Embed Size (px)
Citation preview

Screening
Dr Gerry Bryant
What is screening?
Systematic application of a test or enquiry, to identify individuals at sufficient risk of a specific disorder to benefit from further investigation or direct preventive action, among persons who have not sought medical attention on account of symptoms of that disorder
Sieving, sorting, treating

Why screen?
• Protection of public health
• Prior to entering an organisation
• Protection of the workforce
• For life insurance
• Early diagnosis of disease

Some screening programmes can help
All screening programmes can harm

Pros & cons of screening
Advantages Disadvantages
Better prognosis Safety, inconvenience & discomfort of the test
‘Nicer’ treatment False positive – intervention anxiety Reassurance of a normal test False negative – false reassurance
True positive – lead time bias True negative – perpetuates unhealthy
lifestyle Overdiagnosis of minor abnormalities Ethical issues – informed consent,
coercion, discrimination, stigmatization, medicalisation, genetic underclass
Opportunity cost

Testing a screening programme- Wilson & Junger Criteria (1968)
1 The condition being screened for should be an important health problem
2 The natural history of the condition should be well understood3 There should be a detectable early stage4 Treatment at an early stage should be of more benefit than at a
later stage5 A suitable test should be devised for the early stage6 The test should be acceptable7 Intervals for repeating the test should be determined8 Adequate health service provision should be made for the extra
clinical workload resulting from screening9 The risks, both physical and psychological, should be less than the
benefits10 The costs should be balanced against the benefits

Testing a screening programme- UK National Screening Committee criteria (2003)
The condition1 The condition should be an important health problem.2 The epidemiology and natural history of the condition,
including development from latent to declared disease, should be adequately understood and there should be a detectable risk factor, disease marker, latent period or early symptomatic stage.
3 All the cost-effective primary prevention interventions should have been implemented as far as practicable.
4 If the carriers of a mutation are identified as a result of screening the natural history of people with this status should be understood, including the psychological implications.
Testing a screening programme- UK National Screening Committee criteria
(2003)The test5 There should be a simple, safe, precise and validated screening test.6 The distribution of test values in the target population should be
known and a suitable cut-off level defined and agreed.7 The test should be acceptable to the population.8 There should be an agreed policy on the further diagnostic
investigation of individuals with a positive test result and on the choices available to those individuals.
9 If the test is for mutations the criteria used to select the subset of mutations to be covered by screening, if all possible mutations are not being tested for, should be clearly set out.

Testing a screening programme- UK National Screening Committee criteria
(2003)The treatment10.There should be an effective treatment or intervention for
patients identified through early detection, with evidence of early treatment leading to better outcomes than late treatment.
11.There should be agreed evidence-based policies covering which individuals should be offered treatment and the appropriate treatment to be offered.
12.Clinical management of the condition and patient outcomes should be optimised in all healthcare providers prior to participation in a screening programme.

Testing a screening programme- UK National Screening Committee criteria
(2003)The screening programme13 There should be evidence from high-quality randomised controlled trials that the screening programme is effective in
reducing mortality or morbidity. Where screening is aimed solely at providing information to allow the person being screened to make an 'informed choice' (for example, Down's syndrome and cystic fibrosis carrier screening), there must be evidence from high-quality trials that the test accurately measures risk.
14 The information that is provided about the test and its outcome must be of value and readily understood by the individual being screened.
15 There should be evidence that the complete screening programme (test, diagnostic procedures, treatment/intervention) is clinically, socially. and ethically acceptable to health professionals and the public.
16 The benefit from the screening programme should outweigh the physical and psychological harm (caused by the test, diagnostic procedures and treatment).The opportunity cost of the screening programme (including testing, diagnosis and treatment, administration, training and quality assurance) should be economically balanced in relation to expenditure on medical care as a whole (ie value for money).
17 There should be a plan for managing and monitoring the screening programme and an agreed set of quality assurance standards.
18 Adequate staffing and facilities for testing, diagnosis, treatment, and programme management should be available prior to the commencement of the screening programme.
19 All other options for managing the condition should have been considered (for example, improving treatment and providing other services), to ensure that no more cost-effective intervention could be introduced or current interventions increased within the resources available.
20 Evidence-based information, explaining the consequences of testing, investigation, and treatment, should be made available to potential participants to assist them in making an informed choice.
21 Public pressure for widening the eligibility criteria for reducing the screening interval, and for increasing the sensitivity of the testing process, should be anticipated. Decisions about these parameters should be scientifically justifiable to the public.
22 If screening is for a mutation, the programme should be acceptable to people identified as carriers and to other family members.

11
Randomised control trials of screeningtim
e
randomise
screen no screen
outcome outcome
treat early disease
treat at time of presentation
screen
no disease or risk factor identified
early disease or risk factor identified
outcome
randomise
treat early disease
treat at usual time of presentation
outcome

