD 0.18)
Parietal branch 40 C: r. 0.19 (SD 0.03)
l. 0.20 (SD 0.03) r. 0.32
l. 0.29
100 %
94.4 %
100 %
100 %
100 %
98.3 % 23 P: r. 0.51 (SD 0.18)
l. 0.48 (SD 0.16)
Facial artery 40 C: r. 0.24 (SD 0.05)
l. 0.23 (SD 0.05) r. 0.37
l. 0.40
92.3 %
81.8 %
100 %
97.5 %
98.1 %
94.1 % 15 P: r. 0.55 (SD 0.19)
l. 0.51 (SD 0.19)
Axillary artery 40 C: r. 0.59 (SD 0.10)
l. 0.59 (SD 0.10) r. 1.1
l. 1.0
100 %
100 %
100 %
100 %
100 %
100 % 26 P: r. 1.80 (SD 0.41)
l. 1.62 (SD 0.39)
0.4 mm
0.35 mm
0.3 mm
0.4 mm
1.0 mm
IMT Criteria

Temporal Artery-Anatomy
Lumen Vessel wall Vmax
mm mm cm/s
Parietal 0.8 0.7 57
Frontal distal 0.8 0.7 54
(> 2 cm fra bifurcation)
Frontal proximal branch 0.7 0.7 52
(< 2 cm fra bifurcation)
Common superficial 1.7 59
Schmidt WA, et al. N Engl J Med 1997;337:1336-42

T Parietalis
Facialis transv
Carotis interna
A. Occipitalis
T frontalis
Temporalis com
Carotis externa
Facialis
Examination Technique

Diamantopoulos AP: Ultrasound in Vasculitis. In: Musculoskeletal Ultrasound Review. Springer 2016
Examination Technique
Common temporal artery

Parietal temporal artery
Examination Technique
Diamantopoulos AP: Ultrasound in Vasculitis. In: Musculoskeletal Ultrasound Review. Springer 2016

Frontal temporal artery
Diamantopoulos AP: Ultrasound in Vasculitis. In: Musculoskeletal Ultrasound in Rheumatology. Springer 2016, in print
Examination Technique

Occipital artery
Examination Technique
Diamantopoulos AP: Ultrasound in Vasculitis. In: Musculoskeletal Ultrasound Review. Springer 2016
Facial artery
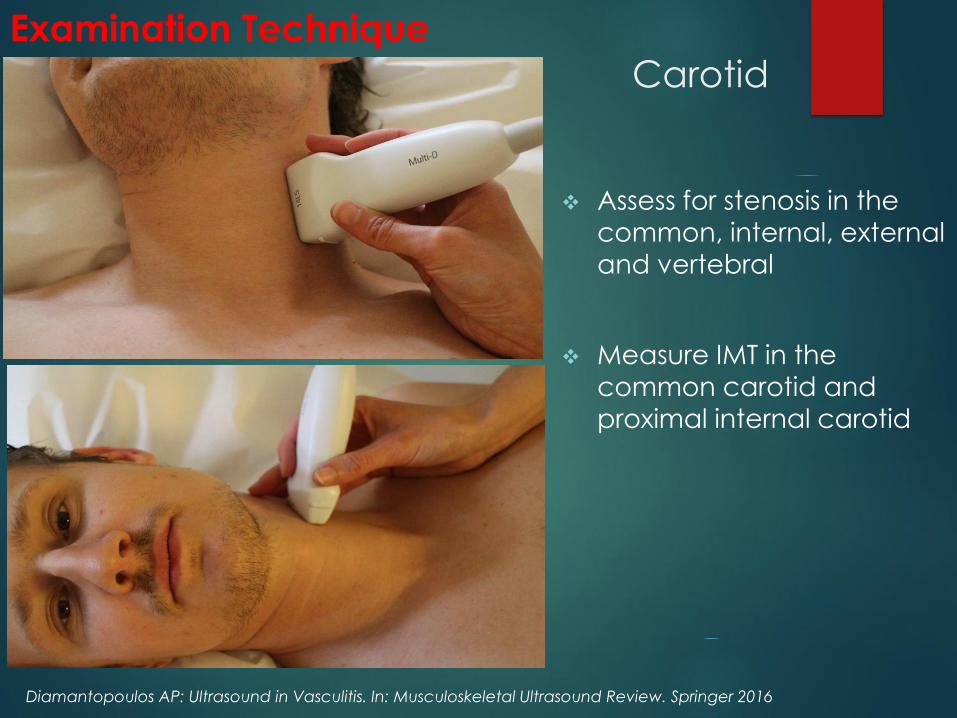
Carotid
Examination Technique
Assess for stenosis in the
common, internal, external
and vertebral
Measure IMT in the
common carotid and
proximal internal carotid
Diamantopoulos AP: Ultrasound in Vasculitis. In: Musculoskeletal Ultrasound Review. Springer 2016

Examination Technique
Axillary and
Subclavian arteries
The examination should be continued distally until the
brachial artery is visible in the
upper arm
Measure peak systolic
velocities (PSV)and intima
media thickness (IMT)
Diamantopoulos AP: Ultrasound in Vasculitis. In: Musculoskeletal Ultrasound Review. Springer 2016

Fast Track Clinic
Diagnosis and follow up
Dr. Diamantopoulos
performs ultrasound
exams at each clinic
visit.
May decrease steroids
if patient is stable or in
remission.
25

26

Giant Cell Arteritis and
The UWMC Experience 27
5 patients with known TA
4 vendors with range of transducer frequencies
12 MHz
15 MHz
22 MHz
24 MHz
40 MHz
70 MHz
RVT’s practiced scanning temporal artery branches

Giant Cell Arteritis and
The UWMC Experience 28
Invited 5 patients with known TA
Had 4 vendors with range of transducer frequencies
12 MHz
15 MHz
22 MHz
24 MHz
40 MHz
70 MHz
Vascular Technologists practiced scanning temporal artery branches

Summary-
Screening for Giant Cell Arteritis
With proper equipment, Vascular Laboratories have a role
Diagnose Giant Cell Arteritis
Follow up and monitor treatment
29

Many of the slides in this presentation were
borrowed from Andreas Diamantopoulous, MD and Elizabeth Jernberg, MD
30

31
32
Thank you for your attention