Embed Size (px)
Citation preview

Salvatore Cazzato
Pneumologia Pediatrica
UO Pediatria-Dir. A Pession Azienda Ospedaliero-Universitaria
Policlinico S. Orsola-Malpighi Bologna
Scegliere con cura per...
l’Asma bronchiale

Recurrent episodes of wheeze, cough, and breathlessness, and physiologically by variable airflow obstruction

Clinical features that increase the probability of asthma
• More than one of the following symptoms: wheeze, cough, difficulty breathing, chest tightness, particularly if these symptoms:
– are frequent and recurrent – are worse at night and in the early morning – occur in response to, or are worse after, exercise or other triggers, such as
exposure to pets, cold or damp air, or with emotions or laughter – occur apart from colds
• Personal history of atopic disorder
• Family history of atopic disorder and/or asthma • History of improvement in symptoms or lung function in response to
adequate therapy
SIGN 2014

< 50% agreement between parents’ and clinicians’ reports of wheeze and asthma. It is important to distinguish wheezing – a continuous, high-pitched musical sound coming from the chest – from other respiratory noises, such as stridor or rattly breathing alternative diagnoses

• until a doctor has heard and documented the presence of true polyphonic (musical) expiratory wheeze, an open mind should be kept about the nature of the sound described.
– Bush et al. BMJ 2015
• “Cough variant” asthma is a controversial topic. • Isolated chronic dry cough in a community setting is rarely if
ever due to asthma – Wright et al. Am J Respir Crit Care Med 1996
• …………..not diagnose asthma unless there is a history of
considerable breathlessness, as well as either or both of cough and wheeze

Features suggestive of a non-asthma diagnosis History
• Presence of prominent upper airway symptoms – rhinitis, snoring, and sinusitis
• Symptoms from the first day of life
– primary ciliary dyskinesia, – aspiration due to incoordinate swallow, – congenital lung and airway malformations
• Sudden onset of symptoms
– suggestive of foreign body aspiration and requires immediate management.
• Presence of chronic moist cough or sputum productiony
for more … weeks and has not resolved with one course of antibiotics, referral is indicated
• History of systemic illness or suggestive of immunodeficiency:
– severe, persistent, unusual, or recurrent infections
• Continuous, unremitting symptoms with no symptom-free days
Physical examination
mod. da Bush et al. BMJ 2015

