Embed Size (px)
Citation preview

Scaling Up TB Infection Control
Infrastructure Considerations
Sidney A Parsons, Ph.D. Pr. Eng.
CSIR: Built Environment, Architectural Sciences.
Tuberculosis Infection Strategy Developing Workshop
22 – 23 Oct., 2007. WHO, Geneva, Switzerland
Stop TB ProgrammeStop TB Programme

Slide 2 © CSIR 2006 www.csir.co.za
Understand the Hazard to Manage the Risk
In attempting to arrive at the truth, I have
applied everywhere for information but scarcely
in an instance have I been able to obtain
hospital records fit for any purpose of comparison”
Florence Nightingale (1863)Florence Nightingale (1863)
Notes on Hospitals:
Infection
Ventilation
Space (spacing and volume)
Lighting
Observation
Nursing care
Hospital administration process
Steel beds (not wood), Glass mugs…
“Functionality and Infection Control”

Slide 3 © CSIR 2006 www.csir.co.za
Infection Control
Understanding the basics:
• Transmission dynamics:
• Food
• Fomites
• Water
• Air
• Air borne Infection:• Environment
• Host immunity and resistance
• Procedures and associated risks
• Disinfection, decontamination and sterilisation for Minimising Transmission

Slide 4 © CSIR 2006 www.csir.co.za
Wells’ Air Centrifuge, 1931
W. F. Wells*. “On Airborne Infection, Study II. Droplets and Droplet Nuclei” , Am J Hygiene, 1934:20. 611-18.
*Instructor, Sanitary Service, HSPH
In 1931 Wells developed his air centrifuge to sample bacteria from air

Slide 5 © CSIR 2006 www.csir.co.za
Droplets and Droplet Nuclei: The Origin
• Large respiratory particles
settle within about a meter of their source
• Fine particles nucleate into
droplet nuclei carried by air currents
Liberated by Coughing or Sneezes (respiratory tract activity):
Jennison [1942]
Richard L Riley M.D. and Francis O’Grady M.D., M.Sc. Et all

Slide 6 © CSIR 2006 www.csir.co.za
Notes from Toman’s TuberculosisQuestions and Answers (Second Edition 2004).
Rieder H, 2004: “Where is tuberculosis usually
spread and how can spread be reduced”
• The Number of cases capable of transmitting M.tuberculosis in a community (principally smear-positive cases)
• The duration of infectiousness of such cases
• The number and duration of encounters between a source of infection and susceptible individuals
Slide 7 © CSIR 2006 www.csir.co.za
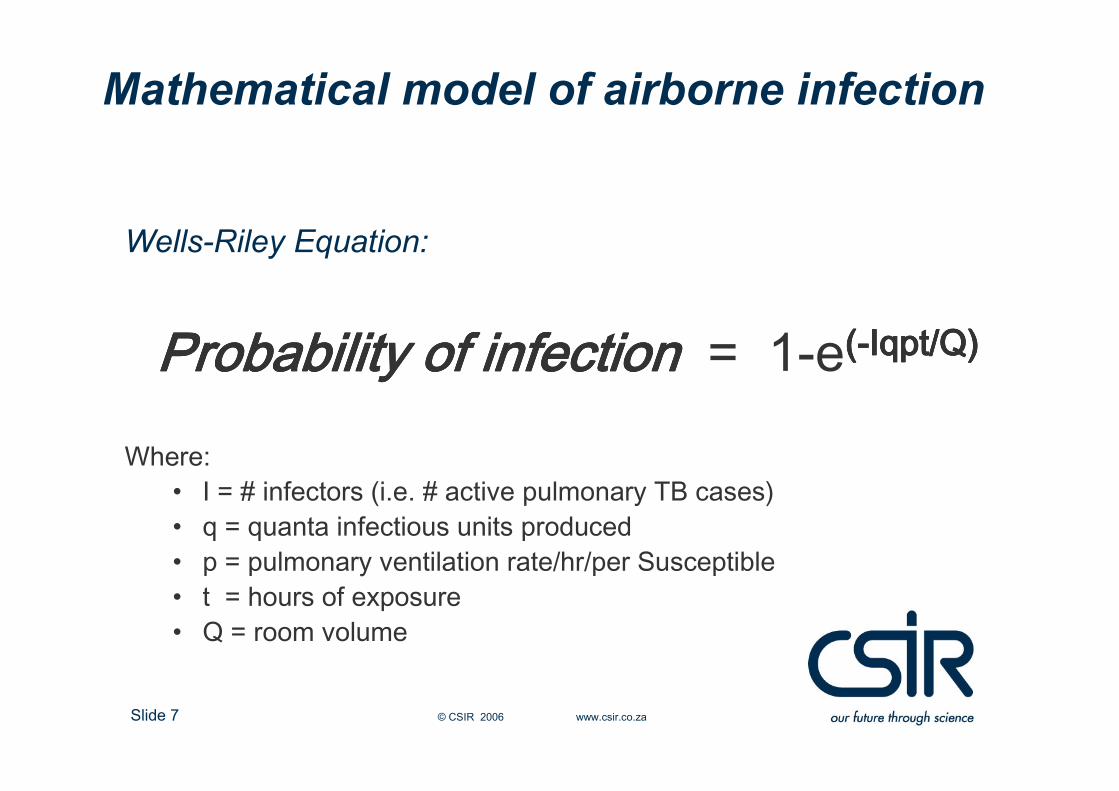
Mathematical model of airborne infection
Wells-Riley Equation:
Probability of infectionProbability of infectionProbability of infectionProbability of infection = 1-e((((----Iqpt/Q)Iqpt/Q)Iqpt/Q)Iqpt/Q)
Where:• I = # infectors (i.e. # active pulmonary TB cases)• q = quanta infectious units produced• p = pulmonary ventilation rate/hr/per Susceptible• t = hours of exposure• Q = room volume