12
Bias in screening programmesLead time bias
35 40 41 43 46
biologic onset of disease
disease detectable by screen
Woman A diagnosed at screen
Symptoms develop - Woman B diagnosed
Woman A & B die of disease
3 year survival
5 year survival
Length time biasover-representation among screen-detected cases of those with long pre-clinical phase of disease - less rapidly progressive
13
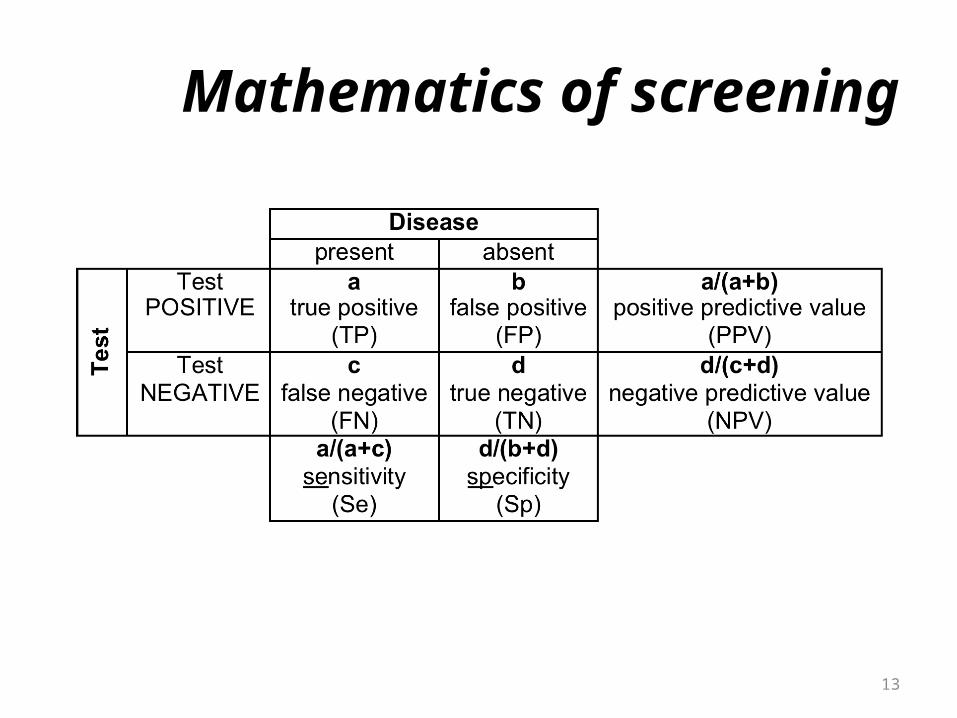
Mathematics of screening

14
Sensitivity and specificity
Sensitivity = a/(a+c)• if you have the disease, probability of testing positive
(want to be high)Specificity = d/(b+d)• if you do not have the disease, probability of testing
negative (want to be high)

15
Predictive values
Positive predictive value = a/(a+b)• probability that a person with a positive test has the
diseaseNegative predictive value = d/(c+d)• probability that a person with a negative test does
not have the disease

NHS Cancer Screening Programmes- Breast Screening (1988)
To detect cancer or DCIS• Who?
– women aged 50-70 years by invite, >70 by self-referral• What?
– mammography• How often?
– every 3 years• Recent changes?
– extend to 47-73 years from 2012• Cost?
– £75m per year in England– £37.50 for each woman invited– £45.50 for each woman screened
• Does it work?– 500 women screened – 1 breast cancer death prevented
• Who does what?– PCT– Primary Care Team– Breast Screening Unit– Breast Surgery

NHS Cancer Screening Programmes- Cervical Cancer Screening (1988)
To detect pre-cancerous changes - CIN• Who?
– women aged 25 to 65 years• What?
– liquid-based cytology of cells from cervical sweep• How often?
– women aged 25 to 50 every 3 years– women aged 50 to 65 every 5 years
• Cost?– £157m per year in England
• Does it work?– estimated prevents 3900 cervical cancers per year in England
• Who does what?– PCT– Primary Care Team– Laboratory– Colposcopy Service
• Failsafe systems– Laboratory– Colposcopy Service

NHS Cancer Screening Programmes- Bowel Cancer Screening (2006)
To detect cancer (and pre-malignant polyps)• Who?
– people aged 60-69 years– self-referral of older people by telephoning 0800 707 6060
• What?– FOB kits – by post
• How often?– every two years
• Recent changes?– roll-out to age from this year
• Cost?– £76.2m per year in England
• Does it work?– 1000 screened - 2 bowel cancers detected– 16% reduction in bowel cancer deaths
• Who does what?– Programme Hub (Eastern)– Screening Centre (Derby)– Cancer Centre (Derby-Burton)– Primary Care

NHS Screening Programmes- Diabetic Retinopathy Screening (2007)
• Who?– aged over 12 years with diabetes mellitus
• What?– digital retinal photography
• How often?– annual
• Who does what?– PCT– Primary Care– Retinopathy Screeners– Ophthalmologist

NHS Screening Programmes- Abdominal Aortic Aneurysm Screening (2013)
• Who? – 65 year old men by invitation– men > 65 years who have never been screened or treated for AAA by self-
referral– not yet available here - roll-out by 2013 (Leicestershire & South Staffs already
included) • What?
– USS of abdomen – diameter of aorta measured• How often?
– once • Will it work?
– affects 1 in 25 men aged 65-74– screening may reduce death from ruptured AAA by 50%
• Who does what?– Local Screening Centre– Vascular Surgery Service– Primary Care

Others• Prostate cancer
– men– PSA test
• Chlamydia– sexually active under 25’s– urine test - postal
• Health check – vascular risk assessment– not yet rolled out ?2013– adults over age 40 years– every 5 years– to assess / reduce / manage risk of stroke, heart disease, kidney
disease & diabetes– age, gender, ethnicity, lifestyle, smoking, family history, BMI, BP,
cholesterol– blood glucose +/- U&Es if indicated

Resources
http://www.screening.nhs.uk
http://www.healthknowledge.org.uk/sites/default/files/documents/interactivel/screening/screening_resources.pdf?op=Resources