Features suggestive of a non-asthma diagnosis History
• Presence of prominent upper airway symptoms – rhinitis, snoring, and sinusitis
• Symptoms from the first day of life
– primary ciliary dyskinesia, – aspiration due to incoordinate swallow, – congenital lung and airway malformations
• Sudden onset of symptoms
– suggestive of foreign body aspiration and requires immediate management.
• Presence of chronic moist cough or sputum productiony
for more … weeks and has not resolved with one course of antibiotics, referral is indicated
• History of systemic illness or suggestive of immunodeficiency:
– severe, persistent, unusual, or recurrent infections
• Continuous, unremitting symptoms with no symptom-free days
Physical examination
• Systemic signs such as clubbing, weight loss, failure to thrive
• Upper airway disease–tonsillar hypertrophy ect..
• Unusually severe chest deformity
• Unexpected signs on auscultation (fixed monophonic wheeze, stridor, asymmetrical signs)
• Chest palpation during coughing or forced expiratory manoeuvres—palpable secretions revealed
• Signs of cardiac or systemic disease, such as a cardiac murmur, abnormalities in heart sounds, weight loss, and unusual systemic infections such as pyogenic arthritis or meningitis
mod. da Bush et al. BMJ 2015
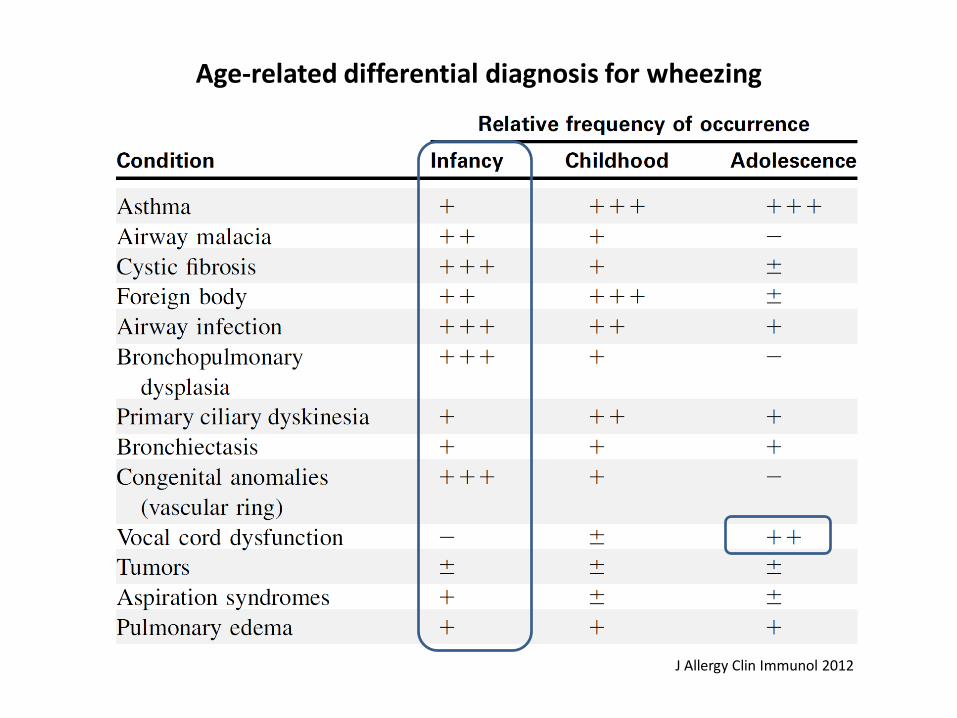
Age-related differential diagnosis for wheezing
J Allergy Clin Immunol 2012

