Embed Size (px)
Citation preview

RWCS 2014
Hooman Dehghan, MDRheumatology FellowStanford University

HPI• 45 yo male with PMHx of migraines, sinusitis and Sertoli-cell-only
syndrome (male sterility/azoospermia diagnosed with testicular biopsy in 2005).
• Patient was in his usual state of good health until late August 2013 when
he experienced acute onset of abdominal pain.
• He presented to the ED, found to have hypertensive urgency with a systolic BP of 200. He was given nitroglycerin, started on IV antihypertensive medication and admitted to the hospital for further work-up.
• He had abd/pelvic CT which showed absence of enhancement involving a segmental portion of the mid-to-lower pole of the right kidney with a suggestion of a filling defect within one of the segmental branches of the right renal artery with concern for renal artery thrombosis.

• He was in the hospital for 3 days, treated with IV heparin and discharged with no definite diagnosis and with no anticoagulation or antihypertensive medications.
• After discharging from hospital, he did not have any abdominal pain but remained hypertensive and had to call his MD who prescribed diltiazem for controlling his BP.
• Notably he reported extensive physical activities, including wind surfing between July and August when he was in Hawaii for vacation and had multiple non-serious trauma with some bruised ribs.

• ROS: No history of HTN or thrombosis in the past. No fever/chills, rash, joint or muscle pain, fatigue, decreased appetite or wt loss. No numbness or tingling in extremities, diarrhea, dysuria, or hematuria. No palpitation or chest pain.
• PMH: Migraines, sinusitis, Sertoli-cell-only syndrome.
• Surgery Hx: septal deviation surgery, testicular biopsy with diagnosis of Sertoli-cell-only syndrome in 2005, L temporal artery biopsy in August.
• FH: no family history of hypercoagulable state/thrombosis or rheumatologic disease. History of Renal ca in maternal grandmother and uncle. Multiple family members with cholecystitis/cholecystectomy.
• SH: drinks alcohol socially. No smoking. Married and has one healthy adopted child. He is an engineer and used to work in Russia where he had his annual medical exam, last unremarkable exam about 2 years ago.
• Allergy: Ampicillin, Chlorpheniramine, Erythromycin

• Home Meds: Motrin , Imitrex , Maxalt, Diltiazem 240mg qday. Arimidex (aromatase inh) for his Sertoli-cell-only syndrome (March-August); already stopped before his current presentation.
P/E:• BP: 146/99 PR: 65 RR: 14 Temp: 36.1 °C (97 °F) Ht: 1.88 m (6' 2") Wt: 183 lbs• General Appearance: NAD • HEENT: EOMI, PERRL, Nose: without ulcers. Mouth: moist, no ulcers. No Sinuse
tenderness. Well healed site of L temporal artery biopsy. • Neck: Thyroid not palpable, no LAP, no JVD or carotid bruits • Chest: Clear, No rales/wheezing • CV: RRR with nl S1 & S2, no M/G/R • Abd: soft, non tender, no mass or organomegaly, +BS , no bruits • Ext: without cyanosis, clubbing or edema, 2+ DP pulses • Neuro: A&Ox3, CN II-XII intact, +5/5 strength BUE and BLE, DTR 2/4, Sensation to
light touch grossly intact. Gait nl. • Skin: nails and nail beds wnl, no color changes in digits, no digital puffiness or
sclerodactyly. No nodules or skin rashes. • MSK: no joint tenderness, swelling, synovitis or deformity, full ROM

Labs:
ESR 6CRP <0.2PR3 <0.2 MPO <0.2ACA IgG/IgM, Beta-2 GP, LAC: Negative
HBS Ag/HCV Ab: negBlood Cx: negUA: SG 1.013, trace blood, neg Pr, 0-3 RBC, 0-2 WBC
Retic 1.2 JAK2 mutation: NegativeFlow cytometry for PNH: Negative

Initial Work-Up:
• Kidney US (8/2013)
3.3 x 2.4 x 2.9 cm focal area of heterogeneous echogenicity within the lateral aspect of the lower pole of right kidney which has absent cortical perfusion. Renal infarction is favored given the absence of vascular flow.
• CT abd/pelvis (8/2013)
absence of enhancement involving a segmental portion of the mid-to-lower pole of the right kidney. A filling defect with one of the segmental branches of the right renal artery which may reflect renal artery thrombosis. In addition, there is apparent luminal narrowing of portions of the superior mesenteric artery involving the ileal branches.
• Temporal artery biopsy (8/2013): Negative

