Embed Size (px)
Citation preview

American Journal of Medical Genetics 118A:52–54 (2003)
Clinical Report
Satoyoshi Syndrome in a Caucasian Girl ImprovedWith Glucocorticoids
Claudia Rafaela Cecchin,1 Temis Maria Felix,1* Richard B. Magalhaes,2 and Tania Weber Furlanetto2
1Servico de Genetica Medica, Hospital de Clınicas de Porto Alegre, Porto Alegre, Brazil2Departamento de Medicina Interna, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil
Satoyoshi syndrome (OMIM 600705) is a raredisorder of unknown cause characterizedby progressive painful intermittent musclespasms, amenorrhea, alopecia, malabsorp-tion, and skeletal abnormalities mimicking askeletal dysplasia. In this report, we describea Caucasian 12-year-old girl that presentedwith characteristic manifestations, includ-ing alopecia, muscle cramps, and short sta-ture with onset at age 7. Prednisone 60 mg/m2
every other day and amytriptiline 25 mg QDwere administered. After 2 months, alope-cia had significantly improved and musclecramps had almost disappeared, so thatglucocorticoid treatment was tapered. Fol-low-up, 9 months later, showed a normallooking and asymptomatic girl.� 2003 Wiley-Liss, Inc.
KEY WORDS: Satoyoshi syndrome; alope-cia; muscle spasms; gluco-corticoid treatment
INTRODUCTION
Satoyoshi syndrome (OMIM600705) is a rare disorderof unknown cause characterized by progressive painfulintermittent muscle spasms, diarrhea, or malabsorp-tion, endocrinopathy with amenorrhea and secondaryskeletal abnormalities [Satoyoshi and Yamada, 1967].
All cases have been sporadic even in large families.The pathogenesis of the disorder seems to involve anautoimmune mechanism. Since the first report bySatoyoshi and Yamada [1967] of two cases with re-
current spasms, approximately 28 cases have beenreported [Satoyoshi and Yamada, 1967; Satoyoshi,1978; Aver’ianov et al., 1984; Yamagata et al., 1991;Ikegawa et al., 1993a,b;Merello et al., 1994; Ehlayel andLacassie, 1995].
CLINICAL REPORT
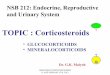
A 12-year-old girl was admitted for diagnostic evalua-tion of painful intermittent muscle spasms, alopecia,and short stature. She was born to healthy non-consanguineous parents and had two healthy brothers.Family history, prenatal, and delivery history wereunremarkable. Her growth and psychomotor develop-ment were normal until she was 7 years old, whenprogressive loss of hair on scalp and eyebrows werenoticed. At 8 years of age, she began to have recurrentand painful muscle cramps and her mother noticed thatthe girl’s growth had decreased. Muscle cramps involv-ing any muscle of the body, including abdomen, upperand lower limbs, and face became increasingly moresevere and frequent. The pain was unresponsive to theadministration of acetaminophen, diclofenac, or potas-sium chloride. There was a history of intermittentdiarrheaand she complained of abdominal pain, nausea,and vomiting. Clinical examination showed an alert andintelligent girlwithanormal face, frontal alopecia, shortstature (133 cm, <5th centile) and appropriate weight(32 kg, <5th centile) (Fig. 1). There were no pubertysigns nor bone deformities. Myoclonic jerks werefrequent during clinical examination.
Complete blood count, urinalysis, serum electrolytes,serum aldolase and liver function tests were normal.Serum creatine phosphokinasewas elevated at 2400 IU/l(normal range: 24-235 IU/l).
Serum T3, T4, and thyroid-stimulating hormone,follicle-stimulating hormone, luteinizing hormone,estradiol, cortisol, immunoglobulins (IgM, IgG andIgA, IgG subclasses), total complement activity, C3
and C4 and antinuclear antibodies were normal. D-Xylose absorption test was normal. Upper gastrointes-tinal (GI) endoscopy showed a 2 cm duodenal erosion.Gastric and duodenal biopsies showed, respectively,chronic gastritis and duodenal ulcer, H. pylori was not
*Correspondence to: Temis Maria Felix, M.D., Servico deGenetica Medica, Hospital de Clınicas de Porto Alegre, RuaRamiro Barcelos 2350, 90035-003 Porto Alegre, RS, Brazil.E-mail: [email protected]
Received 19 November 2001; Accepted 31 July 2002
DOI 10.1002/ajmg.a.10037
� 2003 Wiley-Liss, Inc.