Slide 8 © CSIR 2006 www.csir.co.za
Hierarchy of Controls for the Prevention of M.Tuberculosis Transmission
Administrative
• Ensure OPD’s can
accommodate and support the
rapid triage process and
treatment of infectious cases
• Assess risk and develop
appropriate written protocols
based on the outcome of the
assessment and administer
“Risk assessment and Infection
control plans”.
• Implement and enforce effective
work practices including the
management of patient care
• HCW and facility staff training
Slide 9 © CSIR 2006 www.csir.co.za
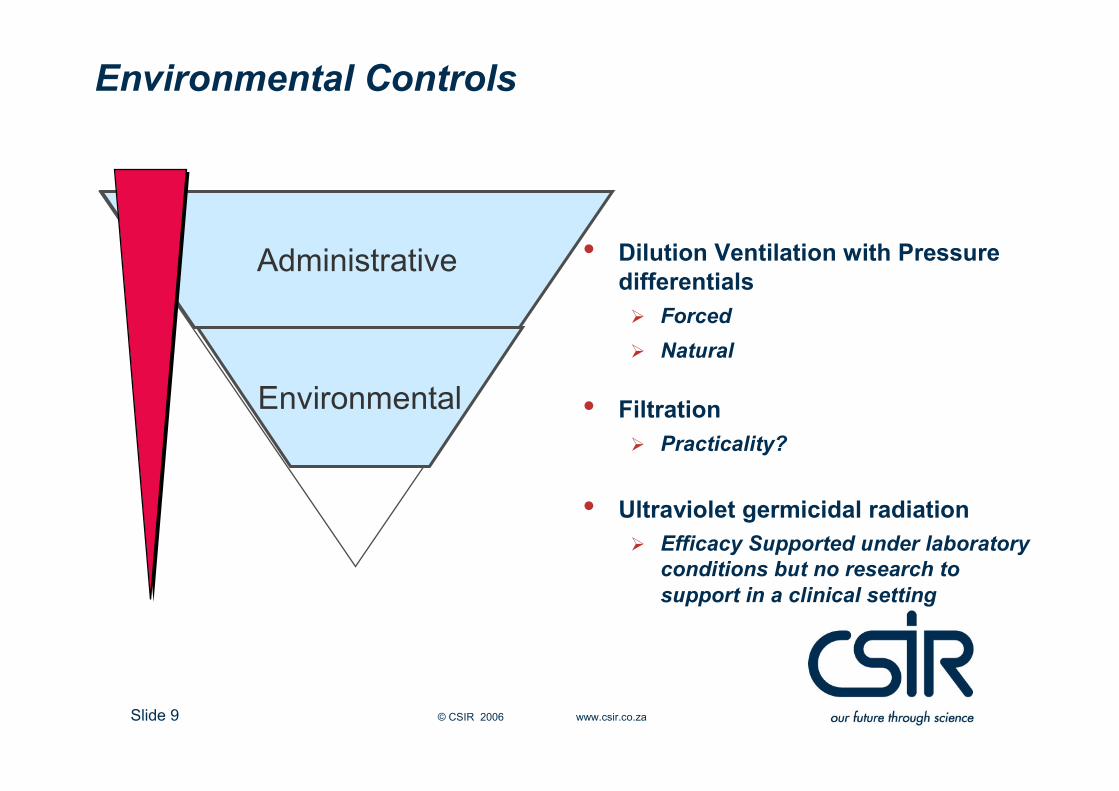
Environmental Controls
• Dilution Ventilation with Pressure
differentials
� Forced
� Natural
• Filtration
� Practicality?
• Ultraviolet germicidal radiation
� Efficacy Supported under laboratory
conditions but no research to
support in a clinical setting
Environmental
Administrative