Further Work-Up:
- Bilat Carotid/Vertebral artery US: No ICA stenosis. Antegrade flow in the R/L vertebral artery. Normal flow in the R/L subclavian artery.
- Echo: Normal LV/RV size and systolic function. Mild TR. RVSP 23 mmHg

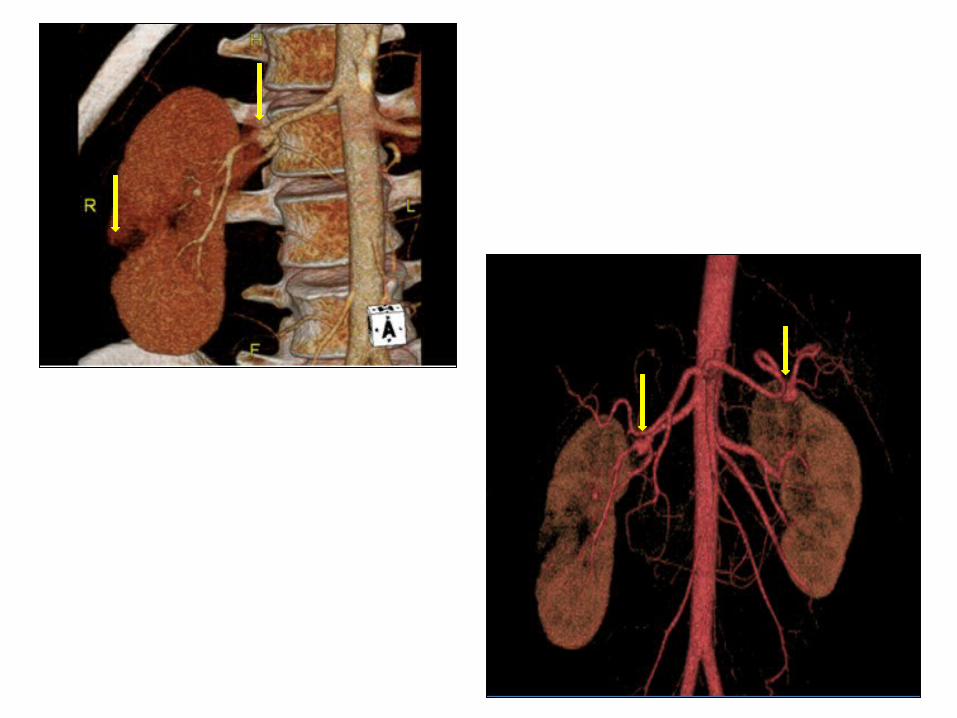
CT Angio Abd/Pelvis (9/2013)
1. SEGMENTAL SCARRING OF THE RIGHT KIDNEY, CONSISTENT WITH HISTORY OF PRIOR INFARCTION. ONGOING LARGE PERFUSION DEFECT OVER HALF OF THE RIGHT RENAL PARENCHYMA. Normal left kidney.
2. MAIN RIGHT RENAL ARTERY, LEFT RENAL ARTERY, SMA BRANCH, AND INTERNAL ILIAC BRANCH ARTERY ANEURYSMS.
3. No calcified and non-calcified atherosclerotic plaque in the abdominal aorta. Abdominal aorta is not aneurysmal.
Multiple visceral artery aneurysms: • 1.2 cm splenic artery aneurysm• 1.0 cm R renal artery aneurysm • 0.8 cm L renal artery aneurysm • 0.4 cm R renal artery branch aneurysm • 4 mm SMA branch aneurysm • 5 mm obturator branch of the internal iliac artery aneurysm




DDX:
• POLYARTERITIS NODOSA (PAN) ?
• FIBROMUSCULAR DYSPLASIA (FMD)?