PARADOXICAL VOCAL FOLD MOVEMENT(VOCAL CORD DYSFUNCTION)
•VCD is defined by the complete or partial adduction or closure of the vocal folds with inspiration and/or expiration. •This maladaptive process is not usually volitional but seems to occur in response to irritation of the larynx or hypopharynx or secondary to emotional or physical stress. •Exercise is a common trigger of VCD in extreme or elite athletes, often misdiagnosed as exercise-induced bronchospasm.
Asthma and comorbidities. Curr Opin Allergy Clin Immunol 2013, 13:78–86
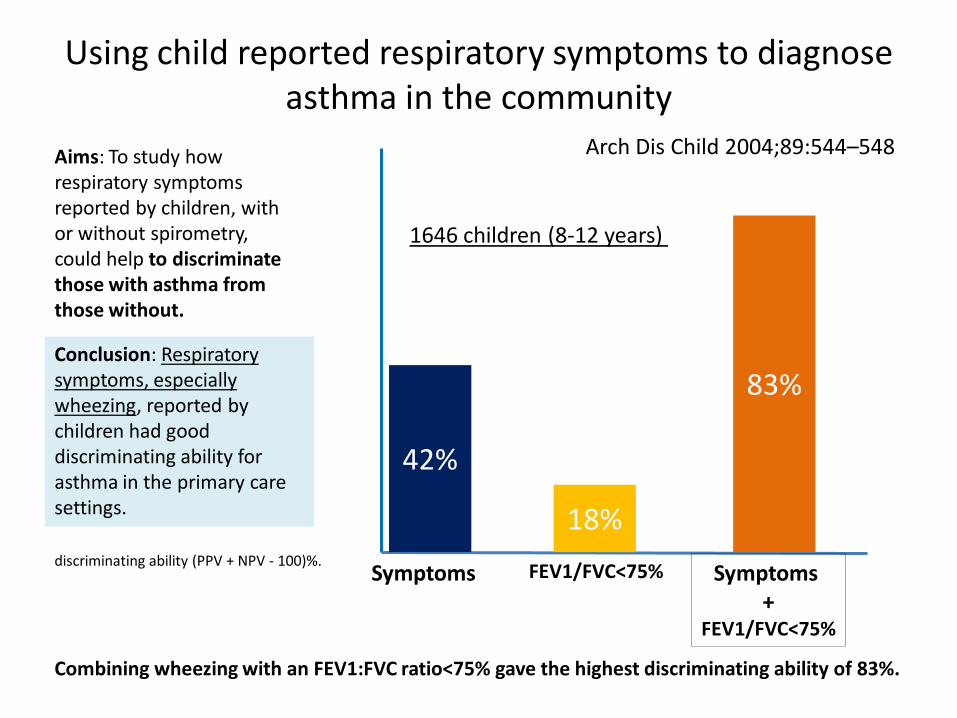
Using child reported respiratory symptoms to diagnose asthma in the community
Aims: To study how respiratory symptoms reported by children, with or without spirometry, could help to discriminate those with asthma from those without.
Conclusion: Respiratory symptoms, especially wheezing, reported by children had good discriminating ability for asthma in the primary care settings.
Arch Dis Child 2004;89:544–548
Combining wheezing with an FEV1:FVC ratio<75% gave the highest discriminating ability of 83%.
42%
Symptomss
18% FEV1/FVC<75% Symptoms
+ FEV1/FVC<75%
83%
1646 children (8-12 years)
discriminating ability (PPV + NPV - 100)%.
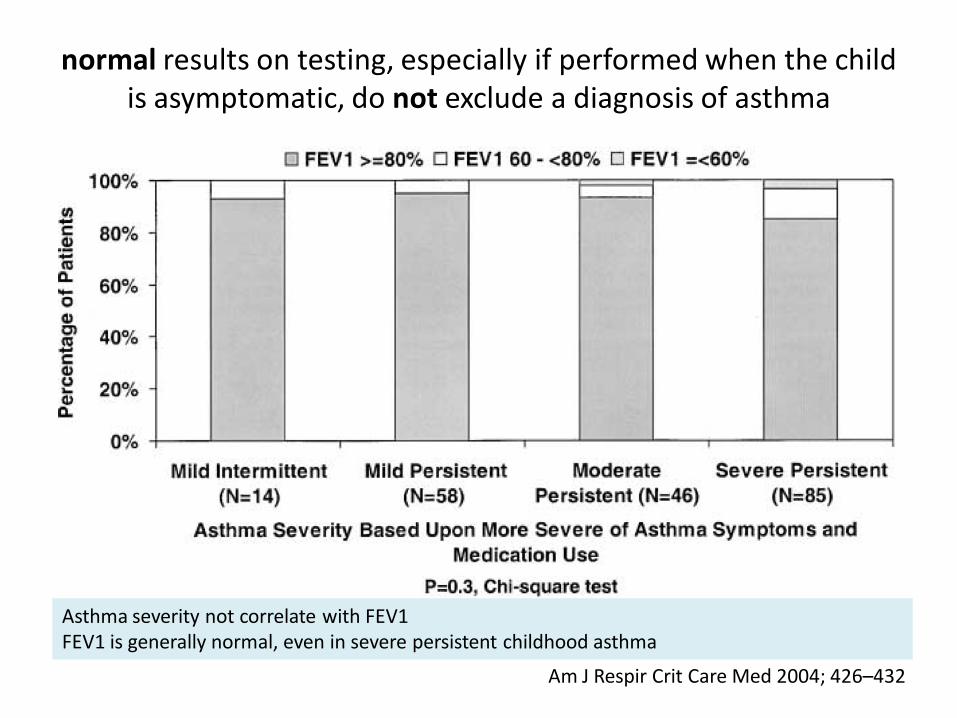
normal results on testing, especially if performed when the child is asymptomatic, do not exclude a diagnosis of asthma
Asthma severity not correlate with FEV1 FEV1 is generally normal, even in severe persistent childhood asthma
Am J Respir Crit Care Med 2004; 426–432

an absent response to bronchodilators not exclude asthma
a positive BDR test is specific for recent wheeze but is fairly insensitive ………positive response is much more likely in children with wheeze than in children without wheeze, but about half of the wheezers will be missed.
Thorax 2005;60:13–16