Slide 10 © CSIR 2006 www.csir.co.za
Infection Control Risk Assessment
� To evaluate the management of the TB infection controlprogram in a facility in order to reduce risk against infection (establish the constraints of the facility to implement such a programme).
� Review existing TB infection control protocols and patient flows through the facility being evaluated.
� Evaluate compliance with personal protection practices
� Evaluate facility engineering controls and maintenance practices, and to determine their effectiveness in reducing or preventing the likelihood of TB transmission.
Some of the objectives of an Infection control Risk Assessment
for TB would be to:
Slide 11 © CSIR 2006 www.csir.co.za
The Risk of Inadequate Maintenance
� Review the Original Design Specifications and Drawings
� Know What Safety Devices are Fitted
� Understand the Operation of the System (Control Algorithms and set
points etc.)
� Understand the Operational Limitations and Determine Improper
Settings
� Identify Poor Design and/or consequent Installation, Testing and
Balancing errors
� Determine cause and effect of Equipment Failures and identify remedial
measures as required.
When Evaluating facility management and engineering controls, including
the maintenance practices, the risk assessment team should:

Slide 12 © CSIR 2006 www.csir.co.za
Extreme / Extensively Drug-Resistant TB (XDR TB)
First reported outbreak (2005/06), Tugela Ferry, South Africa
�53 of 221 MDR-TB patients identified as XDR-TB
�50% not tested previously for TB
�40 tested for HIV and all found positive
�52 died within 16 days of sputum collection
XDR first reported March 2006: Resistance to level 2 drugs suspected and identified in studies of samples from 49 countries internationally
A Moll, NR Gandhi, R Pawinski, U Lalloo, AW Sturm, K Zeller, J Andrews, G Friedland

Slide 13 © CSIR 2006 www.csir.co.za
MDR & XDR-TB
cases expected to
be treated by
country – 2007, 2008
The Global MDR-TB and XDR-TB Response Plan,
June 2007.
WHO, Stop TB Partnership

Slide 14 © CSIR 2006 www.csir.co.za

Slide 15 © CSIR 2006 www.csir.co.za
Infection Control measures must inform the need
However
The Design of the facility offers the solution by responding to
that need
Infection Control measures and the design
response.