Polyarteritis Nodosa (PAN)• PAN is a small and medium–sized arteritis affecting multiple organs,
especially the skin, peripheral nerve, gut, kidney, and heart.
• Age of onset ranges from childhood to late adulthood but averages 40 years.
• Men are twice as likely to be affected than women.
• A minority of patients with PAN have an active hepatitis B infection.
• In the rest of the cases, the cause(s) is unknown (idiopathic).
Diagnosis:• Confirming the diagnosis requires either biopsy specimen showing small– or
medium–sized arteries, or mesenteric arteriography showing microaneurysms or alternating areas of stenosis and dilation.
• Because mesenteric angiography is 60% sensitive, it should be done when there is not a symptomatic site to biopsy.
• Renal biopsy should be avoided unless angiography rules out microaneurysms susceptible to rupture.

ACR Criteria for the Classification of Polyarteritis Nodosa (PAN)
Classified as PAN if at least 3 of the 10 criteria are present:
• Weight loss > 4 kg: since illness began, not related to dieting or other factors. • Livedo reticularis: over the skin of portions of the extremities or torso. • Testicular pain/tenderness: not due to infection, trauma or other causes. • Myalgias, weakness or leg tenderness: Diffuse myalgias (excluding shoulder or hip girdle)
or weakness of muscles or tenderness of leg muscles. • Mono- or polyneuropathy: mononeuropathy, multiple mononeuropathies or
polyneuropathy. • Diastolic BP >90 mmHg: hypertension with the diastolic BP higher than 90 mmHg. • Elevated BUN or creatinine: BUN >40 or Cr >1.5, not due to dehydration or obstruction. • Hepatitis B virus: Presence of hepatitis B surface antigen or antibody in serum. • Arteriographic abnormality: Arteriogram showing aneurysms or occlusions of the visceral
arteries, not due to arteriosclerosis, fibromuscular dysplasia or other non-inflammatory causes.
• Biopsy of small or medium-sized artery containing polymorphonuclear cells: the presence of granulocytes or granulocytes and mononuclear leucocytes in the artery wall.
These criteria have a reported sensitivity of 82.2% and a reported specificity of 86.6% for the classification of polyarteritis nodosa compared with other vasculitides.

Treatment:
• Without treatment, almost all affected patients die within 2 to 5 years.
• Treatment with prednisone (1 mg/kg daily) and cyclophosphamide (2 mg/kg daily) appeared to revolutionize the outcome of polyarteritis nodosa by achieving 70% 10–year survivals and established this combination of agents as the standard therapy.
• Newer studies suggest that prednisone alone may achieve the same high survival as prednisone and CYC, although flares were less frequent in patients taking CYC.
• PAN associated with hepatitis B respond to treatment with prednisone and CYC, but should be avoided as almost all survivors become chronic carriers of hepatitis B and may die later of cirrhosis or variceal bleeding.

Fibromuscular dysplasia (FMD)• Non-atherosclerotic, non-inflammatory vascular disease that causes abnormal
growth within the wall of an artery. • FMD has been found in nearly every arterial bed in the body. However, the most
common arteries affected are the renal and carotid arteries. • There are various types of FMD, with medial fibroplasia being the most
common. Intimal and adventitial are less common forms of the disease. • FMD predominantly affects middle-aged women, but has been found in men
and people of all ages.• Signs and symptoms that FMD patients present with is largely dependent on the
vascular bed(s) affected.
Renal Arteries• The main symptoms associated with renal FMD are hypertension and bruits
audible over the abdomen or flanks. • Complications such as aneurysms, dissections, or occlusion of the renal artery
have been associated with renal artery FMD.

Diagnosis: Time from a patient’s first signs or symptoms to diagnosis is commonly 5 years.
Non-invasive testing:– duplex ultrasonography– magnetic resonance angiography (MRA) – computed tomographic angiography (CTA)
Invasive testing through angiography is the gold standard. However, due to the higher risk of complications this is often is not done early on.
Treatment:• There is no known cure for FMD. Medical management is the most common
form of treatment.
• Blood pressure control is the primary concern when treating patients with renal FMD.
• In cases of renal stenosis and indications for intervention, percutaneous balloon angioplasty may be recommended.
• Patients with carotid or vertebral FMD should be medically managed to reduce the risk of a stroke. Aspirin, Antiplatelets and anticoagulants





