Bronchodilation and bronchoconstriction: Predictors of future lung function in childhood asthma
J Allergy Clin Immunol 2006;117:1264-71
bronchodilator response may indicate good response to inhaled corticosteroids.

A raised FENO is neither a sensitive nor a specific marker of asthma with overlap with children who do not have asthma
Eur Respir J 2005; 25: 455–461
Distribution of nitric oxide levels in exhaled air (FE,NO) in high-risk (●) and low-risk (○) children with (+) and without (-) elevated specific immunoglobulin (Ig)E to inhalant allergens. Children using inhaled corticosteroids were excluded. Bars represent geometric means.
429 children

A raised FENO is neither a sensitive nor a specific marker of asthma with overlap with children who do not have asthma
Eur Respir J 2005; 25: 455–461
Distribution of nitric oxide levels in exhaled air (FE,NO) in high-risk (●) and low-risk (○) children with (+) and without (-) elevated specific immunoglobulin (Ig)E to inhalant allergens. Children using inhaled corticosteroids were excluded. Bars represent geometric means.
429 children
At present, there is insufficient evidence to support a role for markers of eosinophilic inflammation in the diagnosis of asthma in children. They may have a role in assessing severity of disease or response to treatment.
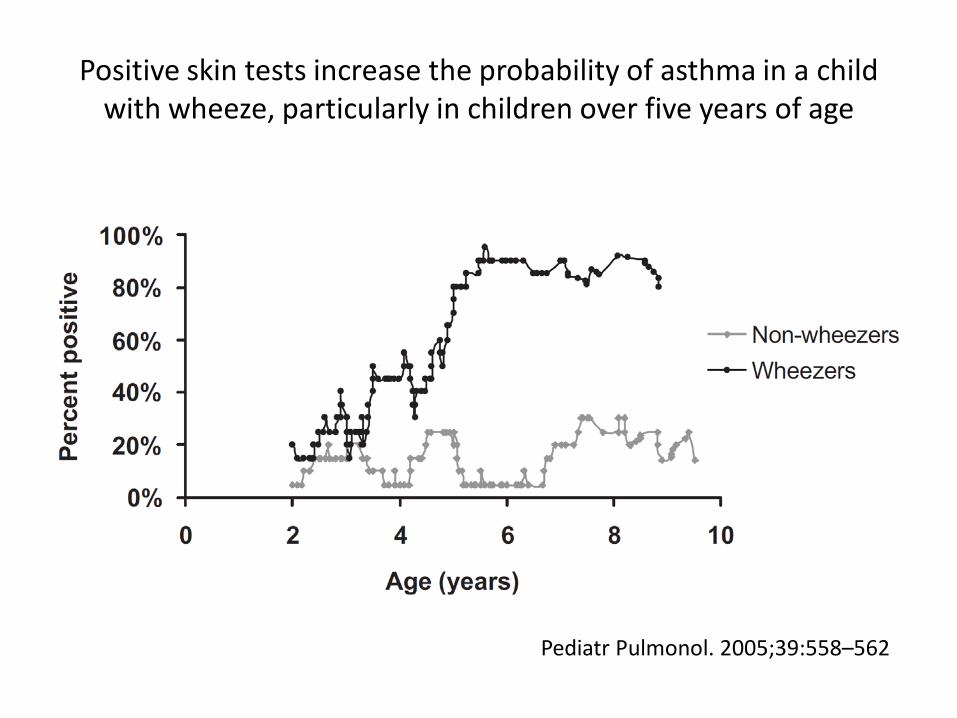
Positive skin tests increase the probability of asthma in a child with wheeze, particularly in children over five years of age
Pediatr Pulmonol. 2005;39:558–562