Slide 16 © CSIR 2006 www.csir.co.za
Sustainable, Safe and Effective Functional and Healthcare
Facilities – Findings from 5 Case Studies in South Africa
Sidney Parsons, Renée du Toit, Nic Combrink, Angela Baker
The challenges of developing a TB Hospital:
� The original business case and needs interpretation
� The design briefing document submitted to the implementing agent
� How aware the hospital management were of the protocols and functional procedures called for in the TB Guidelines for healthcare provision.
� Design to ensure implementation of procedures, and;
� Appropriate Infection Controls (Administrative, Environmental and Personal), against Infection required (Reasons for and methodologies to be adopted by the design team)
.

Slide 17 © CSIR 2006 www.csir.co.za
� Healthcare planning Departments having little appreciation of epidemiological issues and procedures placing the responsibility on healthcare programs finding solutions for bed needs, and design teams needing to “fish” for the needs.
� Healthcare Planning Departments transgressing into the design domain ignoring the need for developing the essential “Briefing Document”:
� Focus on Impact and Building Durability issues far outweighing the need to address to functionality issues.
� Emphasis by building professionals on the Detailing, Documentation and Construction, rather than functionality and procedural issues.
� Following the lead from the Planners with respect to unequal emphasis on Building durability and Impact.
� Costing and development of business proposals most often based on historical, uniformed data.
Sustainable, Safe and Effective Functional and Healthcare
Facilities – Findings from 5 Case Studies in South Africa
(cont.) Sidney Parsons, Renée du Toit, Nic Combrink, Angela Baker

Slide 18 © CSIR 2006 www.csir.co.za
The Modern Challenge:• Scant appreciation of the need of a detailed brief for the planners, with very little input by healthcare staff on needs, with planners confusing the difference between a business plan and briefing document.
• Environments predisposed to infection which are not conducive to healthcare provision, least of all healing should be identified, in order to ensure against the inappropriate accommodation and mixing of;� Patients with infectious diseases
� Immune-compromised patients (and staff)
� Paediatric patients
• Limited understanding of the dynamics of infection control needs (e.g.. airborne infectious diseases) by building professionals and maintenance staff
Parsons; WHO Workshop: Making Healthcare Facilities Safe, IFHE 2006
The need for an appropriate briefing document
Slide 19 © CSIR 2006 www.csir.co.za
Current Facility Shortcomings (out-patient areas):
• Unsuspected cases visiting OPD’s that have not been designed
for triaging of suspected pulmonary cases
• OPD’s not designed for the number of visitors
• Patient flow paths in Hospitals (and clinics) due to department
relationships (i.e. Laboratory, sputum collection and waiting
areas)
• In most cases no outside waiting areas.

Slide 20 © CSIR 2006 www.csir.co.za
Observed practices due to design constraintsNo physical separation among
pts until sputum smear results available
No physical separation among
pts until sputum smear results available
Clinics & wards crowded with
TB “suspects” and susceptibles (PT’s & HCW’s)
Clinics & wards crowded with
TB “suspects” and susceptibles (PT’s & HCW’s)
Rare isolation beds;
no negative pressure rooms.
Rare isolation beds;
no negative pressure rooms.