identified. Omeprazole was administered, with resolu-tion of abdominal pain, nausea and vomiting.
Electromyographic studies showed no abnormalities,neither did the screening for diseases related to inbornerrors of metabolism. A neurology consultant, based onclinical findings and eletroencephalographic studies,ruled out convulsive disorders. Skull and spine radio-graphs and head computed tomography scan showed noabnormalities. Feet radiograph demonstrated sclerosisof some epiphyses of metatarsal bones.
With thediagnosis of Satoyoshi syndrome, prednisone60 mg/m2 every other day was initiated [Kuru et al.,1992; Yamagata et al., 1991]. After 6 weeks, musclespasms had improved. New scalp hair growthwas notic-ed after 8 weeks. Serum levels of CPK were repeatedlynormal. Prednisone was tapered. Follow-up, after 9months of treatment, showed a girl with breast devel-opment at Tanner stage II, weight of 42 kg and 134 cm ofheight. She was asymptomatic while using prednisone20 mg every other day, and amytriptiline 25 mg QD.
DISCUSSION
In this report, we describe the case of a 12-year-oldgirl who presented with clinical findings compatible
with the diagnosis of Satoyoshi syndrome. This casehas a clinical spectrum that is very similar to othersdescribed previously [Satoyoshi and Yamada, 1967;Satoyoshi, 1978; Aver’ianov et al., 1984; Yamagataet al., 1991; Ikegawa et al., 1993a,b; Merello et al.,1994; Ehlayel and Lacassie, 1995].
Although the mechanism of this syndrome is not fullyunderstood, all cases have been sporadic even in largefamilies [Satoyoshi, 1978]. In our case, there was nofamily history of similar disease. The response ofmusclespasms and alopecia to glucocorticoids and the associa-tion of some cases to myastenia gravis support thehypothesis that the pathogenesis of Satoyoshi syn-drome involves an auto immune mechanism [Satohet al., 1983]. Our patient was incapacitated and unableto attend school during the episodes of muscle spasms.Besides that, she was ashamed of her appearancebecause of the alopecia. This prompted us to initiateglucocorticoids, that were tapered once the clinicalpicture improved.
Muscle spasms seem to play a role in producingskeletal abnormalities and have been associated tothe presence of diarrhea, raising the possibility thatthis disease could be a variety of a malabsorptionsyndrome. However, in our patient, an extensiveevaluation ruled out malabsorption. The patient had aduodenal ulcer, which was probably related to the use ofnon-steroid anti inflammatory drugs, since H. pyloriwas not identified.
As it is described by Ehlayel and Lacassie [1995],patients with this condition are considered normal atbirth and infancy. Characteristic phenotype usuallyappears after the first decade of life. Clinically thissyndrome is characterized by:
* alopecia universalis.* progressive painful intermittent muscle spasm
starting between the ages of 6–15 years.* malabsorption, with evident diarrhea in �50% of
the patients.* endocrine disorders,mainly primary amenorrhea
with tendency to hypoplastic uterus and ovariesin most women.
* skeletal abnormalities, probably secondary tomuscle spasms.
The clinical features of the syndrome, particularlymuscle spasms, distinguish it from other disorders.
In our patient,muscle spasms, alopecia, short stature,and intermittent diarrhea were present. These pro-blems started when she was 7 years old, as it is reportedin other cases of Satoyoshi syndrome. This is one of a fewcase-reports of Satoyoshi syndrome in a Caucasianpatient. Her response to glucocorticoids is indisputable,but we do not know yet if we are going to be able towithdraw thismedicine. Careful follow-up ismandatoryin this case.
REFERENCES
Aver’ianov I, Vodolagin VD, Logunova LV, Levina L. 1984. Positivetherapeutic effect of diacarb in the syndrome of progressive alopecia
Fig. 1. Frontal and lateral view of the patient. Notice frontal alopecia.
Satoyoshi Syndrome 53

and diarrhea (Satoyoshi syndrome). Zh Nevropatol Psikhiatr 84:1623–1627.
Ehlayel MS, Lacassie Y. 1995. Satoyoshi syndrome: An unusual postnatalmultisystemic disorder. Am J Med Genet 57:620–625.
IkegawaS,NaganoA,NakamuraK,KurokawaT. 1993a.A case of Satoyoshisyndrome. J Pediatr Orthop 13:793–796.
Ikegawa S, Nagano A, Satoyoshi E. 1993b. Skeletal abnormalities inSatoyoshi syndrome: A radiographic study of 8 cases. Skeletal Radiol22:321–324.
Kuru S, Riku S, Nakayabu Y, Kobayashi Y, Ieda T. 1992. A case ‘‘syn-drome of progressive muscle spam, alopecia, and diarrhea (Satoyoshi)’’treated with steroid pulse teraphy. Rinsho Shinkeigaku 32:612–615.
Merello M, Garcia H, Nogues M, Leiguarda R. 1994. A mastigatory musclespasm in a non-Japanese patient with Satoyoshi syndrome successfullytreated with botulinum toxin. Mov Disord 9:104–105.
Satoh A, TsujihataM, Yoshimura T,Mori M, Nagataki S. 1983. Myastheniagravis associated with Satoyoshi syndrome: Muscle cramps, alopecia,and diarrhea. Neurology 33:1209–1211.
Satoyoshi E. 1978. A syndrome of progressive muscle spasms, alopecia, anddiarrhea. Neurology 28:458–471.
Satoyoshi E, Yamada K. 1967. Recurrent muscle spasm of central origin.Arch Neurol 16:254–263.
Yamagata T, Miyao M, Matsumoto S, Yanagisawa M. 1991. A case ofgeneralized Komuragaeri disease (Satoyoshi disease) treated withglucocorticoid. Rinsho Shinkeigaku 31:79–83.
54 Cecchin et al.