Conclusioni SIGN 2014 • British guideline on the management of asthma
• La diagnosi di asma è clinica
– valutazione dei sintomi e storia
personale e familiare di atopia – esclusione accurata di diagnosi
alternative
• Confermata da evidenza di ostruzione variabile al flusso
– spirometria nella norma non
esclude la diagnosi
• Test allergici (SPT/ IgE specifiche)
– supporta la diagnosi di asma allergica
– fenotipi diversi → asma non atopica
– positività si associa a persistenza di asma in età scolare


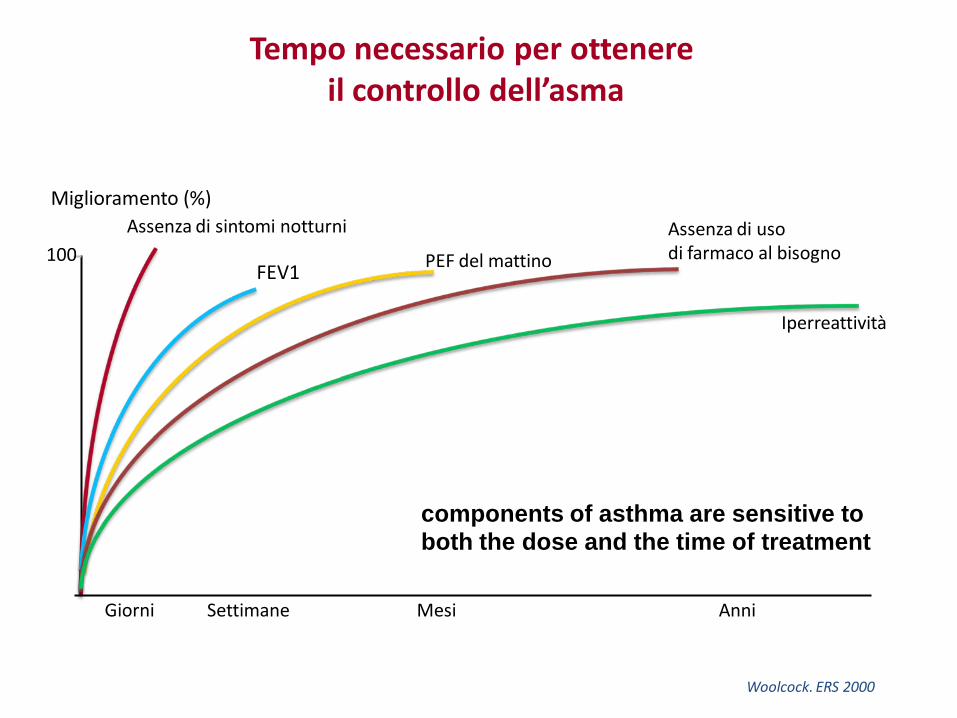
100
Anni
Miglioramento (%)
Giorni Settimane Mesi
Assenza di sintomi notturni
PEF del mattino FEV1
Iperreattività
Assenza di uso di farmaco al bisogno
Tempo necessario per ottenere il controllo dell’asma
Woolcock. ERS 2000
components of asthma are sensitive to both the dose and the time of treatment

Methods:. Data from a free running test and a methacholine inhalation challenge test were available in 218 children
Conclusions: Symptom history still forms the basis for defining asthma in clinical setting. BHR tests only marginally increased the diagnostic accuracy after symptom history had
been taken into account.
0.35 0.47
running test Methacholine test
Sensitivity Specificity
symptoms
0.78 0.97
Symptoms+tests
Symptoms