Slide 21 © CSIR 2006 www.csir.co.za
Patient Pathways
• Proposal to separate
patients suspected
to have TB from other
OPD patients, particularly
from HIV positive patients
• Separate facilities
for MDR and XDR TB
Treatment?
Problem: many HIV
patients with Pulmonary
TB are sputum negative
Triage incl. cough
SN/clerk/Sister?
Sp-
Sp+nebulisation
CD4
counts
Clinic
referral Pt
via OPD
reception
Repeat
visit
First
Visit
Veranda outside clinic
Number given by security
OPD reception admitting clerk:
(computer) data & pt record
Paed 0-4 yrs
Assessment
consult
Immunisation
TB section
Nurses
Education
History
TB drugs
DOT
TB doctor
X Ray?
TB social
worker?
ANC/
O&G/
FPAdult Waiting &
assessment room: vitals,
urine testing, blood sugar
VCT
for
hospital
Paed 5-12
years
consulting
SOPD /
other
Wait/cons
ult
MOPD
Wait
Sputum wait & collection
& TB sputum lab
Pharmacy
General
antibiotics
X-ray
MOPD consulting
MOPD / shared
Procedure /
dressing / blood
General wards
Sputum neg.
TB suspect
patients
Paed OPD
TB wards
TB
confirmed
Home / referral
clinics
R du Toit, Health Facility Planning
Slide 22 © CSIR 2006 www.csir.co.za
Current Facility Shortcomings (in-patient accommodation):
• All types of existing rooms have been pressed into service as
MDR and XDR wards, including offices, staff housing units, etc.
• Wards were originally designed for low-cost habitation by non-
infectious TB patients
• 6 patients and more per room (20 in some facilities)
• Low floor to ceiling height (2,4m) and Inadequate thermal
performance of the building design - windows closed when cold
• Design for long stay patients in certain healthcare settings need
attention ( Landscaped areas for outdoor activity, occupational
therapy etc.)
Slide 23 © CSIR 2006 www.csir.co.za
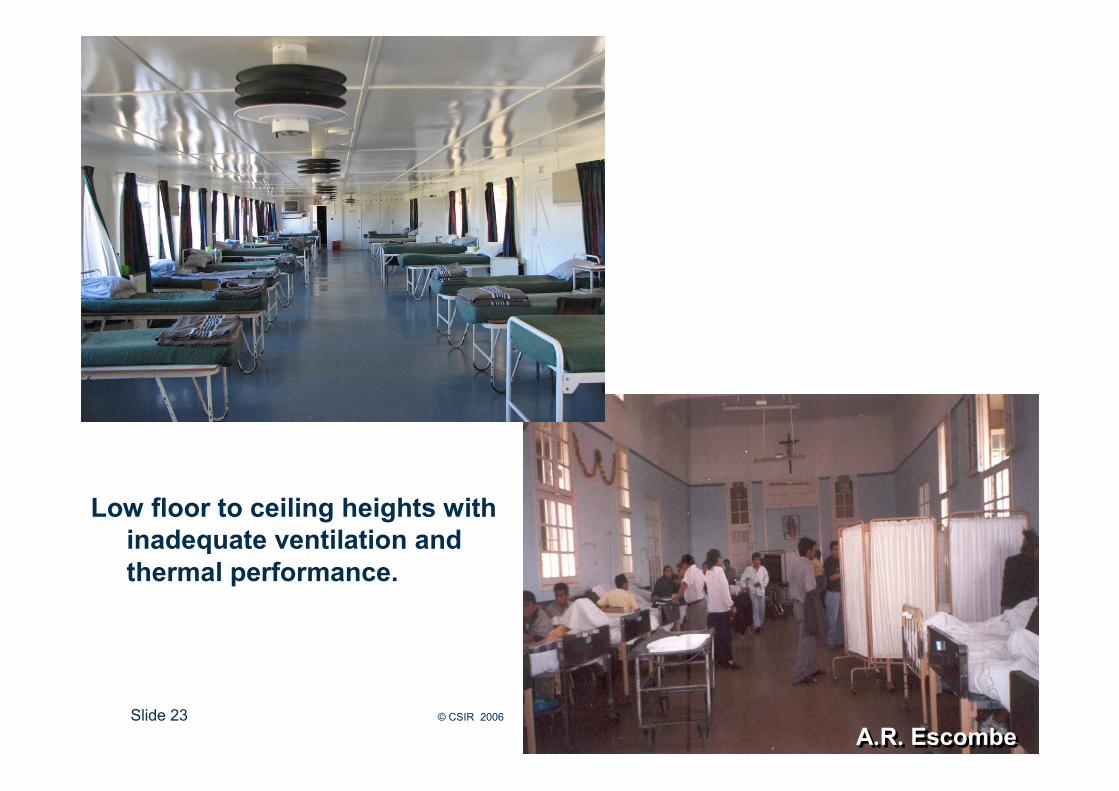
Low floor to ceiling heights with
inadequate ventilation and
thermal performance.
A.R. EscombeA.R. Escombe
Slide 24 © CSIR 2006 www.csir.co.za
Current Ventilation Shortcomings (Observed):
• Rooms ventilated using passages and other patient rooms –possible cross infection opportunity
• Natural ventilation is dependent on user-controlled opening windows
• Inconsistent wind conditions vary natural ventilation rates
• Inappropriate mechanical ventilation measures.
Slide 25 © CSIR 2006 www.csir.co.za
Administrative measures by informed design:
• Active triaging of PHC patients in all identification areas - Clinics, OPD’s etc.
• Early separation into appropriately designed rooms for further diagnosis and management
• Improved management of patients by infectious status and TB strain
• Improved management of patient movement within controlled zones
• Improved service levels in laboratory testing, diagnosis and notification
• Isolation rooms of ‘as-yet-undiagnosed’ patients in all TB Admission wards in all facilities
• Drastic reduction in number of patients per room recommended.
• Improved management of patient flow in all health facilities (patient pathways)

Slide 26 © CSIR 2006 www.csir.co.za
Detailed attention to air rate and flow management:
• Air dilution and pressure gradient design, irrespective of wind conditions, to ensure clean air workspaces
• Effective dilution ventilation by natural or mechanical means (or by mixed mode systems)
• Pressure gradients relative to room functions and layouts
• On-site validation of ventilation design prior to occupation – standard methodology in development
• Regular re-assessment as part of facility risk management SOP
Slide 27 © CSIR 2006 www.csir.co.za
Infection Control measures must inform the need
However
Design of the facility offers the solution by responding to thatneed
But
The solution must be validated to ensure quality of outcome
Health Facilities: The design response

Slide 28 © CSIR 2006 www.csir.co.za
The Risk of Inadequate Maintenance
“AppropriateDesign
Parameters”
“Service level Agreement
Procurement Policies”
“FM Standards
ofProcedures forenvironmentalServices”
“Operatingand Maintenance
Manuals”
“Maintenance”
“Integrated design approach” for engineering controls and for least risk maintenance of
all systems to ensure effective infection control strategies.

Slide 29 © CSIR 2006 www.csir.co.za
The Risk of Inadequate Maintenance:Environment & Health
Whilst being the prime means of intervention, certain systems myalso be the primary Pathogenic transmission mechanism if not maintained:
� Air Systems
� Water Systems
� Environmental (Cleaning) Services
� Services Handling Laundry and Bedding
� Regulated Medical Waste
Guidelines for Environmental Infection Control in
Health Care Facilities
Centers for Disease Control and Prevention
Healthcare Infection Control Practices Advisory Committee (HICPAC)
Slide 30 © CSIR 2006 www.csir.co.za
Issues still to be addressed
Resulting from the policy, further attention must be paid at facilities treating infectious patients over an extended period (2-6 months) to providing access to broader basic social services e.g.:
• Postal services
• Banking facilities
• Visitors
• Education
• Home Affairs processes – ID documents etc.
• Support for Children far from home
• Community Services support for breadwinners under treatment
A balance needs to be struck between the constitutional rights of patients, of staff and the broader community and the affordability of public health measures in order to protect and uphold those rights.
Slide 31 © CSIR 2006 www.csir.co.za
Advocacy and resource mobilization
• On a national level, guidance needs to be provided to healthcarefacility planners and designers
• Engineering and Architectural societies worldwide, need to be informed of the need to include IC in their design guides (e.g. ASA, ASHRAE, CIBSE. RHEVA, IFHE, UIA etc).
• Life cycle costing needs to be undertaken
• IC for airborne diseases needs to be included in the patient safety arena.
“Inform and Educate”

Slide 32 © CSIR 2006 www.csir.co.za
The World Needs Safe and Effective Functional Planning to Ensure Sustainable
Healthcare Provision
Thank YouThank You





























